
Abstract
Studies of adult outcomes of infant domestic adoptions are considered: the range of psychological and behavioural outcomes recorded, the current state of knowledge summarised and the importance of the chosen comparison groups discussed. The social context of infant adoptions is described. Findings from our follow-ups of British infant adoptions in the post-World War 11 period are then briefly reported and set alongside the previous studies. In these follow-ups, infant adopted children were tracked up to mid-life and compared with others born in similar circumstances and with those raised in two-parent families. We summarise findings on the long-term influence of factors in the prenatal period and in the adoptive home environment. We discuss how rearing in adoptive homes may provide protective effects in relation to internalising problems, but may not be as protective in relation to externalising outcomes. Implications for adoption policy and practice are drawn out.
Introduction
When children are transferred very early in life to an unrelated adoptive family, it is of considerable interest to discover whether their lives turn out differently from those of other children and, importantly, why this may be so. This selective review highlights the most relevant and rigorous studies in attempting to answer this broad question. Numerous follow-ups of adopted samples have now been undertaken, but the heterogeneity of the samples involved and the range of circumstances of the adoptions complicate the interpretation of results. The review begins by outlining current findings in follow-ups of mixed adoptive samples, and then focuses specifically on outcomes for children placed in adoptive homes early in life, without known post-natal adversity, and followed-up to adolescence and adulthood.
Behle and Pinquart (2016) undertook a meta-analysis of mental health outcomes in 85 follow-up studies, including international and national adoptees, and samples varying in age at adoption, age at follow-up and the extent of any pre-adoption exposure to abuse and/or neglect. The risk of psychiatric disorder was roughly twice as high among adopted people compared with non-adopted comparison groups. Outcomes were poorer among those who were internationally rather than domestically adopted, and among those placed later, but it was not possible to quantify the impact of pre-adoption adversities. A review of adult outcomes restricted to domestic adoptions (Melero and Sánchez-Sandoval, 2017) concluded that the psychological adjustment of adopted samples was less favourable than that of the comparison groups on indicators of depression, anxiety, personality problems and behavioural disorders, but there were few pointers as to the key drivers of these increased risks.
Against this background we turn now to examine findings from specifically infant domestic adoption follow-ups. The studies we review here reduce heterogeneity by focusing on samples of children placed early in development, in their country of birth and without known post-natal adversity. These adopted individuals may still, of course, be exposed to pre-natal vulnerabilities and may need to deal with the particular ‘psychological tasks’ (Brodzinsky, 1987) theorised to face all adopted individuals (for example, dealing with dual family membership, achieving a secure personal identity and coping with a sense of difference).
Even within these more homogeneous samples, conclusions may vary depending on the nature of the comparison groups investigators choose. Employing a comparison group drawn from a general population that contains many deprived families (as in very unequal societies) may tend to favour adopted groups. But if the comparison group contains more advantaged families (as in more equal and affluent societies), greater differences may be apparent – and a similar pattern may also be found if outcomes for adopted individuals are compared with those of the biological children of their adoptive parents. Some studies have been able to constitute comparison groups of individuals who are genetically related to adopted individuals (as in separated sibling studies). This type of design, which ‘controls for’ genetic factors that may affect later outcomes, provides a strong basis for assessing the effects of different rearing environments; and a related logic underlies studies with comparison groups of individuals who, although not biologically related to adopted sample members, were nonetheless born into broadly similar circumstances. As these examples suggest, assessments of how well (or poorly) adopted individuals have fared may depend considerably on the nature of the groups with whom they are compared.
In a follow-up to adolescence, Keyes and colleagues (2008) found that most adopted individuals were psychologically healthy, but at increased risk of some externalising disorders by comparison with a general population sample. At an older age of follow-up (30–40 years) Loehlin, Horn and Ernst (2007) found slightly less favourable outcomes when the comparison was with biological offspring from the same families: adopted individuals rated themselves as having more anxiety and depression, and more trouble with the law, but effect sizes were generally small and the majority of adopted people were well adjusted.
