
Abstract
Introduction:
This study explored the strategies used by people with systemic sclerosis to perform valued obligatory (self-care), committed (home management, care of others, productivity), and discretionary (leisure and socialization) activities.
Method:
This cross-sectional study included a convenience sample of 92 people with systemic sclerosis who completed the Valued Life Activities Scale (VLA). The VLA categorizes activities into three main domains: obligatory, committed, and discretionary. Participants indicated the type of adaptive strategy used for each activity (assistive devices, personal assistance, limited frequency, and taking more time). Participants also completed a demographic questionnaire and measures of pain, fatigue, depression, and daily activity performance. Frequency counts were calculated for strategies used for each activity. One-way analyses of variance compared the mean use of strategies across the three domains (obligatory, committed, and discretionary). Pearson correlation coefficients calculated relationships between strategy use and pain, fatigue, depression, and daily activity performance.
Results:
Significantly, more strategies were used for committed activities compared to obligatory activities. Limiting the frequency of performing an activity was used significantly more for committed and discretionary activities than for obligatory activities. The least used strategies were assistive devices and assistance from another person. Fatigue and depression were related to strategy use, whereas pain and daily activity performance were not.
Conclusion:
People with systemic sclerosis use adaptive strategies to perform VLA. However, the strategies, most frequently used, such as taking more time or limiting the frequency of performing some activities, may result in relinquishing other valued activities.
Keywords
Introduction
Assistive devices, taking more time/pacing, assistance, and/or limiting the frequency of performing activities or parts of activities are strategies often recommended for people with rheumatic diseases to protect joints, reduce pain, maintain or increase independence, and conserve energy (Backman and Poole, 2020). Assistive device use has received the most attention in the literature and has been reported to vary between 25% and 90% in people with rheumatoid arthritis (RA) and osteoarthritis (OA) (de Boer et al., 2009; Kjeken et al., 2013; Polluste et al., 2012; Thyberg et al., 2004). Device use has been found to be related to age, disease severity, and degree of activity limitations (de Boer et al., 2009; Polluste et al., 2012; Rodrigues et al., 2019; Thyberg et al., 2004). The most frequently used devices reported by people with RA were grab bars, shower chairs, can openers, and built-up handles (de Boer et al., 2009; Thyberg et al., 2004), while can and jar openers and ergonomic knives were the most frequently used devices reported by people with hand OA (Kjeken et al, 2013).
Other strategies studied to a lesser extent include limiting the frequency of performing an activity, taking more time, and getting help from another person (de Boer et al., 2009; Katz and Morris, 2007a; Kjeken et al., 2013). Strategy use has been assessed in different ways which could result in different findings. For example, studies, in which people were shown pictures or given a list of devices or strategies and asked to check which ones they used, found that devices were used more than taking more time or decreasing the frequency of performing certain activities (de Boer et al., 2009; Kjeken et al., 2013; Polluste et al., 2012). Different results were found by Katz and Morris (2007a), who asked about specific strategies used for individual activities. They reported that taking more time to perform activities was the most common strategy used by people with RA followed by limiting the frequency of performing activities. The least used strategies were assistive devices. Other studies suggested that taking more time or limiting the frequency of performing certain activities may lead to changing or stopping the performance of some valued activities (Gignac et al. 2000; Katz and Morris, 2007b; Katz et al., 2006, 2008; Leino et al., 2015; Liu et al., 2016). Indeed, people with RA, OA, and systemic lupus erythematosus (SLE) limited the performance of certain valued activities in efforts to manage their disease (Gignac et al., 2000; Katz et al., 2008; Leino et al., 2015). They spent more time and effort on self-care, household chores, and disease-related activities, including managing medications and medical appointments, which led to decreases in participation in discretionary leisure activities (Gignac et al., 2000; Katz et al., 2006, 2008; Leino et al., 2015). Furthermore, relinquishing valued activities, particularly leisure, has been found to lead to decreased well-being and depression (Gignac et al., 2000; Katz et al., 2007a, 2008; Leino et al., 2015; McDonald et al., 2012; Sandqvist et al., 2005).
Exploration of strategy used by people with chronic rheumatic diseases is important as some strategies may have potentially negative consequences. Research in strategy use has focused on people with more prevalent rheumatic conditions such as RA, OA, and SLE. Yet, systemic sclerosis (SSc), a rare rheumatic connective tissue disease, results in significantly more difficulty performing activities compared to other rheumatic diseases (Jetha et al., 2021; Park et al., 2019). In addition, people with SSc are not referred to occupational therapy (Becetti et al., 2019), yet, express an interest in more information about occupational therapy, daily living, social and psychological support, and coping (Gumuchian et al., 2016; Schouffoer et al., 2011).
