
Abstract
Introduction:
The university of the Free State (UFS) In-Hand Manipulation Assessment Instrument (UFS IHMAI) is a newly developed play-based IHM instrument assessing all components of IHM. With the face and content validity completed, this study aimed to evaluate the construct validity of the UFS IHMAI for 3- and 4-year-old children in Bloemfontein, South Africa.
Methods:
Employing a quantitative methodological design, the study included typically developing 3- to 4-year-old children (n = 220) from 19 Early Childhood Development centres, selected through a two-stage sampling approach. Exploratory factor analysis (EFA), simplified by principal component analysis and varimax rotation, with descriptive statistics, was performed.
Results:
The UFS IHMAI demonstrated strong construct validity, supported by statistically significant Chi-square results, favourable model fit as indicated by the standardised root mean square residual, and high internal consistency reliability reflected by Cronbach’s alpha coefficient. The five-factor solution derived from the EFA grouped subtasks in patterns matching the developmental stages of IHM skills. The descriptive data on the children’s performance across the 12 distinct components of translation, shift, and rotation contextualise age-specific mastery of these movements in play-based tasks.
Conclusion:
The findings confirmed the construct validity of the UFS IHMAI for children aged 3–4 years.
Keywords
Introduction and literature review
In-hand manipulation (IHM) is a multifaceted skill integral to children’s ability to perform everyday tasks, for example, writing, dressing, and playing. IHM involves the movement of objects within one hand without external support, encompassing discrete components such as translation, rotation and shift movements (Exner, 1997; Pont et al., 2008). A conceptual modified classification system for IHM is available, outlining six components, each performed with and without stabilisation, resulting in 12 distinct IHM movement patterns (Pont et al., 2009). However, IHM is a complex phenomenon to assess, influenced by multiple interrelated factors (Exner, 2006, 2010).
Conceptually, IHM movement patterns can be described in isolation. However, in real life, observing IHM during occupational performance is more intricate, as reflected by several assessments described before (Kruger et al., 2021). Early approaches focused on mechanical, singular movements using items such as a pegboard (Breslin and Exner, 1999; Exner, 1993; Pont et al., 2008). Later, functional and play-based tasks were incorporated to elicit the child’s functional performance using items such as scooping beans with a spoon (Pehoski et al., 1997a, 1997b; Visser et al., 2016). More recently, observing IHM within naturalistic and culturally responsive tasks was incorporated, for example, paging through a book (Chien et al., 2010; Raja et al., 2016). However, accurately observing IHM in a naturalistic setting is more complex, as the successful completion of functional tasks often requires the co-activation of different IHM movements. Isolating IHM movement patterns in a functional assessment is more complicated, unless a standardised assessment can guide the therapist in making skilled observations. To ensure that IHM is accurately assessed, a combination of mechanical and play-based activities is necessary to truly elicit the inherent abilities of the child.
Contrary to a single-dimensional client factor such as grip strength, IHM is a learned motor skill mastered through repeated opportunities for practice, alongside the child’s natural maturation. The administration and scoring guidelines must reflect these complexities of skill development. Therefore, clear instructions and practice opportunities must be presented before each task (Exner, 1990). Furthermore, to guide the scoring and interpretation of the child’s performance in the assessment, using developmental indicators becomes essential. However, current literature on the developmental norms of IHM skills remains vague (Kruger et al., 2021; Visser et al., 2014; Visser et al., 2016), which is primarily due to limited empirical research describing the developmental progression of these skills, and the lack of standardised, normative assessments. This limits the clinician’s ability to interpret whether a child’s IHM skill is on par with age-appropriate developmental expectations. Furthermore, subjective interpretation can occur when using instruments lacking structured administration and scoring guidelines. Lastly, an assessment instrument without established psychometric properties, or not commercially available, has restricted clinical use (Kruger et al., 2021).
A recent scoping review (Kruger et al., 2022) suggested that there is no standardised assessment available comprehensively assessing all the components of children’s IHM, that has completed the instrument development process with established psychometric properties and good clinical utility (Kruger et al., 2021). Furthermore, an investigation of current and preferred practices of occupational therapists in South Africa revealed a need for a contextually relevant IHM instrument (Kruger et al., 2022). In response, the development of the University of [removed to ensure blind review] In-Hand Manipulation Assessment Instrument (UFS IHMAI) was initiated, building on previous descriptive studies undertaken using the UFS Checklist (Visser et al., 2014; Visser et al., 2016).
The UFS IHMAI aims to become a ‘standardised, norm-referenced, descriptive, component-based assessment instrument to assess the IHM skills of children in South Africa’ (Visser et al., 2024: 8). A comprehensive and rigorous process underpinned by instrument development theories was undertaken (Benson and Clark, 1982; Boateng, et al., 2018; Kielhofner, 2006; LoBiondo-Wood and Haber, 2014; Polit and Yang, 2016; Rudman and Hannah, 1998). This process included a needs analysis, conceptualisation, instrument design, literature-based item development and expert opinion, initial field testing and item analysis. As part of establishing its psychometric properties, face and content validity studies have been completed (Visser et al., 2024), with construct validity as the next critical step in the ongoing validation of the UFS IHMAI.
Construct validity is essential to verify that the items align with the instrument’s intended purpose and accurately reflect the construct being measured. This current investigation marks the first of a series of psychometric studies on the UFS IHMAI, with inter- and intra-rater reliability to be reported in a subsequent article. The study aimed to determine the construct validity of the UFS IHMAI for 3–4-year-old children in Bloemfontein, South Africa.