Several reports have explored influences on adoption outcomes using Swedish National Registers. Kendler and colleagues (2016) identified children from birth families with known high risk factors where at least one sibling was adopted away as an infant and the other raised by the birth family. The risk of criminal conviction was substantially lower in those adopted away (26%) than the home-reared group (41%), suggesting that adoptive environments can protect against risks of criminality. Kendler and colleagues (2015), in a follow-up of samples to late adolescence, found that the adoptive rearing environment contributed to an IQ score advantage over the non-adopted group. Part of the difference was explained by the educational level of the adoptive parents. Furthermore, Kendler, et al. (2012) reported that risk for drug addiction in adopted children is increased by death or divorce in the adoptive parents, but also by a disturbed adoptive home environment, parental alcoholism and sibling drug misuse. These studies indicate that the adoptive family environment, like any family setting, can clearly have both beneficial and negative effects, and these may be amplified in the context of genetic vulnerabilities.
In follow-ups of an unselected birth cohort to adolescence, Fergusson, Lynskey and Horwood (1995) found no increased risk of internalising disorders (depression, anxiety) among individuals adopted in infancy, but that rates of externalising disorders (conduct problems in childhood, anti-social problems in adulthood), self-reported juvenile offending and substance use were higher than in a two biological parent comparison group (though somewhat lower than among other children who entered single-parent families at birth).
The Early Growth and Development study, initiated at the University of Oregon, is an ongoing prospective follow-up study of adopted samples and is relatively rare in having genetic, pre- and post-natal data which will help in the process of understanding the combined and separate effects of ‘nature and nurture’. However, the studies focus more on parenting influences than comparisons with non-adopted general population outcomes and the findings so far have mostly related to childhood and early adolescence (Leve, et al., 2019).
Summary of infant adoption outcomes
These studies of infant adoption have painted a generally positive picture of later outcomes, although with indications of difficulties in some areas. Interestingly, where studies of more mixed adopted samples (many of whom will have faced pre-adoption adversities in their birth families) have highlighted increased risks of anxiety, depression and other mental health problems, follow-ups of infant-adopted samples seem more likely to identify difficulties in the ‘externalising’ domain (e.g. hyperactivity, delinquent behaviour, conduct and attention problems), whereas the ‘internalising’ spectrum includes a variety of over-inhibited or internally-focused symptoms including anxiety, fear, sadness/depression, social withdrawal and somatic complaints. Separated sibling studies in particular point to some of the aspects of the rearing environment that may be both beneficial and challenging. It has been less usual so far for adoption studies to have access to the genetic and pre-natal data which may also contribute to explanations of outcome.
The British birth cohorts
We were pleased to be able to add to this literature by capitalising on data collected in two of the British birth cohort studies, in order to explore long-term consequences of infant adoption. These unique and continuing studies form part of what Helen Pearson refers to as The Life Project (2016), in which she describes the numerous findings of the various projects and their special value for investigating how early childhood experiences affect the life course (https://cls.ucl.ac.uk/cls-studies/1958-national-child-development-study).
Two of these studies – the 1958 and 1970 birth cohorts – were initiated at periods when infant adoption was relatively common in Britain (see below). As a result, both cohorts included small numbers of children who were born to unmarried mothers and subsequently placed for adoption. Most adoption research has gathered information only after the adoptive placement, and samples have mostly been followed only to adolescence and early adulthood. A great advantage of the cohort study databases is the availability of detailed information collected at the time of the birth, and regular prospective follow-ups until the cohort members were aged about 40 to 50. Beyond being able to examine outcomes over time in many domains, we were thus able to explore possible pre-natal and later family environmental influences on long-term development.
Social and policy context
The social and legal context of adoption will differ in location and in time. It may be helpful to outline the circumstances of the adoptions in the two cohorts (1958 and 1970) which we will be highlighting here. Although adoption as an informal practice has a long history, in Britain, it was formalised in the 1920s (Adoption of Children Act, 1926; Adoption of Children (Scotland) Act 1930), then further regulated in the 1930s and 1940s (Keating, 2009). Figure 1 indicates the numbers of domestic adoption orders granted in England and Wales between the late 1920s and 2012. As it shows, these grew steadily across the 1930s, then increased much more rapidly during the Second World War, reaching a peak in 1946. The post-war years saw some reduction in numbers, followed by a further sharp rise in the 1960s, to a peak of almost 25,000 in 1968. Thereafter, numbers declined equally sharply across the 1970s and 80s, before stabilising at around 5000 per year in the 2000s.
