
Abstract
Fetal alcohol spectrum disorder (FASD) is the leading non-genetic cause of developmental disability in Canada. It poses many challenges at the individual, family and societal levels. This study explores adoptive parents’ experiences of having a child with FASD in their family and how these experiences impact family well-being and, specifically, parenting, family dynamics, sources of support and coping strategies. Using an Interpretive Phenomenological Analysis (IPA) approach, in-depth semi-structured interviews were conducted with eight adoptive parents of children with FASD. Four main themes emerged, each with several subthemes: (1) managing individuals with FASD; (2) navigating family cohesion; (3) psychological warfare; and (4) experiences of supports. Findings showed how FASD affects all aspects of family life and has a constant and cumulative effect on the family’s well-being. Hope, community and parents feeling successful in their efforts were found to have strong connections to well-being.
Introduction
Fetal alcohol spectrum disorder (FASD) is an umbrella term used to describe the lifelong neuro-developmental disabilities that may result from prenatal alcohol exposure (Michaud and Temple, 2013). It is the leading non-genetic cause of developmental disability in Canada (Green, et al., 2014). Canada’s FASD research network (CanFASD, 2017) reports prevalence rates ranging from one to three per 1000 live births in the United States to as high as five out of 100 live births in other countries.
FASD affects individuals, families and societies. Mohamed and colleagues (2020: 243) documented that individuals affected by this condition have: … neurodevelopmental impairments characterised by severe difficulties in three or more of the following domains: motor skills, brain structure, cognition, language, academic achievement, memory, attention, executive functioning, affect regulation, social communication and adaptive behaviour.
Parenting a child with complex needs, such as those living with FASD, requires a breadth and depth of skills, strength and endurance. In addition to regular parenting responsibilities, parents bear a lifelong responsibility and face the complex challenge of working out how to best parent their child within the context of his/her disability. While there is relatively limited research on parenting children with FASD, the existing literature suggests ‘a plethora of challenges’ that are multilayered, intersecting at individual, family and societal levels (Sanders and Buck, 2010: 309). Green and colleagues (2014) suggest that this level of caregiving is ‘an extremely exhausting experience … and may adversely affect not only [parents’] physical and emotional well-being but also their ability to parent’ (p. 418). Family-level impacts can also include stress, financial loss, mental health issues for other family members, interfamilial relationships, isolation, employment and engagement with community and society (Caley, Winkelman and Mariano, 2009). While this research focuses on the relationship between FASD and parenting stress, several studies have reported clinically significant levels (above 90th percentile) of stress among parents (Mohamed, et al., 2020; Watson, Coons and Hayes, 2013). This is particularly concerning given the strong association between parental stress and numerous undesirable outcomes (Neece, 2014).
FASD is a lifelong disability that requires external supports in multiple areas of life for optimal outcomes to be achieved (Rasmussen, et al., 2008; Rowbottom, Merali and Pei, 2010). As Michaud and Temple (2013: 96) state, ‘The normal progression of life might not be an option’ and parenting does not end when children turn 18 years of age (Sanders and Buck, 2010). In addition, the stigmatisation of FASD, together with its often invisible nature, is problematic for everyone involved and has a direct correlation with harmful effects on both individuals and families (Sanders and Buck, 2010; Stade, et al., 2006).
FASD is a multifaceted and pressing issue with implications for individuals, families and society. While high-quality caregiving and home environments are cited as the most important factors for promoting the lifelong success of individuals affected, (Caley, et al., 2009; Sanders and Buck, 2010), most of the current literature focuses on the negative outcomes and the costs and challenges, with very little scrutiny of family experiences. Other than one study that explored the stages of caregiving, parents’ support needs, suggestions for required services and inputs at each stage (see Walls and Pei, 2013), specific research on optimal FASD interventions are ‘limited and unsystematic’ (Mohamed, et al., 2020: 244).
Given the challenges associated with FASD and the high levels of stress experienced by parents, more research is warranted on how family well-being can be optimised. An Interpretive Phenomenological Analysis (IPA) approach draws out the nuances of individuals’ narratives, providing an understanding that may more deeply inform interventions that align with the unique needs of families with FASD. The main objective of this study, therefore, was to understand adoptive parents’ experiences of having a child with FASD in their family and, more specifically, to explore parenting, family dynamics, supports and coping strategies in relation to how they affect overall family well-being.
Methods
Using an IPA approach, eight in-depth semi-structured interviews were conducted. Well-being is a broad topic and FASD is a multifaceted disability with many different aspects. Therefore, to explore families’ experiences of well-being within the context of parenting children with FASD, an adaptation of Patterson’s (2002) Family Adjustment and Adaptation Response (FAAR) Model (adapted model found in Miedema, et al., 2010) was used to provide a conceptual framework (Figure 1).
