
Abstract
Introduction
There is limited understanding of the cultural needs of diverse Black and Minority Ethnic populations such as South Asian older adults, which may be perpetuating occupational injustices and health inequalities faced by these groups. Although cultural considerations are intrinsic to person-centred occupational therapy and increasingly relevant to the changing landscape of health and social care, the profession is criticised for its western-centric focus. This study aimed to gain understanding of the current cross-cultural issues in supporting South Asian older adults in the UK, as perceived by occupational therapists.
Method
A constructivist qualitative design supported by thematic analysis was used, involving seven occupational therapists in the United Kingdom who participated in semi-structured interviews via Skype/telephone.
Findings
Cross-cultural issues were illustrated through the following themes: ‘when the barriers go down’ – cultural mismatch in individualist vs. collectivist worldviews; ‘invasion of the family home’ – cultural inappropriateness of standard interventions; and ‘I go into every assessment assuming nothing’ – recognition of and response to challenges.
Conclusion
This study provides insight into cross-cultural issues in occupational therapy for South Asian older adults, revealing a gap between theory and practice in integrating cultural humility. It highlights the need for a more inclusive, person-centred approach to support culturally diverse populations.
Keywords
Introduction
Within the United Kingdom (UK), there is an increasing culturally diverse and ageing older adult (65+) population (Office for National Statistics, 2012, 2017). Black and Minority Ethnic (BME) people are found to have poorer health outcomes than the general non-BME population as indicated within the Marmot Review (Marmot et al., 2020), and BME older adults in particular are disproportionately afflicted by more health inequalities compared to other groups (Davies, 2011). This ‘hard-to-reach’ population is underrepresented in clinical research, is less likely to access care services, and presents unique complexities compounded by both heterogeneous cultural differences and older age (Liljas et al., 2017).
According to UK census data (ONS, 2012), South Asians (Indian, Pakistani, and Bangladeshi) constitute the largest and fastest-growing BME group in the UK. The group is projected to burgeon from 4.9% of the UK population in 2011 to 10.8% in 2051 (Lievesley, 2010). South Asian older adults, compared to the general non-BME UK population, are known to be at higher risk of both physical and mental health-related chronic conditions including hypertension, diabetes, and vascular dementia, all of which are associated with poorer quality of life (Krishnagiri et al., 2012; Seabrooke and Milne, 2009).
South Asian older adults are also known to delay accessing healthcare services relative to the rest of the UK population (Giebel et al., 2015). Moreover, their lower uptake of care is associated with cultural discrepancies between provider and client (Surood and Lai, 2010), which is likely an issue amongst a predominantly White British (79.2%) healthcare workforce in the UK (NHS Digital, 2020), where there is a lack of understanding of their health-related cultural needs (Fenton and Draper, 2014).
Taking account of a person’s culture is particularly important to occupational therapists as it is a key component of models within the profession, for example the person–environment–occupation dynamic to promote health and wellbeing (Castro et al., 2014; Turpin and Iwama, 2011). Moreover, occupational therapy strives for an ‘occupationally just’ world (Durocher, 2017: 8–16) that postulates the right to access culturally relevant occupations for every individual or group, promoting the equity and empowerment of marginalised populations in particular.
Paradoxically, occupational therapy has been critically scrutinised for its individualist ethnocentrism – the biased focus on western values in its approach – that could arguably be perpetuating the occupational marginalisation of culturally diverse communities (Whalley-Hammell, 2017). This is pertinent to South Asian older immigrants who are likely to identify more strongly with collectivist values and are already at risk of occupational injustices and health inequalities (Davies, 2011; Giebel et al., 2015; Krishnagiri et al., 2012). Furthermore, it is unclear how well occupational therapists are currently meeting this problem in practice. Therefore, this study sought to explore the experiences of occupational therapists in providing occupational therapy to South Asian older adults in order to provide a better understanding of cross-cultural issues and how these might be addressed.
