
Abstract
Background:
Research in occupational therapy that engages both the perspectives of therapists and service users from the Somali community in the United Kingdom is limited. While occupational therapy is acknowledging its Eurocentric foundations, efforts are underway to adapt its models of practice to better suit cross-cultural contexts.
Aim:
To explore occupational therapists’ experiences in working cross-culturally with Somali service users.
Methodology:
A participatory research approach was used. Six virtual online World Cafés were conducted, with a total of 120 therapists participating. Data were analysed using template analysis.
Findings:
Three key themes emerged: (1) Accessing occupational therapy – highlighting the need to reach people and effectively communicate occupational therapy’s role, (2) cultural relevance of occupational therapy – highlighting the need for culturally congruent interventions and (3) from cultural (in)competence to cultural humility – highlighting the importance of diverse occupational therapy teams and the need to develop confidence in culturally humble practice.
Conclusion:
Occupational therapists must critically examine their use of language, terminology, identity and professional culture, as these elements may inadvertently hinder equitable access for diverse populations. This paper calls for continuous efforts to make occupational therapy practices more inclusive and accessible.
Background
Occupational therapy is beginning to critically examine its Eurocentric foundations, particularly the reliance on models of practice that prioritise independence over interdependence (Iwama, 2007). Increasing recognition is being given to the importance of meeting the needs of service users from cultures distinct from our own, or marginalised by predominant culture in each country. In response, there is a shift from a cultural competence model to one of cultural humility, characterised by flexibility, awareness of bias, a commitment to lifelong learning about diversity and an acknowledgement of power dynamics in healthcare interactions (Agner, 2020). This shift is particularly significant in the United Kingdom (UK), where the occupational therapy workforce does not reflect the diversity of England’s population, with only 9% of therapist from minority backgrounds (NHS Digital, 2021). Furthermore, the profession has faced criticism for failing to address systemic injustices (Hammell, 2021). A critical gap remains in research regarding how occupational therapy services align with, and respond to, the needs of minority groups both from an occupational therapy perspective and from the viewpoints of communities and service users (Steede and Gough, 2022).
Health equity in occupational therapy
Occupational therapists are increasingly aware of the need to reflect on their practices to ensure that services are accessible and equitable for all communities (Office for Health Improvement and Disparities, 2022). Yet, in socially disadvantaged areas, access to occupational therapy and related services is often of lower quality, despite greater healthcare needs (Cookson et al., 2021). A study examining general practitioners (GPs), practice-employed nurses and other allied healthcare professionals found that GP practices in deprived areas had fewer whole-time equivalent clinicians compared to those in more affluent areas (Mercer et al., 2023). Patients in high-deprivation locations reported lower satisfaction with both access to and the quality of consultations than their counterparts in low-deprivation areas (Cookson et al., 2021; Mercer et al., 2023), highlighting the risk that occupational therapy services, if not designed with equity in mind, may inadvertently reinforce existing health disparities.
This pattern of inequitable access to healthcare services is also evident internationally. In the United States (US), Hispanic patients were found to have significantly lower referral rates and fewer physical therapy and occupational therapy sessions compared to non-Hispanic White patients (Jolley et al., 2022). Further factors such as age, minoritised status, significant other status and insurance type were identified as influencing the likelihood of receiving occupational therapy (Kinney et al., 2024), thus highlighting the importance of embedding equity, cultural responsiveness and advocacy into practice to avoid perpetuating such disparities.
It is, therefore, encouraging to see international efforts to promote equitable access to occupational therapy. For instance, a scoping review explored the service needs of people with disabilities from culturally and linguistically diverse (CALD) backgrounds (Chu et al., 2024). Across the 14 included in that review, the authors identified several factors as important to supporting access to care including availability of interpreters, clear information about available services, culturally appropriate resources and programmes. Responsive service delivery was characterised by building therapeutic relationships with CALD service users, actively engaging family members in the therapeutic process and fostering connecting with the wider community (Chu et al., 2024). Chu et al.’s (2024) review highlights many factors that need to be considered when designing healthcare services that are culturally responsive and can reduce health inequities. While other studies describe cultural competence and humility in occupational therapy (e.g. Agner, 2020; Singh et al., 2022) and provide guidance on educating learners and practitioners to strengthen culturally responsive practice (e.g. Davis-Cheshire and Crabtree, 2019; Meechan et al,, 2024), little is known about occupational therapists’ experiences of working cross-culturally, representing a critical gap in the evidence base. In another systematic literature review, Crawley (2022) identified only six papers that presented the lived experiences of occupational therapists and students working in cross-cultural services across various countries, including the UK, South Africa, Australia, the US, Canada and Ireland. This review highlighted both strategies for, and barriers to, delivering culturally competent practice.
Although the term ‘Black and Minority Ethnic’ is widely used in the UK to refer to minority groups, there is a risk in treating such a diverse group as a homogeneous entity. Clinical and policy decisions based on aggregated data may, therefore, reflect the needs of some groups while overlooking others (Khunti et al., 2020). Somalis are one such group with CALD backgrounds who have a long history of migration to the UK, particularly since the 1991 Somali Civil War. The most recent census records 176,645 people in the UK identifying as Somali, of whom 43.5% (approximately 76,841) were UK-born (Office for National Statistics, 2023). Somali settlement in the UK dates to the late 19th century. A further significant wave of migration occurred from the late 1980s into the 1990s, when large numbers of Somalis sought asylum in the UK because of the Somali Civil War (Sporton, 2005). Since the late 1990s and early 2000s, the Somali community in the UK has increasingly been shaped by secondary migration from the Netherlands and Scandinavia rather than by direct migration from Somalia (Ahrens et al., 2016; Yasin Abdi, 2025).
