
Abstract
Introduction
Cancer-related fatigue (CRF) is a persistent, debilitating symptom that disrupts daily life and occupational participation. Understanding its impact is vital for developing effective interventions that support fatigue management and meaningful engagement. This study examined CRF’s impact on occupational participation and how individuals manage it.
Method
A mixed-methods design combined semi-structured interviews with the Activity Card Sort-UK. Seventeen participants with CRF (7 men, 10 women) and diverse cancer types were recruited using purposive, maximum variation sampling. Interviews were analysed using framework analysis, guided by the Canadian Model of Occupational Performance and Engagement.
Findings
Quantitative data showed 59% experienced severe fatigue and 80% reported low fatigue self-efficacy. Leisure, social and high-demand activities were most affected. Three qualitative themes emerged: loss of enjoyment and engagement in meaningful occupations; coping through reactive and proactive strategies; and emotional consequences related to disrupted identity and reduced occupational participation. Participants described trade-offs, diminished spontaneity and altered roles. Gender, age and social context influenced both the impact and coping strategies, and many felt unsupported.
Conclusion
CRF impairs occupational engagement and identity. Occupational therapists and multidisciplinary teams should routinely assess CRF and provide tailored, occupation-focused interventions that support fatigue self-management and preserve meaningful participation. Research should further develop these interventions.
Introduction and literature review
Almost half of people younger than 65 will receive a cancer diagnosis in their lifetime (Ahmad et al., 2015). Therefore, managing long-term treatment effects like cancer-related fatigue (CRF) is critical. CRF is commonly defined as a subjective phenomenon, a feeling of persistent tiredness or lack of energy that fluctuates and is not alleviated by sleep or rest (Weis and Horneber, 2015). It affects over half of people undergoing cancer treatment and nearly two-thirds of those with advanced cancer (Al Maqbali et al., 2021). Even post-treatment, about one-third of people experience long-term CRF, which impacts their daily functioning (their overall ability to manage daily life; Wang et al., 2014).
CRF significantly impacts cancer survivors’ ability to carry out daily activities (specific tasks such as cooking and self-care) and quality of life (a broad sense of well-being; Muthanna et al., 2023; Weis and Horneber, 2015), with functional abilities (e.g. physical, social, cognitive) a key component of quality of life measures. Alongside pain and insomnia, fatigue is regarded by people with cancer as one of the most burdensome symptoms (Hong et al., 2016). The James Lind Alliance (2019) identified fatigue management as a top 10 research priority for cancer survivors (Aldiss et al., 2019).
Quantitative studies have revealed that CRF impacts people’s occupational performance (how well a person can do their daily tasks) in multiple domains (Kennedy and Davis, 2017), including the ability to work and social functioning (Jones et al., 2023), sex life, caring responsibilities and relationships with partners, family and friends (Weis and Horneber, 2015). CRF often leads to occupational disruption and imbalance, with 90% of individuals reporting the need to modify their daily routines (Pergolotti et al., 2016). Cancer survivors with fatigue are nearly three times more likely to face unemployment or take sick leave (Jones et al., 2023), while a recent systematic review revealed that older adults with CRF report reduced leisure activity participation (Engels et al., 2021).
CRF also negatively impacts occupational engagement, wherein individuals do not feel connected or involved with their daily activities (Fleischer and Howell, 2017; Kennedy and Davis, 2017). Our previous research has shown that individuals with CRF have reduced enthusiasm for their work (Rossiter et al., 2025). The substantial interference with daily activities is one of the most distressing aspects of CRF, leading to a narrowed world and disconnection from meaningful roles and individuals’ identities (Bootsma et al., 2020). Such disruptions carry additional financial and societal costs, including increased healthcare service use, lost employment productivity and reliance on state benefits (Jones et al., 2023; Rossiter et al., 2025; Weis and Horneber, 2015). This further strengthens the case for developing occupation-focused CRF interventions to manage CRF, improve survivors’ lives and realise potential cost–benefits.
CRF is primarily treated using non-pharmacological interventions, including behavioural and self-management approaches, which are well-suited to occupational therapists (Garvey et al., 2015; Kinsella and King, 2024; Packer, 2013). Occupational therapy interventions commonly include energy conservation, pacing strategies and activity modifications to help individuals optimise their daily routines and activity participation in managing fatigue (Omura et al., 2022). A recent systematic review of self-management interventions for CRF found a beneficial effect on fatigue in more than half of the studies (Agbejule et al., 2022). However, most studies do not specifically focus on occupation-based interventions, further underscoring the need for increased research in this area.
While previous research has measured the impact of CRF quantitatively, few studies have explored individuals’ experiences living with and managing CRF’s impact on their daily lives and occupational engagement. Understanding these lived experiences through qualitative research, supported by quantitative data, is crucial for developing effective and tailored interventions since it provides in-depth insights into the factors influencing fatigue management. Furthermore, fatigue management interventions have typically been focused on symptom reduction rather than modifying activities, environments and behaviours to enable participation in meaningful occupations and optimise functioning. Occupational therapy interventions are well-positioned to address this gap.
This study applies the Canadian Model of Occupational Performance and Engagement (CMOP-E; Townsend and Polatajko, 2007) as a theoretical framework to examine how person–environment–occupation interactions shape CRF management. Consideration of the dynamic interactions and influences of these three components provides a client-centred, holistic and comprehensive lens for examining how various factors influence an individual’s ability to engage in meaningful occupations. This approach addresses the symptoms of CRF (as is common in current CRF interventions) and the broader environmental and personal factors that uniquely shape occupational engagement.
Aim
This mixed-methods study examined how CRF impacts occupational participation and engagement. Additionally, it examined the self-management strategies participants employed to mitigate fatigue-related limitations.
Method
Study design
A mixed-methods design was employed to explore the impact of CRF on daily activities. Given the complexity of the topic and the limited prior research on CRF’s daily functional consequences, qualitative semi-structured interviews were used to enable participants to explore their in-depth experiences and exert some control over the interview direction whilst remaining focused on the research topic (Holloway and Galvin, 2017). Participants completed an Activity Card Sort-UK (ACS-UK; Laver-Fawcett et al., 2016), which allowed the complementing quantitative contextual data to be compared and explored.
