
Abstract
Introduction:
There are over 43,000 occupational therapists across the United Kingdom, with mental health occupational therapists being acknowledged as a main workforce of OT services. However, staff shortages are occurring, and urgent action is needed to retain this important workforce.
Methods:
The systematic literature search was conducted in the CINAHL, PsycINFO and Scopus databases to identify research literature published since 2008. Due to the heterogeneity of the included studies, a narrative synthesis was utilized.
Results:
A total of 20 studies (21 papers) were included in the review. Five thematic factors – well-being at work, organizational work environment factors, job resources, supervision and staffing, along with various subtheme factors emerged from the synthesis. The findings suggest that retaining mental health occupational therapists is a complex issue, affected by many factors. The study emphasizes the triangular relationship among three aspects of well-being (job satisfaction, professional identity and burnout) at work and introduces the concept of a ’Retention Ecosystem’. This illustrates how subtheme factors interconnect and influence the retention of mental health occupational therapists.
Conclusion:
The retention of mental health occupational therapists is revealed to be a multifaceted challenge. There is a need for developing more targeted, meaningful and holistic strategies for retaining the current mental health occupational therapist workforce.
Introduction
Occupational therapy, as a patient-centred health profession, is committed to improving health and well-being through meaningful engagement in various activities. The global presence of over 633,000 practicing occupational therapists, as reported by the World Federation of occupational Therapists (WFOT) (2018) underscores the substantial workforce contributing to healthcare. Collaborating across diverse settings, occupational therapists facilitate individuals, groups and communities in participating in activities that contribute to a fulfilling life (World Federation of Occupational Therapists (WFOT), 2018). With specializations ranging from paediatric to geriatric care, these professionals operate in multiple environments, including hospitals, community services and long-term care facilities (AdventHealth University, 2023). Recognizing the importance of a sufficient number of occupational therapists to meet the population’s needs, further research into workforce dynamics is recommended (Jesus et al., 2023).
In the United Kingdom, occupational therapists are integral to mental health services and are recognized as one of the 14 Allied Health Professions, playing a crucial role in enhancing the daily living of individuals facing mental health challenges (Royal College of Occupational Therapists (RCOT), 2017). Similar recognition exists in Australia (Cook, 2019) and Canada (Canadian Association of Occupational Therapists (CAOT), n.d.), where both acknowledge the critical contribution of occupational therapists in managing mental health issues, particularly during and after the pandemic crisis. Also, despite the fundamental role of occupational therapists in mental health in the United States, their full potential remains largely untapped (American Occupational Therapy Association (AOTA), 2023). Without a concurrent focus on the occupational therapists themselves, the global emphasis on mental health occupational therapy may result in workforce challenges and hinder recruitment and retention in the mental health occupational therapy sector (Rodger et al., 2009).
In the healthcare workforce, job satisfaction is a critical factor influencing staff retention within occupational therapy (Bimpong et al., 2020). Research has shown that staff who are satisfied are less likely to leave their positions compared to those with low satisfaction or who are experiencing burnout (Cosgrave et al., 2018; Mertala et al., 2022). Job satisfaction among mental health occupational therapists (MHOTs) is affected by various factors including workload, support and organizational change, highlighting the intricate nature of their work (Scanlan and Still, 2013). Several studies (Edwards and Dirette, 2010; Roundy et al., 2023) have explored the burnout issues among occupational therapists worldwide, demonstrating that this professional group is considered at high risk for burnout. Considering that burnout frequently impacts medical professionals, examining the role of occupational therapists is essential (Janus et al., 2018). MHOTs, like other health professionals, facing intense workloads and high patient demands, are susceptible to burnout (Painter et al., 2003). They not only face stress like all healthcare workers but also work in less-than-ideal conditions for their specific tasks, such as dealing with distressed individuals and limited patient progress (Painter et al., 2003). These challenges can affect their well-being, therapeutic effectiveness and contributes to retention challenges (Painter et al., 2003; Unison, 2017). However, there have been relatively few studies that specifically investigate burnout among occupational therapists in mental health settings (Lloyd and King, 2004). Furthermore, little is known about the longer-term impacts, such as current workforce shortages, which may deter newcomers from entering the OT field (Haig and Summerfield-Mann, 2016).
Much of the existing research on retention challenges is centred on broader healthcare groups or specific professions such as nursing or physicians, with occupational therapists in mental healthcare systems receiving comparatively less focus. Although some studies have focused on OT retention (Freda, 1992; Millsteed, 2002), there is a noticeable absence of a systematic review that synthesizes evidence on retention factors specifically impacting therapists in mental health services. Occupational therapists are essential to mental health care, playing an important role in service delivery. Considering the adverse effects of high turnover on patient care and safety, it is critical to understand the specific factors that lead to MHOTs considering or deciding to leave their positions. Such insight is vital for developing effective, targeted retention strategies to address this issue.