The UK is now home to the largest Somali population in Europe (Birmingham City Council, 2022). The Somali population in the UK experiences high poverty rates, with 82% of Somali pupils eligible for free school meals. Their educational outcomes are amongst the lowest compared to other minority groups. Although many fled conflicts, Somalis continue to experience stigma and hostility in the UK, especially when living in shared accommodation (Ermansons et al., 2024). These social factors were especially evident during the COVID-19 pandemic, when Somali leaders wrote to a national newspaper highlighting housing pressures, in-work poverty and racial inequalities (Bede and Lewis, 2023; Mudhin, 2021). Such intersecting structural and social disadvantages have direct implications for health equity and access to occupational therapy, reinforcing the importance of recognising the specific needs of distinct communities rather than relying on broad, catch-all categories.
There is also evidence suggesting that the Somali community does not have fair access to services. A report on Somali mental health services found that, although Somalis were interested in accessing support, only 14% had used mental health services. Additionally, 66% of respondents were not aware of any local mental health services (Anti-Tribalism Movement, 2020). In their systematic review of barriers to use of mental health services for African immigrants in the UK, Bassey and Zaka (2024) found a complex intersection between stigma and discrimination, living in temporary housing, cultural beliefs and practices and accessibility of services. They recommended collaboration across key stakeholders to advance equitable and inclusive health services that are culturally sensitive, affordable and accessible.
Context of research
Occupational therapists are key stakeholders to advancing equitable and inclusive healthcare services. However, there is limited evidence of occupational therapy research and practice with the Somali diaspora in the UK. For instance, Pollard et al. (2018) conducted a case study on the occupational needs of Somali people, but did not specifically connect their findings to occupational therapy practice. This gap of evidence presents challenge for occupational therapists working in Northwest London, who identified the need to reflect on Somali service users’ experiences of occupational therapy to inform more culturally responsive practice.
As a starting point, the aim of this qualitative study was to explore occupational therapists’ experiences of working cross-culturally with Somali service users in the UK. Such reflection on practice can help identify ways to enhance the efficacy of occupational therapy in cross-cultural contexts, and support people from Somali and other Black and Minority Ethnic communities in the UK to achieve equitable health outcomes (Crawley, 2022).
This study was conducted in the London Borough of Brent, situated in North West London. Brent is one of the most ethnically diverse areas in the UK, with over 65% of its residents belonging to Black, Asian and minority ethnic backgrounds. The borough also experiences significant health inequalities, with life expectancy and health outcomes varying widely between different communities and neighbourhoods (Brent Council, 2025).
Methodology
We adopted a participatory learning and action (PLA) research methodology, treating all stakeholders as equal partners and collaborators in the research process (de Brún et al., 2017). PLA is designed for research with diverse groups where power asymmetries may exist, and it emphasises reciprocity, mutual respect, cooperation and dialogue (de Brún et al., 2017). Within PLA, World Cafés provide an inclusive setting that allows participants to exchange ideas and perspectives in small, café-like groups, with participants rotating to new tables to discuss different topics (Brown and Isaacs, 2002). They are particularly useful when an issue is not well defined and needs to be explored through deep and several insights (Recchia et al., 2022).
The COREQ 32-item checklist (Tong et al., 2007) for qualitative studies was used to enhance transparency and methodological rigour. Its application informed more explicit reflexive reporting of the authors’ occupational therapy and Somali backgrounds, professional values and interest in addressing inequities in access to services, alongside consideration of how these may have influenced data generation and interpretation. The qualitative analytic approach was clearly articulated and justified in relation to occupational therapy’s emphasis on lived experience and occupational participation. Greater detail was provided on culturally responsive, community-based recruitment and data collection procedures to support ethical engagement with Somali participants. The analytic process was further clarified, and the reporting of findings was refined through clearer distinction between major and minor themes, and increased use of verbatim participant quotations, ensuring that participants’ perspectives remained central.
Research team and reflexivity
The research team included three female occupational therapists with diverse ethnicities including mixed heritage, South Asian and South African, and a male Somali community member employed as a research assistant. Two researchers had PhD’s and worked for universities in the UK and South Africa. One researcher worked for a National Health Service (NHS) Trust.
Relationships with the Somali community were established in 2021 by Atwal and Chauhan Gawde. In a university funded co-production research project, we explored research priorities for occupational therapy with this community, and whether research was needed. The occupational therapists who participated in the current study were not previously known to the research team. However, some of the researchers may have been known to participants because of their position as national leaders in the field.
Participant selection
Participants were selected through convenience sampling. We approached NHS England (London), who sent research invitations to Allied Health Professions leads via email. These leads then forwarded the research invitation to occupational therapists, also via email. Our target was 120 participants, as suggested by Banfield et al. (2021). We received a positive response, with an average of 20 participants per session. No participants took part in multiple sessions. The final total was 120 participants across the 6 World Café sessions: Session 1 (n = 20), session 2 (n = 18), session 3 (n = 20), session 4 (n = 24), session 5 (n = 20) and session 6 (n = 18). We did not collect data on professional role (e.g. occupational therapist and supporter) as part of the formal consent process. Although participants’ backgrounds were discussed during the meetings, we did not have ethical approval to share this information. However, given the focus on professional inclusivity, we believe that the majority of participants were registered occupational therapists.