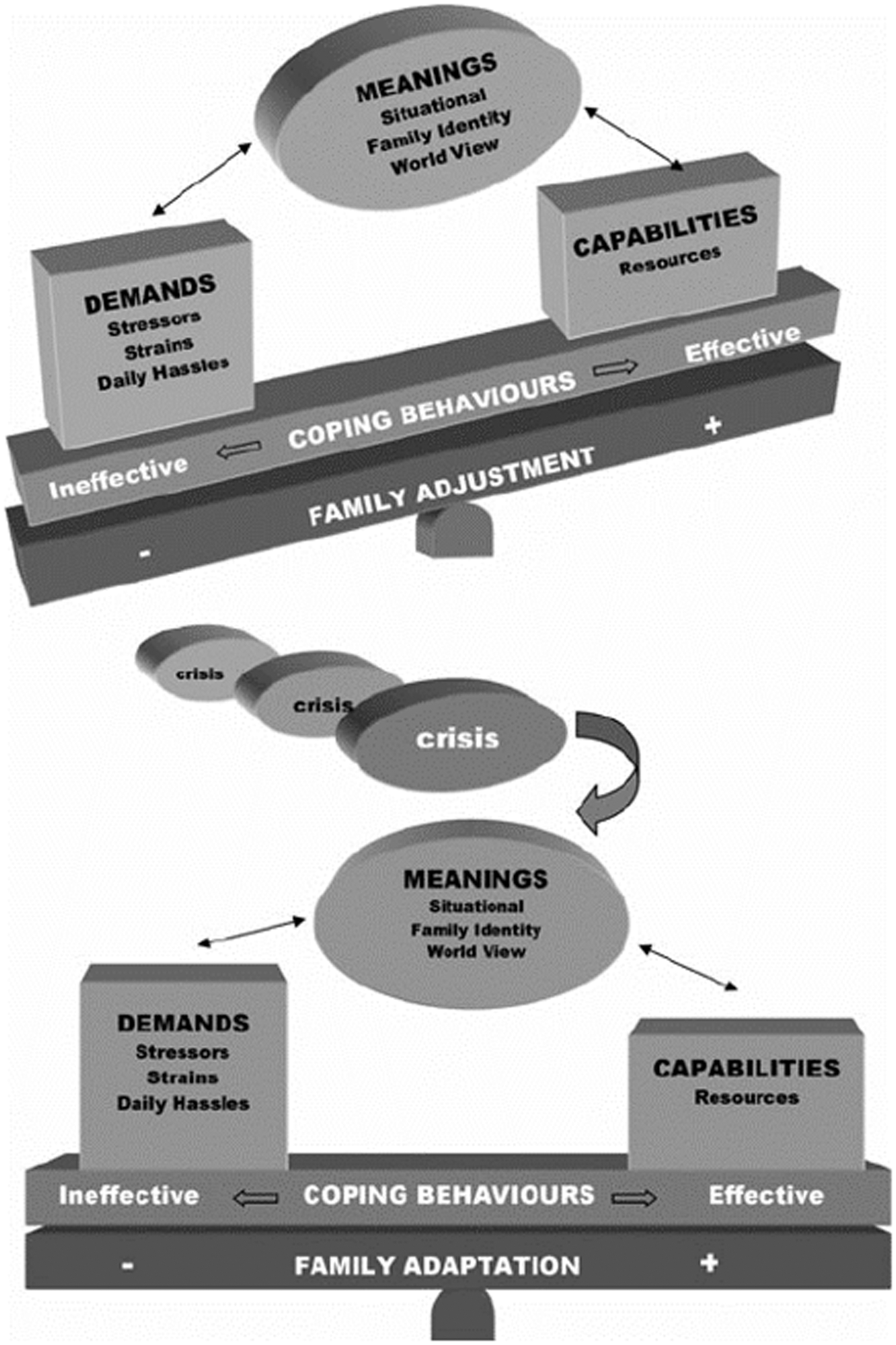
Family Adjustment and Adaptation Response Model (FAAR).
Study participants
Recruitment posters were circulated using the [name of province withheld] FASD Family Network email distribution list. The criteria for participation were to be an adoptive parent and the primary caregiver of a child diagnosed with FASD under the age of 20 years. The eight interviews lasted on average for one hour and 45 minutes and were digitally audio-recorded and transcribed verbatim.
IPA is an appropriate method for studying the phenomenon of a particular lived experience shared by a small homogenous sample (Braun and Clarke, 2013; Smith, Flowers and Larkin, 2009: 50). All the interviewees in this study were women and married to men. The women ranged in age from 45 to 69 years; all had completed high school, three received post-secondary diplomas or certificates and four had university degrees. Five of the eight families also had birth children. All had at least one parent employed and six had annual incomes over CAD$80,000. Three families had multiple children with FASD. Hence, collectively, the eight interviewees had 16 children with FASD diagnoses: nine males and seven females aged between 10 and 25 years. The children had received diagnosis at different ages, ranging from three to 17 years of age. Most had not been formally diagnosed with FASD prior to the adoption placement. Half of the study participants live in rural areas and half in urban centres.
The study received ethics approval from the Joint-Faculty Research Ethics Board at the University of Manitoba. To ensure confidentiality, some non-essential details of stories have been changed and interviewees selected their pseudonyms as well as those of their family members.