This study aims to expand current knowledge about MHOTs by reviewing diverse literature to gain a comprehensive understanding of the factors that influence retention among occupational therapists in mental health services, and to inform effective retention strategies for future studies.
Methods
Search strategy and search process
A systematic approach was employed using three databases (CINAHL, PsycInfo and Scopus). The selection of the databases were discussed by all the reviews. The target population of this research is OTs. CINAHL provides specific sources of scholarly materials for allied health professions, including occupational therapists. PsycInfo identifies scholarly literature on psychology and related fields, aligning with the research focus on the mental health field. To broaden the search, Scopus was chosen to find more related literature. The search was divided into two stages.
Preliminary search
Preliminary unstructured searches were undertaken to familiarize ourselves with the topic and refine the search terms. These findings also shaped the introduction of this article.
The initial search indicated that relevant studies were limited and primarily conducted in Australia. As a result, we decided to broaden our research to include OTs working in mental health services across various countries, and the search terms were broadened to ensure that no relevant articles were accidently excluded.
Structure search
To include relevant articles as much as possible and to keep the relevance of the research question, search terms included in the review are followed:
• Occupational therapist (and derivatives) AND
• Retention OR burnout OR turnover OR job satisfaction (and derivatives) AND
• Mental health OR mental health service (and derivatives)
The search was conducted on 26 October 2023. Full details of the search strategy are provided in Supplemental Appendix 1.
Inclusion criteria
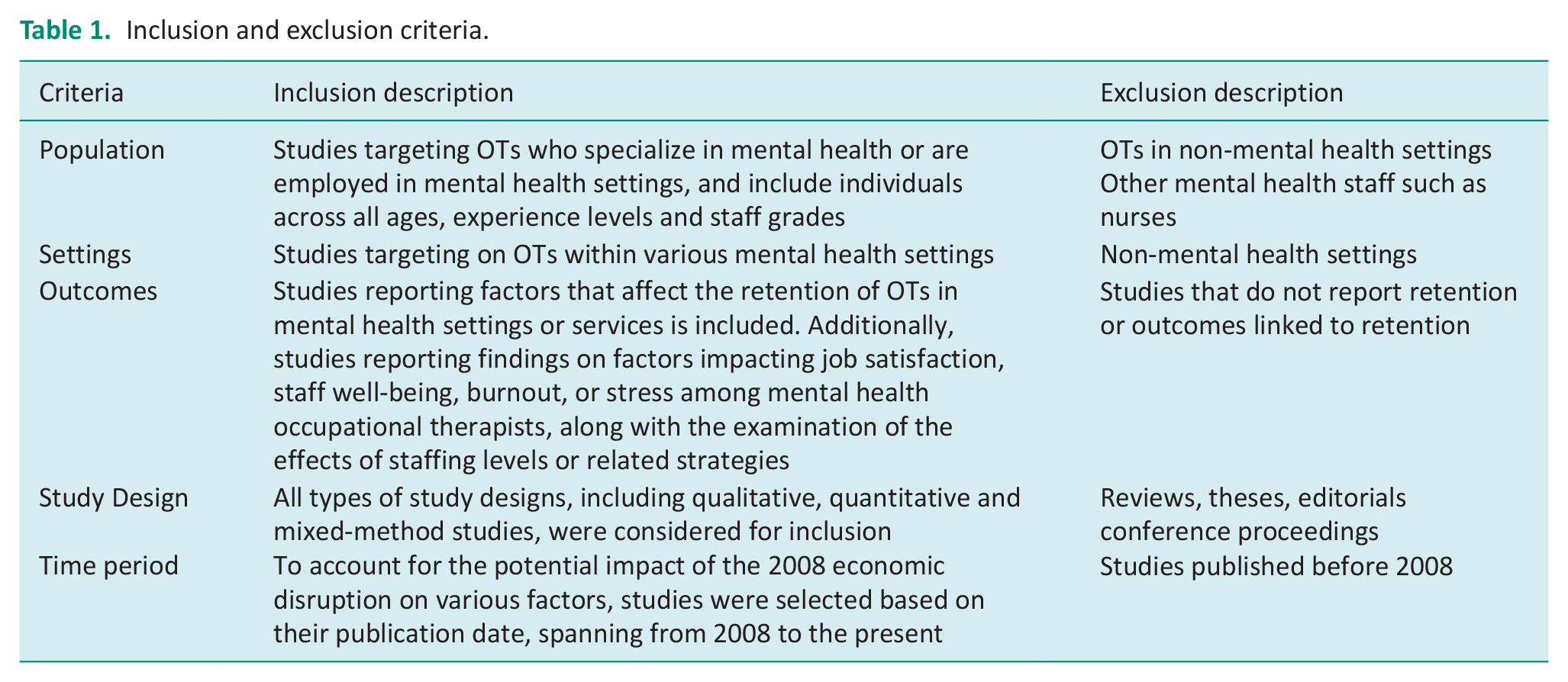
To better align the selection with the research topic and ensure relevance, the criteria outlined in Table 1 were applied. This approach aimed to include a variety of studies on mental health OTs, their working conditions, and retention factors, offering a detailed overview of the field’s current landscape.