Formal qualitative sampling techniques were not adopted, and theoretical saturation was not the goal of this study (McGrath et al., 2023). Because of the method of recruitment used, the number of people who refused to participate is unknown. No participants dropped out or withdrew from the study.
Data collection
The World Cafes used for data collection were hosted online via Microsoft Teams. Virtual World Cafés have previously been used to identify health research priorities (Banfield et al., 2021) and to support teaching on indigenous health issues (Laine-Gossin et al., 2022). They are recognised as providing a safe and inclusive space for participants to share challenges and explore opportunities (McKimm et al., 2020), which was which was particularly important in this study given the focus on therapists’ experiences of culturally diverse occupational therapy practice.
Following guidance of Albrecht et al. (2022), we adapted the World Café methodology for a virtual format. We hosted six online World Cafés, each lasting approximately 90 minutes. This duration, also used by Laine-Gossin et al. (2022), has been noted to sometimes limit participant interaction due to technology barriers. However, this was not a challenge in our study, as the therapists were familiar with the technology and motivated by their commitment to population health. Our rationale for making the virtual World Café sessions shorter was to ensure inclusivity, recognising that practice-based occupational therapists may have limited time away from patient-facing activities. This adjustment appeared to facilitate participation, as evidenced by strong engagement from both therapists and support workers, contrasting with the recruitment challenges noted in similar studies (Albrecht et al., 2022; Banfield et al., 2021).
The research team adopted the role of hosts, maintaining minimal, primarily limited to timekeeping and introducing the interview questions. Efforts were made to create a welcoming and safe environment, including providing clear information on the research aims and ethical considerations. The use of the chat function and emojis was encouraged to complement verbal discussion, offering participants additional ways to contribute. Finally, participants were randomly assigned to café groups, which allowed for diverse perspectives to emerge within each session.
Instead of using multiple breakout rooms, we used single breakout rooms that ran concurrently for all of the world cafes. This approach, also employed by Banfield et al. (2021), did not hinder the achievement of our study’s aims. The single-group setup allowed us to record each session, using the audio–visual recording function in MS Teams. While moving between groups can encourage cross-pollination of ideas (Löhr et al., 2020), all of our participants remained in static groups. This did not limit idea generation, as the occupational therapists were highly passionate and deeply engaged with the topic. Although we provided whiteboards and other interactive tools, participants primarily used the chat and emojis to support their statements or comments.
In line with COREQ Item 17, the open-ended World Café questions were developed iteratively by the research team in relation to the study aims and occupational therapy literature on access, participation and service engagement. Questions were intentionally broad and narrative-focussed to support shared discussion of lived experiences, rather than evaluation of specific services. Draft questions were reviewed and refined with community partners to ensure cultural relevance, accessibility and sensitivity to language and power dynamics. The final set of questions was further refined through team discussion and informal piloting to support clarity, conversational flow and alignment with World Café principles of dialogue and collective reflection.
All six World Cafés discussed the same open-ended questions. This differs from Albrecht et al. (2022), who adapted questions based on varying structures, cultures, interactions and processes. Each café concluded with a wrap-up session to summarise the discussions. Transcripts were created for each session. They were not returned to participants.
Data analysis
Data were coded by Atwal and Plastow using AtlasTI qualitative analysis software. This software supported the organisation and systematic comparison of data across transcripts. The software was used to manage the dataset, apply and refine codes and facilitate comparison of coded material across participants and World Café discussions, strengthening transparency in the analytic process.
Template Analysis was used to analyse the data as it is a nuanced approach to managing large datasets while ensuring that the complexity of participants’ perspectives is preserved (King et al., 2018). In the context of this study, Template Analysis was appropriate as it facilitated understanding of occupational therapy access and provision, while allowing culturally specific or unexpected insights to be captured. An initial coding template was developed using a priori codes informed by the World Café questions, which provided a starting structure for the analysis. The framework was then refined through inductive analysis of the data, allowing new codes and themes to emerge (Brooks et al., 2015).
Each member of the research team reviewed a transcript, applying these codes and also noting any additional inductive codes that emerged from the data. By an iterative process, it means analysis did not follow a single, linear sequence. Instead, the coding framework was repeatedly reviewed and refined as the research team moved back and forth between the data. Where appropriate, multiple codes were applied to the same data segment to reflect the complexity of participants’ accounts. The research team then met to compare coded content across transcripts, discuss areas of similarity and difference and agree refinements to the coding template.