SSc is characterized by thickening and fibrosis of the skin, vascular insufficiency (Raynaud’s phenomenon), and involvement of the internal organs (Denton and Khanna, 2017). SSc disproportionately affects women and is more severe in African Americans (Denton and Khanna, 2017). The tight skin can lead to contractures in the fingers (decreased metacarpal phalangeal flexion and decreased proximal interphalangeal extension). Raynaud’s phenomenon, a disruption of blood flow in response to cold or stress, is a symptom present in 95% of people with SSc (Denton and Khanna, 2017). Persistent Raynaud’s attacks can cause tissue damage, and, in severe cases lead to ulcers, gangrene, and auto-amputations in the fingers and toes (Denton and Khanna, 2017). People with SSc can also have decreased lung and cardiac capacity, resulting in fatigue, one of the most disabling symptoms of SSc .Thus, participation in daily activities is compromised which has been reported to be related to pain, fatigue, and depression (Murphy et al., 2021; Peytrignet et al., 2018; Poole et al., 2015; Sandqvist and Eklund, 2008). With disease progression and increases in symptoms such as fatigue and pain, women with SSc reported relinquishing some daily activities while increasing the time spend in others (Sandqvist et al., 2005; Sandqvist and Eklund, 2008). Using assistive devices and taking more time/going slower were explored in a few studies of people with SSc (Sandqvist et al., 2004, 2005). However, it is not known which strategies are used more frequently, whether people with SSc use additional strategies such as assistance or limits on performing activities, or whether strategy use is related to symptoms such as levels of fatigue, pain, or depression. Using devices may improve performance, and reduce pain and fatigue, while taking more time or limiting the frequency of performing valued activities such as leisure may have negative effects on well-being.
Therefore, the purpose of this study was to explore the types of strategies (assistive devices, personal assistance, limits on frequency of performing activities, and taking more time to complete activities) used by people with SSc to perform valued activities. Since strategy use has been found to be related to overall well-being and continued participation in valued activities, this exploratory study will begin to gather information on strategy use in people with SSc. Understanding strategy use may help occupational therapy practitioners support people with SSc to maintain participation and satisfaction with valued activities. In addition, relationships between strategy use and pain, fatigue, depression, and ability to perform daily activities were also assessed.
Method
Approval for this study was obtained from the institution’s Human Research Review Committee. Participants were a convenience sample recruited at the annual Scleroderma Foundation Conference and through announcements posted on the Scleroderma Foundation website. Participants who met the inclusion criteria (diagnosis of SSc and communication skills in English) were sent a letter describing the study and a packet of questionnaires with directions. A follow-up email was sent to participants who did not return or complete the questionnaires within 2 weeks. Consent was implied by returning the questionnaires. This study was conducted and guided by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies (Von Elm et al., 2014).
Outcome measures
Demographic information was collected on age, disease duration, ethnicity, education level, marital status, and employment status. Participants were asked to respond “yes” or “no” to questions regarding the presence of Raynaud’s phenomenon, digital ulcers, lung, and gastrointestinal symptoms, as these symptoms have been reported to affect activity performance (Peytrignet et al., 2018; Sandqvist et al., 2004). In addition, participants rated the severity of pain and fatigue on a visual analog scale from 0 (none) to 10 (severe).
The Health Assessment Questionnaire
The Health Assessment Questionnaire (HAQ) was used to measure difficulty with daily activities (Fries et al., 1980; Khanna et al., 2008; Poole and Steen, 1991). Reliability and validity of the HAQ have been established for people with SSc (Johnson et al., 2005). The HAQ included eight categories: dressing and grooming, arising, eating, walking, hygiene, reach, grip, and outside activity. Items in each category were rated from 0 (no difficulty) to 3 (unable to do). The highest scores from each category were summed and divided by 8 to yield a total score ranging from 0 (no disability) to 3 (severe disability). HAQ scores of 0–1 are generally considered to represent mild to moderate difficulty, 1–2 suggest moderate to severe disability, and 2–3 indicate severe to very severe disability (Khanna et al., 2008).