Methods
Study design
A quantitative, methodological study design was used. A methodological design is commonly used during the development and evaluation of instruments, and typically progresses through four stages, namely (i) definition of concepts; (ii) formulation of the instrument items; (iii) developing an instruction manual and (iv) determining the instrument’s validity or reliability (LoBiondo-Wood and Haber, 2014). This study represented a component of the fourth stage focusing on determining the instrument’s construct validity.
Study population
Typically developing 3- and 4-year-olds attending Early Childhood Development (ECD) centres in [removed to ensure blind review] formed the study population. Of the 331 ECD centres in Bloemfontein, 178 are registered and 153 unregistered with the Departments of Basic Education (DBE) and Social Development. In South Africa, the DBE oversees the education system (all schools from Grades R to 12), promoting universal access to quality education (Department of Basic Education, Republic of South Africa, 2021; Department of Social Development, Republic of South Africa, 2006).
The number of children aged 3–4 years attending ECD centres was unknown at the time of the study (Statistics South Africa, 2022). An estimated target population of 5296 was based on an average of 40 children per ECD centre, with 8 children per age group (3- and 4-year-old) factored in, considering that children aged 0–4 years can attend. The estimated target population was calculated by multiplying 16 children by 331 ECD centres, resulting in 5 296 children.
The inclusion criteria were 3- to 4-year-old children attending registered or unregistered ECD centres, whose language of teaching and learning was English, Afrikaans or Sesotho, who would understand visual and verbal instructions, and whose parents provided written consent for their child to participate, with the child giving assent. Children were excluded if they had visual or auditory impairments that would prevent them from following instructions, and those with fine motor or hand function challenges that might affect their participation in the assessment.
Sampling
Sampling of the ECD centres: A two-stage sampling approach was applied. First, registered and unregistered ECD centres in Bloemfontein with 10 or more children were conveniently sampled. Subsequently, a probability cluster sampling method was employed to randomly select a limited number of clusters (ECD centres) from the identified pool. Among the 178 registered and 153 unregistered ECD centres, 163 registered and 138 unregistered centres being sampled. In the first round, 40 centres from each group were contacted, yielding responses from 15 centres. In the second round, 25 centres were randomly sampled, with 11 responding. Thereafter, simple random sampling was done in both rounds.
Sampling of the children: After the ECD centres were sampled, parents/guardians received a questionnaire and consent letter to complete at the sampled ECD centres. Children meeting the criteria, as determined from specific questions in the questionnaire, and for whom parental consent was obtained, were included in the study.
A target sample size of at least 260 participants was set to ensure construct validity. This calculation was based on the 13 item sets, totalling 26 items, in the UFS IHMAI, multiplied by 10 (Boateng et al., 2018). In total, 200–300 children would be appropriate for factor analysis (Guadagnoli and Velicer, 1988).
Due to practical considerations, including time, budget constraints and resource availability, only 220 children were eligible for the study, and all were conveniently included. This led to 19 ECD centres being included, with 71 children from unregistered and 149 from registered centres meeting the eligibility criteria.
Measurement instrument
The UFS IHMAI, currently in the refinement stages of development, was used as the data collection method. It consists of an assessment kit, and administration and scoring guidelines containing standardised instructions in English, Afrikaans and Sesotho. Administering the instrument required approximately 30 minutes per child.
The instrument covers all components of IHM (finger-to-palm translation, palm-to-finger translation, simple shift, complex shift, simple rotation and complex rotation both with and without stabilisation). The instrument comprises 13 item sets, each presented in a playful task-based activity. Instructions to the child include verbal and visual guidance, and two opportunities to practise. Contextually relevant activities, for example, dressing, beading or drawing, and familiar materials, for example, coins, pegs and marbles, were used.
For each item set, there are two progressively graded items, denoted by A and B. Items that can assess different components of IHM are further denoted by i, ii and iii, referred to as subtasks, with 39 subtasks in total. Variations exist among the item sets in terms of the opportunity afforded to observe and assess different components of IHM, depending on the nature of the activity. For instance, item 1A allows for the assessment of a single IHM component, whereas subtasks 5Ai and 5Aii enable the scoring of two distinct IHM components within item 5A, due to the co-activation and inter-dependability of skills required to complete the task (see Table 1).
Scoring summary according to in-hand manipulation components and sub-tasks (N = 220).