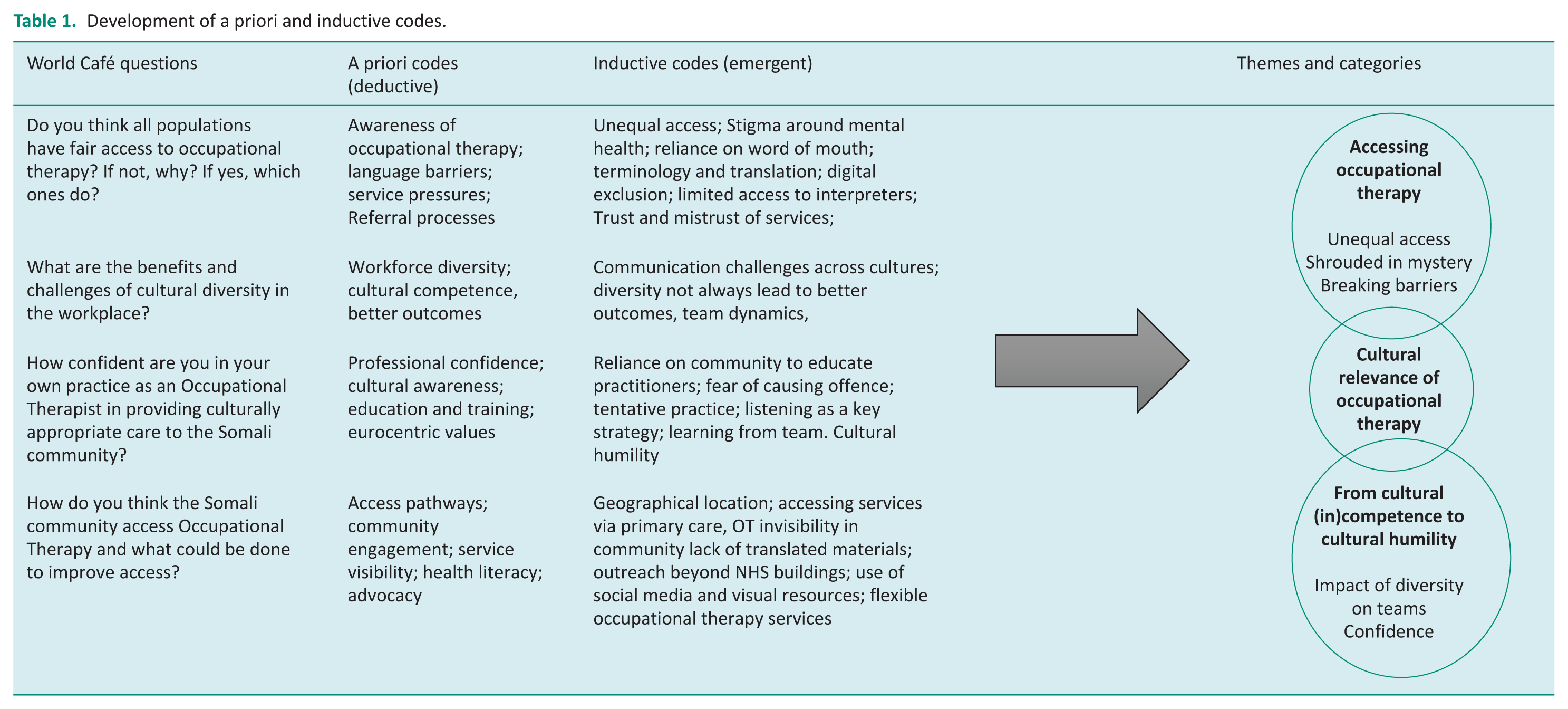
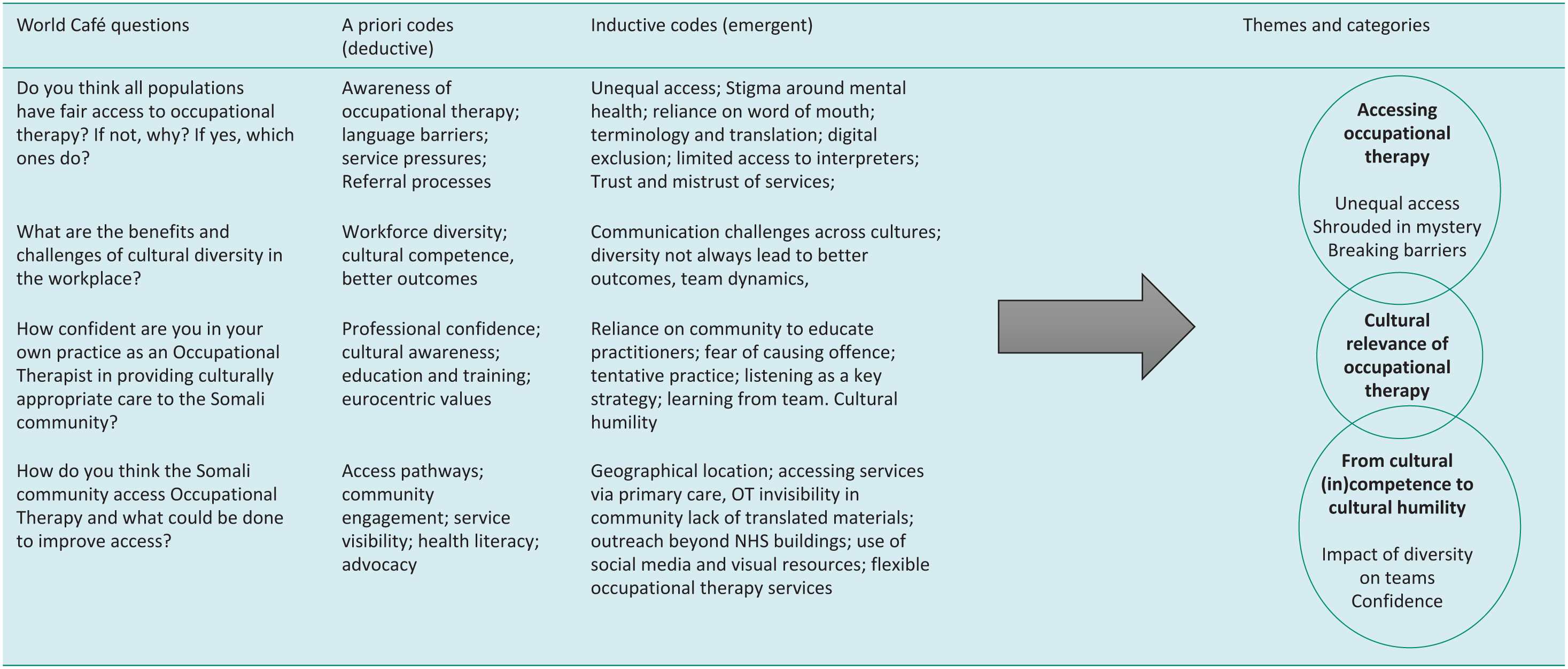
While a priori codes provided a useful starting point, they did not fully capture the breadth or specificity of participants’ accounts. New codes were, therefore, generated inductively where data did not align with existing codes or categories, particularly in relation to culturally specific experiences of accessing occupational therapy and perceptions of professional representation. Refinement of the framework was an iterative process, involving comparison of coded data across transcripts and ongoing discussion within the research team to consider how emerging insights related to, extended, or challenged the original analytical structure. This process enabled the framework to move beyond the initial questions to reflect participants’ priorities more closely, strengthening the interpretive depth of the analysis and informing the final set of themes, and their categories, presented in Table 1.