The Center for Epidemiological Studies Depressive Scale
The Center for Epidemiological Studies Depressive Scale (CES-D; Radloff, 1977) was used to measure depressive symptoms as depression has been linked to decreased participation (Poole et al., 2015; Thombs et al., 2007). Participants rated how often depressive feelings were experienced within the past week from 0 (rarely or none of the time/<1 day) to 3 (most or all of the time/5–7 days). Scores for each item were summed to obtain a total score ranging from 0 to 60; higher scores indicated greater depressive symptoms (Radloff, 1977; Thombs et al., 2007). The CES-D has been shown to be reliable and valid in people with SSc (Thombs et al., 2008).
The Valued Life Activity Scale
The Valued Life Activity Scale (VLA; Katz et al., 2006; Katz and Morris, 2007a) measured strategy use in three main domains of activities: obligatory, committed, and discretionary. Obligatory activities include basic self-care such as dressing, hygiene, and mobility. Committed activities are associated with productive roles, including meal preparation, household maintenance, paid work, and caregiving. Discretionary activities include leisure activities such as hobbies, socialization, sports, gardening, etc. For the activity on the VLA, participants indicated whether they used any of four types of strategies (assistive devices, personal assistance, limits on frequency, and taking more time) to perform each of the activities. More than one strategy could be selected for each activity. We used 28 items from the 33-item VLA that included response options asking whether any of the four types of strategies were used to perform the item. Correlations between the VLA and the HAQ were found to be good to excellent (r = .83) in people with SSc (Poole et al., 2023).
Data analysis