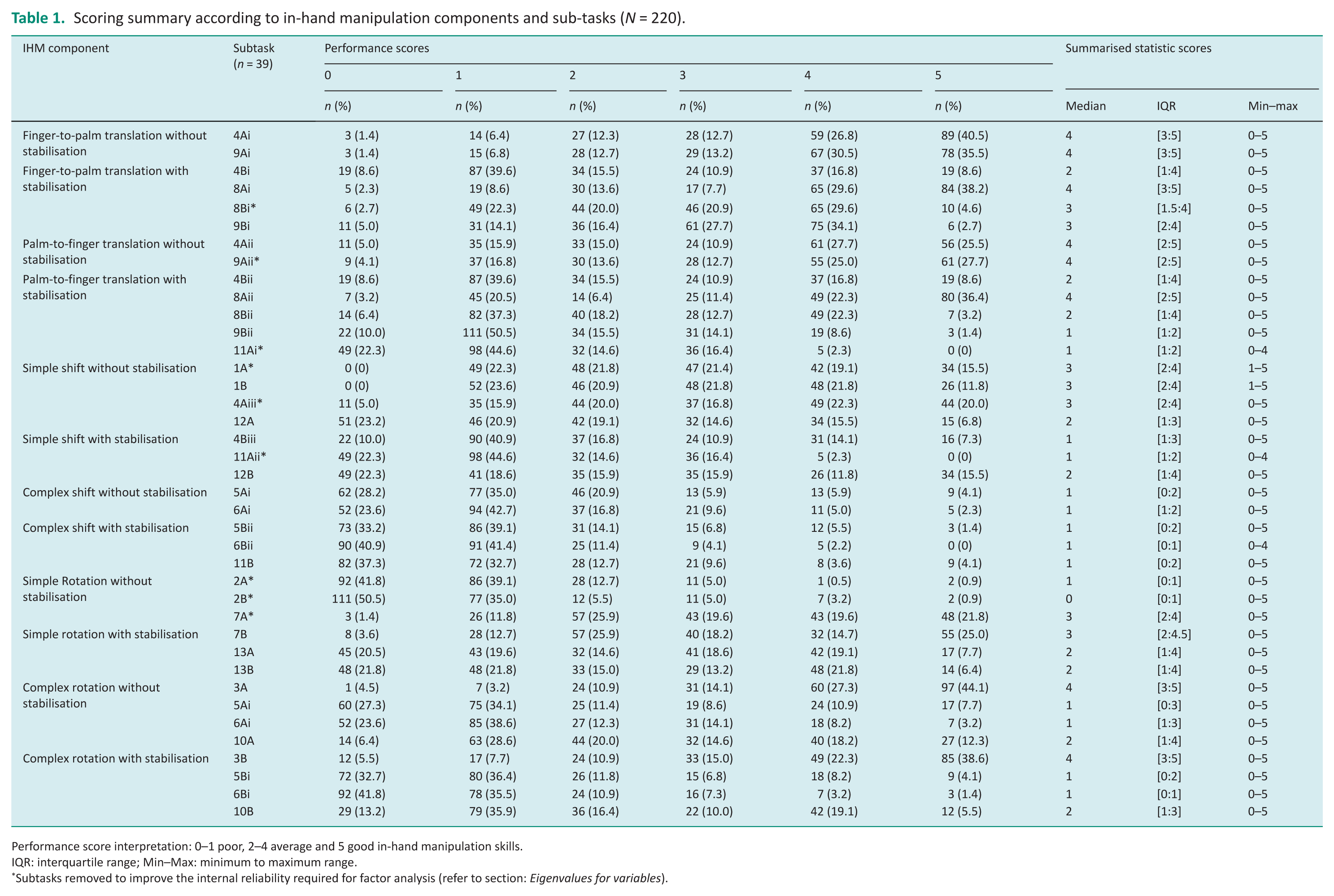
Performance score interpretation: 0–1 poor, 2–4 average and 5 good in-hand manipulation skills.
IQR: interquartile range; Min–Max: minimum to maximum range.
Subtasks removed to improve the internal reliability required for factor analysis (refer to section: Eigenvalues for variables).
For each subtask, a performance score was calculated based on the combination of scores for the child’s ability to complete the task and the quality of their performance, ranging from 0 to 5. A child’s IHM skills were interpreted as either good (a score of 5), average (a score of 2–4) and poor (a score of 0–1; see Table 1).
Pilot study
A pilot study refined logistical aspects of scoring, administration time, item clarity, video recording, and training on the data-capturing systems. Fieldworkers, working in pairs, collected data in both pilot and main studies. From the eligible sample, 14 children (7 per age group) were assessed, allowing all fieldworkers to administer and score children of both ages. Modifications to the administration process included regular breaks, discontinuing assessment for non-cooperation or reluctance, repeating instructions for children with shorter attention spans and discouraging the use of the non-dominant hand. The pilot study data were excluded from the analysis.
Measurement process
After the ECD centres and teachers consented, teachers distributed information and background questionnaires to parents/guardians in hard copy. Low response rates were addressed with reminders and by having the teachers collect the consent forms and questionnaires.
On collection day, venues were arranged at the ECD centres. Child-size table arrangements were considered during the IHM assessment at a child-sized table, as Smith-Zuzovsky and Exner (2004) noted performance could be influenced at adult-sized tables. Administration of the instrument occurred in the child’s home language.
Data collection occurred over the course of 3 weeks by the researchers and trained fieldworkers in bilingual pairs. One fieldworker assessed the child while the other recorded scores on paper. Scoring accuracy was later confirmed using the video recordings before capturing the data on REDCap (REDCap Consortium; Nashville, TN, USA) by the same research pair.
Analysis
Descriptive statistics, including frequencies and percentages for categorical data, and medians and interquartile ranges (IQRs) for continuous (numerical) data, were computed for the whole group. Exploratory factor analysis (EFA) was conducted to describe the construct validity of the UFS IHMAI. EFA is used to investigate a measurement instrument’s underlying factor structure and identify factor organisation from participant responses (Osborne, 2015). Due to the relatively small sample size compared to the number of items, EFA was simplified to principal component analysis with varimax rotation. A scree plot of eigenvalues guided the number of factors; thereafter, internal consistency was evaluated to determine whether the items in each factor measure the same construct.
Items that did not load well on the final factors were discarded and the remaining items were classified into factors by command item content. Internal reliability was assessed with Cronbach’s alpha. Data analysis was performed by a biostatistician using SAS/STAT software (Statistical Analysis System), Version 9.4 (SAS Institute Inc.; Cary, NC, USA; ©SAS, 2016).
Results
Demographic profile
In total, 220 3- to 4-year-old children were included in the study; 100 (45.5%) were 3 years old and 120 (54.5%) were 4 years old. More than half (n = 122; 55.5%) were female and 196 (89.1%) were right-hand dominant. Most children (n = 137; 62.3%) were assessed in English, 65 (29.5%) in Afrikaans and 18 (8.2%) in Sesotho.
Table 1 provides a descriptive scoring summary of the children’s IHM performance. The performance scores are organised according to the IHM components. Each of the 39 subtasks’ performance scores, including the median, IQR, minimum and maximum values, are provided to serve as an introduction guiding the process of construct validity.