Inclusion and exclusion criteria.
Study selection
Search results from three databases were exported to EndNote 21, where duplicates were removed. This was followed by screening titles and abstracts. Full-text articles were then reviewed to select studies meeting the inclusion criteria. This process was collaboratively undertaken by three researchers (WY, EW and SO). Researcher WY took the initial step of downloading and examining full papers of all tentatively selected studies to verify compliance with the inclusion criteria. During the full-text review phase, all researchers thoroughly read each paper and collectively made decisions regarding their eligibility. Additionally, eligible studies were also identified by screening the reference lists of related studies, and a manual search was conducted to find relevant literature.
Data extraction
Data were extracted using an excel spreadsheet designed specifically to gather the necessary information to answer the research question. The extracted data included the study design, study population, country of study, setting of the study, main findings and the authors’ conclusions. Regarding the study population, only data pertaining to MHOTs were extracted; data on study participants who were not occupational therapists were not included in the table. The research process was primarily conducted by researcher WY, in collaboration with researchers SO and EW. Discrepancies was identified and resolved through discussion.
Quality assessment
Assessing the methodological quality of the included papers is essential for ensuring the reliability and validity of the synthesized evidence. Due to the heterogeneity of the included articles, quality assurance was conducted utilizing established tools tailored to the included specific studies methods.
The Joanna Briggs Institute (JBI) Critical Appraisal Tools for Qualitative Research (Lockwood et al., 2015) was used to assess the quality of qualitative studies. AXIS critical appraisal of cross-sectional Studies (Downes et al., 2016) was used to assess the quality of all quantitative survey studies. The Mixed-Methods Appraisal Tool (MMAT) tool version 2018 (Hong et al., 2018) was used to appraise mixed-method studies.
Disagreements among review authors regarding the quality assessment of specific studies were resolved through discussion. It is important to note that while the assessed quality of the articles will be thoroughly commented on in the review, no articles will be excluded based on quality criteria, ensuring a comprehensive representation of the available evidence.
Data synthesis
This research employs narrative synthesis approach to present its finding, due to the significant diversity observed among the selected studies in terms of study design, the validated surveys or scales employed, data collection methods and the outcomes reported. Given this diversity, a meta-analysis is deemed unsuitable for this report. Instead, a narrative approach is chosen, allowing for the analysis of relationships within individual studies and between different studies (Popay et al., 2006). We chose the narrative approach as our primary method for conducting the synthesis. To complement this, we also employed thematic synthesis, which allowed us to analyse differences between cases (Zelčāne and Pipere, 2023).
To incorporate quantitative findings into our narrative synthesis, we utilized a technique known as ‘qualitization of data’, as outlined by Pluye and Hong (2014). This process transforms statistical data gathered from surveys, questionnaires and secondary data sets into text. This methodological choice ensures a comprehensive understanding of the synthesized evidence, contributing to the rigour of this research. The data transformation process can be seen in Supplemental Appendix 2 in the supplementary resources.
Results
Search results and study selection
In the initial search, a total of 1218 papers were identified. By removing duplicates, 80 papers were excluded. Subsequently, 991 papers were eliminated after title review and 83 more were excluded following abstract review. After a full-text assessment, 45 additional papers were excluded due to lack of relevance. In full-text review stage, we also found an overlap between two studies (Ceramidas et al., 2009; Ceramidas, 2010). In Ceramidas (2010), the author extracted the Australian results from Ceramidas et al. (2009) and provided a more detailed description. Therefore, we decided to combine them into one entry as one of the included studies. The selected articles were supplemented by searches for citations and references. In the final stage, 20 articles were included. Additionally, one more article was identified from the references cited within the selected studies, bringing the total number of included papers to 21, with the total number of included studies remaining at 20. For an overview of the study selection process, please see Figure 1.