Data analysis
Step one of the content analysis included a close examination of each individual transcript. Step two included grouping similar themes from all eight transcripts onto one master spreadsheet. In this step, we identified 25 broad themes with 1555 specifically related quotations. The interpretive element of IPA re-emerged in the third step of analysis as writing began. In this step, the content of each of the 25 broad themes was examined to draw out the essence of the participants’ narratives as a whole. Through this process, new themes and subthemes emerged and a narrative model was developed to illustrate and disaggregate the complexity of the intertwined narratives.
Findings
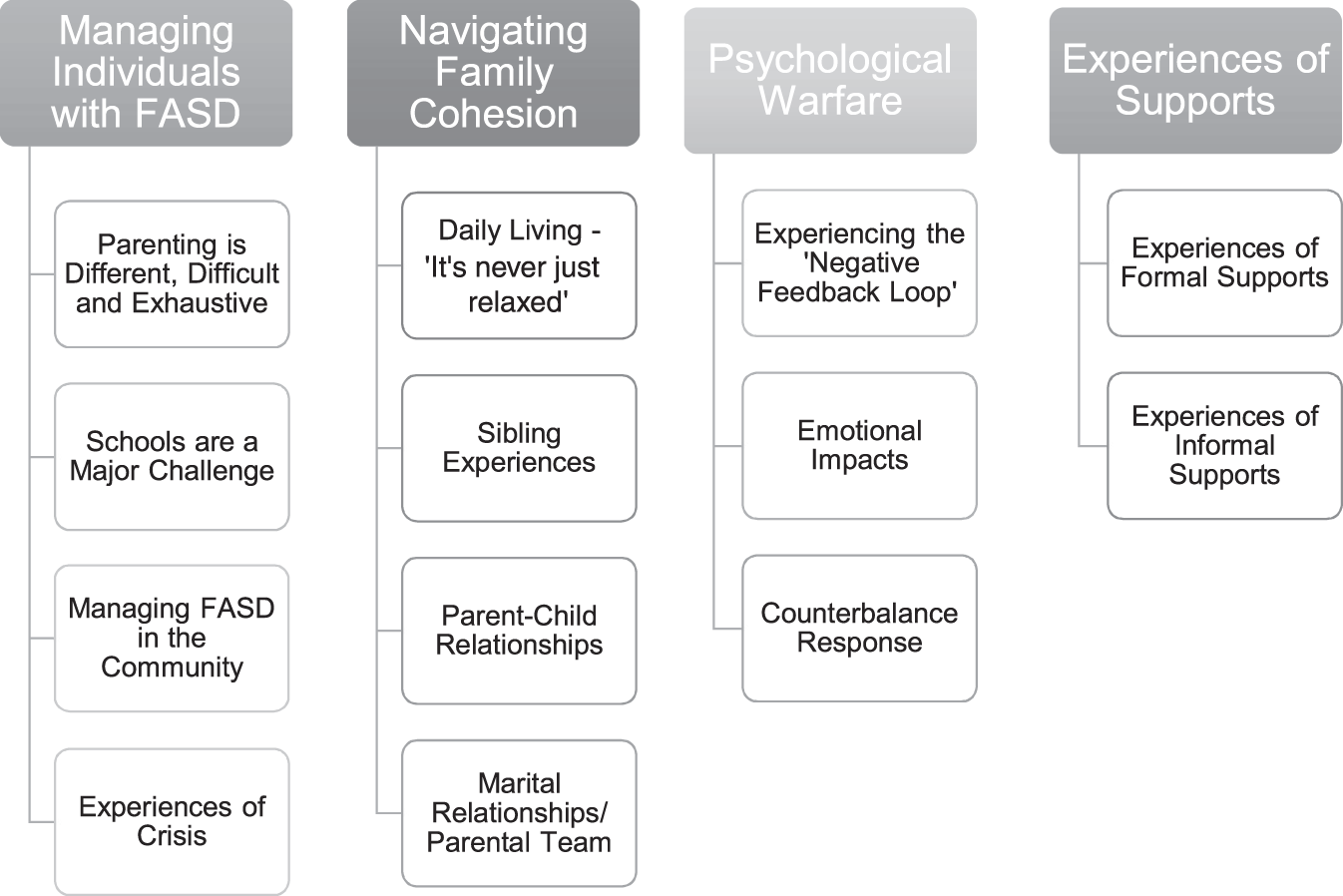
Four main themes, each with subthemes, emerged from the analysis and are visually represented in Figure 2.
Narrative model.
Theme 1: Managing individuals with FASD
This theme is the most directly related to the individual level, namely the tasks associated with parenting, managing schools, coping with crises and the impact of FASD on family interactions with the community.
Parenting is different, difficult and exhausting
Parenting children with FASD is a nuanced experience and study participants spoke of its many different facets. Among these were: obtaining the diagnosis through a long-drawn-out assessment process; parents educating themselves about FASD; the never-ending trial and error interventions because typical parenting strategies do not work; learning how to accommodate and not trigger their children; maintaining their own calm during volatile situations; and co-regulating strategies. They shared how the particular ages of their children were significant and how FASD compounds typical adolescent challenges. Also mentioned were managing multiple diagnoses, functioning as case managers and navigating their children’s peer relationships. Several of them explained how this experience had altered their own life course as parenting demands did not decrease as their child grew older.