Development of a priori and inductive codes.
Findings
Data analysis revealed rich findings about occupational therapists’ experiences of working cross-culturally with members of the Somali community in the UK. Three themes emerged: ‘Accessing occupational therapy’, the ‘Cultural relevance of occupational therapy’ and ‘From cultural (in)competence to cultural humility’. Together these themes highlighted that working cross-culturally requires skills in communication, listening and relationship-building, starting within a multicultural occupational therapy team working in partnership with communities.
During the discussion rounds, participants identified several key themes reflecting the complexities of real-world practice. These included challenges in ensuring timely access to interpreters, persistent funding constraints, limited time available to engage with participants and restricted opportunities for training and professional development. Participants also highlighted anxieties about the risk of unintentionally offending individuals from diverse cultural backgrounds. Although there was a clear motivation to enhance practice, this was accompanied by growing frustration regarding inadequate access to resources.
Braun and Clarke (2021) recommend using pseudonyms or codes that preserve confidentiality while remaining reader friendly. For example, CC1 refers to the world café one, followed by a pseudonym of the therapist who attended. In our research, we have uneven distribution of data across themes, which is common in qualitative research. Braun and Clarke (2006; Braun et al., 2019) emphasise that the richness and analytic importance of a theme, rather than its size, determines how much space is given to it. In this case, some themes are longer because they capture a central organising concept that integrates multiple sub-themes or codes (King, 2004).
Theme 1: Accessing occupational therapy
Unequal access
Ensuring that occupational therapy is accessible to members of the Somali community meant reaching those who are ‘kind of off the radar’, effectively communicating the role of occupational therapy to service users and increasing its visibility at a community level.
There was a perception that not all minority groups had equal access to occupational therapy (CC1 JC, VS, CC5 RM). ‘There is an issue with the communities that we serve and kind of the different young people from different backgrounds not accessing CAMs. So, we know our data is skewed with regards to the number of children from a white background who can access services’. (CC5 LM) ‘There’s no leaflets in community centres or Mosque. T’s just word of mouth. Do they understand what OT is? So, we’re trying to make sure there are other services that are signposting them to us, but I’m just the only occupational therapist on the team, so there’s staffing issues’. (CC4 LB)
Factors influencing access were related to awareness and complexities surrounding the referral process (CC2 BN) as well as access to digital technologies (CC2 KO). One occupational therapist stated, ‘I guess if you don’t have access to something, it won’t be relevant to you’ (CC1, VS), similarly another OT stated, ‘It comes down to whether the Somali community feel that we’re accessible to them if we’re not accessible, it’s not going to be relevant’ (CC1 HN). Factors perceived to influence access include geographical location (CC2, HS) and knowledge about OT (CC4 VJ).
In some services, there was a view of an overrepresentation of certain ethnic groups. ‘In our service black men are very overrepresented which indicates perhaps they’re not being picked up, at the earlier intervention stage. So, see things for how they really are’ (CC7 SP). There was also perceived stigma around mental health (CC2 HN) and issues related to trust which could be linked with professionals working with the police (CC1 EM, CC2 HN). Additionally, the Somali community felt that their issues were not being resolved or taken seriously (CC1. HN).
It was also noted that language barriers led to cultural clashes (CC5, WP). Access to interpreters was seen as difficult, which impacted inclusion in occupational therapy interventions (CC4 F CC5, WP, MNR, CC6 SR). Further challenges were associated with large and complex caseloads (CC4 F and MNR). ‘I don’t understand why it’s so difficult to get hold of an interpreter. I guess in terms of access to mental health groups, interpreters are often seen as disrupters, and it has been known that people haven’t been able to attend groups we couldn’t get an interpreter there in the room’. (CC4 T)
The terminology occupational therapists used to explain their role was seen as leading to misunderstandings both with the Somali community and with interpreters (CC1, EM, PM, CC3 ZX). ‘But it’s also impacted by things like, translators. I don’t know how confident I feel. It’s not their fault. I think the language we use and the way we explain things. It’s quite tricky to get that cross’. (CC6, SS) ‘If you have a child with autism for example who needed advice for sensory regulation. But someone might not know what sincerely regulation is. So, you have tried to explain what your role is as an OT is, but because of the language and terminology that you’re using, people still don’t know what an OT is does. So, what is simplest way that someone who’s out of health can understand what occupational therapy is?’ (CC1 FM)
‘We’re kind of shrouded in mystery’ (CC4 NS)
A lack of understanding of occupational therapy and what it could offer was another perceived barrier to accessibility of occupational therapy services. There was view that there was a general misunderstanding in wider health care about occupational therapy (CC4 N, CC5 RM, ST, CC5 RM, ST, CC 1, KO, CC2TP, CC3 ZX), especially accessibility for children and young people (CC4 NAS, SSR) ‘People ask me what is that? I never heard of it before. And just in terms of like accessing people knowing what OT is, I feel like in general, unless you’re involved in health services, people generally have difficulty knowing what an OT is’. (CC2 EM)
Talking about health conditions was seen as problematic due to translation issues meaning that terms had to be described (CC1 EM). Occupational therapists also felt that it was difficult to explain occupational therapy to the community in a way that was relatable. Additional complexities were perceived to arise from teams delivering either occupational therapy-specific interventions or more generic work (CC4 DJ). It was believed that the community themselves would know if occupational therapy was relevant to them (CC1, PM, CC1 EM). However, the relevance of occupational therapy could only be determined if there was access to information about it and an understanding of collective communities (CC2, HJ, CC3 ZX).