Literature review
Despite growing awareness in the UK and internationally of the need to support BME populations in health and social care (Dawson et al., 2018; NHS England, 2018) that includes a call for stronger action in the NHS Long Term Plan (2019), it is still a largely under-researched area and health inequalities in diverse care settings remain (Fenton and Draper, 2014; Krishnagiri et al., 2012; Salway et al., 2020). Furthermore, there are currently no existing studies exploring the culturally specific needs of the population in terms of occupational therapy service provision. One study, by Krishnagiri et al. (2012), highlighted occupational engagement patterns unique to South Asian older immigrants, but only on a non-clinical day-to-day basis with healthy participants. There is extensive literature covering occupational therapy interventions for older adults, but the populations are predominantly westernised and/or Caucasian (Barney and Perkinson, 2016).
Cultural considerations are essential to inclusive and person-centred practice, as conveyed in the current WFOT Position Statement on Diversity and Culture (2010), which itself also aligns with human rights legislation (United Nations, 1948). This is reflected in Royal College of Occupational Therapists (RCOT) practice guidelines (2015) and in major models of practice used in occupational therapy (Turpin and Iwama, 2011). Growing recognition of the complex and evolving nature of culture in the profession led to the birth of the ‘cultural humility’ approach to maximise culturally sensitive practice (Castro et al., 2014; Whalley-Hammell, 2013). In response to the more conventional ‘cultural competence’ perspective that is criticised as reductionist (Whalley-Hammell, 2013), cultural humility involves embracing the complexities of culture as it asserts that cultural differences are multi-faceted and situated within the provider–client dynamic, which also encourages critical self-reflection. Furthermore, it highlights the importance of context and the re-alignment of power imbalances to facilitate inclusive participation that empowers those from culturally diverse backgrounds.
However, the process of actualising cultural humility in occupational therapy remains unclear (Derawsheh et al., 2015). There are discrepancies in how the term is used, and there is little evidence showing how well this approach has been integrated in practice (Whalley-Hammell, 2013). Occupational therapy is criticised for being heavily rooted in western ideology, where practice models, assessment tools, and interventions that are widely used amongst older adults are biased towards promoting independence (Turpin and Iwama, 2011; Wales et al., 2016). It is therefore problematic when applied to people from more collectivist cultures, including South Asian older adults, who value interdependence more (Giebel et al., 2015; Krishnagiri et al., 2012). In fact, parallels have even been drawn between the hegemonic Eurocentrism of occupational therapy and historical colonialism (Emery-Whittington and Te Maro, 2018). The profession itself may therefore be ironically perpetuating the occupational injustices that ethnic minority groups may be at risk of, which calls for the need for a ‘decolonisation’ of occupations. This is increasingly relevant to the changing landscape of the profession, where occupational therapists have a growing role in ensuring equity and health promoting in diverse settings to address occupational injustices amongst marginalised populations including BME older adults (RCOT, 2017).
In fact, research suggests that South Asian older adults experience various cultural barriers in accessing both mental and physical health services in western countries (Giebel et al., 2015; Horne and Tierney, 2012; Surood and Lai, 2010). Some of these factors include differences in health beliefs and behaviours, family dynamics, culture of care, religious practices, acculturation, and language differences (Krishnagiri et al., 2012; Surood and Lai, 2010). This may be further complicated by the increased risks associated with older-aged immigrants related to cultural identity, cultural dissonance, loss, and discrimination (Krishnagiri et al., 2012). However, the majority of these studies are either not specific to occupational therapy, or the emphasis is on client factors such as barriers to care, rather than issues encapsulating the therapeutic dyad between clinician and client, and broader contexts that appear to align with the cultural humility perspective (Whalley-Hammell, 2013). Seeking further understanding of the cross-cultural issues in occupational therapy with South Asian older adults could prove illuminating on how occupational therapists are currently integrating cultural humility into clinical practice, to enable occupational justice for the population.
Therefore, this study aims to explore the cross-cultural issues perceived by occupational therapists in supporting South Asian older adults in the UK.
Methods
Design
Thematic analysis was used in this phenomenological study to explore occupational therapists’ perceptions of cross-cultural issues in supporting South Asian older adults (Braun and Clarke, 2013). This constructivist qualitative approach embraces complexities and subjectivities of the participants’ unique perspectives, taking account of contextual influences such as westernised statutory services and the clinician’s culture. It also aligns with the cultural relativist standpoint relevant to the study and the values of occupational therapy (Iwama, 2007).
