
Abstract
This study has two aims: to explore the experiences and impact of adoption among five adults (three males and two females, all over the age of 55) adopted from mother and baby homes in the UK and Ireland, and to establish each participant’s state of mind (SOM) with regards to attachment using the Adult Attachment Interview (AAI) (George, Kaplan and Main, 1985–1996). It makes use of all information gained from the AAI by analysing the interview transcripts in two ways: (1) using the AAI scoring system (Main, Goldwyn and Hesse, 2003) to assess SOM; and (2) thematic analysis of the transcripts to produce an inductive set of themes. It was found that all participants had an insecure SOM with regards to attachment. For four out of the five participants, this was unresolved/disorganised, and the category ‘preoccupied’ was the most prevalent underlying three-way classification. Qualitative analysis of transcripts identified four overarching themes: (1) identity and belonging; (2) trauma; (3) ‘silenced’ coping; and (4) adverse parenting which reflected their experiences of adoption. The findings indicate that the participants were highly susceptible to trauma associated with loss. They also highlight the importance of suitable adoption placements and vetting of potential adopters. The clinical and research implications of the results and their contribution to the broader discussion of trauma related to adoption are discussed.
Keywords
Introduction
Mother and baby homes were institutions developed to provide accommodation for unmarried mothers and their children. Many of these establishments gained notoriety because of the maltreatment that occurred within them. The report by McCormick and colleagues(2021) on mother and baby homes in Northern Ireland was based on an extensive search of records and oral histories collected from women, staff and the children who experienced them. The report states that ‘in the vast majority of cases, trauma and, often, mental health issues have been an outcome of birth mothers’ experiences around their pregnancy’ (McCormick, et al., 2021: 21). The survivors reported that the consequences were more prevalent where adoption was the outcome, and that the institutions created barriers to accessing their birth records. Available evidence suggests that 26% of children were left with their mothers, 32% went into institutional care, 23% were adopted and 15% went into foster care.
Adoption research offers a unique insight into the nature of attachment relationships. Many adoptees and care-experienced individuals are faced with attachment disruption and the task of forming attachments to new caregivers. The length of time spent in care and the quality of care, as well as adoption pre-histories, vary significantly among individuals. But it is likely that infants placed for adoption will have experienced prenatal or birth complications and have had parents with higher levels of psychopathology than for the general population (Edens and Cavell, 1999). However, mother and baby homes were atypical from an adoption and fostering perspective. Unlike the removal of children from high-risk homes and maltreatment, this practice was unnecessary; these children had caregivers. Previous research considering risk factors attributed to birth parents’ lifestyle, addiction or abuse in the pre-adoption period may not therefore apply to mother and baby home survivors. Women were committed to the homes and children were removed from their care only because they did not conform to what was deemed socially acceptable by religious orders at the time.
Mother and baby homes were also unique from an attachment point of view because some children could spend their early lives with their mothers, albeit in an institutional setting. Meta-analytical findings have shown that institutional care is a risk factor for disorganised and insecure attachment classifications (Lionetti, Pastore and Barone, 2015; van den Dries, et al., 2009) and attachment disorders (Kennedy, et al., 2017). In addition, adoption itself appears to be a further risk factor for insecure attachment and disorganised classifications (van IJzendoorn and Juffer, 2006). Knowledge of attachment classification is important because attachment security can profoundly impact an individual’s life course. Clinical research has found a strong association between psychiatric diagnoses and attachment insecurity (van IJzendoorn and Bakermans-Kranenburg, 2008) and that attachment security is a protective factor against mental ill-health (Bakermans-Kranenburg and van IJzendoorn, 1993; Fearon, et al., 2010; McMahon, et al., 2006) and physical ill-health (Dagan, et al., 2018; Ehrlich, 2019; Ehrlich, et al., 2019). There also appears to be a transgenerational risk of parental insecurity, as adult attachment classification measured by the Adult Attachment Interview (AAI) can predict infant attachment patterns (van IJzendoorn, 1995).