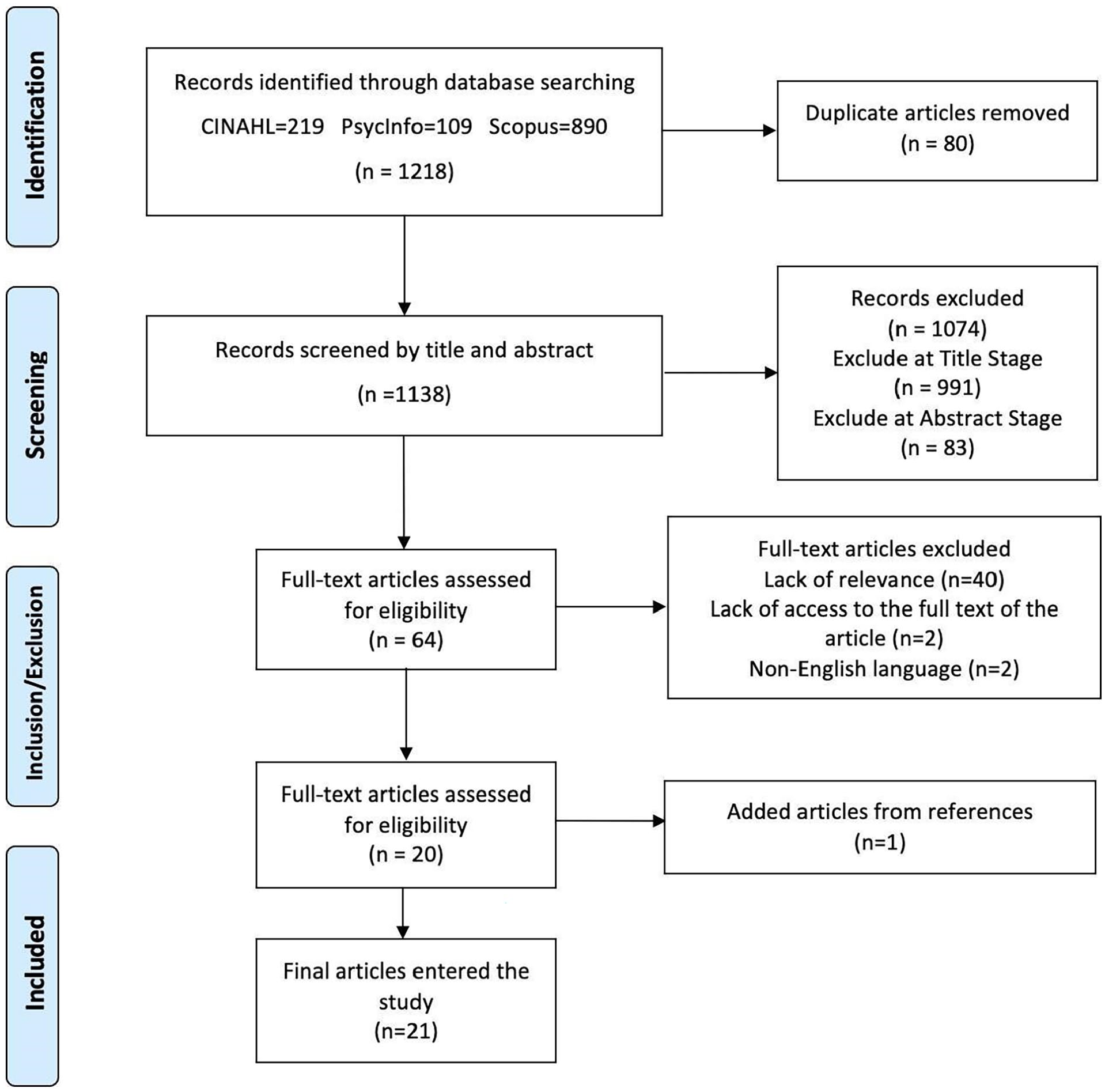
Study selection process.
Description of the included studies
Table 2 presents characteristics of 21 peer-reviewed papers since 2008, involving 1069 MHOTs, excluding unspecified numbers in Phoenix and Taylor (2023) and Ceramidas et al. (2009). Conducted across six countries, with the majority in Australia (10), followed by the United Kingdom (4), Sweden (2), Ireland, the USA, Turkey and Bahrain (1 each). The mental health services included in the studies comprised state-run or territory-run Mental Health Services, Ministry of Mental Health Services, NHS, Mental Health NGOs, Psychiatric Services and Private Services. The studies were conducted in different settings within the mental health services: over half of the studies (N = 11) were conducted in settings including community mental health service, while the others included Inpatient Settings (acute wards, forensic wards, etc.), and psychiatric clinics.
Study characteristic.