The Canadian Model of Occupational Performance and Engagement (CMOP-E; Townsend and Polatajko, 2007) informed both interview question design (Appendix A) and analysis. Interview questions focused on the impact of CRF on the performance of and engagement with occupations concerning productivity, self-care and leisure domains, alongside environmental, physical, cognitive and affective facilitators and barriers.
This study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research checklist (Tong et al., 2007) to ensure transparency and rigour in qualitative reporting. A completed checklist is available on request.
Participants, recruitment and ethics
Purposive maximum-variation sampling was used via a recruitment flyer posted on UK cancer support forums and social media (due to COVID-19 pandemic restrictions) (e.g. breast, colorectal and prostate groups). Male cancer types (e.g. prostate and testicular cancer) were specifically targeted to increase the diversity of the research.
Eligible participants were encouraged to contact the research team if they were interested in participating, wherein the research team confirmed eligibility. Participants were included if they were adults (18+), currently receiving or within 2 years of cancer treatment and living in the United Kingdom. Individuals were excluded if they could not participate in English due to a lack of translation resources. After discussing the research with participants, participants who remained interested were sent the participant information sheet and consent form.
Interviews were conducted via telephone or Microsoft Teams, per participants’ preferences and COVID-19 restrictions. Participants’ consent was recorded verbally by reviewing consent form items and obtaining consent statements. Consent was obtained verbally due to COVID-19 restrictions, which could have made sending and receiving post challenging for clinically vulnerable participants.
Participation was voluntary, and participants could stop the interview or withdraw from the study at any time. Participants were signposted to support services verbally and in the participant information sheet. The study design and documentation received ethical approval from the Faculty of Environmental and Life Sciences ethics committee, University of Southampton (reference: 48218).
Data collection
Quantitative measures
Consenting participants completed a demographic questionnaire and three further measures before interviews. These included the Functional Assessment of Chronic Illness Therapy-Fatigue Scale (FACIT-F) to measure fatigue (Butt et al., 2013) and the Perceived Self-Efficacy for Fatigue Self-Management to measure perceived self-efficacy for managing fatigue, both validated for use with cancer populations (Hoffman et al., 2011; Yellen et al., 1997). An adapted (with consent) Microsoft Word tick box version of the ACS-UK (Laver-Fawcett et al., 2016) was used specifically to explore the impact of CRF on activity participation (the extent to which individuals were involved in occupations). This enabled electronic completion during COVID-19 restrictions.
The quantitative measures were used to facilitate sample description and qualitative context. Participant responses, particularly to the ACS-UK, were further explored during qualitative interviews to elicit more detailed responses. Participants chose whether to complete the ACS-UK electronically or verbally pre-interview.
Qualitative in-depth interviews
Semi-structured, in-depth individual interviews were used to collect data between October 2020 and April 2021. No repeat interviews were conducted. The mean interview length was 79 minutes (range: 36–129 minutes). Telephone or video (using Microsoft TEAMS) interviews were used. Interviews were audio- or video-recorded to allow verbatim transcription.
A semi-structured interview guide (Appendix A) was used to conduct the interviews. The interview guide included open questions and followed a logical funnel structure starting with broad questions, e.g. ‘What fatigue symptoms do you have?’ which gradually narrowed to more focused questions to answer the research question and gather in-depth insights on specific domains (e.g. work, leisure; Hennink et al., 2020). The interview guide aligned with CMOP-E domains and was developed in collaboration with a patient representative with a previous head and neck cancer diagnosis and history of CRF. All questions were asked, but in different orders depending on participants’ responses to allow participants some control over the interview. Follow-up questions and prompts were used according to participants’ responses. Interview questions focused on perceptions and impact of fatigue, ACS-UK responses, the impact of CRF on occupations (including leisure, productivity, self-care, work and relationships), self-management of fatigue and desired support.
Interviews were conducted by the first-named author (C.B.; N = 7 interviews) and the second-named author (L.R.; N = 10 interviews). C.B. and L.R. both identify as female. Both C.B. and L.R. are occupational therapists and researchers; participants were informed about their positions and experience. Their professional backgrounds as occupational therapists could have resulted in assumptions about occupational impact. Therefore, steps were taken to be reflexive (see section ‘Data analysis’). C.B. has extensive qualitative research experience and a background in working in cancer services, and L.R. was trained in qualitative research interviewing for the study. C.B. and L.R. had no previous relationship with the participants.
Data analysis
Before analysing the qualitative data, authors C.B. and L.R. analysed the ACS-UK data by extracting it, entering it into Microsoft Excel and running descriptive statistics.
Transcriptions were analysed using framework analysis to systematically compare data within the research team (Gale et al., 2013) and NVivo software. Authors C.B. and L.R. conducted all analyses. Table 1 shows how Gale’s framework analysis stages were followed.
Stages of framework analysis.