No trend of consistent performance was observed in any of the collections of translation, shift and rotation. Instead, performance varied considerably across the different IHM subtasks. When considering the median scores of the 39 subtasks, none of the tasks had a median score of 5, indicating no consistently good performance in the children’s IHM skills. Twenty-four subtasks had median scores of 2–4, reflecting average performance, while 15 subtasks had median scores of 0–1 (poor performance). Regarding maximum scores, items 11Ai, 11Aii and 6Bii were the only tasks where children did not achieve a score of 5. Each of these items had a median score of 1, supposedly being particularly challenging and indicating poor performance among the children.
For the translation components, the children performed average in the finger-to-palm translation with and without stabilisation subtasks, indicated by the average median scores. Eighty-nine (40.5%) children performed well, scoring 5 in item 4Ai. For palm-to-finger translation without stabilisation, all items obtained average median scores. However, in the palm-to-finger translation with stabilisation, only three of the five subtasks obtained average medians. Notably, 111 (50.5%) children performed poorly in subtasks 9Bii.
For the shift components, the children performed average in all five subtasks of simple shift without stabilisation. For simple shift with stabilisation, the median scores ranged from poor to average, except for item 12B obtaining an average median score of 2. Poor performance was observed for both complex shift with and without stabilisation subtasks, as indicated by the poor median score of 1 across all five subtasks. Ninety (40.9%) and 91 (41.4%) children performed poorly in subtasks 6Bii (IQR 0:1).
For the rotation components, the children performed average in all subtasks for simple rotation with stabilisation. For simple rotation without stabilisation, only one subtask had a median score indicating average performance. Again, 111 (50.5%) children performed poorly in subtasks 2B. In the complex rotation with and without stabilisation subtasks, the median scores ranged from poor to average. Of interest, 97 (44.1%) of children performed well with a score of 5 for item 3A, while 92 (41.8%) performed poorly, scoring 0 in subtask 6Bi.
Cronbach’s alpha was calculated for the 39 subtasks, of which nine variables were removed as indicated in Table 1 by an asterisk (*), improving internal reliability. All further analyses were based on the remaining 30 variables. The following results pertain to the construct validity results of the instrument.
Eigenvalues for variables
The scree plot suggested the presence of five factors with eigenvalues exceeding 1, which collectively explained 64.03% of the variance illustrated in Figure 1 (right). Notably, all five factors exhibited eigenvalues surpassing the threshold of 1.0, illustrated in Figure 1 (left), and were retained for further analysis (Hair et al., 1998).
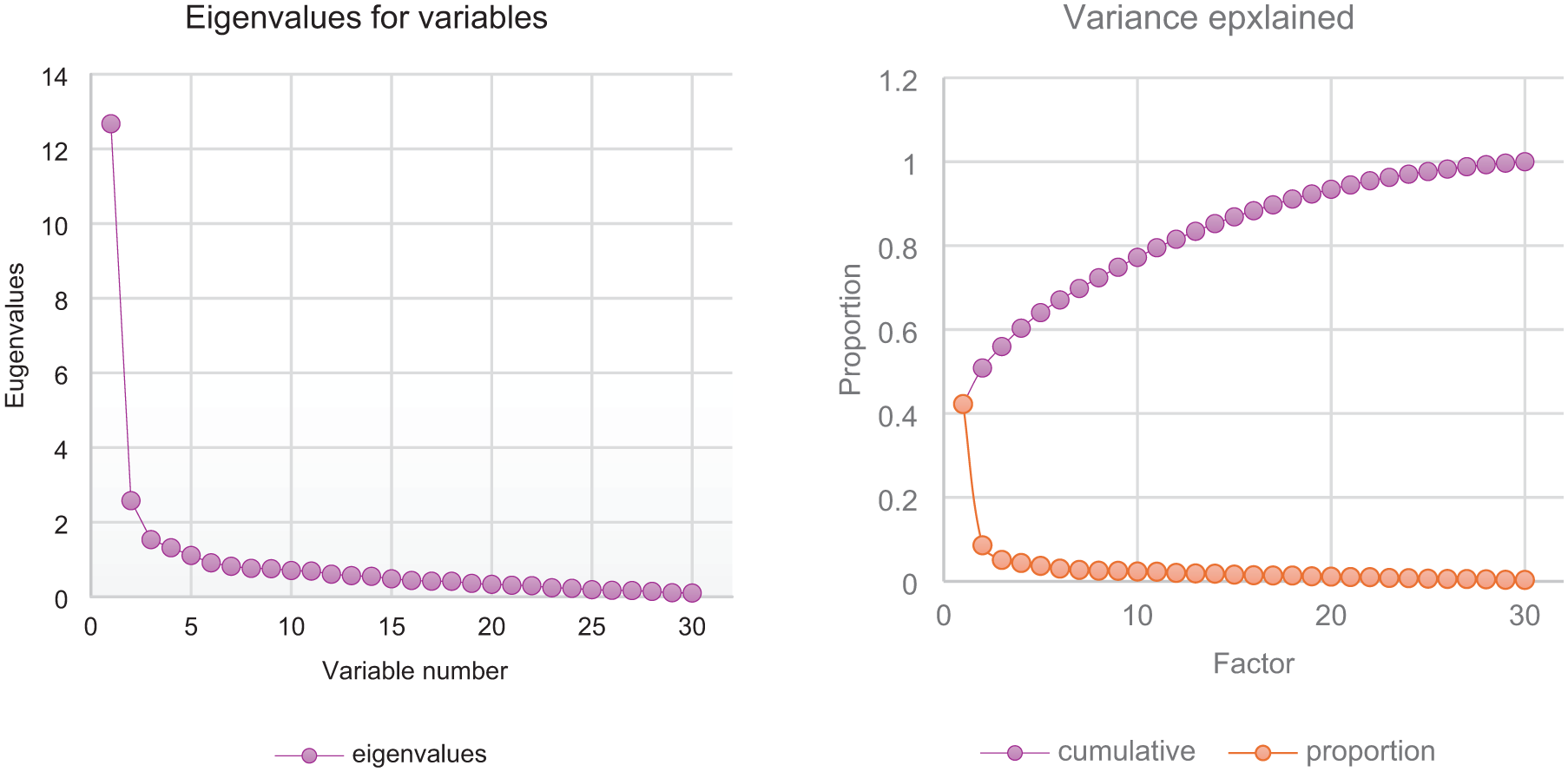
Scree plot of eigenvalues (left) and variance explained (right) for the remaining 30 variables.