The Berkeley Adult Attachment Interview (George, et al., 1985) remains the gold standard measure of adult attachment. It comprises an hour-long semi-structured, semi-clinical interview containing 20 questions that focus on the interviewee’s early and present-day attachment relationships and past experiences and the effects of these on current functioning (Main, 1991). It places two demands on the interviewee: to recall and reflect on their attachment life histories while simultaneously maintaining a coherent and collaborative discourse. The analysis of the transcripts therefore centres not only on the speaker’s ability to recall events from their childhood, but also on the coherence and plausibility of their narrative. From this information, it allocates the speaker to a classification for their overall state of mind (SOM) with respect to attachment (Main, Kaplan and Cassidy, 1985). The SOM is said to provide ‘rules and rule systems for the direction of behaviour, the felt appraisal of experience, and the direction and organisation of attention and memory’ (van IJzendoorn, 1992: 80).
There are five main classifications to which the participant can be assigned: secure-autonomous; insecure-dismissing; insecure-preoccupied; unresolved with respect to loss or trauma; and cannot classify. There are also 12 further sub-classifications. An extensive body of research has shown that the individual differences in the narratives produced during the AAI significantly correlate with infant responses during a behaviour-based assessment of separation and reunion known as the Strange Situation Procedure (SSP) (Ainsworth, et al., 1978; van IJzendoorn, 1995). This well-established relationship between parental AAI classification and infant SSP attachment pattern has been found among foster carers with their foster children (Dozier, et al., 2001). It has even been shown to predict infant attachment pattern before the first child is born (Fonagy, et al., 1991).
Despite numerous reports and commentaries, there appears to be no empirical research on the impact of adoption from mother and baby homes, even though it is known that over 10,500 women were admitted to such establishments in Northern Ireland alone (McCormick, et al., 2021). It is, therefore, unimaginable how many lives across the UK and Ireland have been affected by this practice. This study aims to shed light on the attachment and experiences of the now-adult children adopted from this source, and to inform future research and clinical practice.
Methods
Participants
Participants were recruited as part of a broader study of attachment in older (30+) adopted and care-experienced adults recruited via social media posts on Twitter and Facebook. Five of the participants in this study cohort were born in mother and baby homes in Ireland and the UK. These individuals were then grouped and analysed separately for the current study.
Procedure
Due to the ongoing Covid-19 pandemic, a decision was made for researcher and participant safety that interviews should be conducted via an online format. Although only audio was recorded, video was used by both parties throughout to recreate an in-person interview. Both participant and researcher undertook the interviews in a quiet and private area of their homes, away from other people. The interviews were transcribed verbatim in accordance with the guidelines detailed in the AAI manual supplementary material (Main, Goldwyn and Hesse, 2003).
Measure
The AAI (George, Kaplan and Main, 1985–1996) was used to determine participant SOM with regards to attachment. It takes approximately one hour to administer; the interviews for this study lasted on average for one hour and 11 minutes. The analysis rates inferred parental behaviour across five different scales, followed by scoring from 12 state of mind scales. It then allocates the participant to one of the classifications laid out in the classification section of the manual. There are three main organised states of mind:
secure-autonomous (F) insecure-dismissing (Ds) insecure-preoccupied (E).
Two further classifications, unresolved/disorganised (U/d) and cannot classify (CC), are possible along with 12 sub-classifications.
Speakers are considered secure if they appear to be valuing attachment, if they are objective about relationships and experiences and seem able to flexibly switch between the two demands of the interview. A secure narrative is, therefore, coherent and collaborative. Both types of insecure classifications (Ds and E) have marked incoherences in their discourse. Participants deemed to be insecure-dismissing (Ds) dismiss or minimise attachment relationships and their impacts; they defend against conscious awareness of attachment difficulties and may idealise or degrade relationships. Preoccupied (E) speakers, in contrast, do the opposite; they give sustained and obsessive attention to attachment relationships and experiences and maximise their effects, expressing this through anger or, more rarely, passivity or fear. In addition to these three organised strategies, speakers who show lapses in monitoring of reasoning or discourse during discussion of loss or trauma are placed into the unresolved/disorganised (U/d) category and transcripts that cannot be placed into any of the previous categories are assigned CC.
Data analysis
The study made use of all information gained through the AAI by analysing the interviews in two ways: (1) using the AAI scoring system to reveal each participant’s SOM; and (2) analysing the transcripts qualitatively to produce an inductive set of themes.