Interviewees found the FASD assessment process very taxing. They spoke of years of not knowing, waiting and advocating. All the while, they were trying to manage some very difficult situations with their children without the safety net of a diagnosis. One of the biggest of these was that typical parenting strategies do not work with FASD children. They described a big learning curve with a lot of trial and error to figure out new ways of parenting. Michelle phrased this poignantly as ‘learning to adapt the family’. It is not the child with FASD that adapts, rather it is the rest of the family that adapts to him or her. The family is the accommodation for the child.
Participants also reported that co-regulation is a big part of what they have to do on an ongoing basis in order for their children to function, and that this has to integrate accommodation, parenting, teaching and managing the disability. They shared how it can be both explicit, as in facilitating the tasks of daily living or teaching steps to new skills, or less noticeable as much happens ‘behind the scenes’. Co-regulation takes a great deal of the parents’ time and energy, requires exceptional organisational and management skills, extends over a long period of time – well into adulthood – and can be exhausting and frustrating for parents. In addition, while the child may need all this support, it does not mean they want it or accept it. Parents described how they respond to this opposition by trying to co-regulate using some ‘behind the scenes’ indirect strategies, such as co-ordinating with outside supports, planning ahead, using environmental accommodations and implementing habits of structure. They shared how often their best efforts do not succeed as they often cannot control all the variables, especially during the adolescent years. They mentioned that the characteristics of FASD seem to undermine and sabotage their attempts at positive support, leaving the child with FASD and the family to suffer the consequences.
Schools are a major challenge
School success emerged as a high priority for parents and a marker of overall parenting achievement. However, school experiences were also one of the families’ biggest stressors. With school comes a new set of challenges and triggers for children. Their high levels of vulnerability were also worrisome, especially when they move to middle and high school environments that are not equipped to deal with FASD characteristics or accommodate children’s needs. Participants felt that FASD is a disability that is little understood, and felt that the nature of the current school system seems to set the children up to fail.
Advocacy, educating school personnel, good consistent communication and collaboration between parent and school all require a lot of extra effort from parents. They also explained how a poor school experience can contribute to the ‘negative feedback loop’ and increases their stress levels, and how their hands were somewhat tied when it comes to implementing strategies to support their children in school.
Although a formal diagnosis of FASD is necessary for the schools to obtain supports or allow for accommodations, one mother, Linda, voiced her frustration that FASD is not recognised by schools as a disability that qualifies for supports: ‘even with a diagnosis, it does not mean schools know how to support or accommodate for this diagnosis’.
Managing FASD in the community
Interviewees provided examples of both positive and negative experiences in their local communities, including how the invisible nature of the disability and the associated stigma affect the family. They mentioned issues of social inclusion for both children and parents, and how the community’s response can make a difference to their lives.
Most of the interviewees had children without the physical features of FASD and this invisibility posed some challenges for parents. As Candace explained: Even if you are talking to other people, they really don’t know what you’re facing at home because on the outside it can appear that the girls are fine.
The mothers spoke of their needs for social inclusion as an important part of well-being for both children and families. However, the characteristics of FASD seemed to complicate their ability to engage in the community. Leaving the house increased the probability of triggers as environmental accommodations and routines are critical to children’s stability but are much more difficult to navigate outside of the home. They explained how this resulted in social isolation and exclusion from engagement in extra-curricular activities for both child and parents.
Experiences of crisis
While there is always a certain level of continuous stress and challenge for families, several interviewees also had undergone crisis-level experiences with their children and families. Among these were children’s substance misuse, early pregnancy, abusive partners, placing grandchildren for adoption, multiple rapes, attempted suicide, running away, stealing, assault and having children incarcerated. Three of the eight interviewees mentioned needing to obtain alternative living arrangements for their FASD child as the violence against the parents or siblings escalated to a level that was no longer manageable or safe.
Children with FASD can be extremely vulnerable. In addition to everyday safety concerns, there are also more serious safeguarding issues. Some of the most stressful and overwhelming times occur when the child loses control, is raging and nothing seems to be working. Mothers described this as overwhelming, scary and dangerous. The challenging behaviour ranged from yelling and screaming and throwing and destroying things to outright violence against parents and siblings. Michelle recalled, ‘There was a time when we wouldn’t even leave knives hanging around because she’ll grab the first thing that she’s got and throw it …’ Balancing the needs of all family members was an ongoing concern, especially when it came to escalated behaviours.
Several participants mentioned calling the police or the mobile crisis response team on occasions when things escalated beyond their capacity. They felt that their options were limited when they reach this point. As Ann described: I mean, basically if you have a son like [Jason] who's big enough and out of control enough to be physically frightening to everyone in the family … if you have an abusive spouse you leave them if you're lucky. But if you have an abusive child, there’s really nowhere to turn.
Theme 2: Navigating family cohesion
Family cohesion emerged as the main overall goal of the study participants and one of the most critical markers of family well-being. They shared their overarching philosophies that family success and cohesion mean togetherness, activities, being healthy and happy, having fun together and enjoying reciprocal relationships. Despite this core value, many mothers spoke of how the characteristics of FASD ‘put a wrench’ into their family cohesion.