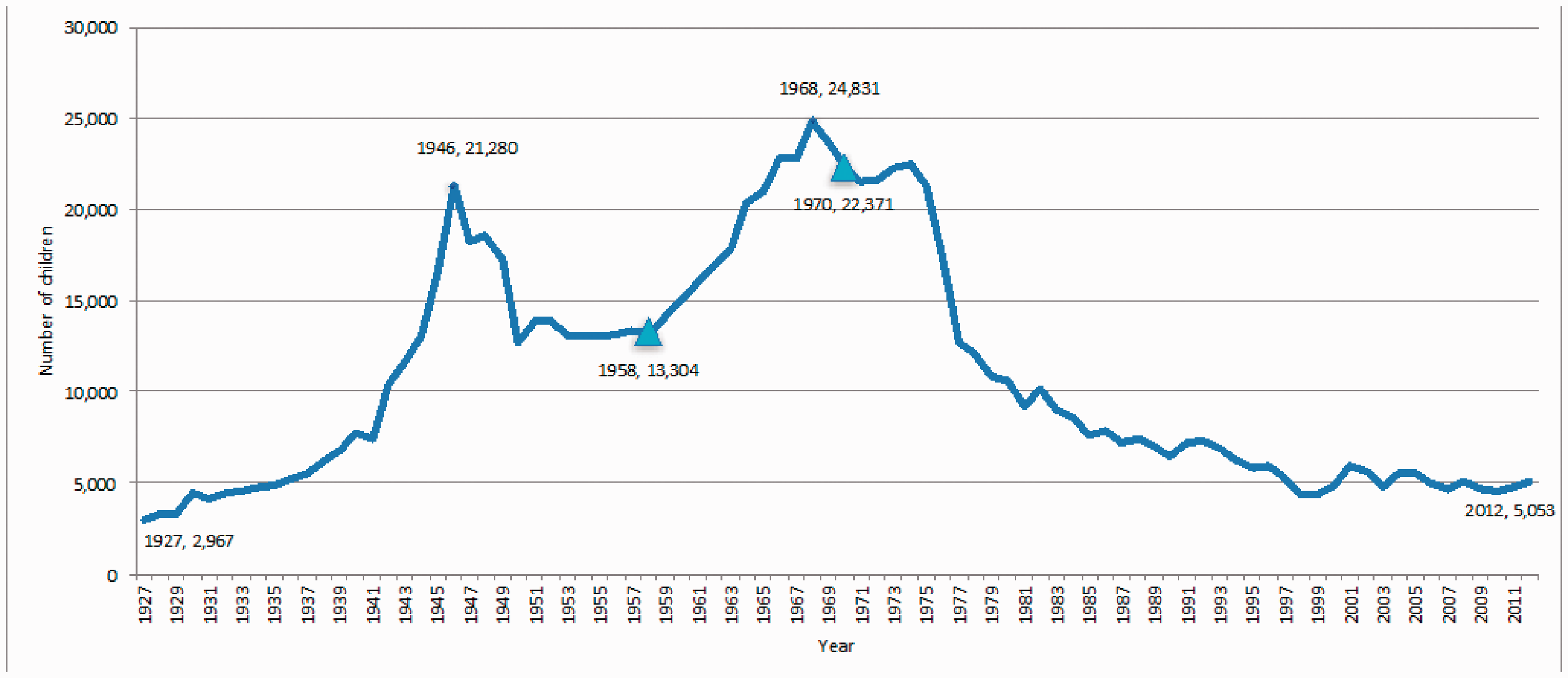
Domestic adoption 1927–2012 (England and Wales).
The total numbers of children adopted in England and Wales in our two study years (1958 and 1970) were 13,304 and 22,373 respectively (ONS, 2013a). However, these figures do not distinguish between adoptions from care and other arrangements such as step-parent adoptions (ONS, 2013b). In 1968, for example, when adoptions were at a peak of 24,831 (ONS, 2013a), adoptions from care numbered 16,164 (Howe, Sawbridge and Hinings, 1992). As Figure 1 illustrates, the 1958 and 1970 birth cohort studies were initiated in the era when domestic adoption was still relatively common, and pre-dated the substantial drop in the number of adoptions that occurred from the 1970s onwards (Triseliotis, Shireman and Hundleby, 1997).