An inductive approach was taken to the qualitative analysis due to the lack of research within this population. Thematic analysis (TA) was guided by Braun and Clarke’s (2006) six-step framework and managed by NVivo 12. Transcripts were line-by-line coded and initial codes were sorted into categories. Once an initial thematic framework was created, datasets were reassessed with potential themes in mind. Each theme was reviewed in correlation to references from the transcripts and the dataset as a whole. TA was conducted by two researchers who independently analysed the transcripts and then met to agree on the final themes. Decisions regarding refinement and sub-themes were recorded throughout the entire process in NVivo 12.
Ethical considerations
The study was reviewed and approved by the University School of Psychology Ethics Committee. The researcher undertook training in administering and using the AAI prior to the study. The interviews were carried out through virtual media and the researcher was in close contact with supervisers at all times. Participants were fully informed, provided written consent to participate and were given information on support services.
Results
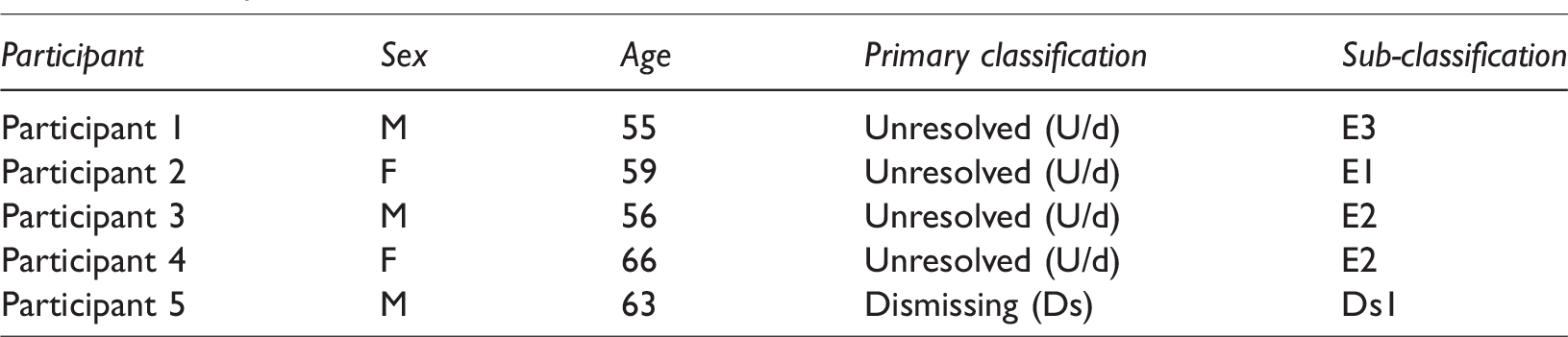
The results of this study are presented in two sections: AAI classifications (Table 1) and thematic framework and themes.
Participant AAI classifications.
The AAI classifications
All five participants were classified as having an insecure SOM by the AAI scoring system, as shown in Table 1. Four of them were unresolved (U/d) and ‘preoccupied’ (E) was the most prevalent organised classification. When participants are rated as unresolved, the coder must choose a best-fitting alternative organised classification. In the case of participants 1–4, this underlying classification was insecure-preoccupied. The preoccupied classification takes three forms: angrily preoccupied (E2) (most common), passively preoccupied (E1) and fearfully preoccupied (E3). Two participants had the subclassification E2. During E2 interviews, the speaker goes beyond what is asked in the question and overwhelms the narrative with grievances of one or both parents. Participants 1 and 2 exhibited rarer forms of the preoccupied classification, falling into the sub-classification E1 (passively preoccupied) and E3 (fearfully preoccupied) respectively. The E1 sub-classification is found approximately in two out of 120 normative transcripts and, interestingly, is also uncommon in clinical and violent populations (Main, Goldwyn and Hesse, 2003). Finally, Participant 5’s transcript was classified as insecure-dismissing and placed into the Ds1 sub-classification, making him the only participant to have an organised yet insecure primary classification. In his transcript, he appeared to dismiss most attachment-related thoughts and seemed unaware of the effects of early experiences.
Thematic analysis
The second part of the research involved analysing the transcripts qualitatively to identify an inductive set of themes. This produced four superordinate and 12 sub-themes, as shown in Table 2.
Thematic framework.