Reflexivity was an important aspect of the research process and was ensured through regular use of a reflective journal and critical discussion with supervisors (Braun and Clarke, 2013). The researcher’s bicultural Chinese-Canadian background and experience with different cultures may have facilitated certain insights in stimulating discourse on the topic; however, it was important to bracket the researcher’s own cultural influences and student position through reflexivity to maintain emphasis on the perceptions of the participants (Fisher, 2009).
Ethics
Ethical approval was granted by the Research Ethics Coordinator at Leeds Beckett University. A participant information sheet and consent form were provided, from which written and verbal informed consent was gained from all participants before commencing interviews. This ensured participants’ understanding of the voluntary nature of their participation, along with their anonymity, confidentiality, and right to withdraw. Responsiveness of the researcher during interviews was important in preserving emotional integrity, for example by providing validation and reassurance when participants discussed self-perceived weaknesses in dealing with cross-cultural issues (Braun and Clarke, 2013). This study was conducted in partial fulfilment of an MSc Occupational Therapy degree with no other conflicts of interest.
Participants
Participants (Table 1) were recruited electronically by invitation via purposive and snowball sampling through the Royal College of Occupational Therapists’ Older People Specialist Section (RCOT-SS OP) and LinkedIn. All participants self-screened to meet the inclusion criteria stipulating Health and Care Professions Council (HCPC) registration, western non-BME ethnicity, having practised in the UK in the past two years, and having experience providing occupational therapy to first- or second-generation South Asian older adults. The exclusion criteria omitted those with close affiliations with South Asian culture for the purpose of examining the specific cross-cultural dynamic.
Participant information.
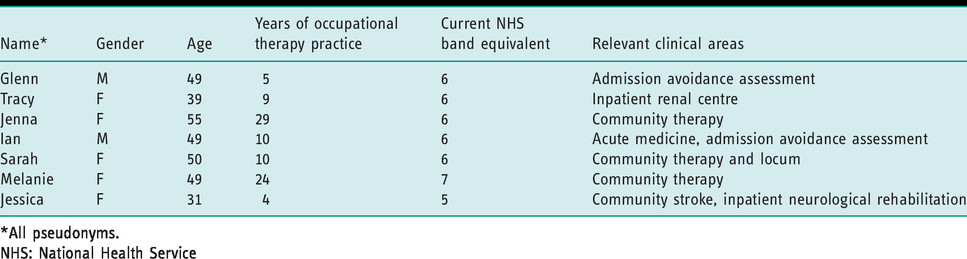
*All pseudonyms.
NHS: National Health Service
Data collection
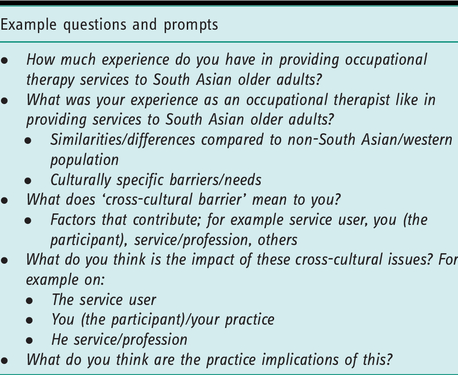
Semi-structured interviews were conducted, accompanied by the use of an interview guide (Table 2) with prompts to increase consistency. The prompts were flexible and encouraging of open discussion (Braun and Clarke, 2013). The main topics included perception and understanding of cross-cultural issues, their approach in response to this, and practice implications. Skype and telephone interviews were used as they were time-efficient and readily accessible to the working practitioners living across the UK. Two participants chose to be interviewed over Skype with video, and the other five via telephone. Interviews ranged from 30 to 50 minutes in length. They were digitally recorded with consent and transcribed verbatim. Field notes and reflective notes were documented after each interview, which captured researcher influences.
Example questions from the interview guide.