The babies in our study cohorts were born mostly to young unmarried mothers who relinquished their babies for adoption (rather than, as in many more recent studies of infant adoption placements, babies being removed due to safeguarding concerns), and the infants were then placed shortly afterwards with the new families. Unmarried motherhood was relatively rare at this period; only 4% of mothers in the 1958 birth cohort study had their babies out of wedlock, and this figure had only risen to around 6% by 1970. Although the babies were relinquished for adoption, the circumstances and weighing of alternatives prior to this decision will doubtless have been complex and fraught for many. At the time there was no assisted conception and so the only choice for child-free couples wanting a family was by adoption. The criteria for recruitment and selection were narrower than in more recent years, meaning that adoptive families would have been more advantaged in terms of material circumstances, home ownership and educational level.
Compared to the periods before and after the births of our two cohorts, there were few major policy changes in adoption between 1958 and 1970. Although debates about more ‘open’ adoptions and potential for contact with birth family members took place in the late 1960s, these were yet to be enacted in policy-making, and both cohorts were adopted before the next set of major changes to adoption practice in the 1970s (via the Children Act 1975, Adoption Act 1976 and Adoption (Scotland) Act 1978).
Nevertheless, broader policy and cultural changes between the two cohorts are likely to have influenced the circumstances of birth parents, assessments of adopters and attitudes towards adoption. In 1958, social housing was limited and often of poor quality. Means-tested benefits were available to unmarried mothers but were largely seen as stigmatising, and access criteria were strict (Thane, 2011). Under the Labour Government of the 1960s, higher spending occurred on social security and health, and the increased building of both social and private housing, as well as protection of tenants’ rights (ONS, 2013c). Although IVF was not yet available, changes in family planning included greater access to contraception. The Abortion Act 1967 also legalised abortion on a wider variety of grounds across England, Wales and Scotland. Alongside these developments, attitudes towards women, single parents and adoption were also changing.
Birth parents’ perspectives were largely absent from research and policy at that time. The attitude of the birth mother’s own parents and the circumstances of the birth father, among other factors, may have influenced the decision about whether to keep or relinquish their child (Yelloly, 1965). In working-class families, fewer financial resources may have been offset by a greater willingness to absorb a child into the wider family network (Thane, 2011). Birth mothers who wanted to keep their children faced considerable social stigma: an example of ‘moral luck’, where although other young people were also sexually active outside marriage, those women who became pregnant were viewed as ‘deviant’ (Howe, Sawbridge and Hinings, 1992). Attitudes towards birth mothers have fluctuated over time rather than developed in one direction: ‘at all times, sympathy and condemnation have co-existed and conflicted in shifting measures’ (Thane, 2011: 12). Although policy and practice have changed since our two cohorts of children were placed, debates continue about the rights of birth parents and support for those who lose their children to adoption (Gupta and Featherstone, 2019).
Follow-up of infant adoptions identified via the British birth cohorts
Several earlier reports have documented child and early adult outcomes for adopted infants in one of the samples we will be reporting on here: the 1958 British birth cohort (Lambert and Streather, 1980; Seglow, Kellmer Pringle and Wedge, 1972). In an early adult follow-up, the adopted women showed few difficulties, but there were indications of increased problem levels among the men, in some instances associated with a more persistent pattern of behaviour problems extending from childhood (Maughan and Pickles, 1990). At age 33, adopted women’s social and emotional adjustment was again positive, but outcomes for men showed difficulties in specific domains including increased risks of unemployment and more restricted levels of social support (Collishaw, Maughan and Pickles, 1998).
Mid-life follow-up: aim and methods
In our mid-life follow-up of infant domestic adoption samples we set out to provide evidence on mental health, well-being, life satisfaction and externalising outcomes in 40- to 50-year follow-ups of infant-adopted samples. We compared outcomes for the adopted samples with those of two other groups: (i) the large majority of cohort members raised in two biological parent families, and (ii) other children who, like the adopted children, were born to single mothers but who remained with them and in their families of origin. (We call them ‘birth comparisons’ as they shared characteristics with those who were subsequently adopted.) Where group differences are identified, we explored both pre- and post-natal factors that may have contributed to these effects. Readers are referred to the full report of the samples, methods, measures, ways of dealing with data loss and analysis of results in our recently published article (Sehmi, et al., 2020). This current article presents a concise description of the study in order to allow for a fuller discussion of the implications of the findings.