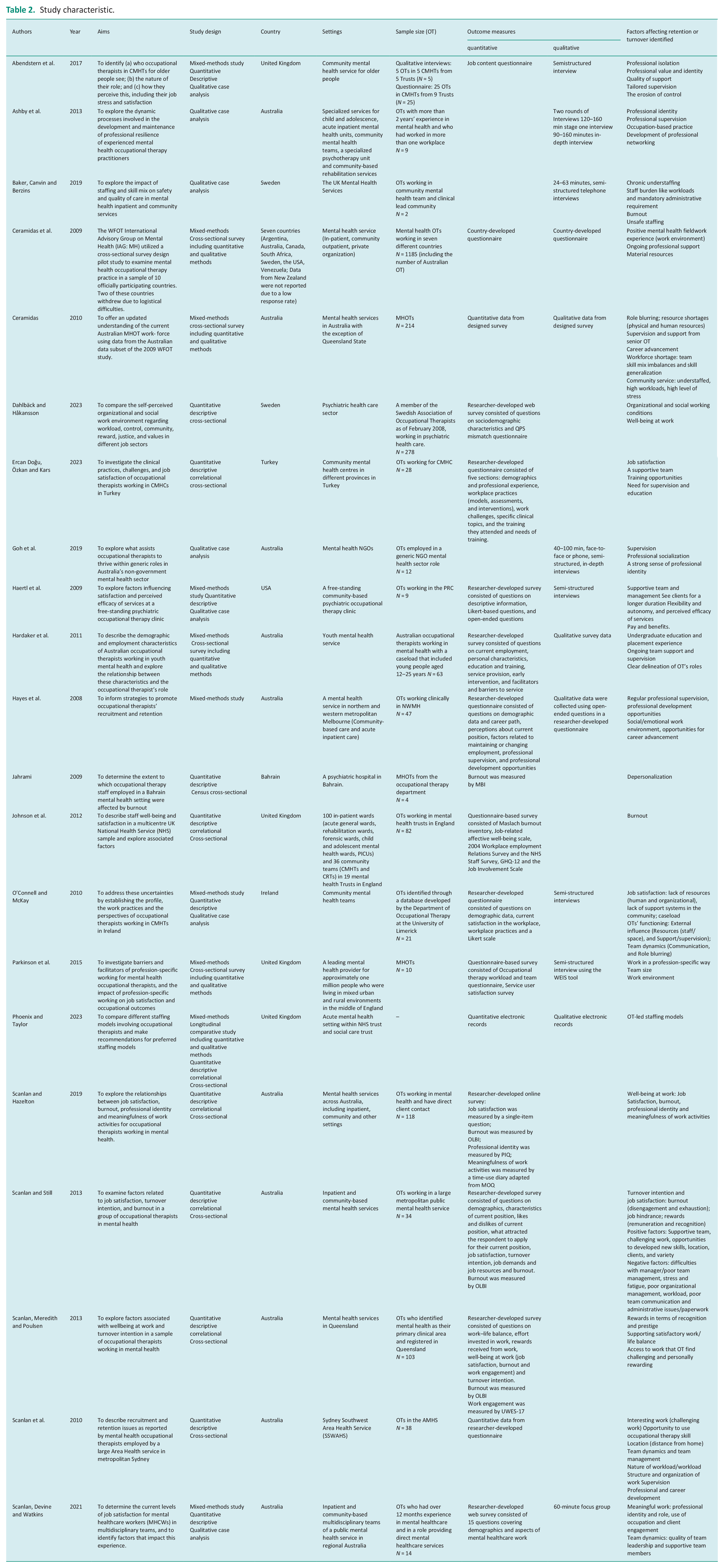
This review includes different study designs: nine mixed-methods, eight quantitative and three qualitative. Quantitative studies were cross-sectional, utilizing surveys or questionnaires, while qualitative studies were all case studies conducting 40–100 minutes in-depth interviews with MHOTs.
Only five studies (Ashby et al., 2013; Hayes et al., 2008; Scanlan et al., 2010; Scanlan et al., 2013; Scanlan and Still, 2013) directly investigated factors influencing MHOTs’ retention, turnover intention and resilience. The other studies, while focusing on areas like job satisfaction, burnout and work environment, still provided valuable insights into retention determinants. This diversity in design and focus resulted in a wide range of outcome metrics.
Quality assessment
The included studies were categorized into three study designs: (1) Qualitative research (n = 3; Ashby et al. 2013; Baker et al. 2019; Goh et al. 2019) (2) Quantitative descriptive research (n = 8; Dahlbäck and Hakansson, 2023; Ercan Doğu et al., 2023; Jahrami, 2009; Johnson et al., 2012; Scanlan et al., 2010, 2013; Scanlan and Hazelton, 2019; Scanlan and Still, 2013) (3) Mixed-method research (n = 10) (Abendstern et al., 2017; Ceramidas et al., 2009; Ceramidas, 2010; Hardaker et al., 2011; Hayes et al., 2008; Haertl et al., 2009; O’Connell and McKay, 2010; Parkinson et al., 2015; Phoenix and Taylor, 2023; Scanlan et al., 2021). Details of the individual assessments for each category and the specific studies are available in Supplemental Appendix 3 of the supplementary documents.