Daily living – ‘It’s never just relaxed’
While this subtheme was intimately entangled with others, the interviewees perceived never being relaxed as an overall state that they lived with on a continual basis, and which they identified as one of their top challenges. It refers to how family members experience their daily living environment and how the constant nature of certain behaviours – frustration, volatility and ‘never being relaxed’ – affects everyone’s well-being. The mothers mentioned living in a heightened state of arousal; they shared the sentiment that there is always ‘something’ going on with their children and how this constant and frequent concern has a cumulative effect on family well-being.
Along with this underlying tension, participants reported daily frustrating, annoying and impulsive behaviours, frequent flare-ups, rages and meltdowns, regular aggressive outbursts and the daily communication from schools that a problem had arisen. Families had to live with explosive outbursts or shut-down behaviours on a regular basis, ‘leaving everyone to pick up the pieces’ (Marie) both literally (the physical damage of whatever has been thrown) and psychologically (the emotional impacts of living in a volatile environment). Parents mentioned that meltdowns or rages were unpredictable and could be triggered by the simplest of events, and that it was the family who had to bear the brunt of the incident before and after the child’s medications had taken effect.
Participants emphasised the ‘unpredictable predictability’ of their children’s difficulty with adaptation and how living with very impulsive and reactive youngsters complicates the family’s daily functioning, as any deviation from plans, such as uncontrollable variables like wind direction on a walk or a sudden mood change, dictate what a family can or cannot do on any given day.
Sibling experiences
The way that FASD in the family impacts other children’s experiences had important ramifications for family well-being. All of the participants who had other children at home spoke of various difficulties. They shared their experiences and expressed their sadness about how challenging sibling relationships cause friction for the whole family, generating experiences of abuse and living with violence, damages sibling relationships and lands parents with additional parenting tasks of navigating accommodations that respond to everyone’s needs.
Linda’s statement that ‘it’s not fair to the other kids’ speaks to the Catch 22 position in which parents find themselves. Ann was forced to decide that it was no longer safe for her son to live in their home because of safety concerns and the effect that his violence was having on the rest of the children. She referred to this decision as the ‘Sophie’s Choice’ of parenting moments.
In their attempts to survive, parents described how they navigate these situations as best they can through accommodations, coping and survival strategies. They reported needing to simultaneously engage strategies to optimise the functioning of their child with FASD, while at the same time supporting the sibling in ‘being the accommodation’ and teaching them to ‘protect themselves in volatile situations’. Professional counselling services, mediation and physical separation were the main strategies used to respond to the psychological impact of FASD on siblings.
Parent–child relationships
Several interviewees explained that the parent–child relationship had also been affected by FASD, and in many ways. Candace explained that some of its characteristics impeded her ability to have strong relationships with her two daughters with FASD, despite her capacity and desire to foster close relationships. Participants expressed how the pushing away of parental support, continual aggression and violence, attachment trauma and the lack of reciprocity of relationship from their child make doing the things they need to do to be supportive a lot harder.
Nevertheless, despite all these challenges, these adoptive parents seem quite adept in identifying even the most minute cases of positive behaviour. Their ability to identify this reflected their capacity to filter it through a disability lens. The dissonance, therefore, is between the intellectual understanding of the disability-related behaviour and the emotional response to the state of the parent–child relationship.
Marital relationships and the parental team
Interviewees discussed challenges and protective factors related to their marriage and co-parenting. The importance of the integrity of the marital relationship and the necessity of parenting as a team within the FASD context seemed crucial to overall family well-being. Both parents being knowledgeable about FASD strategies and both being able to parent at equivalent levels were considered critical for optimal success as most participants discussed needing to be able to ‘tag off’ when either of them had reached their emotional limit.
While participants acknowledged that different personalities and parenting approaches are normal in a parenting team, several described the challenge presented if their spouse was at a different point in their knowledge journey and in acceptance and understanding of the disability. This created a stress imbalance between the parents which could be serious if a misdirected reaction to the child by one parent set off a chain reaction that served to increase stress in the other parent.
The extensive parenting requirements and the impact of managing FASD in the long-term, combined with the lowered satisfaction with family cohesion, clearly affect marital relationships in significant ways. One common example is the lack of opportunities for parents to spend time together due to difficulty in obtaining specialised childcare; others arise from the extra time and energy needed for high priority issues and altered life courses due to children’s longer dependency on parents. All interviewees spoke about the impact of FASD on their marriages and the challenge and importance of maintaining strong relationships for overall family well-being.
Theme 3: Psychological warfare
The theme ‘psychological warfare’ was coined by a mother who identified it as the hardest part of her experience, a view with which the others generally concurred. This theme is especially pertinent to individual caregivers and includes how the whole FASD experience in the family impacts them emotionally, while at the same time demands that they respond in a way that maintains equilibrium for them personally and for the whole family.
The ‘negative feedback loop’
One mother described something she called ‘the negative feedback loop’ and explained how the contradiction between parents’ positive strategies and the negative feedback from children and society creates a level of self-doubt that poses the biggest challenge, not only to managing the FASD characteristics on a daily basis, but also for maintaining psychological equilibrium for the parent. All participants shared elements of this theme. As Ann commented, ‘The greatest challenge is keeping yourself strong to be able to keep doing the right thing, even when it doesn’t always produce the right results.’