Collective communities place a strong emphasis on family (CC3, ZX). For some occupational therapists, the reliance on family was perceived to making their role less relevant. They just think we provide this equipment. Can you provide this equipment? So, it’s a bit of a challenging in terms of how we’re going to help them (CC4 SG).
‘Breaking barriers by going into their community’ (CC7 RA)
Various strategies were suggested to increase the visibility of occupational therapy. These included social media, utilising community centres, places of worship (CC2 JJ, P, TM) and engaging in advocacy work (CC2 VJ, CC7 RA). Other strategies included improving accessibility via GPs (CC7 RA) and community leaders (CC7 T). There was also an awareness of the need to clearly articulate the role of occupational therapists’ (CC1PM, CC2 VJ) and to showcase what they could offer to communities (CC3 ZX). One participant suggested videos or leaflets translated into multiple languages, as well as mobile occupational therapy clinics (CC7 T). Having a role model from the community was seen as important for building relationships with the community (CC6 KI). ‘His English was very limited, but he wanted to access the community. I knew the language barrier. I requested to see if anyone from the team came from the Somali community and luckily enough I did. They co worked with that person. So it was quite nice for them to gain that relationship and that rapport. It helped me to understand a little bit more of what that clients’ needs were and to co work with them’. (CC7 RA) ‘There’s been a big push to work closer with third sector partners. I’ve yet to really see OT embrace working with culturally appropriate advocates . . . moving away from NHS buildings and trying to really embrace working in people’s communities when they’re running OT groups (CC4 TM)
One occupational therapist described challenges in the community related to accessing services through a GP ‘I guess there’s quite a few hoops to go through before you reach an occupational therapist. It might be via a GP for example, so to get to the OTs where I am, you’d need to go to your GP, have an effective conversation so that the GP does refer you. But then there’s another hoop you wouldn’t come straight to OT. Then you have a generic assessment ‘(CC7, SP)
Theme 2: Cultural relevance of occupational therapy
To make occupational therapy more culturally relevant to the community, some occupational therapists incorporated interventions that aligned with their clients’ beliefs (CC7 T). There was also a view that occupational therapists needed to think more creatively about the models and the frames of references used in practice (CC4 T). Barrier to culturally relevant care were attributed to differing beliefs about healing. There were perceived conflicts between Occupational therapy and Somali community. ‘I mean, figuring out someone’s lens is difficult, particularly in an acute setting, I’d met with this big group of refugee women in Westminster and one of the things that they were talking about was how the hate going to physio. Their physios give them exercise sheets because their view was that healing is through touch. It made me think again of the stroke setting and we would often be asked by family members to massage the leg, massage the arm and we’re kind of like, no, no, no. That’s not how it works, So I think there’s middle roads that we just missing altogether’. (CC1 JC)
There was also a view that the values of the Somali community conflicted with those of occupational therapy in the UK, particularly when contrasting individualism and independence with collectivism and interdependence. The family and the community wanted their voices to be heard, which was sometimes seen as ‘stepping over a patients boundaries’. ‘Our values can be quite Eurocentric as we’re looking at someone as an individual, we’re looking at them being independent, having autonomy and choice. . . but it could be for someone in the Somali community, their lifestyle is quite connected to their community. I can speak, I guess, from my own culture as well, decisions that I make about my health and care are influenced by my family and my wider community There might be a lack of understanding maybe from the OT perspective about that lens kind of looking at someone more as an individual versus as a part of a wider community’. (CC1 VS)
Within the World Cafes, the term ‘interdependency’ and the values held by occupational therapists were also debated. ‘Is there a clear understanding of interdependency, does it apply to everyone? We always focus on function, fun and participation. But what does that mean to the other parties? What does that mean to clients? We use technologies that are not easily understood by communities, whether that is Somali community or whether that’s ethnic other ethnic background minorities. . . I don’t know how to explain really, but I just feel the word interdependency doesn’t necessarily apply to many ethnic minorities’.
Theme 3: From cultural (in)competence to cultural humility
The findings of this study also revealed that the development of cultural humility is a process that is influenced by the diversity of the occupational therapy team in which therapists work, as well as the confidence they had in themselves to meet the needs of Somali service users in their cross-cultural practice.