In the assessment of qualitative research studies, a cut-off point was set where at least six out of 10 questions needed to be answered with ‘yes’ (6/10) to indicate that the study is of high quality (Nan et al., 2022). All included qualitative studies achieved a score of 8 but lacked details on the researchers’ backgrounds (Q6 & Q7).
In evaluating quantitative studies, AXIS differentiated their quality into high (70–100%), fair (60%–69.9%), and low (0%–59.9%) categories. Although all studies fell into the high category (70%–85%), only three were likely representative of the intended population (Dahlbäck and Hakansson, 2023; Ercan Doğu et al., 2023; Jahrami, 2009;), and just two addressed non-response bias concerns (Jahrami, 2009; Johnson et al., 2012). Furthermore, one study’s (Scanlan and Hazelton, 2019) sampling and selection methods were deemed suboptimal, noting that surveys targeted occupational therapists in leadership roles with an ‘at arm’s length’ recruitment approach.
Mixed-method studies varied in quality (40%–100%), with all qualitative components meeting criteria except for two studies (Hardaker et al., 2011; Parkinson et al., 2015) with insufficient qualitative data interpretation. Five studies (Abendstern et al., 2017; Hayes et al., 2008; Parkinson et al., 2015; Phoenix and Taylor, 2023; Scanlan et al., 2021) failed to represent the target population adequately due to limited setting descriptions and small sizes, and only three studies (Hayes et al., 2008; Haertl et al., 2009; Parkinson et al., 2015) were considered to not have a low response rate.
In conclusion, the quality of the studies was not very satisfactory but reached an acceptable level. Although the quality of some studies, such as Parkinson et al. (2015), is relatively poor, no study was excluded, aiming to offer a broad view of factors affecting MHOT retention.
Findings
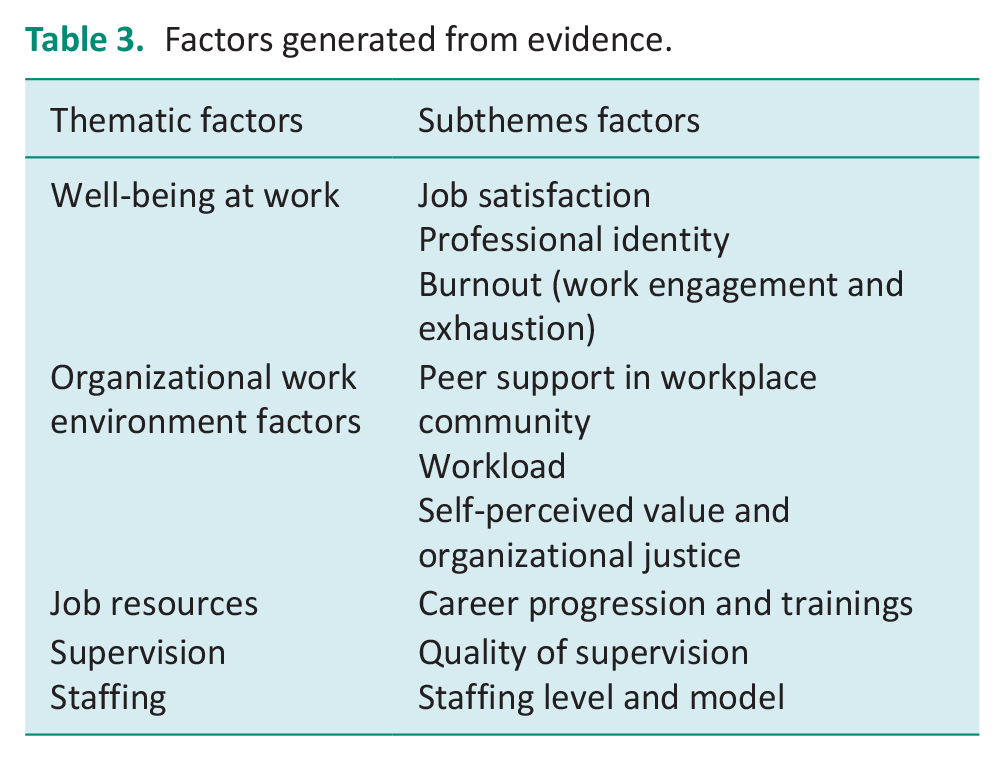
Research has identified a range of factors affecting the retention of MHOTs, with certain factors recurrently mentioned across multiple studies. To better identify the factors impacting MHOT retention across studies and to compile the evidence, various factors have been listed in Supplemental Appendix 4. To better interpret the collected evidence, we categorized the factors to answer the research question (See Table 3).