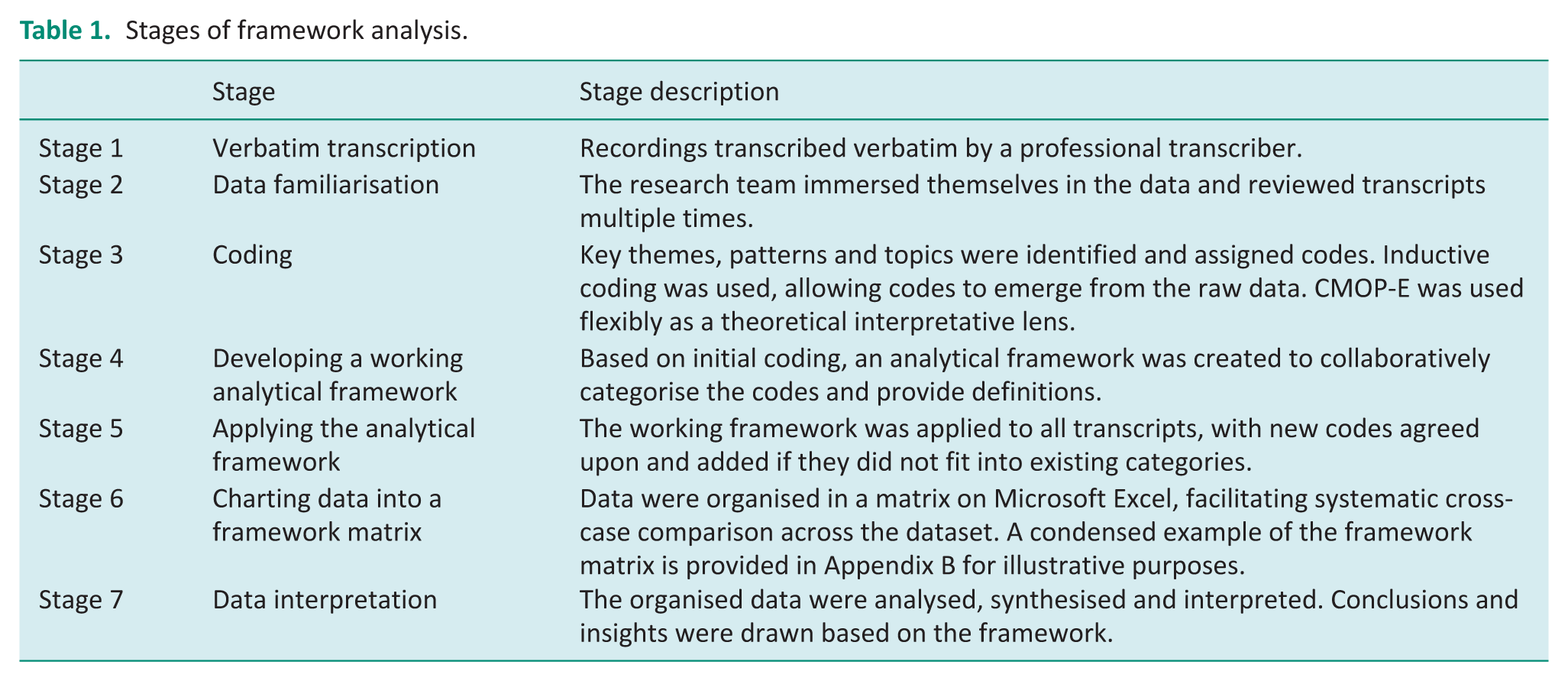
To increase rigour and reflexivity, C.B. and L.R. independently coded the first three transcripts and collaboratively agreed on a coding schedule and working analytical framework. C.B. and L.R. met regularly and discussed new codes and emerging themes throughout the analysis. Respondent validation was not conducted due to the time-sensitive nature of data collection and the potential burden on participants managing CRF. C.B. and L.R. kept reflective diaries to consider any potential influences and mitigate potential biases. Entries were added after interviews and during analysis. Thematic saturation was observed when no new codes or themes emerged during the final interviews, indicating sufficient depth and coverage of participant experiences.
Findings
Participant characteristics
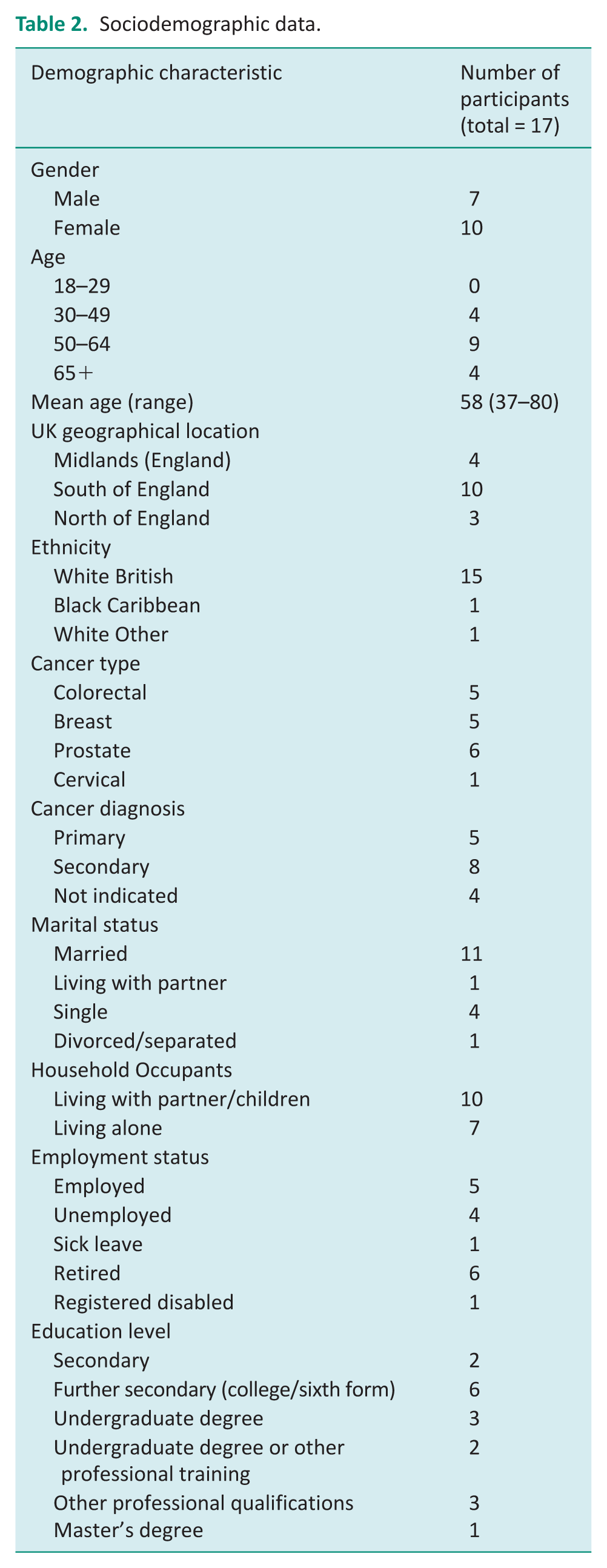
A total of 23 potential participants contacted the research team, of whom 17 participated in the study. The six non-participants did not provide reasons for non-participation and did not reply to emails after initial contact.