Data analysis
Thematic analysis of the data was conducted according to Braun and Clarke’s six-phase guide (2006) to identify the final themes that convey the participants’ perceptions of the explored phenomenon. Manual transcription aided data familiarisation. Inductive thematic analysis was conducted, where codes were generated line-by-line in a bottom-up manner, which is appropriate in exploring new perspectives. Themes were then identified through interpretation on a latent level to draw connections with the underlying conceptualisations and theory relevant to culture and occupational therapy practice, in congruence with the study’s constructivist paradigm (Braun and Clarke, 2006). Data saturation was evident from the repeating patterns of themes identified, and reinforced by the sample size (n = 7), which is sufficient for interview-based projects (Braun and Clarke, 2013). Researcher reflexivity was supported by simultaneous reflective note-taking, which documented critical reflections of thought processes, reactions, and the researcher’s own cultural influences (Braun and Clarke, 2013). Furthermore, the credibility of coding, themes, and overall findings was strengthened by expert peer-review and discussions with experienced research supervisors.
Findings
This research explored the cross-cultural issues perceived by seven occupational therapists (five female and two male) from across the UK in working with South Asian older adult clients. Participants (pseudonyms used) have clinical experience ranging from 4 to 29 years across a variety of clinical settings (Table 1). All participants expressed enthusiasm and openness in discussing the topic, which may not be representative of other occupational therapists; nevertheless, the challenges they experienced despite their motivation to support the cultural needs of the population are helpful in furthering understanding of the phenomenon. Moreover, their confidence in their cultural knowledge surrounding the population varied, and the majority had limited training in cultural issues.
Thematic analysis revealed three major themes that captured the occupational therapists’ perceptions of cross-cultural issues when supporting South Asian older adults. These are supported by verbatim quotes, and further explained in the discussion section.
When the barriers go down
All participants spoke about a different culture of care involving more interdependent family roles common amongst South Asian older adults compared to that of westerners. This contrasted with occupational therapy services, which often promote independence. The collectivist versus individualist cultural mismatch was therefore found to be a significant cross-cultural barrier to providing meaningful support. Glenn stated that ‘[there are] expectations that only the younger members of the family just … naturally take over the care of an elder … there is not that same expectation [as with Western cultures] for an elder to be as independent, while Tracy suggested that it was ‘difficult to do any functional assessments … that would be of any meaning to them … because when they’ve got unwell as older adults … [they] get cared for’. In terms of discharge-planning, ‘families get to a point where they can’t cope any longer’ (Glenn), as they are often reluctant to accept extra-familial support options including 24-hour placements and packages of care. ‘When we start talking [about] social care, that’s when the barriers go down… the family does that and that is part of their culture’ (Glenn).
Promoting independence, particularly in personal care occupations, is a central tenet of the profession. However, this may not be a meaningful occupation to all. For example, ‘when you go in to do rehab and get them to wash and dress themselves, they want things to be done for them … so that’s a barrier’, Melanie stated. Subsequently, the need to find a compromise is perceived to be challenging. That’s the culture, so we need to respect that … but at the same time, it’s getting that balance of getting them to understand they’re doing this … in order to get their function back … you have to adapt therapy and treatment and the functional tasks to do things as they normally do it rather than how we would do it in our culture. So yeah, that’s a little bit of a challenge. (Jessica)
Invasion of the family home
All participants described some cultural inappropriateness of the occupational therapy interventions they usually provide, particularly in the context of South Asian older adults’ physical and social living environments, to which interdependent family involvement is central. Tracy felt that she was often ‘giving information they don’t necessarily wish [for]’. You try to be as minimal as possible because it’s like … an invasion of the family home!… They’ve got grandchildren using the toilet, you can’t issue a Mowbray or something like this … cause you’re trying to kind of think of the other members in their family. (Tracy) There’s no capacity for modifications or it’s difficult putting in equipment … particularly if they need downstairs living … because they have extended family living in such small properties. (Melanie) They randomly go to stay with another daughter … they seem to be able to choose which family member they go and stay with. (Melanie)
Washing and dressing is another example of an activity of daily living that families may prefer to support themselves, which renders external packages of care unsuitable. This may also be influenced by cultural practices such as religious ablutions and codes of dress such as Sikh turban-wrapping, which participants describe a lack of familiarity with.