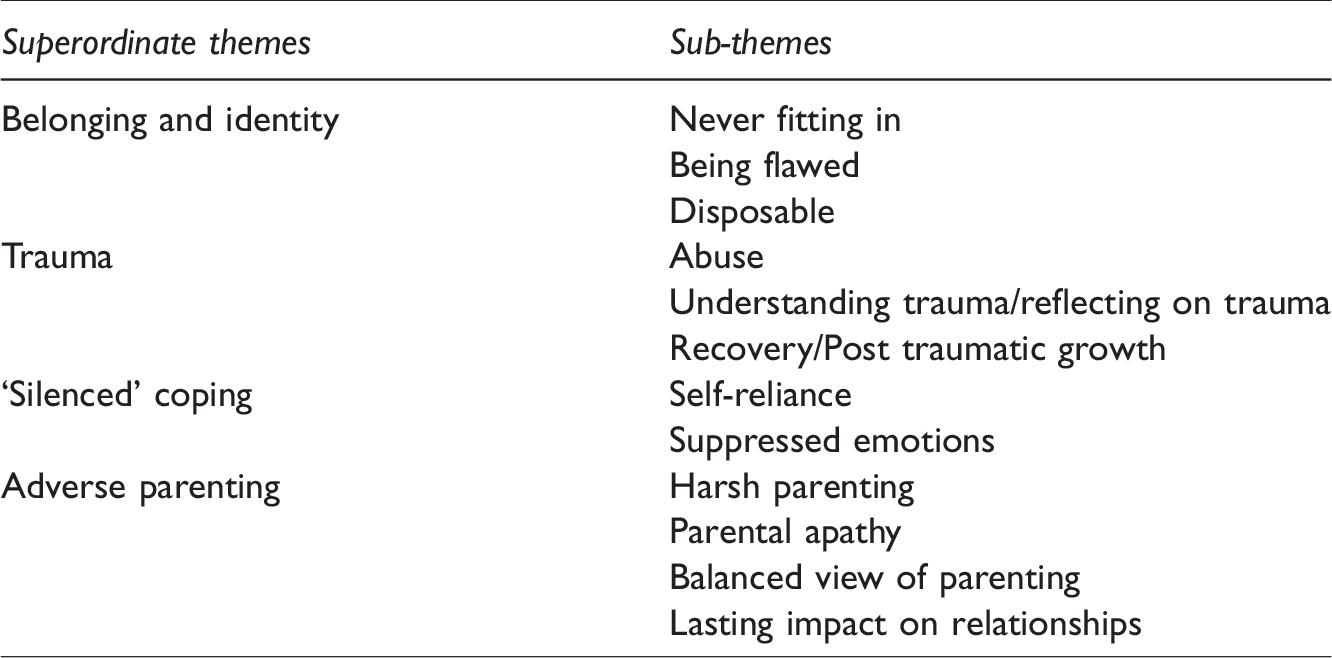
The four superordinate themes were: (1) belonging and identity; (2) trauma; (3) ‘silenced’ coping; and (4) adverse parenting. Although the impact of adoption was not directly questioned, all participants spoke of the effect their adoption from mother and baby homes had on their attachment relationships. Each theme will now be discussed in more detail.
Belonging and identity
The theme ‘belonging and identity’ captures how participants’ adoptive status affected how they saw themselves and how they viewed their relationships with others. All stated that they never felt as if they fitted in with family and/or peers. Some had expressed a marked difference between themselves and other family members, either in childhood or adulthood, as Participant 1 explained: But the way I processed it is, I’m not the same as everybody else, that I’m very different. So, you have Jamie is a member of the family, Sarah is a member of the family, Jill is a member of the family, but there is something a little bit unusual about me. I’m not a member of this family. But you always, always live with the idea that [you’re] never, never good enough – no matter what you do, what success you have, there’s always a little bit that holds back. Participant 2 highlighted how this feeling may be related more generally to being an adoptee: Um, but … I felt flawed, and I don’t know and that might be a common thing for adoptees anyway.
Participants spoke of feeling disposable in romantic relationships or recounted memories of adoptive parents threatening to ‘send them back’ or disowning them. Even those who had not reported memories of direct threats of abandonment mentioned still feeling as though this might happen or mentioned fears of being ‘sent away again’: … though I do remember my mother being very angry once and seemed to be telling me she was going to send me back.
Trauma
A prominent theme identified from the data was trauma. Four out of the five participants spoke of the trauma they had experienced and the process of coming to terms with it. The same participants also spoke of their recovery processes. It is significant that the only one who did not mention trauma, Participant 5, had an insecure-dismissing SOM.