Complaints or reports about their child’s poor behaviour from schools and other parents, children not being invited to birthday parties, involvement with criminal justice and social services and pejorative judgements from family and friends were all reported by participants. The incongruence between parental capacity and failure to achieve positive outcomes is a major challenge to their psyches. As Ann stated: It’s a million experiences like this … things happen that shouldn’t happen [children’s behaviour] … in our society we have such an assumption that good families produce good children. We don’t have a story for where good families produce vulnerable children or vulnerable adults.
Emotional impacts
Interviewees talked at length about the emotional impacts associated with their experiences. In addition to frustration, they mentioned feelings of guilt, helplessness, fear and worry, grief and loss, and debilitating levels of chronic stress.
Guilt emerged in several contexts. There are usually a multitude of difficult parenting decisions when it comes to FASD and parents take the brunt of their psychological impact. These include using ineffective strategies prior to diagnosis, wondering if an earlier diagnosis would have prevented current problems, high anxiety, relinquishing care to Child and Family Services and, as Ann said, ‘a million other situations we are put in that only come from parenting a child with a disability’.
Feelings of helplessness and fear were related to regularly being unable to control someone else’s behaviour. One interviewee described it as a ‘double whammy’, first feeling helpless in that their child is not accepting the support they need, and second being traumatised by the consequences suffered by the child. Participants expressed how their own vulnerability is intrinsically tied to their FASD experience.
The interviewees described numerous grief experiences, including anticipatory grief where they projected their child’s trajectory into the uncertain future without much hope. For example, Linda feared that her child was ‘not going to make it’ and was already experiencing the grief about what their family might experience in the coming years. For many families, this fear and worry starts when the children are relatively young and seems to increase as they get older, as society makes more demands and the children’s capacity for independent living becomes more apparent. When children do not accept parental supports or are not eligible for other community services, parents feel very uncertain about how their children will be successful, or at minimum, be protected from exploitation.
The dominant response from the study participants was that they were experiencing high levels of chronic stress compounded by the feeling that there were no viable solutions. This stress included all aspects of the family experience and ranged from extreme (during times of crisis), to daily and ongoing pressures of managing the characteristics of the disability. Parents agreed that ‘it’s a long road’ and that despite all the accommodations and interventions, acceptance, education and understanding, families still have to live in challenging contexts and ‘deal with’ or cope with the realities described.
Counterbalance response
In their attempts to counteract the impacts of life with FASD, the interviewees revealed certain characteristics about themselves – their coping activities, attitudes, values and beliefs. All spoke of striving for equilibrium and actively prioritising self-care. Several shared how their own personality characteristics served as a protective factor for managing FASD and coping with the level of challenge. The strengths that seemed to benefit their overall well-being were deriving personal rewards, ‘helper’ personalities, positivity, patience, homebody, happy, strong, articulate, and advocacy skills. Maintaining calm in a storm was discussed as a key accommodation in parenting strategies, but also as a means of coping. Open, honest and consistent family communication is one of the key tactics used by families. They stressed that it is important to know how FASD in the family is affecting everyone and to validate everyone’s feelings.
There were connections between formal and informal systems of support and participants’ coping strategies. Parents expressed the need for respite in order to keep parenting successfully; for example, having a mental break or having time to engage in self-care and enjoyable activities.
Several interviewees mentioned that being able to talk with someone who understands the disability in a safe and nurturing environment helps them cope. Most mentioned using formal counselling services and several attended FASD support groups. Peers were also key for coping, as was a sense of humour.
The mothers described taking a positive and ‘one day at a time’ approach and seemed quite adept at picking out when their children were doing well or not, and then focusing on the positives and projecting how those attributes could be optimised in the future. Parents not only celebrated successes but also redefined what they look like to them. For instance, the child just showing up every night at nine, not throwing knives at family members and, once in a while, apologising after an explosive rage were seen as successes. Other participants mentioned being content with their positive efforts rather than any outcomes for their child. So, although acceptance did not change the challenge, it seemed to provide parents with a sense of peace and feeling that they were no longer fighting battles they could not win. It seemed to be heavily connected to experiences of loss and is a process that takes time.
Hope emerged as another critical factor in maintaining the parents’ endurance and motivation to continue. Family resilience became evident through the interviews and some participants recognised how these experiences, despite being characterised by some as ‘walking the path through hell’, had very much contributed to enriching them as people. There was a duality of this experience as parents had to manage the grief for their child’s disability while simultaneously trying to enjoy a ‘normal’ life.
Theme 4: Experiences of supports
The theme of supports encompassed two subthemes covering formal and informal supports.
Experiences of formal supports
Interviewees talked at length about formalised support for both their children and families, whether in education, counselling, daily living, respite, residential treatment and help with navigating the system.
Accessing knowledge about FASD is one of the first such supports sought after diagnosis. Michelle recalled that every bit of information was helpful to her for both immediate needs and anticipatory planning, especially through adolescence and towards early adulthood. All participants engaged in ongoing FASD education, but identified reaching a point when they had enough information and this support became less relevant.