I go into every assessment assuming nothing
A cultural gap was evident to all the participants when providing occupational therapy to South Asian older adults and their carers, which is recognised as a challenge that needs addressing. It appears that cross-cultural barriers are attributed to the profession’s overly western-centric approach. You know [occupational therapists] try to find what’s meaningful to be independent … but I don’t know if that’s meaningful … they just appreciate ‘oh you’re older, you’re more into [being] interdependent or dependent on your family’ … so it can be hard trying to work as an OT [occupational therapist] with that. (Tracy) I was getting [a Sikh patient] to do an attention task, alternating between male and female names … then he explained that in his culture, men and women’s names are the same … he couldn’t do it because it didn’t make any sense. A lot of the assessments are based on western culture. (Jessica)
Nevertheless, in order to effectively support the population, participants stressed the importance of an ‘open’ and equal approach that embraces individual differences. I suppose it’s just making sure that they’re able to do what they want to do … same with every patient – you’re setting goals that they want to be able to achieve. From that respect, it kind of isn’t really any different. It’s just that their goals might be quite different to a British culture person’s goals. (Jessica) I’m learning all the time … and not trying to impress my sort of western background on them … I try to treat people all the same … I try to let the patient and the family speak … It’s a very open approach … I go into every assessment assuming nothing, ‘cause things can come with a bit of a surprise to you. (Glenn)
Discussion
This study is a snapshot in time showing how occupational therapists are meeting the challenge of cultural relevance in practice, particularly in the current UK context. This is revealed through the occupational therapists’ perceptions of cross-cultural issues in supporting South Asian older adults, captured in three major themes: ‘when the barriers go down’; ‘invasion of the family home’; and ‘I go into every assessment assuming nothing’.
The meaning and relevance of culture in people’s lives is intrinsic to occupational therapy in enabling people to engage in occupations that are meaningful to them for optimal health and wellbeing (Iwama, 2007). Indeed, some espouse that ‘occupation’ is both a means and an end within occupational therapy and is itself a sociocultural construct (Whiteford and Wilcock, 2000). There is growing awareness of the ever-shifting complexities of culture in occupational therapy practice (Castro et al., 2014). Subsequently, there is a need to understand and examine how cross-cultural issues are addressed in supporting marginalised groups from an increasingly diverse clientele, particularly South Asian older adults in the UK, who face significant health inequalities and thus occupational injustices (Durocher, 2017; Iwama, 2007; Krishnagiri et al., 2012). This study suggests some examples regarding how these challenges are manifested in clinical practice, echoing philosophical and theoretical literature that questions the very foundations of the profession (Whalley-Hammell, 2013). Occupational therapy and even the conceptualisation of ‘occupation’ itself is criticised for its ethnocentric focus on independence and autonomy, characteristic of the hegemonic western societies that it is derived from (Whalley-Hammell, 2017). Therefore, there are ethical and therapeutic concerns about its approach towards more collectivist BME societies such as those originating in South Asia, which this study exemplifies.
The first theme illustrates the tension in worldviews, which the western therapists perceive to be a significant cross-cultural barrier in supporting the population that they identify difficulty with. This is in congruence with literature theorising the irrelevance of the profession’s ‘universal’ approach in the face of unfamiliar cultural needs (Whalley-Hammell, 2013). Iwama (2007) portrays this ‘cultural irrelevance’ as a threat to the sustainability of the profession as it goes against the very grain of the ‘holistic’ and ‘person-centred’ approach it promotes. Moreover, these findings provide insight into the clinical implications of cross-cultural issues when supporting the population in occupational therapy practice, reinforced by concrete examples. The findings also align with previous literature on South Asian older adults that conveys cross-cultural barriers to general healthcare, for example contrasting family dynamics and health beliefs, and occupational needs unique to the group (Giebel et al., 2015; Horne and Tierney, 2012; Surood and Lai, 2010). Where cultural incompatibility between provider and client is already associated with lower access to western-based care (Surood and Lai, 2010), culturally irrelevant occupational therapy interventions are potentially iatrogenic, which may perpetuate existing health inequalities per se (Castro et al., 2014).