Impact of diversity on teams
There was view that diversity alone in teams did not always have led to positive outcomes in care, nor did it ensure that patients’ cultural needs were being met (CC1 VC). However, having a diverse team could contribute to more culturally sensitive care ‘A lot of my team is pretty white and so I have noticed in the past where like some of my some of my colleagues that I work with might not pick up on certain things that I would. We went to see the patient, we wanted to get him up and moving, but he wanted to first make sure he had his turban on. The physiotherapist didn’t fully gather that, so I had to step in and just make we should get that done first and then we can go. You don’t need to rush the situation. So, I think sometimes it’s even like small things like that, that people don’t always pick up on. And I think the same could be said for the Somali community because we don’t really have that representation in our team’. (CC6 FA)
Factors that attributed to negative outcomes were cultural differences which were perceived to have an impact on team dynamics (CC7 T). Communication also became more difficult amongst team members which could lead to conflicts (CC3 S). ‘Think there’s a little bit of barrier based on cultural differences, you know, in language, in communication styles, you know some points, leads to misunderstandings and it hinders some effective collaboration’. (CC7 AL) ‘I’m from South Africa originally and the way South Africans communicate sometimes it’s very direct and you know, you can offend people by being very direct because some people are very polite in the way that they communicate’. (CC1 JC)
There was a view that occupational therapists who had not grown up in London did not understand the subtle nuances of how cultures interacted and were unaware of ‘their own shortcoming’ (CC4 GV). Diversity within teams and representation was viewed as a means of understanding diversity and the person (CC6 IM). ‘We have got people from 16 different nationalities. There is a massive respect for everyone whatever they think. We go out and socialize together. . .. Learned more and more from colleagues at work. . .So just because somebody takes the time to go for prayers or go to mosque on Friday at a certain time, you can’t then assume that somebody who looks the same or who’s from the same ethnicity will want the same time off or the same holidays, or that they would follow the same dietary requirements’. (CC4, ND) ‘Really important that the healthcare workers reflect the patient group as well. . . representation is important and it’s important for patients. That the healthcare workers can understand, their point of view and where they’re coming from’. (CC6 FA)
Improving the diversity of the profession was a motivating factor. ‘The reason why I wanted to become an OT is because I wanted to show that level of diversity within OT and to express that to the clientele that we work with. I come from Bangladesh background. I work in perinatal community team and I’ve noticed that there is a lot of Bangladesh community and I’m able to communicate and talk to them and kind of find that cultural differences and stuff like that. So I think it does bring a different element of a relationship’. (CC7 RA)
Confidence
Across our World Cafes, most occupational therapists reported depending on the community and or the patients to educate them about culture. One therapist noted ‘We grow to understand that person and what’s important to them and their background and that kind of thing’ (CC1 HG). Another one stated ‘I don’t want to offend people, but because I don’t have a good understanding of all the different cultures that they are. . .more cautious, I would say when approaching someone who’s from a community where I think’.
For some occupational therapists, this meant they were more tentative in their approach (CC1 JC). ‘I have supported people from the Somali community before, but I can put my hands up and say I’ve probably had to lean on them to support me and guide me with understanding that as well (CC1 HN)/ Listening was viewed as important’. (CC1 M, CC4 V) ‘If you work in a fast-paced service, do you have the time to understand those cultures? I guess it’s, making sure that you have that time to do that, and you know at the end of the day it’s a service user that’s getting an injustice’. (CC1 HN)
Discussion
In the UK, the NHS has a legal responsibility to ensure equitable access to health services, including occupational therapy (NHS England, 2023). While health inequalities are often attributed to environmental and social determinants within communities (Office for Health Improvement and Disparities, 2022), As analysis progressed, it became clear that while structural and environmental factors shape access to occupational therapy, many of the barriers described by participants were also rooted within the culture of the profession itself. Through iterative refinement of the analytical framework, participants’ accounts consistently pointed to issues of role clarity, professional language and underlying assumptions about practice that were not fully captured by the initial focus on access alone. These patterns shifted our attention towards factors that are, in principle, within the profession’s control and therefore resolvable. The discussion that follows reflects this analytic shift. The discussion is organised around the three interrelated themes: accessing occupational therapy, the cultural relevance of occupational therapy, the need for culturally congruent interventions and a shift from cultural (in)competence to cultural humility.
Participants in this study consistently identified barriers to accessing occupational therapy that were linked to occupational therapists’ difficulty in clearly and consistently explaining their role and the services they offer. Our study highlights the importance of other health professionals understanding the role and scope of occupational therapy, particularly given that professionals such as GPs act as gatekeepers within the referral process.
These findings align with existing literature demonstrating poor awareness of occupational therapy across health disciplines, both within the UK and internationally (Edwards et al., 2024; Malka et al., 2024; Mani and Velan, 2020; Mthembu et al., 2022). Although doctors may recognise occupational therapy as an essential profession, they are often unaware of its full scope of practice (Vij, 2023). This lack of clarity is particularly concerning in the context of current policy ambitions to integrate occupational therapists into primary care and reduce health inequalities (RCOT, 2026).
Participants also highlighted that limited understanding of occupational therapy among service users acts as a barrier to engagement. This may be particularly challenging for the Somali community, as there are no registered occupational therapists in Somalia (World Federation of Occupational Therapists, 2022). However, a lack of service user understanding of occupational therapy extends beyond one community. International studies similarly report low levels of public awareness of occupational therapy (Banamah et al., 2023; Rahja and Laver, 2019), suggesting that this represents a broader professional challenge rather than a culturally specific deficit.
The cultural relevance of occupational therapy highlighted challenges in communicating the profession’s role and scope across linguistic and cultural contexts. Participants described how the absence of equivalent terminology in languages such as Somali often led to misunderstanding, limiting meaningful engagement with occupational therapy services. These difficulties were not solely linguistic but also conceptual, as professional terminology often failed to translate in ways that were both culturally and semantically meaningful. This reflects longstanding critiques of occupational therapy’s inconsistent and obscure professional language (Creek, 2006; Lycett, 1991). These challenges are further compounded by differences in health-related discourse across cultures, with mental health difficulties in Somali contexts often articulated through physical symptoms rather than the psychological language that underpins clinical practice (Linney et al., 2020).