Factors generated from evidence.
Theme 1: Well-being at work – Job satisfaction, Professional Identity and Burnout (work management and exhaustion)
Well-being at work is essential for retaining MHOTs and consists of three primary components: job satisfaction, professional identity and burnout (Scanlan and Still, 2013). Burnout itself includes work engagement and exhaustion (Scanlan et al., 2013; Scanlan and Hazelton, 2019). Several factors have been identified that impact well-being at work, and there are also interrelationships among the three aspects.
Job satisfaction
Job satisfaction is the overall happiness and fulfillment one feels in their work, identified as key in lowering turnover intentions and enhancing workplace well-being (Scanlan et al., 2013).
Support is the most significant factor impacting job satisfaction, with five studies (Ercan Doğu et al., 2023; Haertl et al., 2009; O’Connell and McKay, 2010; Scanlan and Hazelton, 2019; Scanlan et al., 2021) directly identifying support from colleagues, teams and leaders as crucial for safeguarding job satisfaction. In contrast, challenges with managers can increase MHOTs’ intent to leave, as found in the study by Scanlan et al. (2013).
Another factor emphasized by MHOTs was the use and practice of OT-specific skills. Studies (Parkinson et al., 2015; Scanlan and Hazelton, 2019) show higher satisfaction when roles are primarily OT-focused. One study (Goh et al., 2019) particularly suggested NGOs could boost MHOTs’ satisfaction by valuing their profession-specific skills. But this doesn’t imply MHOTs should only undertake OT-specific tasks and avoid generic duties. As one participant stated:
When I am doing generic work . . . I am always an OT at some level. I’m quite comfortable with that. I am focusing on people’s functional abilities. I am focusing on the way they are relating to people, how independent they are. I am always doing that. (Participant H in Abendstern et al., p.26)
However, it is not advisable to overload MHOTs with generic roles, as an experienced MHOT from a public sector stated:
The MHOT role is becoming more generic, and we are at risk of losing some of our core OT skills unless we can retain experienced OTs to mentor and guide new OTs. (Abendstern et al., p.413)
Abendstern et al. (2017) concluded finding a balance between specialist and generic roles for MHOTs could lead to greater job satisfaction among MHOTs and may be beneficial for workforce retention and recruitment.
Job resource is another critical factor in job satisfaction, including rewards and supervision. Interestingly, rewards aren’t just monetary, MHOTs satisfied with their pay sometimes report lower job satisfaction (Scanlan and Hazelton, 2019). They prioritize non-monetary rewards like recognition, prestige and acknowledgement from managers and peers colleagues (Scanlan et al., 2013; Scanlan and Hazelton, 2019).
Meanwhile, MHOTs can find job satisfaction through meaningful work and patient engagement (Scanlan and Hazelton, 2019; Scanlan et al., 2021). Studies (Haertl et al., 2009; Scanlan et al., 2021) have pointed out that engagement with patients could facilitate job satisfaction for MHOTs. Because MHOTs can achieve job satisfaction when working directly with clients (Scanlan et al., 2021) and when they are able to see clients for a longer duration (Haertl et al., 2009). This may be due to the nature of OT work, which emphasizes client-centred practice.
Professional identity
Research consistently indicates that maintaining professional identity is crucial for MHOTs, affecting job satisfaction and retention. Studies (Ashby et al., 2013; Scanlan et al., 2010; Ceramidas, 2010; Parkinson et al., 2015; Phoenix and Taylor, 2023; Scanlan and Hazelton, 2019; Scanlan et al., 2021) have documented the erosion of this identity when OTs engage in tasks outside their specialized field. A comparative study by Phoenix and Taylor (2023) evaluated two different staffing models: an OT-led team and an experimental model incorporating OTs into ward shift numbers. The experimental model was associated with a lack of professional identity, which correlated with poor retention rates. Some OTs reported, ’OTs are too busy doing non-OT work’. This lack or loss of professional identity was also described in other studies as a reduction in MHOTs’ roles (Scanlan et al., 2021) or role blurring with a nursing focus instead of an OT focus (Ceramidas, 2010).
Scanlan and Hazelton (2019) using the Professional Identity Questionnaire (PIQ), found that only 35.6% of occupational therapists felt their work was primarily OT- focused. Further analysis identified a significant statistical correlation was found between the meaningfulness of work activities (value to self) and professional identity, suggesting that professional identity could be enhanced by allocating work tasks based on individual occupational therapists’ preferences, thereby optimizing valued activities and dividing the workload.
Further emphasizing the importance of role-specific work, Parkinson et al. (2015) observed that MHOTs engaged in occupation-centric tasks tend to have a more positive views on their roles. Thus, reinforcing the core efficacy of occupational therapy and providing opportunities to utilize specific OT skills is fundamental in preserving professional identity and fostering resilience (Ashby et al., 2013; Scanlan et al., 2010).