In addition, this study sheds light on the ironic reality of occupational injustices for South Asian older adults within occupational therapy services, despite intentions for the contrary (Durocher, 2017). The population may inadvertently experience occupational marginalisation as their opportunities to engage in meaningful occupations are restricted due to the invisible norms of a dominant western society, the Eurocentric framework of which has even been likened to colonialism (Emery-Whittington and Te Maro, 2018; Whalley-Hammell, 2013). The repercussions of this emerge in the second theme, ‘invasion of the family home’, which also alludes to occupational alienation risk, as occupational therapy interventions may obstruct meaningful occupations in the home environment (Durocher, 2017). The home is a particularly important interdependent social space that shapes occupational possibilities for South Asian families, in which shared occupations, roles, and identities are nurtured (Krishnagiri et al., 2012). This includes feeding rituals, religious practices, and the venerated and cared-for elder role (Tummara-Narra and Sathasivam-Rueckert, 2013), as described by participants. Occupational therapy in western countries is known to focus heavily on maximising safety and independence in older adults’ home environments (Durocher, 2017), which occupational therapists therefore felt to be an unwelcome ‘invasion’ that could impede interdependent family participation for the population. Nevertheless, occupational injustice is ultimately determined by the individuals themselves, so interpretations should be made cautiously.
This study highlights a need to adopt a more holistic perspective that incorporates cultural needs in occupational therapy practice, in order to enable people of diverse backgrounds to fulfil their actual wants and needs in accordance with their unique sociocultural milieu (Whalley-Hammell, 2017). Fitting to those of more interdependent cultures, it is within an occupational therapist’s remit to support not only individuals, but also families and populations, to facilitate collective occupations. Perhaps there should be a shift in focus towards engaging meaningful family co-occupations rather than individual performance for more collectivist societies. This is relevant to the emerging role of occupational therapists in supporting marginalised groups, including BME older adults in diverse settings (RCOT, 2017). However, the struggles perceived are reflective of growing tensions in occupational therapists’ professional and moral identities due to traditional practice being restricted by the overarching socio-political and economic context (Durocher, 2017). This could be considered an occupational injustice for therapists themselves. Western hegemony and National Health Service pressures for discharge in the UK are examples of factors that may undermine therapists’ capacity to deliver truly person-centred – and hence culturally appropriate – services.
The occupational therapists in this study are trying hard to make sense of these cross-cultural issues and are recognising the sheer complexities of this challenge, which the third theme, ‘I go into every assessment assuming nothing’, conveys. The need for an open approach by ‘assuming nothing’ is recognised. This is in contrast to the more traditional concept of ‘cultural competence’ that entails a more reductionist understanding of a specific cultural group’s values and beliefs, while narrowly focusing on ethnicity and assuming that culture is knowable. ‘Cultural humility’ is the contemporary version of this approach, and is associated with strong clinical rapport and therapeutic progress (Hook et al., 2013). It constitutes lifelong learning and embraces the multi-faceted and ever-evolving nature of culture as influenced by critical race theory (Iwama, 2007). It takes into account various forms of intersectionality, including gender, class, migration history, acculturation, language, and the complexities of older age relevant to the population, all of which may present multiple challenges, which participants discussed. Furthermore, this perspective acknowledges that cross-cultural issues lie within the therapist–client partnership and the socio-political context, rather than the client themselves (Whalley-Hammell, 2013), encouraging critical self-reflection.
Conversely, although addressing power imbalances and privilege is also fundamental to the cultural humility approach, there was limited discussion of this. This may therefore require further research to explore it in more depth. Moreover, despite evidently trying their best to understand and address cross-cultural issues in supporting the population, participants expressed a lack of confidence in this and described it as a ‘challenge’. This may indicate that they have not been sufficiently equipped for this, which is in congruence with the limited training they reported. Nevertheless, there was evidence of cultural humility particularly from their critical reflection of the profession and acknowledgement of population heterogeneity as discussed above. In fact, participants were open in discussing the difficulties they experienced, which itself is fundamental to the cultural humility approach. It is even more admirable considering the difficulties surrounding discourse in cross-cultural issues (Castro et al., 2014), and their honesty and reflective stance is greatly appreciated in this research. This could also be helpful for others to learn or receive validation from, and could serve as an impetus for further discussion and action.