Demographic characteristics are summarised in Table 2.
Sociodemographic data.
Quantitative findings
Table 3 presents fatigue severity, self-efficacy and Activity Card Sort-UK (activity participation) scores.
Clinical questionnaire data.
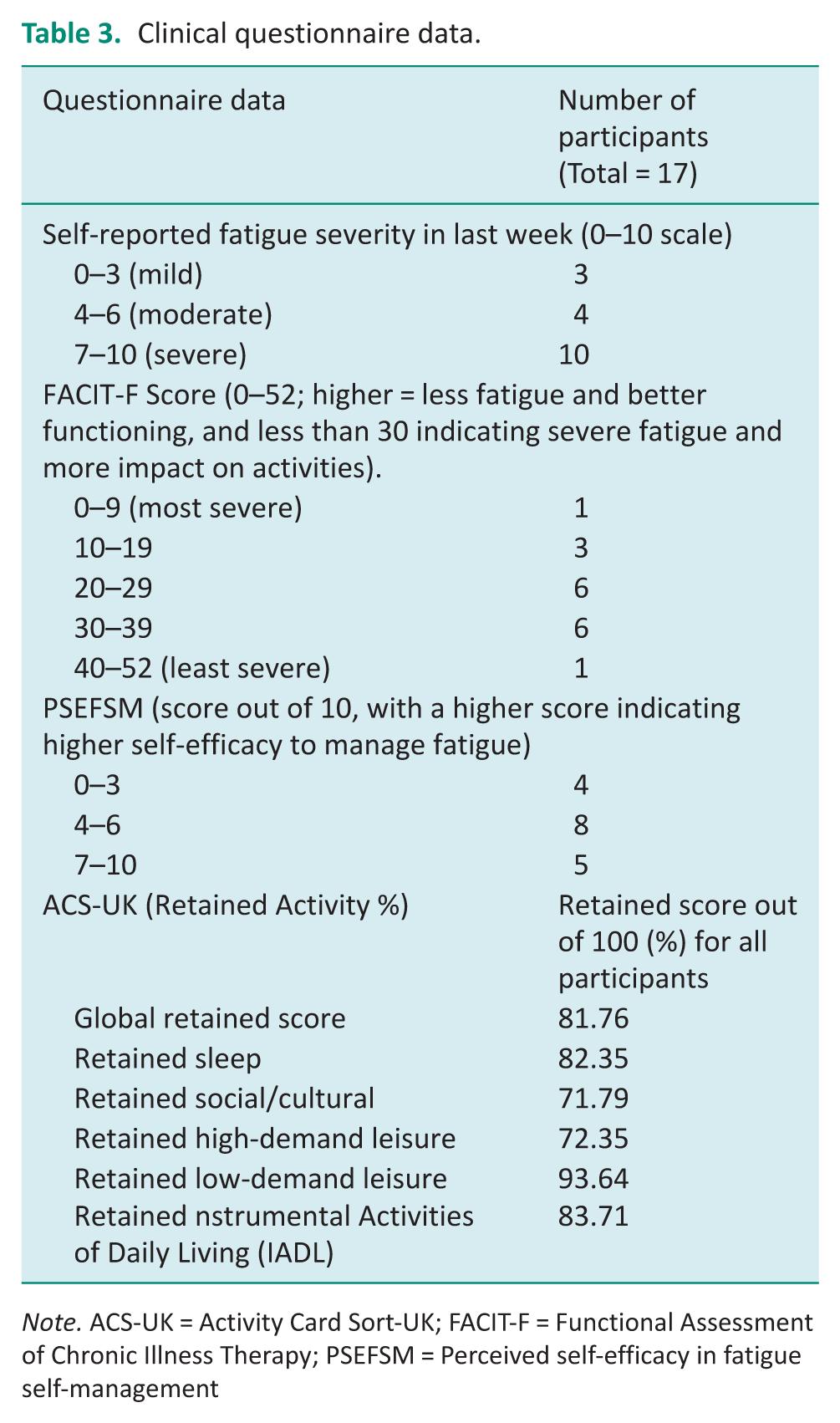
Note. ACS-UK = Activity Card Sort-UK; FACIT-F = Functional Assessment of Chronic Illness Therapy; PSEFSM = Perceived self-efficacy in fatigue self-management
According to the FACIT-F scores, 59% of participants reported severe fatigue scores (<30/52), and the same percentage self-reported their fatigue severity level as ⩾7, indicating severe fatigue. Most participants (80%) had low self-efficacy for managing fatigue (scores ⩽6/10), with males reporting higher mean scores (6.5 vs. 4.3 for females). The ACS-UK scores revealed that participants experienced reduced activity participation in all areas. CRF most impacted social/cultural (retained activity score: 72%) and high-demand leisure activities (retained activity score: 72%).
Qualitative findings
Three interconnected yet distinct themes were identified from the analysis, each revealing how CRF impacts occupational engagement and quality of life: (1) Decreased enjoyment and engagement in previously valued occupations, (2) adjusting occupations and managing fatigue through reactive adjustments and proactive self-management and (3) the well-being and identity-related consequences of continuation or loss of meaningful occupations. These themes are supported by participant quotes, contextualised with pseudonyms, ages, genders, and diagnoses to highlight individual experiences and group patterns that recognise common themes. Data are presented from both an individual and group perspective to acknowledge the value of individual experiences and recognise common themes.
Decreased enjoyment and engagement in previously valued occupations
This theme explores how fatigue, alongside other related factors such as treatment symptoms and health anxieties, profoundly disrupted participants’ ability to derive engagement and enjoyment from activities they once found meaningful. Leisure activities were particularly impacted, aligning with the quantitative ACS-UK data showing substantial social/cultural and high-demand leisure participation reductions.
Trevor (male, aged 68, colorectal cancer) poignantly describes this loss and being left with only essential activities:
The greatest impact is leisure; it’s personal. It’s as if the fatigue and cancer have taken that side of my life away, and it’s just left me with the closed in four walls bit and the basic bit of getting on with life.