The theme from cultural (in)competence to cultural humility identified a key enabler, namely the adoption of relational and reflective approaches aligned with cultural humility rather than cultural competence. Participants described varying levels of confidence when working cross-culturally, with some expressing hesitation due to perceived lack of cultural knowledge. Others, however, emphasised the importance of building relationships over time and co-leading interactions with communities. These findings align with critiques of client-centred practice that call for occupational therapists to reflect on their own social positions, including their gender, ethnicity, socio-economic status, sexual orientation and spiritual beliefs, and to understand how these may affect therapeutic relationships. Our findings support collaborative relationship-focussed practice that is contextually relevant, nuanced, safe and promotes rights-based self-determination (Restall and Egan, 2021). Participants also highlighted the value of diverse teams in supporting culturally responsive practice. Team diversity enabled shared reflection on cultural nuances and reduced individual pressure to ‘get it right’, suggesting that cultural humility is not solely an individual attribute but a collective professional responsibility.
In the short term, occupational therapists can take several immediate steps to improve cross-cultural practice. These include using clear, accessible language to explain the role and scope of occupational therapy to both service users and referrers, and prioritising relationship-building as a core component of intervention rather than an optional precursor. Hammell (2009) proposes including occupations that foster belonging and contributing as a focus for practice. Malfitano et al.’s (2019) scoping review exploring collectivist orientations within occupational therapy concluded that the field needs to further develop knowledge and practices addressing injustices, which are grounded in a collectivist epistemology. Similarly, Tsatsi and Plastow (2021) highlighted the occupational need for interdependence, in their participatory action research with Sepedi people with enduring mental health problems in South Africa.
Therapists should work collaboratively with interpreters, recognising their role in supporting shared understanding rather than solely translation, and remain attentive to how professional terminology is conveyed across languages. Adopting a stance of cultural humility may support more meaningful engagement than attempts to achieve cultural competence. Drawing on the strengths of diverse teams and creating space for shared reflection can further enhance confidence and responsiveness in practice. Together, these actions require minimal structural change but have the potential to improve access, relevance and equity within occupational therapy services
Strength and limitations
The World Café offered several strengths when engaging with occupational therapists, particularly in its ability to foster collaborative dialogue and collective knowledge-sharing across different practice areas. Its informal, café-style format helped to reduce power dynamics, encouraging broader participation and supporting authentic conversations. The method also aligned closely with occupational therapy values of collaboration, participation and co-production. However, the participatory ethos occasionally raised expectations for immediate change, necessitating careful management of participants’ hopes and clarifying the project’s scope. While inclusivity was prioritised, there remained a risk that some conversations lacked depth, particularly when discussions reflected limited professional insights. In addition, senior occupational therapists could still influence the direction of dialogue, despite the egalitarian intentions of the method.
The use of static groups rather than rotating participants may have limited the diversity of opinions expressed, as participants could have been influenced by dominant voices within their small groups. However, the level of engagement may have mitigated this limitation.
Conducting the World Cafés virtually via Microsoft Teams made the study accessible to a broad range of participants, minimised geographic limitations and provided a safe space for discussing sensitive topics. One limitation is that participants did not provide feedback or validation on the themes identified, although we have presented findings at community events with occupational therapists and Somali community organisations. The use of convenience sampling limited the diversity of participants.
Conclusion
This research provides valuable insight into occupational therapists’ experiences of working cross-culturally with members of the Somali community in the UK. Although we asked them about working with this specific group of people, the findings speak to a range of factors that impact occupational therapy practice in CALD settings. Our findings sparked our own critical reflection and highlighted the work we need to do within our professional culture as occupational therapists. This work includes grappling with the thorny issue of language and terminology within the profession, and the way in which we communicate our role and scope of practice to others. We believe that this work will make our services more accessible, relevant and culturally safe.
Key findings
The language we use to describe what we do may limit understanding about the role and scope of occupational therapy in the Somali community and among other health professionals.
Occupational therapists are still predominantly using a cultural competence model, whereas Somali community prefer a cultural humility model.
There is a need to adopt a more inclusive and collectivist approach to occupational therapy.
What the study has added
This study highlights the importance of cultural humility, effective communication and inclusive practices in occupational therapy, emphasising the need for therapists to reflect on cultural nuances and adapt their approach to diverse communities.
Footnotes
Acknowledgements
We wish to acknowledge all the occupational therapists who took part in the study, and the members of our Research Steering Group who have guided our approach to the research process.
Research ethics
London South Bank University Research Ethics, ETH2324-0084.
Consent
Informed consent to participate was obtained from participants and the consent was both written and verbal.
Patient and public involvement data
Patient and Public Involvement in the research was included at all stages of the research including development of the research focus and questions, monitoring of the progress of the study and in reporting of the submitted research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Royal College of Occupational Therapist Foundation Grant £ 93,662.
Contributorship
AA Co produced the design of the study, facilitated conversation cafes, analysed data and co-wrote the paper.
CV Co produced the design of the study, recruited participants, facilitated conversation cafes, analysed data and co-wrote the paper.
FH managed the research process, facilitated conversation cafes and co-wrote the paper.
EN Co produced the design and the study and critically reviewed the paper.
NP Co produced the design of the study, analysed data and co-wrote the paper.