Samples
The 1958 British birth cohort has followed the lives of 17,416 babies born in one week in 1958 (Power and Elliott, 2006). Similarly, the 1970 British Cohort Study (BCS70) has followed the lives of 16,569 babies born in one week in 1970 (Elliott and Shepherd, 2006). All were born in England, Scotland or Wales. Further details on the British birth cohort studies are available from the Centre for Longitudinal Studies, University College London (www.ucl.ac.uk/ioe/departments-and-centres/centres/centre-longitudinal-studies), and the data-sets for the 1958 and 1970 cohorts can be accessed from the UK Data Archive.
Both cohorts have been studied on repeated occasions since birth; in the 1958 cohort the oldest age at follow-up at the time of our analyses was 55 years. The adoption group (n = 180) within the cohort consisted of children born to unmarried mothers and placed predominately with non-relatives. The great majority were infant adoptions (49% placed within six weeks of birth, 77% during the first three months and only 8% after 12 months of age). The comparison groups comprised other children born to unmarried mothers but who remained with their biological parent(s) (n = 363); and a general population sample including all remaining cohort members (i.e. those born to married parents) (n = 14,361). The rationale for including the birth comparison group was to make it possible to investigate biological and other influences on development.
In the 1970 cohort the oldest age at follow-up was 42 years. Of the adoption group (n = 166), 56% were placed at or before six weeks, 83% by 12 weeks and 17% at slightly older ages, the latest at 15 months. As in the 1958 cohort, other babies born to unmarried mothers but who remained with their biological parent(s) formed one comparison group (n = 613), and the remainder of the cohort, born to married parents, made up the general population sample (n = 14,148). Fifty-six percent of the adopted children were male in the 1958 cohort, 51% in the 1970 cohort. Minority ethnic children were rare in both these samples.
Inevitably, over the long span of these studies, each follow-up had missing data, which reduced the sample size and could potentially influence the study results (for example, because participants cannot be traced, decline to co-operate or do not respond to individual questions). Inverse probability weights were used in all analyses to take some account of selective attrition.
Measures
The following is a brief listing of the main items and measures used in the follow-ups over time. At the birth sweeps, the studies recorded birth weight, teenage motherhood (under 20 at birth), mothers’ smoking during pregnancy (more than 15 cigarettes a day), the timing and number of ante-natal visits and the mother’s marital status. Later in childhood (when the adopted children were in their adoptive homes), family, social class and home ownership were recorded as well as parental involvement and teachers’ reports on the parents’ interest in the child’s education. Child and adolescent internalising and externalising problems were rated by parents on the Rutter A2 Scale (Rutter, Tizard and Whitmore, 1970). In adulthood, participants reported on consultations with a doctor or specialist about mental health problems in the last year. Psychological distress was assessed by the Malaise Inventory (Rutter, Tizard and Whitmore, 1970) and well-being by the Warwick-Edinburgh Mental Well-being Scale (Tennant, et al., 2007). Participants also rated their life satisfaction, physical health and activity levels. Anti-social problems recorded in adulthood included high-frequency smoking, alcohol and substance misuse. Criminality in adulthood was indicated if participants said they had been found guilty in a criminal court since the previous study contact; for the 1970 cohort this covered ages 16–30, and for the 1958 cohort ages 23–33.
Results
Below we present a brief summary of the results.
Pregnancy. In both 1958 and 1970 cohorts, the adopted group and the birth comparisons were much more likely to be born to a mother aged under 20 in comparison with the general population. These two groups of mothers were also more likely to have smoked during pregnancy, to have attended fewer ante-natal visits, to have attended their first visits later in the pregnancy and to have had babies of lower birth weight.
Childhood circumstances. Although the children placed for adoption and the birth comparison group had similar pre-natal experiences, their childhood material, educational and social environments diverged. Living in a two-parent family, in a non-manual social class home, owning a home and having a father who was educated beyond compulsory age were much more likely to be the case for the adopted than the birth comparison group – and indeed more so than in the general population. Home circumstances across a range of indicators were clearly more advantaged for the adopted children.