Trevor discussed the ‘massive’ impact on his high-demand leisure occupations, such as playing bowls, fishing and dog walking for his friend. Though he continued instrumental activities like cooking, his engagement appeared hollow: ‘I’m cooking for something that I know I’m not going to enjoy. . . I know I’m going to be tired while I eat it’.
For many, fatigue compounded and centrally influenced other challenges, such as treatment side effects and health anxieties, contributing to reduced occupational engagement. For example, Jane (female, aged 58, colorectal cancer), a former chef, linked her waning enthusiasm for cooking and baking to both fatigue and cancer-related food anxieties:
Because I’m just too tired and half because since I was diagnosed, I have had a little bit of a problem with food mentally because I used to be a very healthy eater, and then I couldn’t understand why I got bowel cancer because they say it’s people that eat all processed foods and of course being a chef I had quite a lot of interest in cooking so now there’s so many things I can’t eat. So it’s dampened my interest in cooking and baking, etc.
The impact extended to work, socialising and even dating. Younger participants (aged ⩽50, n = 4), like Kate (female, aged 39, breast cancer), articulated how fatigue made romantic relationships seem insurmountable and a low priority they lacked energy for:
If I cannot summon the energy to wash my hair, there’s no way I can summon the energy to wash my hair and put on make-up, put on a decent outfit, travel to a bar or restaurant to meet somebody to go on a date.
Adapting occupations and managing fatigue through reactive adjustments and proactive self-management
This main theme encompasses two sub-themes reflecting how participants navigated fatigue in their daily lives: (1) Reactive adjustments and (2) proactive self-management. Reactive adjustments are trade-offs, coping mechanisms and decision-making processes that minimise the immediate impact of fatigue, whereas intentional self-management strategies are proactive, preventative and purposeful actions.
Reactive adjustments
Energy limitations forced participants to make difficult compromises to meaningful occupations regarding quality, frequency or manner of participation. Participants reported engaging in their previously valued occupations in different ways, for instance, doing them for shorter periods, taking breaks, planning extensively or intentionally not committing to plans and waiting to see how they feel each day to avoid disappointment. The term ‘trade-off’ highlights how participants balanced their desire to remain engaged in their occupations with their limited energy resources. Kirsty (female, aged 60, secondary breast cancer) described meticulously planning her week to avoid overexertion:
I have to be careful that I don’t overdo it, that I don’t have too many things going on in the week. I have to look at my week and think: I’m seeing this person that day; I’m seeing somebody else the next day. Can I cope with that from a point of view of tiredness and overdoing it?
By contrast, Vicky (female, aged 62, breast cancer) abandoned planning altogether to protect herself from the unpredictability of fatigue and resultant disappointment from cancelled plans:
It’s so unpredictable. . . if I want to plan to go somewhere, I have to think right: what am I going to do if the fatigue kicks in? Is there anywhere I can quickly get a taxi home? So it undermines my confidence. . . If I don’t plan to do anything and I just make my decision every day about what I’m going to do, then I don’t have disappointment. It’s an awful way to be, not planning anything.
Both extensive planning and feeling unable to plan anything due to fatigue appeared to be necessary coping strategies for participants, but resulted in missed opportunities and loss of spontaneity.
Similarly, Trevor discussed making adaptations to redefine participation. Trevor (male, aged 68, colorectal cancer) attempted to sustain his fishing hobby by simplifying logistics – carrying gear directly from his car – but still faced days when fatigue rendered even this impossible:
I’ve fished all my life. I used to love to go fishing, but I couldn’t cope with that, and some days when I was feeling not too bad, I’d say to my wife I think if I feel a bit better tomorrow, I might go fishing, I could just take myself off to the lake, and I can drop the tackle from the car I haven’t got to move it around, and she’d go yes, yes. And you’d get up the next day, and you are wiped out, and you can’t cope with it.
Others, like Danielle (female, aged 56, secondary breast cancer), replaced high-demand leisure occupations with lower-demand alternatives: ‘I’m doing things more that I can just sit and rest like crosswords and reading’. Another similar sedentary restful activity for participants included watching television.
The work adjustments reported by working-age participants were pervasive, including taking extended sick leave, reducing their hours or commencing early retirement. Some younger participants also reported the challenges of coping with fatigue while managing multiple other responsibilities alongside work, such as parenting duties.
For a small number of participants, time away from work and physically strenuous occupations facilitated pleasurable engagement in new occupations and interests, as explained by Roy (male, aged 62, primary prostate cancer): ‘I have done probably 15 cakes. I’ve never baked before’.
Gender and life stage influenced the trade-offs made. For instance, when reflecting, Nick (male, aged 46, secondary prostate cancer) attributed a combination of the cancer diagnosis, reduced working hours, reduced testosterone and increased fatigue to him prioritising more family time: ‘If you throw a lack of testosterone into that which frankly makes you less interested in sex and women it realigns your priorities and love suddenly jumps to the top of the pile’.
Participants reported balancing paid work or housework with self-care through trade-offs. They explained that if they continued with one activity, they had to reduce or lose another. This finding was particularly prevalent for younger working-age participants juggling multiple responsibilities and those living alone. If participants prioritised work, this impacted their ability to engage in leisure occupations and vice versa. One participant, Kate (female, aged 39, secondary breast cancer), described how she prioritised her yoga practice before starting work but did a shorter session and compromised ‘on the work side of things’ by working later. Another participant was frustrated with balancing chores and walking:
I get quite frustrated that I either have to do a little bit of housework or I can go out for a walk. I can’t seem to manage to do both things. I can’t multi-task anymore; I can only do one thing in a day, basically (Jane, female, aged 58, colorectal cancer).
Proactive self-management
Alongside making practical adjustments and trade-offs, participants actively developed and employed diverse fatigue management strategies, including pacing/resting, planning, prioritising, keeping a fatigue diary, physical activity, mindfulness and reframing perspectives by adjusting expectations and changing how they do occupations (e.g. batch cooking, seated activities). Planning and resting were the most commonly reported strategies. Some participants, such as Trevor (male, aged 68, primary colorectal cancer), found resting alleviated his fatigue: ‘I think since I’ve started doing that [giving myself rest breaks] and getting more rest, I think my fatigue levels are coming down’.