Most participants had experienced physical, emotional or sexual abuse, either at the hands of their adoptive parents and/or others. One participant recalls the physical abuse committed by his adoptive father: Er, and then when he when I got up to kind of 13, 14, h-he used the closed fist quite a bit as well. So quite violent.
Participant 4 spoke of sexual abuse by an unknown perpetrator: ‘… unfortunately, I was sexually abused as a child.’
Everyone who spoke of trauma also talked about the lengths they had gone to understand or reflect on it and seemed generally aware of its possible impact on current functioning. For example: I’ve got quite a strong startle reflex, and, um, I’m always, I can [see] how that’s carried into adulthood as if I’m with a partner, I might say, ‘Are you all right?’ and like my partner says, ‘Stop, asking if I’m all right’, but really, I know that’s a hangover from childhood going, ‘Are you all right, Mummy?’. I had therapy and I’d become clearer thinking, you know, you sort of start to realise that actually my reaction to something is completely – not right. So why am I doing that? I am able to contribute to the adopted community in a very rich and a very meaningful way. And I don’t think I would be able to unless I had the experiences I’ve had.
‘Silenced’ coping
When asked about their childhood, all participants indicated that they did not feel as if they could approach their adoptive parents in times of hurt or distress and, as a result, had learned to cope with hurt by themselves. This theme was created to capture references to absence of feelings of needing help and the suppression of help-seeking behaviours. Every participant recounted self-reliance when hurt or upset in childhood. The following quotation from Participant 3 was expressed in response to the question ‘What did you do when you were upset as a child?’: ‘Erm, I generally, just got on with it and shut up.’
Similarly, Participant 4 recalls handling physical hurt independently: ‘I’d come off of a swing, though really badly hurt and walked myself home.’
As a consequence of feeling as though they could not turn to their parents in childhood to alleviate distress, participants spoke of learning to cope by suppressing and internalising their emotions when upset: I probably would have an internal tantrum and get over it and then try to figure out how to deal with the situation.
One participant describes regulating her behaviour to hide distress: … things you let show and you’d internalise them … even a small, you know, as a sort of, probably a 10-year-old, you could face and, you know, just make it look as though you were fine.
Adverse parenting
The final theme derived from participants’ narratives concerned adverse parenting. Four out of the five participants reported harsh parenting through severe disciplinary actions or emotional maltreatment, which left a lasting impression on them. Participant 1 recounts how his adoptive father would physically punish him for wrongly repeating the alphabet: Ahm, and I’m dyslexic and I have a memory of me repeating the alphabet and every time I got it wrong, he would hit me with a wooden spoon. … which was torturous for us as children, because as soon as we were, kind of big enough to be able to go working with him, he dragged us to go out working with him, hail, rain or fucking shine.
Only one person, Participant, 5, did not mention harsh parenting of any kind.
Descriptions of parental behaviour in childhood revealed parental apathy, either through examples of the uninterest shown or belittling of their achievements and activities. For example, one participant spoke of receiving the lead role in a play and that her parents did not turn up to watch. In a later quotation she states that she would have been surprised if they had: But, ahm, you know where you stand when your parents don’t turn up … I probably wasn’t expecting them to turn up. I’d probably be shocked if they had. She was a single mum with four kids, ahm, it was very, very stressful. She had to learn how to drive a car, she had to learn how to get a job. Ahm, and she was stressed and she took it out on us, and took it out on me. [Birth mum came] to visit and I used to love seeing her, but then she would go and I’d be very upset. So, I then started to associate her coming with the upset of her leaving. So, it was extremely confusing, and I ended up ah, having a very mixed relationship with [birth mum] arriving in the first place, at least that’s my theory. And, in … when I look back on my, my adolescence, and my adult life, I can imagine or I can see this pattern of me sort of wanting a relationship, but also sort of wanting to hold back at the same time. I think there's always a sense I don’t want to rely on any one person. I don’t want to, I don’t want to commit to that person because I don’t want to give everything to that person, because what happens if they go?
Discussion
This study explored the experiences of and assessed the state of mind with respect to attachment in five adults adopted from mother and baby homes. The study aims were achieved using the AAI and participants’ narratives were analysed in two ways: (1) using the AAI scoring system (Main, Goldwyn and Hesse, 2003) to uncover each participant's SOM; and (2) thematic analysis of the transcripts which produced an inductive set of themes.