Interviewees also mentioned the value of specialised counselling services. For some, this was very specific to the ‘practical things’ of managing FASD while for others it focused on the grief that results from their specific family experiences. In both cases, having someone who was aware, understanding and knowledgeable about FASD was seen as the most critical factor.
Childcare or respite was another support that all interviewees highlighted as a priority need. It allows time for relationships with other children and spouses, a chance to engage in FASD education and to plan ahead, practice self-care and coping strategies and, sometimes, just to clean the house without interruption. However, formal services did not seem readily available, and did not always fit the family’s needs. Participants shared how some characteristics of FASD make respite necessary but still difficult to come by. No one was currently receiving formal respite services and all reported damage to family relationships as a result of limited resources in this area.
Parents told of using mainstream community organisations for their children’s recreation and leisure needs, but had to advocate and advise those running them to make the provision suitable for their child. They stressed that there was an element of ‘fleeting luck’ in successfully getting what they wanted. For Michelle, writing to her Member of the Legislative Assembly (MLA) opened some doors, and giving Child and Family Services an ultimatum was another strategy that worked. They all shared their frustration with navigating the system of formal supports and overcoming barriers and meeting thresholds, for instance not satisfying the eligibility criteria of being ‘disabled enough’, not knowing what supports are available and their time and locations, services not fitting with work schedules, being bounced around the system, having to pay for psychological services and having no one to turn to during times of crisis.
While families’ experiences of formal supports are undoubtedly a source of help, unfortunately they are also a source of additional stress.
Experiences of informal supports
The value of informal supports of family, friends, teachers, neighbours and peers emerged as a prominent theme and these could be both psychological and instrumental. Several interviewees spoke of the contributions made by their extended families and reflected how ‘lucky’ they were to have such help. Having relatives who accepted their child as a person proved especially important. Aside from psychological supports, extended families also provided practical help like respite, although this was not always consistent and tended to decrease as children grew older. Having friends who understand the realities and unpredictability of FASD was also seen as important as it aids the social inclusion of the family and enhances the mental well-being of parents. Similarly, connection with others who were experiencing similar types of challenges in their families proved important for their well-being. This can involve giving as well as receiving, as Michelle explained when she described how being supportive to peers contributes to her own well-being and Lynn talked about how her advocacy work was helpful to her as well as others.
Interviewees made clear a connection between economic resources, supports and accommodation capacity. Family income affected the provision that families could make in relation to their home environment and paying for things like babysitters, recreation activities and psychological supports. Homes were often damaged by children’s outbursts and their extended period of development meant extra costs for things like five years of level one swimming or 10 weeks of specialised summer programming. In Ann’s words, ‘It’s outrageous what this can cost.’ Only one interviewee received any kind of economic support.
Several mothers stated how there is still a long way to go regarding FASD awareness and understanding among the general population. Candace summed this up when she said that she felt that no one really knows what it is like to parent a child with FASD. Parents shared feelings of being judged and/or of not feeling validated for the challenge and efforts being put into their parenting.
All participants agreed that a supportive and understanding community has many benefits for the whole family and is critical for overall well-being. They mentioned that community understanding and acceptance ‘opens doors for them’ and has the potential to create supports for both their children and their families. Participants identified ‘community champions’ in schools, recreation services, churches, employment offices and the police as especially significant. They concluded that it contributes to everyone’s well-being when a community embraces their children, sees their positives and adapts in ways that help the child feel and become successful so that they can contribute their unique gifts and skills.
Discussion
This study has explored adoptive parents’ experiences of having a child with FASD in their family and how those experiences impact family well-being. The findings suggest that maintaining family well-being within this context is extremely challenging and study participants were universally steadfast in their position that FASD affects the whole family in significant ways. The constant and cumulative nature of the effects of the disability challenges families, resulting in high levels of chronic stress. They have to make adaptations and accommodations over the years as they strive for well-being. The interviewees emphasised that demands outweigh even the highest levels of capabilities, making external supports necessary to help maintain well-being.
The Family Adjustment and Adaptation Response (FAAR) model intersects family stress theory with resiliency theory, postulating that ‘families engage in active processes to balance family demands with family capabilities as these interact with family meaning to arrive at a level of family adjustment or adaptation’ (Patterson, 2002: 350). This is reflected in our findings, which show the many demands and capabilities of families, as well as the adaptations and accommodations they make in attempts to gain family equilibrium.
The model proposes that families restore some balance by either enhancing their capacity, decreasing their challenges and/or by shifting values and beliefs. Within the current state of the FASD context, equilibrium at a level that would be defined as high-quality family well-being may not be possible.
Research on family well-being within the FASD context is limited. One study exploring caregiver needs and stress surveyed parents about their well-being and found that participants have ‘many well-being concerns’ (Bobbitt, et al., 2016: 110). Another found that participants have lower than average subjective well-being scores (Shenaar-Golan, 2017) and Mohamed and colleagues (2020) reported clinically significant levels of chronic stress among families with FASD. However, these findings have to be viewed in the light of Bobbitt and colleagues’ (2016) interesting finding that there were more significant overall well-being concerns reported by adoptive and biological families, compared to foster families.