Table 2 shows the factor loadings drawn from the varimax rotated factor pattern analysis, namely the 5 factors for the 30 subtasks. The factor loadings ranged from −1 to +1 and are arranged from the highest per factor to the lowest. The values that are highest per column indicate which factor they relate to. The IHM components per subtask are indicated in Table 2, providing guidance and insight into the interpretation and conceptualisation of the identified factors (Osborne, 2015).
Factor loadings per subtasks by means of varimax rotated factor pattern analysis.
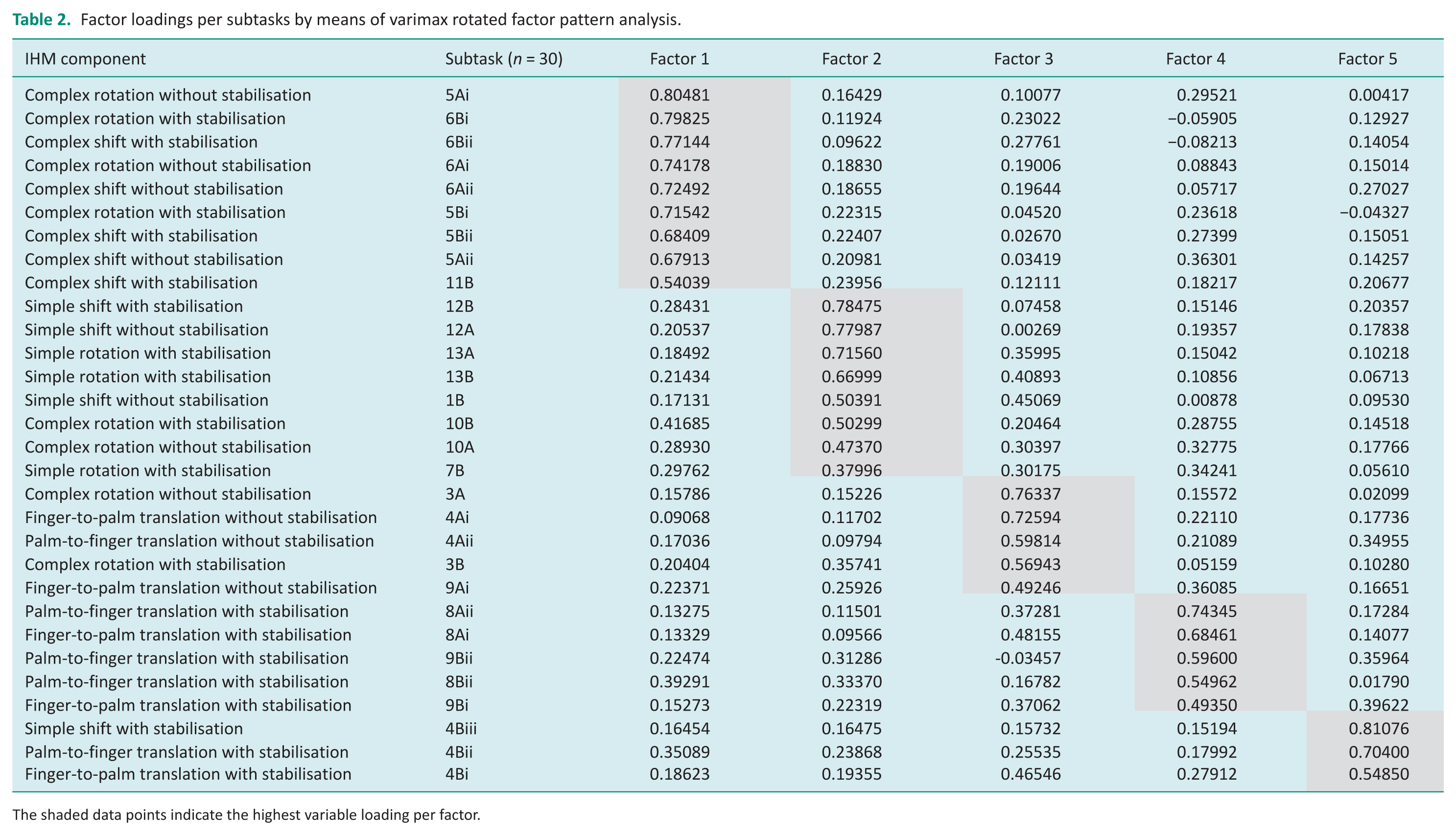
The shaded data points indicate the highest variable loading per factor.