The AAI analysis determined that all participants had an insecure SOM which in most cases was unresolved. The most prevalent three-way organised classification was ‘preoccupied’. Participants 1 and 2 had rarer preoccupied sub-classifications, E1 and E3, the first of which is found in approximately two out of 120 normative samples and does not have a higher prevalence in clinical or violent populations (Main, Goldwyn and Hesse, 2003).
Qualitative analysis of the transcripts produced four themes: issues of belonging and identity; the prominence of trauma in participants’ discourses; adverse parenting from adoptive parents; and the tendency for participants to internalise emotions and cope with distress by themselves, a response we have labelled ‘silenced’ coping.
The findings are consistent with previous research which found institutionalised settings and subsequent adoption to be risk factors for disorganised and insecure attachment classifications (Lionetti, et al., 2015; van den Dries, et al., 2009; van IJzendoorn and Juffer, 2006). A meta-analysis of more than 4200 AAI classifications conducted by van IJzendoorn and Bakermans-Kranenburg (2008) revealed that both types of insecure SOM are over-represented in clinical populations. Specifically, individuals with borderline personality disorder and those who have experienced abuse or suicidal ideation more often have an insecure-preoccupied classification. Unresolved classifications are also strongly correlated with borderline personality disorder, abuse and suicide and, again, are over-represented in clinical populations. The unresolved classification, therefore, remains crucial in understanding patients with various clinical diagnoses. Our AAI analysis supports these findings; most participants had experienced abuse in childhood and had primary classifications of unresolved and forced three-way organised classifications of ‘preoccupied’.
The four participants who had an unresolved classification had higher U scores regarding loss, meaning that they exhibited signs of disorientation and disorganisation during discussions of loss – more so than trauma. Benjamin and colleagues (2019) postulated that loss of a loved one could be exacerbated in adoptees due to the past loss of birth parents. In addition, Goldwyn and Hugh-Jones (2011) reported that the experience of a permanent and sometimes sudden loss of one or both birth parents through fostering or adoption is in itself traumatic. Goldwyn and Hugh-Jones (2011) also found evidence for disorientated speech, namely failure to name, during separation discussions. While participants in the current study did not exhibit marked disorientated speech when referencing the separation from their birth parents or adoption, there were eight references to separation from birth parent(s) through adoption being perceived as a loss. Those who took part in the Goldwyn and Hugh-Jones (2011) research were adolescents aged 14 to 17 years old and it is possible that over time and through experience our participants have learned to resolve verbal incoherences regarding separation from birth parents.
The McCormack (2021) research and the Final Report of the Commission of Investigation into Mother and Baby Homes (2021) both show that the experiences of women who were committed to mother and baby homes were traumatic. The present study echoes this finding in mother and baby home adoptees as trauma was a prominent theme alongside unresolved SOM in almost all participants. Research has shown a significant relationship between parental unresolved AAI classification and infant disorganised attachment patterns (van IJzendoorn, 1995). Main and Hesse (1990) theorised that the exact mechanism that gives rise to lapses in the monitoring of reasoning or discourse during discussions of loss or trauma could also bring about frightening and frightened parental behaviour during interactions with their children. It is likely, therefore, that mother and baby home adoptees were already at risk for transgenerational trauma. This, combined with early life spent in institutional care, permanent separation from birth parents, and abuse and harsh parenting from adoptive parents presents a sobering insight into the aftermath of mother and baby homes.
Findings also indicate that issues with identity and belonging were a consequence of adoptive status. All participants spoke of not fitting in with peers or family members, feeling flawed and feeling disposable. Given how participants spoke about themselves, this finding would imply that self-esteem has been affected by adoption. However, this diverges from meta-analytical findings of over 10,000 adoptees (Juffer and van IJzendoorn, 2007) which found that adoptees, albeit adoptee children, had higher levels of self-esteem than non-adoptees. However, given the uniqueness of mother and baby homes and time spent in institutions, it is difficult to directly compare mother and baby home survivors with all adoptees.