Problem levels in childhood. Internalising problems in childhood and adolescence were equivalent in all three groups, but they were more problematic for the birth comparisons in the 1970 cohort when aged 10. Externalising problems were greater than in the general population in adolescence in both adopted and birth comparison groups (1958). This might suggest problems of similar origin. However, this difference was not repeated in the adopted group in the later cohort (1970).
Mental health problems in adulthood. A central question was whether the mental health of the adopted group differed from that of the comparison groups. Malaise Inventory questionnaire scores for the adopted group were equivalent to the general population, but higher problem scores were recorded for the birth comparisons (mainly due to higher scores for the birth comparison group women). Differences appeared to be associated with more positive material circumstances and greater levels of parental involvement in adoptive families. In the 1970 follow-up group differences were less marked: at age 30, comparisons with the general population were not significantly different and at age 42, the birth comparison group had somewhat higher scores than the general population. It may have been less stressful to be raised by a birth parent over a decade later due to changed attitudes and better provisions for single mothers (see Thane, 2011, on unmarried motherhood). Help-seeking for mental health problems was no greater among adopted individuals than for the general population, but more common for the birth cohort in the 1958 sample.
Well-being. In terms of positive mental health, self-ratings of well-being and life satisfaction for the adopted group were similar to those of the general population, but rated lower by the birth comparison group in both cohorts. These assessments did not therefore show the increased vulnerabilities reported in follow-ups of adoption samples containing more adverse early experiences.
Anti-social behaviour. A somewhat different pattern emerged in the behavioural domain. Poorer outcomes were evident in terms of anti-social behaviour, smoking and alcohol problems, for both the adopted and the birth comparison group, compared with the general population. In both cohorts, rates of self-reported convictions were higher in both the adopted and the birth comparison groups than in the general population, and the adopted and birth comparison groups did not differ significantly. Rates of criminality were, as expected, much higher for men than for women.
Links with poorer outcomes. To explore possible predictors of poorer externalising outcomes, we constructed a combined adult externalising scale (1958 cohort only) based on any adult convictions, mid-life smoking and problem drinking. Both the birth comparison group and the adopted sample had higher scores on this scale than the general population sample. Three pre-natal adversities (biological mother’s age, maternal smoking in pregnancy and limited ante-natal visits) were found to be independently associated with this adult externalising scale. By including these factors in the analysis we found that almost a third of the differences between the adopted and general population samples could be attributed to maternal age and maternal smoking in pregnancy (both known to be associated with increased risks for anti-social outcomes, see Murray, et al., 2010) and limited ante-natal care – likely to be an index not only of poor detection of risks to the pregnancy, but also of pregnancy stress. Other associated factors in pregnancy and inherited characteristics from both biological parents may also have made a contribution to the externalising outcomes.
Comparing these results with previous infant adoption long-term outcome studies
Some difficulties present themselves in setting our findings alongside previous studies, based as they were in various countries and at different historical periods. Sample sizes differed and age at follow-up ranged from about age 16 to age 40. Our samples were assessed later: on average in their 40s and 50s. In addition, while most prior studies (like ours) were based on representative samples, some were different in that the birth parents were selected for known high risk.
Our findings are in agreement that most adoptive participants were psychologically healthy, although each study contained a proportion with less favourable outcomes. Those mixed samples commented on earlier, where many of the children had adverse early lives, were at risk of more serious psychiatric outcomes, whereas this proved not to be the case in our study. None of the previous studies were able to assess the influence of any specific factors on the pre-natal period or the adoptive environment.
Strengths and limitations
As far as we are aware, this is the first study to follow unselected homogenous infant adoption samples across the lifespan up to mid-life. It was based on large national longitudinal data sets, which have enabled us to examine life patterns based on standard measures at regular intervals over a long period of time. We have explored, within the data that were available, some potential influences on later outcomes. The ability to consider the contribution of pre-natal factors in adoption research is fairly rare.
It is important to recognise the nature of this study and the questions it is able, and not able, to address. The data drawn on were not designed primarily with the adoption experience over time as the focus. Adoption research and theorising has frequently focused on putative psychological and environmental stresses peculiar to adoption. However, information on the psychology of adoption was not available here: for example, the studies do not tell us about such factors as the relationship between adopters and adopted people over time; the quality of intimate relationships in adulthood; nor issues of adoptive identity, possible sense of abandonment and difference; nor knowledge of and contact with the birth family and adoptive family over the life-span. None of these questions formed part of the content of the interviews and questionnaires in the large population-based cohorts. No genetic information was available on the birth parents and so the influence of factors inherited from the birth family is unknown, although there is likely to be a complex interaction of inherited and environmental influences. The possibility of examining the long-term effects of alcohol use during pregnancy, even at modest levels, could not be examined as those questions were not asked at the time.