Descriptive statistics were calculated for the demographic and disease symptoms variables, and the HAQ and CES-D. Frequency counts for use of the four strategies were calculated for each VLA item and mean scores were calculated for each category of activity (obligatory, committed, and discretionary). One-way analyses of variance (ANOVA) compared mean strategy use across the three activity categories. Tukey’s Honestly Significance Difference post hoc tests were performed as indicated. IBM SPSS (version 25.0; IBM Corporation, Armon, NY, USA) was used for data analysis. The significance level was set at 0.05. Pearson correlation coefficients were calculated to assess relationships between strategy use and pain, fatigue, the HAQ, and the CES-D. Portney and Watkins (2015) suggested general criteria whereby correlation coefficients from 0.25 to 0.50 represent fair relationships, 0.50 to 0.75 represent moderate to good relationships, and above 0.75 represent good to excellent relationships.
Results
In all, 120 participants met the inclusion criteria and were sent questionnaires; 92 returned the questionnaires for a response rate of 77%. The demographics of the participants are shown in Table 1. The majority of participants were female, White, married, highly educated, had Raynaud’s phenomenon, gastrointestinal symptoms, symptoms of depression, and had minimal to moderate disability on the HAQ. Almost half of the participants had lung involvement while a third reported finger ulcers.
Demographic characteristics and disease symptoms of participants.
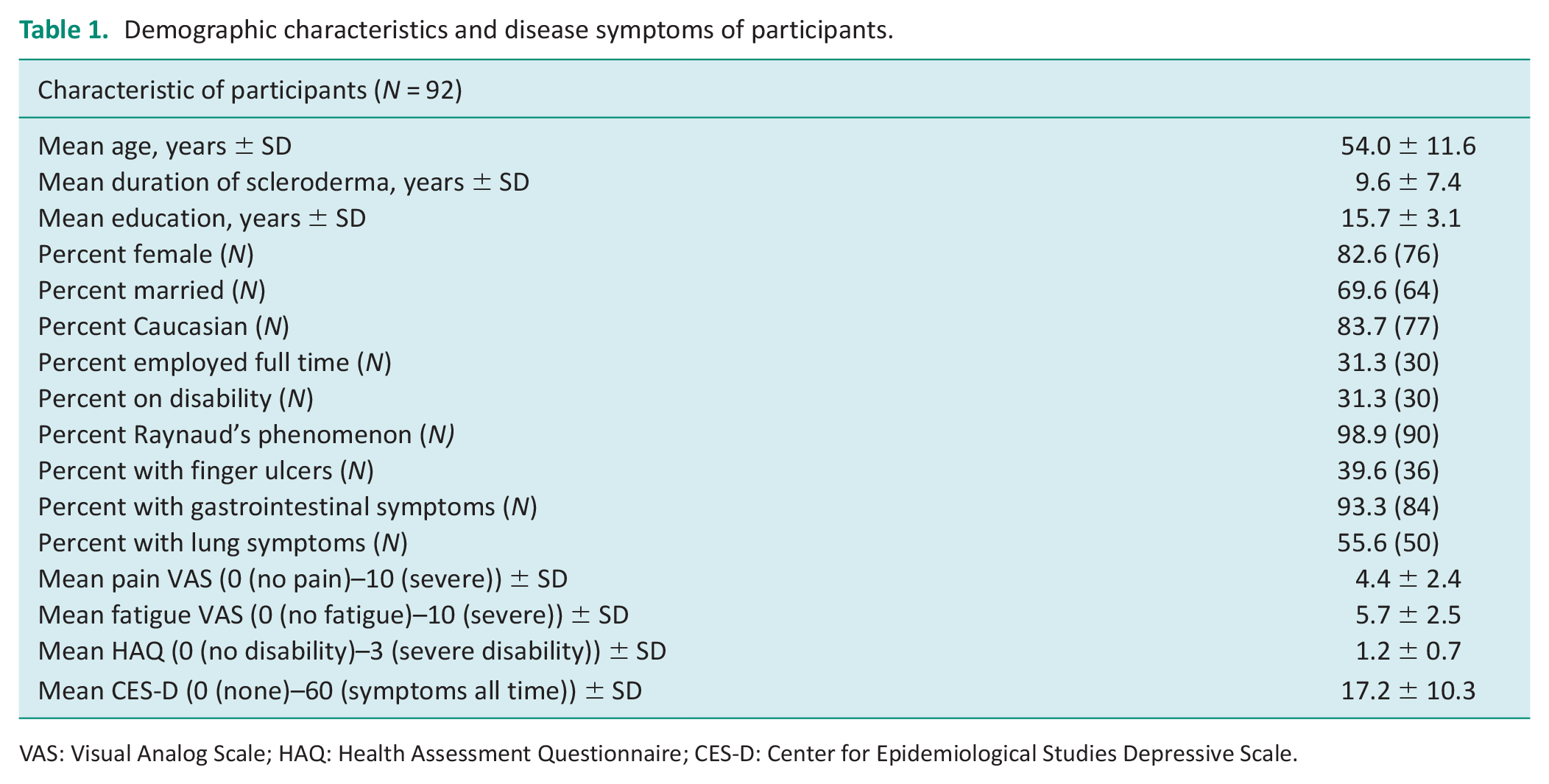
VAS: Visual Analog Scale; HAQ: Health Assessment Questionnaire; CES-D: Center for Epidemiological Studies Depressive Scale.
The number and percentages of participants who used at least one of the four strategies for the different activities on the VLA are shown in Table 2. In general, the most common strategy used for all three categories of activities was taking more time, followed by limiting the frequency of performing the activity. Personal assistance was the least used strategy for obligatory activities, while assistive devices were used the least for committed and discretionary activities.