Several factors hold particular weight relative to balancing well-being within the FASD context. The constant and cumulative nature of the condition has an impact on the well-being of the family. The exhaustive challenging nature of family life that results is reported in the literature (Green, et al., 2014; Michaud and Temple, 2013; Sanders and Buck, 2010), with more specific enquiries showing higher level of challenges resulting from certain FASD characteristics, namely externalising/disruptive behaviours, cognitive and social/maladjustment issues and challenges with adaptive and executive functioning. Our findings corroborate those studies as interviewees referred to living in environments of constant tension. They also suggest that families with FASD have an adjusted scale for well-being with a much lower baseline.
The meanings that families attribute to demands and capabilities is an important construct of the FAAR model and ‘shape the nature and extent of risk, as well as the protective capacity of a family’ (Patterson, 2002: 351). Petrenko, Pandolfino and Roddenbery (2016) looked at how attributions that parents ascribed for misbehaviour of children with FASD influenced both their parenting strategies and levels of confidence or frustration. The authors suggest a correlation between participants’ FASD knowledge and neurodevelopmental attributions that resulted in more antecedent parenting strategies being used, as well as higher levels of parent confidence and greater success in managing behaviours. Our study similarly shows that parents’ capacity to feel sincere empathy for their child’s experience and their ability to dissect and focus on even the smallest positives influence families’ well-being in positive ways.
The FAAR model also postulates that adjustments are ongoing as families attempt to balance their daily demands against their existing capabilities. When those demands significantly exceed capabilities, periods of crisis can result, leaving families in disequilibrium. The parents in our study have been adapting and accommodating for a long time. Accommodations are extensive, and one of the significant features of the FASD experience is that adapting the family is the primary accommodation.
The negative feedback loop emerged as an interesting component. Society has high expectations of parents and makes judgements when things go off track. Societal blaming of parents when children experience adverse outcomes is detrimental to parents’ well-being. The negative feedback loop feeds self-doubt and challenges parents’ competence. One study reports higher levels of stress associated with feeling blamed and suggests that the unique needs of children with FASD compromise parents’ perceived ability to parent successfully, amplifying that stress further (Mukherjee, et al., 2013). The invisible nature and societal stigmatisation of FASD compounds this experience. As the FAAR model suggests, several parents shifted their views and beliefs as they readjusted their family structures. This drive for success was evident in how they changed their definitions of success. Despite negative feedback, parents redefined what it meant to be successful as a parent and were generally content with their efforts even though they did not always achieve optimal results. These findings align with literature that indicates higher stress levels being more associated with child-specific characteristics rather than parents’ own perceived capacity (Mohamed, et al., 2020).
Lack of knowledge at the community level, challenging and stressful school situations and the power of community to make a difference all emerged as having potential effects on family well-being. Interviewees found that there were high levels of advocacy work required to access supports. This is echoed in the literature. School emerged as a priority marker not only of individual but also of family success. However, it also acted as a source of high levels of chronic stress for families.
Worry for the future was prominent among the families studied. The counterbalance to this seems to be hope. Several elements of our findings revealed hope, among them accessing necessary supports, living in an accepting community, witnessing examples of positive outcomes, supportive peer relationships and projecting positive futures. As Shenaar-Golan (2017: 312) argues, ‘hope positively correlates and is a predictive factor of subjective well-being’.
Limitations of the study
Among the study limitations was that the research was restricted to eight adoptive families of children with FASD from similar socio-economic status. Also, the participants were all married women. As such, the findings are limited to one perspective within the family. More complete demographic and contextual information about the children in the sample was not included due to concerns about maintaining anonymity. This, too, could be a weakness as higher levels of family stress have been correlated to certain features of FASD, namely difficulty with executive function, as well as to characteristics of the adoptive carers (Mohamed, et al., 2020).
Recommendations and conclusions
This study contributes to the growing body of FASD research with findings that support recommendations for service delivery for this unique population. The general message from the mothers who had adopted children with FASD is that ‘it could be way better’. In part, this is an expression of how they recognise that they are not reaping the rewards of higher family well-being that typically align with the level of effort and family capacity they possess. It also recognises that additional external supports are critical to achieve and maintain optimal levels of family well-being in these contexts.
High-quality caregiving and home environments are indicated as the critical protective factors and most effective interventions to achieve positive outcomes for individuals with FASD. But this study shows how the whole family is impacted by the condition in significant ways and so contributes to a greater understanding of how to support caregiving and optimise family environments. A family-centred approach to care and intervention is recommended, with a focus on alleviating the collateral impacts on families and reducing caregiver stress.
While the participating families built a lot of endurance, stamina and resilience in order to function at full capacity, their efforts were often outweighed by the demands brought on by FASD characteristics that created disequilibrium for the family. Even in ideal domestic circumstances, families remain vulnerable. External supports in the community are highlighted as an effective way of helping families maintain balance but there are major gaps in the necessary services. Continued efforts are needed to educate and sensitise community partners to the valuable role they can play in supporting the well-being of families with FASD. But as this and other studies conclude, no single input – whether from parents, relatives, community resources or professional services – is sufficient to meet the complex needs of families with FASD over the child’s whole lifespan. A tailored, multi-disciplinary and multi-sectoral approach to supports and interventions is the only option.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.