As indicated in the introduction, the character of infant adoption in the post-WWII period is very different from the current population of older, ex-care, often neglected or maltreated children now placed for adoption in Britain. Our samples are almost entirely Caucasian. Major changes have taken place in adoption legislation and practice over time, and also in advances in developmental psychopathology. However, it would not be sensible to disregard these findings as of only historical interest. It is important to recognise that there are many essential and continuing similarities: adoption by non-relatives continues to involve parents raising a child as their own and children growing up separated from their birth family.
Discussion
The aim of this study was to investigate the mid-life outcomes of two cohorts of infant adoptions. Law across the UK considers adoption as a life-long experience, for example in England: ‘the paramount consideration of the court or adoption agency must be the child’s welfare, throughout his life’ (Adoption and Children Act 2002, Part 1, section 1(2), emphasis added). It is therefore important to produce evidence on long-term outcomes.
Using information gathered from the 1958 and BCS70 cohorts we were able to assess the psychological outcomes and make a comparison both with those who were raised in two biological parent families, and also with children who (like the adopted children) were born to single mothers, but who remained in their families of origin. We explored both pre- and post-natal factors that may have contributed to differences in outcome. This further follow-up of the British birth cohort studies has shown that the infant adopted group does not, on the majority of measures, have worse outcomes than the non-adopted general population sample born at the same time. Increased risks reported in other studies were not found here – for most outcomes. Most people adopted in infancy (a potentially vulnerable group) were faring well at mid-life.
As expected, these British infant domestic adoption outcomes are much more favourable than those adoption studies based on children with adverse childhood experiences (including depriving orphanage care, sustained familial maltreatment or neglect). These adopted adults did not appear to have placed any excess demand on the mental health services. The birth comparison group (other children born to and raised by their single mothers) fared least well. These children grew up in less favourable circumstances materially and in terms of social class and home ownership. They may have experienced negative social attitudes and the limited welfare provision of the time, although for some this will have been mitigated in part by support within their own families and communities.
In contrast to much recent adoption research, the infant domestic adoption study does not involve samples that were exposed to prolonged early adversity nor discontinuity of care. As far as we are aware, during the brief period that mother and child were together, there was no maltreatment and so such children are unlikely to have been emotionally or behaviourally dysregulated when placed with the adopters. However, we cannot rule out the possibility of inherited temperamental difficulties.
Some vulnerabilities appear to remain, even when there is no apparent post-natal adversity. It is suggested here, and consistent with much other research, that aspects of the pregnancy could affect development adversely. Smoking in pregnancy may possibly interfere with foetal brain development (for a recent review see Ekblad, Korkeila and Lehtonen, 2015). Pregnancy at a young age carries greater risk of low birth weight, pre-term birth and poorer child outcomes (Moffitt and the E Risk Study Team, 2002). Recent evidence suggests that younger age at first birth may also be associated with genetic vulnerabilities to disinhibited behaviours and poor self-control (Richmond‐Rakerd, et al., 2020). Late-seeking and insufficient ante-natal care may have meant less good health advice, poor detection of problems and more risks to the pregnancy. Although not assessed in this study, we might suppose that stress during unplanned pregnancy in the young unmarried mothers might be linked to developmental problems. For a review of the effects of maternal stress in pregnancy, see Glover (2011). It is important to recognise that such risk factors, like protective factors, have been derived from studies of large samples, and so indicate what may happen rather than what will happen for any individual child.
Even in these low-risk, non-maltreated adopted samples where there was no evidence of maltreatment or multiple moves, there were clearly elevated risks on externalising problems for a sub-group in mid-life. This was a consistent finding across both cohorts. We have no evidence that these groups of children were exposed to the types of parenting often found to be associated with anti-social behaviour so, although we cannot rule it out for individual children, the anti-social outcomes for the sub-group of adopted people are unlikely to be due to adverse adoptive parenting. Developmental risks are therefore more likely to be implicated, related to genetic and pre-natal factors. Psychological stresses related to being adopted may also have played a part in some cases.