In general, there is limited understanding of culture, including inconsistencies across the profession in how it is defined, which may have wider ethical, socio-political, and economic repercussions on diverse populations such as South Asian older adults (Castro et al., 2014). Evident in the findings, a gap between theory and practice remains (Derawsheh et al., 2015), and it is currently perceived that the onus is on the therapist to address these issues at the client-level despite the lack of concrete guidance (Whalley-Hammell, 2013). However, critical examination of structural and ideological barriers is also necessary (Fisher-Borne et al., 2015; Iwama, 2007; Whalley-Hammell, 2017) to facilitate transformation on the micro, meso, and macro levels appropriate to tackling these deep-rooted occupational injustices (Restall and Ripat, 2008; Whalley-Hammell, 2017). For instance, third-sector collaborations, post-graduate training initiatives, and policy change through the RCOT to enhance culturally sensitive practice could address insufficient education in guiding culturally sensitive practice (Derawsheh et al., 2015), and qualitative studies like this are important in informing the development of such interventions (Horne and Tierney, 2012). Furthermore, a more systemic approach is particularly relevant to contemporary occupational therapy, which strives to innovatively meet changing health and social care needs (RCOT, 2017). An example of this is promoting good health practices for marginalised populations such as South Asian older adults, including those who have not even accessed support in the first place (RCOT, 2017). Occupational injustices could thereby be addressed more effectively, contribute to the ‘decolonisation’ of occupations, and ensure equitable access to meaningful occupational engagement for all (Castro et al., 2014; Whalley-Hammell, 2017).
Study limitations
Limitations of this study included the influence of the researcher on the interpretation of the perspective presented, such as her limited experience as a student during the research process and bicultural background, though this was taken account of reflexively via journaling and supervision throughout. Nevertheless, the researcher’s Asian heritage, evident in surname through electronic communications and video, which a few participants asked about, may have influenced what participants shared due to caution related to the controversial potential of discussions around culture (Castro et al., 2014). Although video feedback may have influenced the interviews compared to voice-only calls, similar overarching themes were reached. Moreover, all participants conveyed an interest in and openness to discussing the topic, sharing experiences from solely physical-oriented healthcare settings. A larger sample that includes differing attitudes and mental health contexts may provide a more comprehensive analysis to capture the full extent of the issue and increase research transferability. Regardless, findings should be interpreted carefully due to heterogeneity within the population of South Asian older adults (Krishnagiri et al., 2012). In addition, further participatory research on the narrative of the clients and their carers/family members would be essential for a thorough understanding of the cross-cultural issues experienced.
Conclusion
This study explored the cross-cultural issues perceived by occupational therapists when supporting South Asian older adults in the UK. The findings mirror literature criticising the western focus of occupational therapy, providing evidence of its implications for clinical practice and the challenges faced by occupational therapists (Whalley-Hammell, 2017). These consequences may potentially perpetuate occupational injustices and health inequalities that the complex population already face. This study also demonstrates how occupational therapists are currently meeting this challenge, revealing that a gap between theory and practice remains (Derawsheh et al., 2015), despite the importance of culturally sensitive practice and its increasing pertinence to the changing landscape of the profession and the UK context (RCOT, 2017). This research provides some insight into the barriers that prevent the integration of cultural humility into occupational therapy practice. More person-centred occupational therapy practice and increased critical discourse about culture may enable inclusive participation in meaningful occupations for all culturally diverse populations.
Key findings
There are cross-cultural issues, and implications relating to them, perceived in occupational therapy practice for South Asian older adults. A more holistic, person-centred approach that promotes cultural humility may facilitate more inclusive practice.
What the study has added
This study contributes further understanding of cross-cultural issues in occupational therapy practice for South Asian older adults, highlighting the need for more inclusive person-centred practice to address occupational injustices for culturally diverse populations.
Footnotes
Acknowledgements
The first author would like to thank the occupational therapists who took the time to share their experience and insights, as well as the Royal College of Occupational Therapists Specialist Section – Older People for facilitating access to participants. The first author would also like to thank Dr Angela Murphy and Miranda Thew for their support and supervision of this research.
Research ethics
Ethical approval was obtained from the Leeds Beckett University Research Ethics Coordinator (Reference: 49736) on 14 June 2018.
Consent
All participants provided written and verbal consent before the interviews for this study.
Declaration of conflicting interests
This research was submitted in partial fulfilment of an MSc Occupational Therapy degree.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Contributorship
Nichole Yam was responsible for the development of the research study and design, carried out the methods, applied for ethical approval, and wrote the first draft of the manuscript. Dr Angela Murphy and Miranda Thew provided supervision including continual feedback and support to the first author across the entire research process. All authors contributed to revising the manuscript and approved the final version for publication.