However, many others, like Vicky (female, aged 62, secondary breast cancer), lacked awareness of effective fatigue management strategies and felt unsupported by healthcare professionals: ‘It would be interesting to know if there was anything I could do to manage it because. . . I don’t feel there is anything I can do to manage it’.
Participants felt healthcare professionals often did not discuss or adequately address fatigue. Kate (female, age 39, secondary breast cancer) criticised the lack of timely intervention to address her difficulties and felt like banging her ‘head against a wall for quite a while’. Many participants described initiating fatigue-related conversations themselves. Those who accessed occupational therapists or physiotherapists (typically those with secondary cancer) benefitted from structured strategies such as activity diaries and problem-solving techniques. Kate (39, female, secondary breast cancer) emphasised the importance of trial and error, reflection and having professional support to develop effective strategies.
Most participants reported developing strategies themselves, for example, exercising, but did not realise this was an evidence-based recommendation or followed advice from supportive friends and family members. Susan (female, aged 69, colorectal cancer) tied her adaptive self-management skills, such as taking breaks, to her managerial background. Notably, male participants reported higher mean self-efficacy (PSEFM scores), and those rating their self-efficacy as ⩾7 reported in the interviews that they could manage fatigue independently without healthcare professionals’ input.
The well-being and identity-related consequences of continuation or loss of meaningful occupations
This theme concerns the profound emotional consequences experienced by participants from the loss or modification of meaningful occupations due to fatigue. Participants’ ability or inability to engage in valued activities (their occupational performance) often led to feelings of frustration, guilt and a loss of self-identity. Participants frequently expressed feeling alienated from their former selves. Ellie (female, aged 45, colorectal cancer) summarised the dissonance she felt from being more restful and less active, saying: ‘It’s kind of like not me’.
Trevor (male, aged 68, colorectal cancer) mourned his active identity:
The fatigue impacts me massively because even though we’re in our late 60s, me and my wife, we’ve always been very active. We’ve been people who walk, and socially, I play bowls; it just stops me doing everything. I used to be captain of three bowls teams; I went fishing; I had a dog for years and walked the dog. . . in fact, I was walking the legs off the dog (Trevor, male, aged 68, colorectal cancer).
Adjustments often came at a personal cost, caused participants distress and impacted their sense of self-worth and identity. They also adapted their occupations to cope with fatigue and sometimes found these adjustments reduced their enjoyment and satisfaction in the activities, indicating reduced occupational engagement. For instance, for Susan (female, aged 69, colorectal cancer), the emotional cost of modifying social behaviours was deeply tied to her values of independence and resulted in avoidance of social events:
I’m very independent, and I wouldn’t want to moan or say I’m tired; I would try and stick it out, and then it’s not a great pleasure when you’re sticking it out for the wrong reasons.
Feelings of personal failure resulting from feeling disconnected from their usual identity were a common interview theme, with many participants discussing their inability to perform occupations they once valued as a source of sadness. Roy (male, aged 62, primary prostate cancer), for instance, felt conflicted between his stubbornness and the need to accept the limitations imposed by fatigue: ‘I’m a stubborn sort of person. I’ve tried my hardest, I’ve failed, I have to adapt around it. I can’t move a hill; I can only walk round it’.
Work disruptions further exacerbated identity struggles as participants described being someone they never used to be. Sarah (female, aged 37, secondary breast cancer), unable to work for the first time, wrestled with feelings of guilt: ‘I start to feel guilty that I haven’t done anything because I’ve never been this person; I’ve never had cancer before, so I’ve never been this person where I’ve had to sign off from work for this amount of time’.
Discussion and implications
To our knowledge, this is the first UK-based qualitative exploration of how CRF impacts occupational engagement and the self-management strategies individuals employ to mitigate these impacts. Supported by quantitative data from the ACS-UK, our qualitative findings highlight CRF’s substantial disruption of daily life, particularly in leisure, social, and work domains. Most previously published research on the impact of CRF on daily activities is quantitative and has not used an occupational lens to inform the study design. Given the distress caused by occupational loss and identity shifts, these insights are crucial for developing person-centred, holistic, occupation-focused CRF interventions.
This research has revealed the following key insights: (1) CRF has a substantial impact on occupational performance and engagement, necessitating adjustments, trade-offs and self-management strategies; (2) loss or modification of valued occupations diminishes enjoyment, well-being, and identity, exacerbating emotional distress and (3) experiences of CRF management vary by demographics (e.g. gender, age and working status), underscoring the need for tailored interventions.
Impact of CRF on occupational engagement
Quantitative data revealed severe fatigue and low self-efficacy levels for managing fatigue among participants. Both ACS-UK and qualitative findings demonstrated CRF’s pervasive impact, with leisure and social participation most impacted. The severe impact on participants’ ability to engage in meaningful leisure occupations caused them emotional distress. Participants reported being reduced to the ‘basics’ of life (e.g. personal care), leading to occupational disruption and imbalance (Anaby et al., 2010). This finding aligns with the CMOP-E (Townsend and Polatajko, 2007), emphasising leisure’s role in well-being (Nivestam et al., 2023). This corroborates a small number of other studies, which have found that cancer disrupts people’s usual leisure occupations and results in more passive leisure occupational engagement (Engels et al., 2021; Fleischer and Howell, 2017; Shipp et al., 2015; Sleight, 2017). However, none of these studies focused specifically on the impact of CRF on leisure and social occupations; this study adds further insight into this topic, a crucial first step in developing effective CRF interventions (Skivington et al., 2021).
Notably, this study adds to the literature that reduced enthusiasm for previously valued occupations stemmed not only from fatigue but also from intersecting cancer-related symptoms (e.g. treatment side effects and health anxieties). This multifactorial disruption illuminates the complex interaction between fatigue and the broader challenges imposed by cancer and highlights the need for person-centred, holistic interventions addressing CRF within the broader context of cancer survivorship.