Strategies used to perform valued activities.
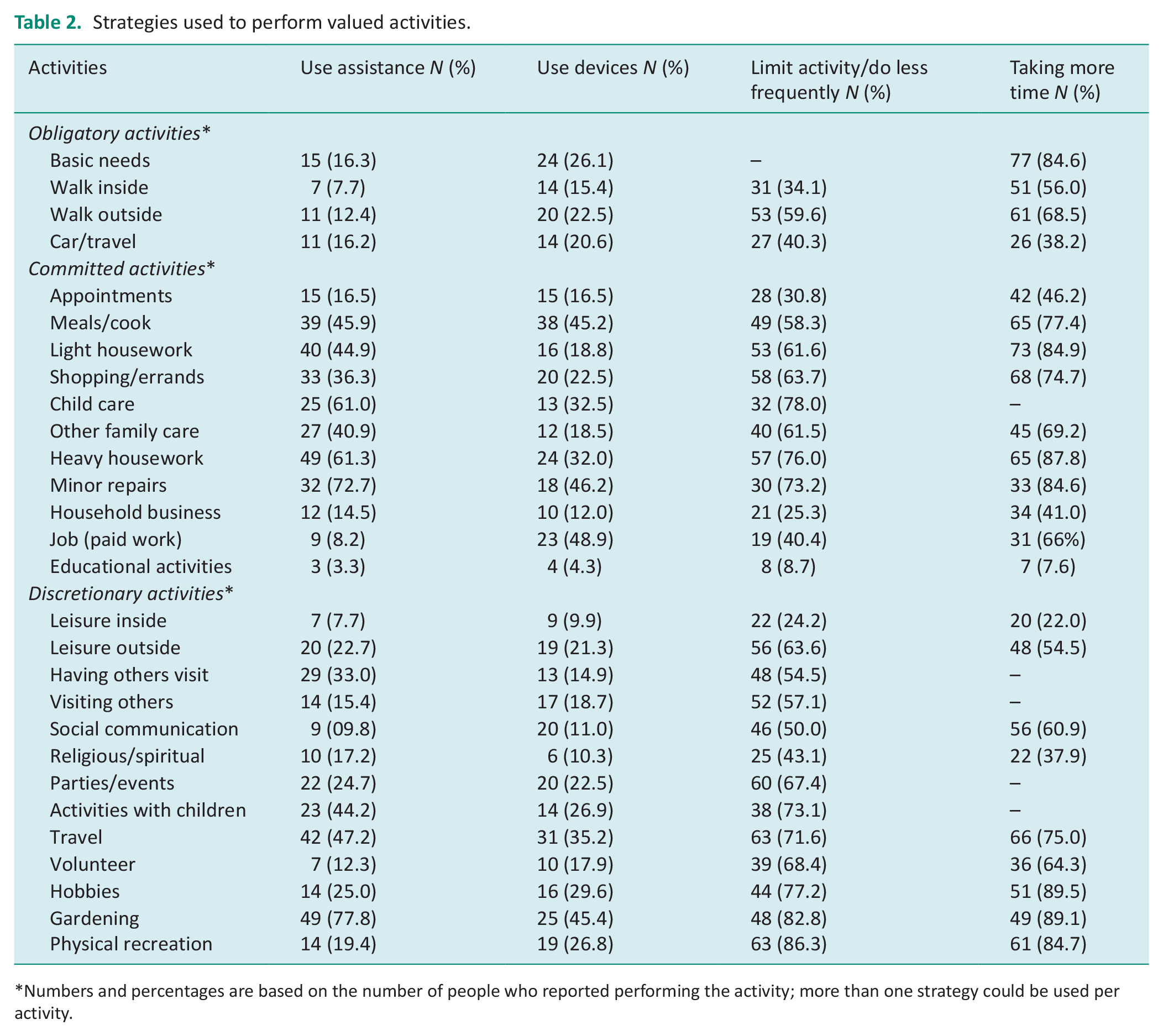
Numbers and percentages are based on the number of people who reported performing the activity; more than one strategy could be used per activity.
Table 3 shows the results from the ANOVA comparing the mean use of strategies for the three categories of activities. There were significant differences in mean total strategy use (F(2,273) = 5.87, p = 0.003), personal assistance (F(2,273) = 20.50, p < 0.001), and limits on the frequency of performing activities (F(2,273) = 4.75, p < 0.009). For the mean total strategy use, significantly more strategies were used for committed activities than for obligatory (p = 0.002) but there were no significant differences in total strategy use for committed activities compared to discretionary (p = 0.124) or for obligatory compared to discretionary activities (p = 0.316). Personal assistance was used significantly more for committed compared to both obligatory (p < 0.001) and discretionary activities (p < 0.001) and more for discretionary compared to obligatory activities (p = 0.034). Participants used the strategy of limiting performance significantly more for discretionary activities than for obligatory (p = 0.011) but not more than for committed activities (p = 0.055). There was no significant difference in limiting performance between committed and discretionary activities (p = 0.822). There were no significant differences across the three categories for taking more time/going slower (F(2,273) = 1.75, p = 0.176) or for assistive device use (F(2,273) = 0.97, p = 0.381).
Comparison of mean strategies for categories of valued life activities.