By and large, however, the adopted group had prospered. Transfer early in life to an adoptive home was primarily intended to provide a secure, loving family, but it also will have given most children the advantages of a somewhat privileged childhood because of the recruitment and selection process operated at the time. It may also have provided a protective effect to counter any psychological distress related to pre-natal vulnerabilities. In addition to financial support and material aspects, there are likely to be other beneficial factors that adoptive parents pass on: access to educational and occupational expectations, influences of school and community, all of which may combine to smooth the path to a more comfortable and satisfying adult life.
Implications
Caution must be exercised in making recommendations based on outcomes for children who were born in very different circumstances from those of today. Smoking during pregnancy is a known risk, but rates of smoking have reduced considerably as a result of health education campaigns. On the other hand, problem substance use has increased in the population as has the incidence of Foetal Alcohol Syndrome (FAS) (Popova, et al., 2017). Good quality and accessible maternity health services, where concerns can be freely expressed and support and advice received, remain crucially important. Our findings support the continued promotion of effective and non-stigmatising intervention programmes during pregnancy to reduce risks due to smoking and any other known hazards to infant health.
However, the small group, mostly male, who exhibited ‘externalising’ problems are a cause for concern. Greater understanding is needed of the mechanisms linking the genetic, pre-natal and peri-natal factors with the anti-social behaviour of a minority of the adopted and birth comparison groups. It appears that some negative behaviours may not be entirely amenable to the benefits of a positive, stable adoptive home. The earlier such difficulties are identified, the sooner appropriate interventions can be put in place to prevent long-term negative trajectories. Prospective adopters of infants should be advised, frankly but sensitively, of the possible consequences for their children of these early vulnerabilities. A balance should be struck between observing the principle of honesty about possible risks, in order that an informed decision can be made about adoption, while not deterring a potentially valuable resource for the care of children. As behaviour problems might emerge during childhood, the earlier they are identified, the sooner appropriate support can be put in place to try to prevent long-term negative trajectories.
The study indicates that both biological and environmental factors have an influence on development. It is possible that genetic influences have been underplayed and environmental/psychological explanations have predominated in the adoption theory and practice literature. Researchers oriented to the field of child welfare may have focused more on psychological stresses and their consequences for placement stability and for later psycho-social outcomes.
Baden and O’Leary (2007) have addressed the question of long-term adoption outcomes and the importance of integrating research findings with counselling practice. Their review of outcomes stresses that concerns will apply only to a sub-set of adopted adults. Our study indicates that concerns may not only be about internal conflicts (identity, sense of self, abandonment, etc.) but we would also want to highlight the possibility of externalising behaviour as problematic outcomes. Those adopted adults seeking psychological services will be better served if training is more adoption-related, if it embraces a life-span perspective and if practitioners are alert to pre-natal as well as post-natal adversities. However, more needs to be known about what interventions, of what kind, to which adopted people and applied at what stage in life, can contribute to positive adjustment. A major advantage of nationally representative samples such as those we studied is that all the participants can be assessed, not just the people who seek and attend services. It may be that people in the sub-group with externalising problems cause distress to others by their behaviour, but are less likely to acknowledge the need to seek counselling help.
Conclusions
In general, infant-adopted adults in the samples we studied fared well in most, but not all, of the measured outcomes. The most unexpected aspect of the findings was the differing patterns of internalising and externalising problems. For the former, the beneficial adoptive environment appears to have contributed to protective processes. For the latter, such protective influences were much less apparent, and the findings pointed instead to long-term consequences of very early risks.
Future research into adoptive samples beyond mid-life could potentially show whether the protective processes persist into later life stages and whether health risks become evident at a later stage. Research more closely focused on the adoption experience may be able to complement the type of study reported on here in order to investigate outcomes such as the quality of adult relationships, a secure sense of identity and preoccupation with origins.
Footnotes
Acknowledgements
This study was funded by the Nuffield Foundation (KID 41956). We are grateful to members of our Advisory Group (Stephan Collishaw, Gordon Harold, Amanda Sacker, Julie Selwyn and John Simmonds) for their valuable comments and support; to the UK Data Archive for access to the main data; and to staff at the Centre for Longitudinal Studies, University College London, for additional help with data checking.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.