Crucially, the present study highlights the importance of appropriate adoption placements and scrutiny of potential adopters. Adoptive parents’ abuse and adverse parenting caused participants to engage in emotional internalising and suppression of help-seeking behaviour. But despite these negatives, a growing body of research shows that when adoptive or fostered children are provided with sensitive and well-organised placements, they can develop secure attachments with their carers and others (Bakermans-Kranenburg, et al., 2011; Smyke, et al., 2010; Steele, et al., 2009).
Strengths and limitations
The current research has several strengths; it is the first study to utilise the AAI with a sample of mother and baby home adoptees. To our knowledge, it is also the first study to use the AAI analysis in combination with thematic analysis, both analyses being performed by the same researcher who is AAI trained. Using this approach, we were able to present a more thorough understanding of attachment difficulties and trauma faced by the participants. Furthermore, we have not neglected sub-classification reporting in our results. Sub-classification provides additional information regarding the participants’ SOM, which is relevant both clinically and empirically. Finally, by interviewing participants directly, respondents could represent themselves and their experiences in their own words, giving rise to nuances in the data that would have been missed using self-reports. The findings contribute to the broader discussion of trauma related to adoption and give practitioners a small-scale insight into a unique care-experienced population.
A limitation of the study is that participants were recruited via a larger study of care-experienced and adopted adults. As mother and baby home survivors were not the focus of recruitment, many survivors who may have wanted to talk about their experiences may not have volunteered. Additionally, a larger sample size would have enabled us to test for a significant difference between our AAI findings and the ratios expected for the general population from clinical populations.
Clinical implications
The relationship between attachment and trauma is inextricable. Mothers such as those committed to mother and baby homes, with traumatic life histories and therefore probable insecure or unresolved attachment classification, increase the likelihood of their children having a similar classification (Lyons-Ruth, et al., 2005; Main and Hesse, 1990; van IJzendoorn, 1995). Practitioners should consider the use of attachment-based interventions, such as Minding the Baby (Sadler, et al., 2013), to break this cycle of transgenerational trauma transmission. As well as the likely transgenerational risks faced by this population, participants faced abuse and harsh parenting at the hands of their adoptive parents. The most recent update of the Berkeley Longitudinal Study showed that intervening trauma was strongly associated with a change in security from infant Strange Situation pattern to adult AAI classification (Main, Hesse and Kaplan, 2005). Thus, there is a need for trauma-informed practice and appropriate intervention that address the additional traumatic experiences faced by patients with similar life histories.
Our results also indicate that participants may be more susceptible to unresolved loss. This information could be particularly relevant to practitioners working with similar populations to inform therapeutic interventions to address loss. It is important that AAI analysis carried out in clinical settings distinguishes between those who are unresolved and unresolved with regards to loss or trauma, as the two may bring about different interventions.
Future research
Research focusing on birth parent separation as a loss to adoptees is limited. A recent study (Barroso and Barbosa-Ducharne, 2019) concluded that most adoptees within their sample did not identify loss with their adoption experience. Yet participants in the current study were unresolved with regards to loss. This finding cannot be attributed to loss of birth parents specifically because separation from birth parents is not currently considered on the loss scale of the AAI. Unlike the responses in the Goldwyn and Hugh-Jones (2011) study, no signs of marked disorientated speech during discussions of birth parents were observed.
Nonetheless, there were eight references coded to separation as a loss during the qualitative analysis of the transcripts. Therefore, disorientated speech or further lapses associated with unresolved classification might have been observed if a special interest question regarding this separation had been added to the AAI protocol. Future research could fruitfully further investigate adoptees’ perception of loss of birth parents, perhaps including the impact of shame. It is extremely likely that mothers committed to mother and baby homes felt and were made to feel shame for having children out of wedlock, and feelings of shame are known to be a significant predictor of PTSD symptoms (Andrews, et al., 2000; Lee, et al., 2001). Finally, to advance the field of attachment research and clinical understanding of attachment, more transparency is needed in future reporting of AAI classifications, including sub-classification and the specific cause of unresolved status.
Conclusion
This was the first study to analyse the attachment SOM and adoption experiences of the now-adult children adopted from mother and baby homes in the UK and Ireland. All participants had an insecure attachment SOM, the majority had an unresolved SOM and ‘preoccupied’ was the most prevalent forced three-way classification. The results indicate that this group of adoptees may be more susceptible to trauma associated with loss and the value of securing appropriate adoption placements and vetting of potential adopters.
Footnotes
Acknowledgements
We would like to thank our participants for making this research possible.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.