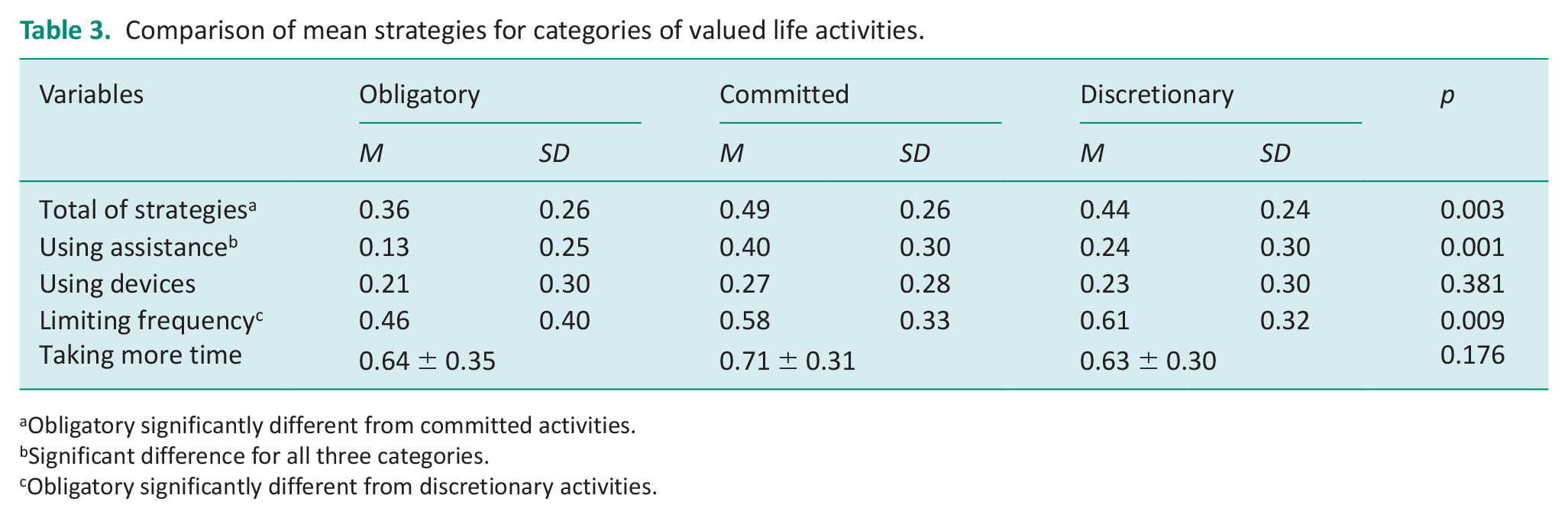
Obligatory significantly different from committed activities.
Significant difference for all three categories.
Obligatory significantly different from discretionary activities.
Table 4 shows the relationships between strategy use and pain, fatigue, disability (HAQ), and depressive symptoms (CES-D). Pearson correlation coefficients showed fair relationships between fatigue and depression and mean total strategy use, assistance, assistive device, and limits on the frequency of performing the activities. There was a fair relationship between the CES-D but not fatigue and the use of more time. Pain and HAQ scores did not correlate with total strategy use or any of the individual strategy use.
Correlations between fatigue, depression, pain and disability, and strategy use.
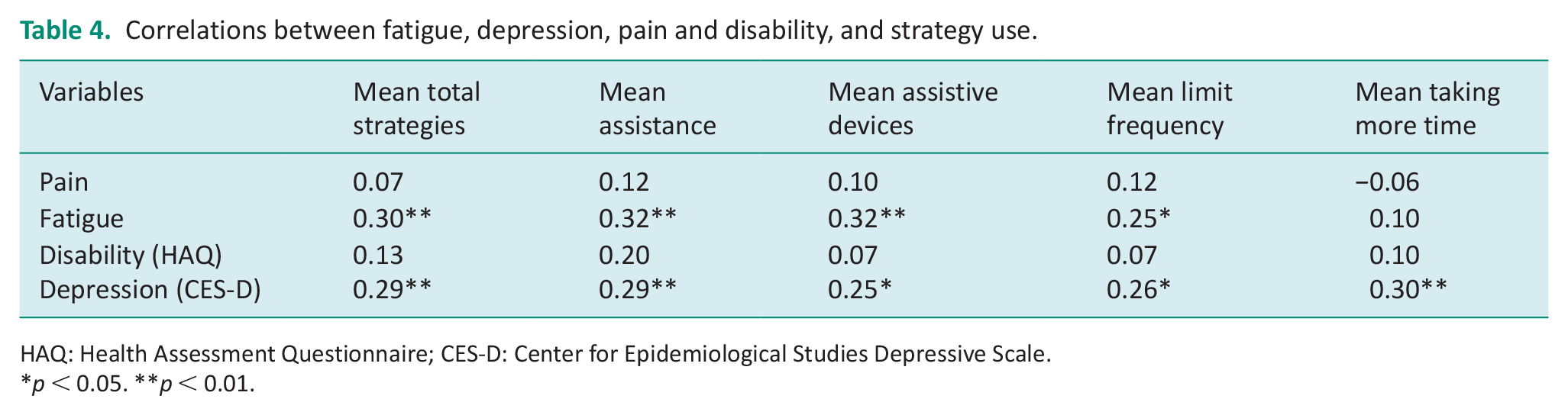
HAQ: Health Assessment Questionnaire; CES-D: Center for Epidemiological Studies Depressive Scale.
p < 0.05. **p < 0.01.