CRF self-management strategies and adaptation
To maintain occupational participation despite CRF, participants commonly adjusted their activities, shifting from high- to low-demand leisure occupations (e.g. passive hobbies) or modifying how tasks were completed. These modifications included planning ahead, taking rest breaks, doing less overall or reducing demand in another area to compensate.
A novel finding of this study was that both planning and avoiding planning (in an attempt to mitigate disappointment) led to frustration for participants. While energy conservation strategies often advocate planning (Sadeghi et al., 2016), our study reveals that rigid planning added emotional strain when fatigue was unpredictable. This suggests a gap in current occupational therapy interventions, pointing to the need for flexible, adaptive approaches.
Although few participants reported receiving it, professional fatigue management guidance helped participants, a consistent finding in previous quantitative research (Milzer et al., 2024; Stone et al., 2000). Pacing and rest were most commonly reported in this study. Higher self-efficacy for fatigue self-management, previous relevant employment experience and a supportive social network facilitate effective self-management, reinforcing the role of personal factors in the CMOP-E framework for modifying self-management behaviours as part of successful adaptation (Chan et al., 2016). These factors warrant attention when developing CRF interventions. Those who accessed occupational therapy or physiotherapy (typically metastatic cancer patients) reported structured strategies (e.g. activity diaries) as beneficial, though professional input was often delayed or patient-initiated.
While some participants experienced meaningful engagement with new, lower-energy activities (e.g. baking, crafting), others experienced frustration and distress, particularly when these activities still proved challenging. This finding is novel for CRF but builds on another study’s finding that men with breast cancer found meaning in new occupations such as advocacy (Potter et al., 2023). Individuals with cancer may benefit from professional input to manage their feelings around adapting to CRF through trying new occupations.
Psychological and identity-related consequences of CRF
The loss or modification of meaningful occupations precipitated identity disruption, with participants expressing grief over their ‘former selves’. Resting or not working to help manage fatigue, combined with changes in occupational engagement, contributed to feelings of identity loss and further reduced enjoyment for occupations that participants once valued. Fatigue-related occupational loss is a novel contribution of this paper that aligns with Bury’s (1982) concept of ‘biographical disruption’, a term used to describe how an individual’s sense of self and identity can be threatened by illness or disability. Our findings also corroborate other research on cancer-related identity shifts as participants grappled with role loss (e.g. as workers) while others mourned abandoned hobbies or social roles (Hopkins et al., 2024; Park et al., 2009).
Recent studies have qualitatively explored the potential for using art-based activities to help women reflect on identity changes following cancer treatment (Ranger et al., 2023). Our findings underscore the potential for occupational therapy CRF interventions to incorporate identity redefinition strategies, such as creative-based reflection, to mitigate distress caused by occupational loss and resultant identity changes. Furthermore, the holistic nature of the CMOP-E framework proved valuable in understanding how CRF links occupational disruption and identity, supporting its utility in future CRF intervention-development studies.
Demographic variations and tailored interventions
Our study revealed several illuminating age- and gender-related differences. Younger participants (aged ⩽50) emphasised CRF’s impact on sex and dating, which are areas often overlooked in the literature and clinical practice, with more focus on clinical areas of concern, self-care and productivity domains (Al-Abdin et al., 2021; Mackenzie, 2021; Rose and Hughes, 2018). Our younger participants also discussed in detail the substantial impact of CRF on their caring and work responsibilities (as identified through extended sick leave, reduced hours or early retirement) and how these impacts affected their identity.
Men reported higher self-efficacy for managing fatigue than females and less need for external support than female participants, who often voiced frustration at the lack of professional input regarding their fatigue issues. This is consistent with research indicating that males typically exhibit lower help-seeking behaviours (Thompson et al., 2016). Male participants also highlighted how fatigue, testosterone changes and cancer collectively altered their perceptions and reshaped their priorities. Males are often under-represented in intervention-development research, which can make interventions better suited to females (Knox et al., 2022).
Limitations and future research
This study has some limitations. The research aimed to complete an in-depth qualitative exploration (with supporting quantitative data) of the topic. Therefore, the sample size was purposefully heterogeneous but relatively small and may not be generalisable. The study sought to recruit a diverse sample, and we recruited participants of a range of ages, a mix of genders, diagnoses and various living situations. Our recruitment strategy resulted in the inclusion of three of the four most common cancer types (breast, prostate and colorectal; Cronin et al., 2018). However, no lung cancer participants were recruited, and all but two participants were White British. Participants were also only England-based. To increase diversity, we provided accessible research materials and advertised widely, targeting male cancer forums to increase the representation of males. Active recruitment of diverse populations (e.g. ethnic minorities and lung cancer patients) should be a priority in future studies.
The research was conducted during the COVID-19 pandemic, resulting in a necessary reliance on social media recruitment (excluding individuals not engaged with these platforms) and utilising a paper-based adaptation of the ACS-UK, with potential validity implications. Conversely, this also resulted in interesting findings relating to working from home and fatigue management, which were explored in-depth in another paper (Rossiter et al., 2025). Additionally, some participants felt the pandemic restricted their activities in addition to their fatigue levels, so findings need to be considered in this context.
This study has highlighted the adverse impact of CRF on occupational engagement, providing valuable insights to inform the development of tailored person-centred interventions. Intervention development should adopt a co-design approach with patient contributors, tested in a future randomised controlled trial.
Implications for occupational therapy
This study illustrates how CRF creates occupational injustice and reduces occupational engagement, disrupting productivity, leisure and self-care, revealing occupational needs that occupational therapists could address. Yet, occupational therapists remain underutilised in the cancer care pathway and may only support palliative care patients (Buckland and Mackenzie, 2017). Our study strengthens the case for expanded OT roles. Earlier occupational therapy involvement in the cancer pathway could address patients’ needs in a more holistic and personalised way, as advocated by Macmillan Cancer Support (2024). Leisure and social participation could be emphasised based on our findings.
This research also emphasises the importance of tailored occupation-focused strategies addressing identity shifts. Fatigue management interventions are rarely occupation-focused (Hopkins et al., 2024). This study supports an approach that recognises identity shifts, values and feelings towards the alterations individuals need to sustain occupational participation and engagement.