Exploratory structural equation modelling was performed and produced a significant result from the Chi-square test, χ2(45) = 1175.0011, p < 0.0001. Despite this result, it is important to recognise that while this test could be informative in evaluating the overall fit of the model, it does not offer a comprehensive explanation for why a model might not meet its criteria. Additionally, it is acknowledged that Chi-square tests are sensitive, and statistical significance does not necessarily indicate inadequate fit (Barrett, 2007). Hence, the standardised root mean square residual (SRMR), smaller than 0.08 with a precise value of 0.0712, signified a favourable alignment between the proposed model and the actual data (Hu and Bentler, 1999). Furthermore, the favourable SRMR values supported the construct validity of the proposed model (Osborne, 2015), indicating that the model effectively represents the relationships among the measured variables.
Table 3 summarises the factor names and the calculated Cronbach’s alpha coefficient for the five factors, and a total for the entire [removed to ensure blind review] IHMAI. In addition, Table 3 provides a measurement summary of the scoring mode and children’s performance scores. The summary consists of the sum of subtasks encompassed by each factor, as it informs the total achievable score that could be obtained. The median score, representing the midpoint of the data distribution, indicated that half of the children’s collective scores for those subtasks fell below and half above this value, providing a robust measure of central tendency, particularly as there was a skewed distribution of scores. The range values indicate the range of the children’s scores, providing insight into the overall spread and variability.
Factor naming, Cronbach’s alpha coefficient and measurement summary of the scoring model.
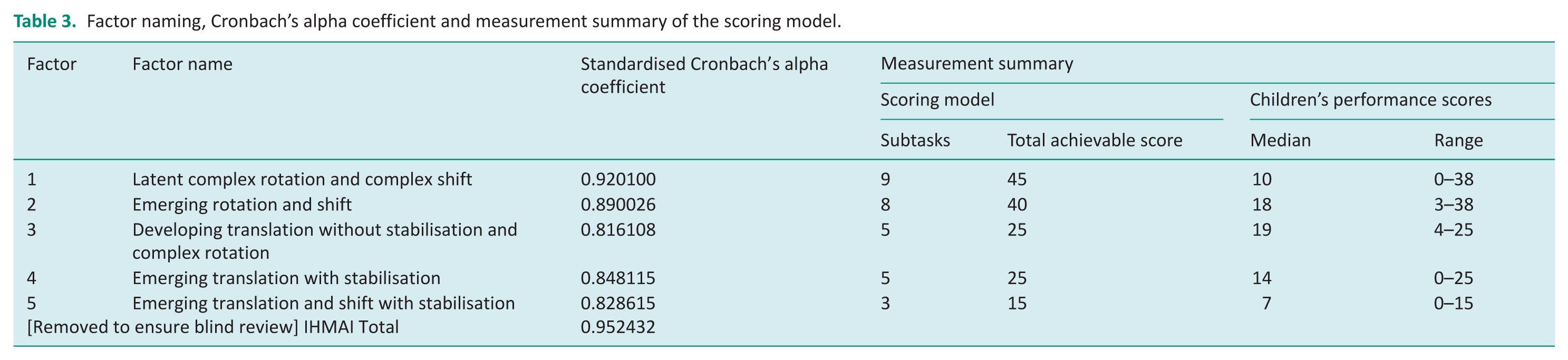
The factor naming was justified based on the following considerations: the IHM skills involved, stage of development, and the relationship between the median and minimum-maximum range. Latency of the IHM skills of complex rotation and complex shift was evident as the median was 10 in relation to a total achievable score of 45. This indicates that half of the children could not obtain a score higher than 10 out of 45. Furthermore, no child was able to achieve the maximum score of 45 for factor 1, with 38 being the best score obtained. Therefore, although this skill occurred to a degree in some children, it was not yet apparent in all children’s performance for this age group.
Emerging IHM skills, referred to in factors 2, 4 and 5, were apparent as the median for each factor was at 18 out of 40, 14 out of 25 and 7 out of 15, respectively. Contrary to factor 1, the children were able to achieve fairly distributed scores in those subtasks. Factors 4 and 5 displayed a maximum score related to the total achievable score, indicating children in this age group who could perform all the subtasks. For factor 2, the maximum score was 38, which was lower than the total achievable score of 40, indicating that there were no children who could perform all the subtasks. The minimum score was 3, confirming that all the children were able to perform some aspects of the subtasks. Hence, all three factors indicated that IHM has started to emerge. However, as it appeared to be difficult for this age group, there was not yet a consolidation of these skills.
Developing IHM skills became apparent in factor 3 with a median of 19 out of 25, indicating that half of the children obtained a score higher than 19 out of 25. For this factor, a minimum score of 4 indicated that all the children could perform some aspects of the subtasks. The maximum score correlated to the total achievable score of 25, indicating that some children could perform all the subtasks. The IHM skills of translation without stabilisation and complex rotation were therefore more developed, but not yet fully mastered, as the majority of all the 3- and 4-year-old children performed well in this factor.
During the calculation of the Cronbach’s alpha, the error variance was 0.09, indicating that the fraction of test scores that were attributable to error was small (Tavakol and Dennick, 2011). As seen in Table 3, respectively, the five factors ranged with an acceptable Cronbach’s alpha coefficient value between 0.82 and 0.92. Cronbach’s alpha coefficients surpassing 0.90 can suggest that some items are essentially measuring the same thing, which may signal redundancy, as in the case for factor 1. This may warrant removing overlapping items or shortening the scale in future studies. The internal consistency of the UFS IHMAI was found to be acceptable, as substantiated by a Cronbach’s alpha coefficient of 0.95 calculated for the UFS IHMAI in its entirety. This indicates that construct validity was developed as the item sets within the instrument reliably measure a single underlying construct (Tavakol and Dennick, 2011).