Discussion and implications
To the best of our knowledge, this is the first study that specifically focused on strategies used by people with SSc to perform valued activities. Participants used a variety of strategies to perform valued activities. Taking more time/going slower was the most common strategy reported across all three categories of activities. Taking more time/going slower is often suggested as a pacing strategy to save energy (Backman and Poole, 2020; Leino et al., 2015). This strategy may be easier to implement than obtaining devices, getting personal assistance, or limiting the performance of an activity. Over 80% of our participants reported taking more time for basic needs, light and heavy household tasks, minor repairs, gardening, hobbies, and physical recreation (Table 2). However, studies have reported that taking more time to perform obligatory activities including disease management may lead to reduced participation or the relinquishment of valued discretionary (leisure) activities which have been shown to have negative consequences such as decreased well-being and depression (Gignac et al., 2000; Katz and Morris, 2007b; Leino et al., 2015; Sandqvist et al., 2005).
Limiting the frequency of performing activities was used more than assistive devices or assistance from another person. This strategy was used more for committed and discretionary activities than for obligatory activities similar to findings by others (Katz and Morris, 2007a; Leino et al., 2015; Sandqvist et al. 2004). Specifically, we found that over 50% of people in our study reported limiting the frequency of performing 7/10 committed activities and 11/13 discretionary activities. This finding is not surprising since obligatory activities, including dressing, toileting, hygiene, and mobility, are essential in meeting basic human needs and people want to perform these independently. Furthermore, studies with people with SSc show that committed activities, in particular household activities, are more difficult to perform than obligatory and discretionary leisure activities (Poole et al., 2015; Sandqvist et al., 2005) so people may relinquish or use other strategies. In addition, people may begin to decrease participation in discretionary activities due to the extra time and effort used to perform obligatory and committed (Katz and Morris, 2007a, 2007b) activities.
Our findings regarding assistive device use as a less frequently used strategy were similar to those reported for persons with RA (Katz and Morris, 2007a; Sandqvist et al., 2004). It is possible that assistive devices were used less because they can be costly and/or information and resources for obtaining equipment or training on how to use devices are not easily accessible (Goodacre and Goodacre, 2003; Polluste et al., 2012; Poole et al., 2019). While insurance often does not cover the cost of many devices, several devices for household committed activities are increasingly more commercially available such as larger-handled kitchen tools, electric can openers, food choppers, power tools, ergonomic keyboards, etc. Over 45% of people reported using assistive devices for meals/cooking, minor repairs, and paid work (see Table 2). Studies with people with other rheumatic diseases report increased independence and well-being with assistive device use, especially when people have hand impairments (Kjeken et al, 2013; Sandqvist et al., 2004). However, studies with people with SSc reported that more information was needed on what devices were available and resources for obtaining them (Milette et al., 2019; Poole et al., 2019; Schouffoer et al., 2011).
Personal assistance was also not used as frequently as taking more time and limiting the performance of activities, possibly due to lack of availability or reluctance to ask for help (Goodacre and Goodacre, 2003; Poole et al., 2019). Participants in the current study reported getting assistance from another person more for committed activities than for obligatory and discretionary activities. One reason may be due to the physical demands of many committed activities, which can be a challenge, especially for people with SSc who have decreased lung and cardiac capacity and hand impairments. In addition, it may be easier to ask for help, as many committed activities, such as shopping, meal preparation, and cleaning, are important for, and can affect all household members. Leino et al. (2015) reported that people with RA used assistance for household chores especially those that require more strength such as cleaning and vacuuming. The same study also reported a reduction in leisure due to the time and energy spent on committed household activities. Yet, requiring, negotiating, and asking for assistance has been reported to be associated with feelings of failure, dependency, resentment, being a burden, and “giving in” to the disease (Goodacre and Goodacre, 2003; Gumuchian et al., 2016; Poole et al., 2019). Gignac et al. (2000) suggested that reliance on others has both positive and negative features and exploration of what “help” means to people for different activities and under what conditions help might be viewed positively. Leino et al. (2015) also suggested that cultural role expectations, such as for the performance of household chores by women, may affect whether help is viewed positively or negatively.