Our study has also demonstrated that CRF interventions could benefit from tailoring to the needs of different demographics (e.g. younger, working-age and different genders). Participatory workshops could be used to tailor strategies by demographic, aligning with Macmillan Cancer Support’s (2024) call for patient-centred care. Using the CMOP-E (Townsend and Polatajko, 2007) proved valuable for considering the dynamic interaction between the person, their occupations and the environment. This model could guide occupational therapists in supporting individuals with CRF to adapt to occupational disruptions, identity or role changes and achieve occupational balance. Occupational therapists are well-suited to supporting people with this occupational adaptation process (Hopkins et al., 2024).
Given limited resources, occupational therapists would be well placed to offer educational interventions to patients and oncology practitioners. Developing and testing tailored occupation-focused interventions for CRF management, particularly focusing on leisure, work, socialising, values, meaningful occupation and identity, is necessary to facilitate adaptive self-management.
Conclusion
This study revealed that CRF disrupts all occupations, particularly work, leisure, socialising and cultural domains, with a cascading impact on identity, well-being, and occupational balance. Current fatigue management often neglects occupation-focused strategies, leaving patients to adapt independently with variable success. More emphasis should be placed on these areas by services. Occupational therapists are uniquely positioned to address these gaps through tailored interventions that foster occupational adaptation and engagement. Future research should prioritise co-designed, occupation-focused CRF interventions, ensuring they are accessible, flexible and responsive to individual needs.
Key findings
CRF disrupts occupational participation and engagement, particularly in leisure/work/social domains, causing distress and impacting identity.
Individuals with CRF seldom receive professional support.
CRF experiences vary, suggesting tailored interventions are needed.
What the study has added
The study provides novel insights into how CRF impacts occupational engagement and how individuals self-manage these challenges. These findings are critical for occupational therapists to develop and deliver evidence-based occupation-focused interventions to address CRF’s functional and psychosocial consequences. Centring the lived experiences of individuals with CRF bridges a gap in current literature and offers a foundation for person-centred strategies.
Footnotes
Appendix
Example of framework matrix.
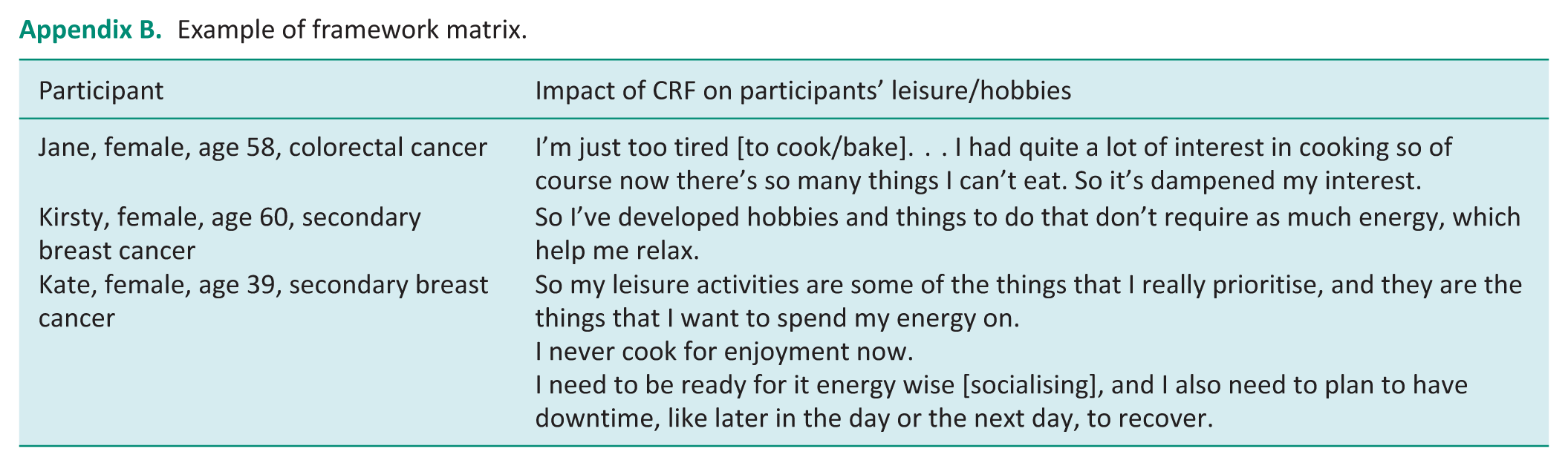
| Participant | Impact of CRF on participants’ leisure/hobbies |
|---|---|
| Jane, female, age 58, colorectal cancer | I’m just too tired [to cook/bake]. . . I had quite a lot of interest in cooking so of course now there’s so many things I can’t eat. So it’s dampened my interest. |
| Kirsty, female, age 60, secondary breast cancer | So I’ve developed hobbies and things to do that don’t require as much energy, which help me relax. |
| Kate, female, age 39, secondary breast cancer | So my leisure activities are some of the things that I really prioritise, and they are the things that I want to spend my energy on. I never cook for enjoyment now. I need to be ready for it energy wise [socialising], and I also need to plan to have downtime, like later in the day or the next day, to recover. |
Acknowledgements
We would like to acknowledge Peter Johnson for his contributions to the study design and reporting as a patient representative and service user with a history of cancer and CRF. Peter Johnson has also previously been a facilitator and patient voice for a patient programme with Self-Management UK.
Research ethics
This study was approved by the Faculty of Environmental and Life Sciences ethics committee at the University of Southampton on the 6 July 2020. Study ID: 48218.
Consent for participation
Recorded verbal consent for each consent form item was provided by all participants. This was not written consent due to changes in ethics processes due to COVID-19 measures at the time.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was included in the planning and progress of the research and reporting of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the RCOT Constance Owens early career researcher award and was supported by the University of Southampton, where CB holds a substantive position.
Contributorship
CB conceived and designed the study, obtaining funding and ethics approvals. CB and LR completed participant recruitment, data collection, and data analysis. All authors reviewed and edited the manuscript and approved the final version.