Discussion
This article reports on the first construct validity study of the UFS IHMAI using EFA, with a sample size of 220 3- and 4-year-old children, confirming a five-factor solution. This is the first field study that uses a novel, play-based IHM assessment instrument to evaluate the performance of the young child during a developmental phase characterised by rapid acquisition of object manipulation skills. Between 3 and 6 years, children’s IHM skills are focused on developing more consistent and mature movement patterns in order to manipulate a variety of objects for skilled use and placement (Pont et al., 2009). Abzug et al. (2020) stated that by 3 years of age, IHM skills start to emerge, making standardised assessment possible, as all the children who participated in the field testing were able to engage in the play-based activities. The descriptive data obtained of 3- and 4-year-olds (see Table 1) contribute to the understanding of South African children’s IHM performance (Visser et al., 2014; Visser et al., 2016).
The conceptual considerations that guided the development of the UFS IHMAI and the interpretation of these factors are important to frame the discussion. These conceptual considerations are outlined below. First, aspects related to the child’s developmental age, hand function and structure (e.g. hand size, underlying hand mechanisms, tactile discrimination; Parry et al., 2024). Second, aspects related to the object property used in the assessment includes the size, number of objects, texture, weight, shape and spatial orientation, as well as the object’s familiarity and uses (i.e. object affordances) to the child. Third, aspects related to the task complexity are depicted by the required activation or co-activation of multiple IHM movements; for example, the number of movements required to complete the task (a single movement, repeated movements or specific sequence of movements) and the hand position during the movement (supination, pronation or neutral). Finally, aspects related to the child’s performance skills are discussed, including the child’s understanding of the task, motor learning and skills acquisition (maturation of movement and compensation strategies) that is influenced by the opportunities allowed to practise the movement, and the verbal and visual guidance provided during administration of the subtasks (Abzug et al., 2020; Case-Smith and Pehoski, 1992; Henderson and Pehoski, 2006; Pehoski et al., 1997a;)
Within the instrument, it was noted that latent complex rotation and complex shift (Factor 1) had an alpha coefficient exceeding 0.90, indicating possible redundancies and suggesting item reduction for this age group (Tavakol and Dennick, 2011) in future studies. As item 11B had the lowest factor loading (Table 2), it can be considered for removal. The subtasks of items 5, 6 and 11 loaded onto Factor 1, and their complexity may be attributed to the objects used and task requirements. In these items, unfamiliar objects (keys, ruler and pencil) were used in an unfamiliar way for this age group. The object sizes in relation to the child’s hand size and the supinated position of the hand while manipulating the objects may also play a role. In addition, the task required co-activation of various IHM skills, further contributing to the movement complexity.
In comparison, children performed better in simplistic tasks, such as items 3 and 10 (Table 1), for which a single IHM skill was required for successful completion. Hence, the complex nature of the items within this factor highlights that for children in this age group, complex rotation and complex shift are not yet functionally integrated and are in a phase of non-manifestation, confirming the latency of these IHM skills. Furthermore, at this age, complex rotation is a difficult skill to apply without external support (Haegele, 2021), and various compensation strategies are used (Pehoski et al., 1997a; Tavakol and Dennick, 2011; Visser et al., 2014).
Three of the five factors reflect emerging IHM skills in this age group, and can be interpreted in light of the underlying conceptual considerations. Emerging rotation and shift (Factor 2) were comprised predominantly of items 10, 12 and 13, with an average median performance score of 2 (Table 1). Subtasks 1B and 7B had lower factor loading (Table 2). The objects used in these item sets were both more familiar to the children (buttons and beads) and used in a familiar manner, contributing to the more evident motor learning patterns observed. The highest loading subtasks were related to the dressing activity, a familiar daily activity often modelled by parents. The simple shift movement activated in these subtasks supports that this is an emerging skill in 3- to 4-year-olds (Exner, 1993; Haegele, 2021).
Similarly, emerging translation with stabilisation (Factor 4) comprised items 8 and 9 that show a clustering of skills based on the task complexity. The children displayed average performance with medians ranging from 2 to 4 (Table 2). As seen in Table 1, translation is an emerging skill as palm-to-finger translation, in particular, is more difficult than finger-to-palm translation in this age group (Exner, 1997; Haegele, 2021). For subtask 9Bii, the increased difficulty might be related to the child’s hand size and number of objects required to be held.
For emerging translation and shift with stabilisation (Factor 5), the subtasks of 4B have been grouped, confirming contextual dominance as the children’s performance was shaped by the interaction between the play-based task and the child. While the children performed average in the two translation movements, with a median score of 2, they performed poorly in the simple shift with stabilisation component, with a median of 1 (see Table 1). This poor performance correlates with the other simple shift with stabilisation subtasks, confirming that this skill emerges around the age of 4 (Haegele, 2021).
The last factor, developing translation without stabilisation and complex rotation (Factor 3), included the two subtasks of 4A, subtask 9Ai and item set 3. The children obtained a median of 4 for all these subtasks (Table 1). Conceptual considerations that may explain the good performance include familiar objects (money coins) used, and the object size and weight in relation to the child’s hand size (Andersen Hammond et al., 2009). The skill acquisition displayed in these subtasks confirmed that as infants watch others and explore the use of tools, they develop detailed mental representations thereof, guiding their understanding of object affordances and allowing practising the movement for motor learning (Kaur et al., 2020). Hence, for this age group, the children’s good performance in translation without stabilisation and complex rotation in familiar tasks is more developed and functionally integrated.