The findings from the current study imply occupational therapy as occupational therapy practitioners often recommend taking more time/going slower as pacing strategy to conserve energy when performing activities, yet, taking more time on obligatory activities may cut into time and energy available to spend on other valued activities, such as leisure. This imbalance in time use is associated with stress, depressive symptoms, and lower well-being and life satisfaction in people with rheumatic conditions (Backman, 2004; Gignac et al., 2000; Katz and Morris, 2007b; Sandqvist et al., 2005). As stated above, although people with SSc have significant restrictions in participation in daily activities, they are often not referred to occupational therapy. As such, they do not know what resources and strategies are available. Occupational therapists can evaluate people for a device or other equipment needs, train clients and caregivers on the effective use of devices/equipment to promote independence and provide resources. Furthermore, occupational therapy practitioners may help people prioritize goals and negotiate and explore the positive and negative aspects of different strategies (Goodacre and Goodacre, 2003). Occupational therapy practitioners need to evaluate the difficulties associated with obligatory and committed activities and suggest techniques, assistive devices, exploration of assistance, and environmental modifications to decrease the physical effort associated with these to enable people to continue to participate in other valued activities.
We also found that higher levels of fatigue and depression were related to more strategy use while pain and ability to perform daily activities were not. However, we cannot ascertain whether more strategy use was due to fatigue or depression or vice versa. Future studies could examine whether introducing or changing strategy use would result in less fatigue or depression and increase participation; or whether interventions to reduce fatigue and manage depression would result in less or different strategy use. Future studies could examine whether strategy use and performance of valued activities change with disease progression in SSc. This information could better inform occupational therapy practitioners as to intervention to help people with SSc participate in meaningful activities.
There are several limitations to this study. First, the sample size was small (n = 92). Second, the sample was one of convenience. However, the characteristics of our sample were similar to other studies of people with SSc (Becetti et al., 2019; Khanna et al., 2019; Schouffoer et al., 2011). Third, data collection took place at one point in time so changes in strategy use over time could not be determined. Future studies could examine whether strategies use changes with disease progression and the effect on well-being. Fourth, since participants could select more than one strategy for each activity on the VLA, we could not isolate individual strategy use. Using more than one strategy may be more realistic as to strategy use in the real-world environment, especially with a chronic condition that fluctuates in symptoms and severity. In addition, we did not ask participants open-ended questions about strategy use. Future studies could investigate reasons why participants chose to use the different strategies.
Conclusion
In conclusion, this study investigated strategy use in people with SSc. We found that a variety of adaptive strategies were used to perform VLA. The most frequently used strategies were taking more time and limiting the frequency of performing some activities. Lesser used strategies were assistive devices and personal assistance. People also used strategies more for committed activities. Fatigue and depression were related to strategy use while pain and daily activity performance were not. Information about strategy use is important to gain a more complete understanding of how people perform daily activities and facilitate continued participation in them. Occupational therapy practitioners are the ideal professionals to evaluate and suggest strategy use in people with chronic conditions such as SSc. Further studies are needed to assess the implications of changes in strategy use over time for people with SSc and other chronic diseases to identify strategies that could be improved through occupational therapy interventions.
Key findings
People with SSc use more strategies to perform committed activities than obligatory self-care activities.
The most frequently used strategy was taking more time while the least used strategy was using assistive devices.
What the study added
Previous studies with people with SSc only examined strategies for using assistive devices and taking more time. This study found that people used a variety of strategies to perform daily activities including obligatory, committed, and discretionary activities; however, taking more time was used the most followed by limiting the frequency of performing the activity. The least used strategies were assistive devices and assistance from another person. In addition, more strategies were used for committed activities. Fatigue and depression were related to strategy use, whereas pain and daily activity performance were not.
Footnotes
Acknowledgements
We thank the people with scleroderma for their participation in this study and the Scleroderma Foundation. We would also like to thank Patricia Katz, PhD for allowing us to change the wording on the Valued Life Activities Scale from rheumatoid arthritis to scleroderma for this study.
Research ethics
This study was approved by the Human Research Review Board at the University of New Mexico (approval number 08-256).
Consent
Informed consent was implied by completing the questionnaires as approved by the University of New Mexico Human Research Review Committee.
Consent
Informed consent was implied by completing the questionnaires and approved by the HRRC.
Patient and public involvement data
Patients and public involvement did not occur at any state of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
JLP conceived the study, design and gained ethical approval. All authors (JLP, MPB, AP, and VSH) were involved in the literature search, data collection, data analysis, and were involved in writing and editing the manuscript. All authors approved the final version of the manuscript.