While the theoretical model of IHM proposes 12 distinct components, it is noteworthy that the construct of simple rotation without stabilisation was not included in the factor analysis. All the subtasks measuring this construct lowered the internal reliability of the instrument and did not have any significant contribution to the factor loading. There was a discrepancy in the scores obtained for these subtasks, as children performed average for 7A using nuts and bolts, while poor performance was observed in subtasks 2A and 2B that used a real coin (Table 1). It is possible that while the coin is a familiar object, the child’s unfamiliarity with the specific movement required (rotating the coin on its edge) might have affected their performance. The smaller surface area of the coin reduced grasping ability, resulting in ineffective object manipulation. Conversely, although the nut was unfamiliar, it had a larger manipulation surface and the weight provided more intense somatosensory feedback, which could explain the children’s better performance. The interaction between object characteristics and task demand can influence the functional manifestation of a skill in the developing child. This is an excellent illustration of how motor skill performance is more task-integrated than component-isolated (Andersen Hammond et al., 2009).
The five-factor solutions from the EFA grouped the subtasks in patterns that matched developmental stages of motor skill performance, rather than the expected theoretical classification system that proposed 12 discrete IHM components (Pont et al., 2009). This raises the question of whether the IHM components can be distinguished and independently observed in practice, as proposed in theory, yet confirming the theoretical definition of IHM skills as a complex phenomenon relying on the coordinated interaction of multiple systems, such as the child’s development, the play-based task demands and the environmental context. This mismatch between the theoretical expectations of the IHM classification system and the empirical data, the five-factor solution, is a common phenomenon in early instrument development (Boateng et al., 2018).
Strengths and limitations
To minimise scoring and measurement errors, all fieldworkers and researchers received in-depth training. Both fieldworkers checked the paper-based scores and clarified uncertainties by referring to the video recordings. Trained raters at the UFS reviewed the videos to assess inter- and intra-rater reliability.
A delay in data collection required a second round of sampling due to the limited time and slow returns of consent forms that affected recruitment. Despite the smaller-than-anticipated sample size, 220 participants proved sufficient for factor analysis.
Implications for occupational therapy research and practice
Future research should include separate factor analysis studies for each age group to clearly identify developmental differences in IHM skills, as well as factor-analytic studies spanning all age groups targeted for inclusion in the UFS IHMAI. Additionally, an in-depth review and refinement of the assessment instrument is recommended to identify areas requiring improvement, as streamlining the instrument by removing redundant items may enhance its efficiency without compromising reliability. Finally, further psychometric evaluation of the UFS IHMAI, progressing towards standardisation, is recommended to support its clinical utility and accessibility for practitioners.
Implications for occupational therapy practice include the potential of the UFS IHMAI, once fully developed and standardised, to improve the precision of therapists’ assessment of IHM in young children, especially in ECD settings where assessment of hand function is critical for school readiness and daily task participation. Enhanced assessment accuracy may, in turn, support more targeted intervention planning tailored to the child’s specific manipulation challenges.
The instrument may also assist in the early identification of children at risk for fine motor and hand function difficulties, facilitating timely intervention and potentially improving long-term functional outcomes. Furthermore, using a psychometrically sound instrument such as the UFS IHMAI aligns with the profession’s commitment to evidence-based practice and contributes to the repertoire of standardised assessments informing clinical decision-making.
Conclusion
Establishing construct validity is essential in the development of standardised assessment instruments. This study contributes to the growing body of psychometric evidence for the UFS IHMAI, specifically in relation to 3- to 4-year-old children in South Africa. Strong evidence of construct validity was demonstrated, supported by Chi-square test results reflecting statistical significance, favourable model fit as indicated by the SRMR, and high internal consistency reliability reflected by Cronbach’s alpha coefficients. The five-factor solution derived from the EFA-grouped subtasks aligning with motor developmental stages offers insight into the complexities of developing IHM skills.
The study provides descriptive data on children’s performance across the 12 components of translation, shift and rotation, contextualising age-specific mastery of these movements in play-based tasks. These findings establish a foundation for future refinement of the instrument and underscore its potential as a standardised, evidence-based tool that can contribute to best practices in paediatric occupational therapy assessment.
Key findings
Construct validity of the [removed to ensure blind review] IHMAI for 3- to 4-year-old children was determined.
The five-factor solution with high internal consistency aligns with developmental stages.
Descriptive results broaden understanding of IHM at this age.
What the study has added
This study presents the first construct validity evidence for the UFS IHMAI, with a developmental factor structure, descriptive IHM performance data and refinement considerations toward a standardised, performance-based tool for therapists.
Footnotes
Acknowledgements
The authors thank the fieldworkers who assisted with the data collection – Chanté Koen, Chané Fourie, Karla van Staden, Kimberley Gemmell, Kirsten Campher, Melissa Prinsloo, Natalie Pieters, Natasha Ruiter and Nina Wattel; and Dr. Daleen Struwig, medical writer/editor, Faculty of Health Sciences, UFS, for technical and editorial preparation of the article.
Research ethics
The Health Sciences Research Ethics Committee (HSREC) of the University of the Free State. (ref: UFS-HSD2022/1166/2305). Video recordings were only made of the children’s hands to minimise the inclusion of identifiable features and were stored safely on Figshare, a password-protected platform. All assessment data were captured and stored on REDCap, a secure password-protected platform.
Consent
Written Informed consent was obtained from all children’s parents/guardians, and verbal assent was obtained from children. Ethical practice was ensured by obtaining approval from the Free State Department of Education (FSDoE). Permission was obtained from the ECD centres, followed by meetings with the teachers to inform them of the study. Children who met the inclusion criteria and whose parents/guardians provided consent were selected and assigned a unique research number to maintain confidentiality and comply with the South African Protection of Personal Information Act. Assent was obtained from the children.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public were not included at any stage of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
CB, MV and AK researched literature and conceived the study. CB, MV, AK and MN were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. CB wrote the first draft of the manuscript. CB, MV and AK wrote the next article drafts. All authors reviewed the manuscript and approved the final version of the manuscript.