Burnout (work engagement and exhaustion)
Burnout was found to have a statistical correlation with MHOTs’ turnover intentions (Scanlan and Hazelton, 2019). Two studies indicated a significant risk of burnout among OTs. In the studies by Johnson et al. (2012) investigating the mental health workforce in England, OTs were one of two professions that reached the high burnout threshold. Similar to Jahrami (2009), which reported that MHOTs were found to have higher levels of burnout and depersonalization among the mental health workforces.
Two other studies discussed the factors related to work engagement and exhaustion. Feelings of stress/fatigue and the demands of contact with service users and their families were identified as factors associated with higher disengagement and exhaustion, as well as increased burnout. Conversely, factors such as supervisor support, feedback, participation in decision-making and opportunities for involvement in research or quality improvement are linked to lower levels of burnout (Scanlan and Hazelton, 2019). Effort was identified as a factor with a mixed pattern (Scanlan et al., 2013). High effort was associated with greater exhaustion, but high effort accompanied by high rewards may have a positive impact on work engagement, as rewards can motivate people to engage in their roles more fully (Scanlan et al., 2013).
Theme 2: Organizational work environment factors
MHOTs’ decision to stay in their positions is greatly influenced by their work environment, shaping how they view their professional experiences, including workload, workplace relationships and feeling valued and treated fairly (Dahlbäck and Hakansson, 2023). Therefore, this theme is consisted of three subthemes: workplace community, workload, value and justice.
Peer support in workplace community
Support from colleagues, managers and team is considered as the most important components within workplace community, of seven studies identified this (Abendstern et al. 2017; Dahlbäck and Hakansson 2023; Haertl et al. 2009; Hardaker et al. 2011; Scanlan et al. 2010; Scanlan et al., 2021; Scanlan and Hazelton 2019). Team dynamic is essential for MHOTs, and a supportive team was influenced by qualities of colleagues and leaders:
It’s about having the right fit for the team rather than the right set of skills for the team. Skills can be learnt, but personalities can make or break a supportive team. (A community-based OT in Scanlan et al., p.83)
However, one study reported that among all sectors, OTs working in psychiatric healthcare reported the most negative attitudes towards their workplace community (Dahlbäck and Hakansson 2023). Studies have found that MHOTs who face difficulties with managers or work within unsupportive or dysfunctional teams are more likely to leave their jobs (Scanlan et al., 2010; Scanlan and Hazelton, 2019). Conversely, MHOTs who are part of a supportive team and have supportive management are better able to engage with their positions (Hardaker et al., 2011; Haertl et al. 2009).
The social work environment is also related to MHOTs’ retention issues (Hayes et al. 2008), and professional socialization was identified as an important component in this matter, considered a useful strategy for maintaining therapists (Ashby et al. 2013; Goh et al. 2019). Professional socialization includes informal and formal professional networks, acting as ’protective factors’ for MHOTs to feel consolidated within their profession. Offering professional supervision by an occupational therapy colleague and developing professional networks are discussed as effective strategies to support MHOTs (Ashby et al. 2013; Goh et al. 2019).
Workload
While ‘workload’ is an objective term, in this context, we are concentrating on MHOT’s perceptions of their workload and its characteristics. Unfavourable workload conditions, such as high workloads and insufficient time, have been identified by MHOTs as factors that can negatively impact their retention (Ceramidas, 2010; Dahlbäck and Hakansson, 2023; Hayes et al., 2008; Scanlan et al., 2010). In a survey assessing workload, OTs in psychiatric healthcare reported a more unfavourable workload compared to those in other sectors (Dahlbäck and Hakansson, 2023). Ceramidas (2010) highlighted understaffing as a primary cause of high workloads and insufficient time. Furthermore, the nature of the workload is also considered crucial for MHOTs, with more engaging work being seen as a positive aspect for their job satisfaction (Scanlan et al. 2010).
Self-perceived value and organizational justice
Self-perceived value refers to those that are consistent between personal and workplace values, and trust in management’s future handling and willingness to recommend the workplace to others (Dahlbäck and Hakansson, 2023), and organizational justice is a term which means employees’ perceptions of fairness in the workplace (Greenberg, 1987), such as managerial impartiality and a willingness to prioritize addressing obstacles (Dahlbäck and Hakansson, 2023). Both the presence of conflicts between personal and workplace values and experiences of unfair treatment signal poor conditions in the work environment. Aspects of value and justice were identified in one study as factors affecting retention (Dahlbäck and Hakansson, 2023), indicating that OTs in psychiatric care reported the lowest means with regard to value and justice.
Theme 3: Job resources
Career progression and trainings
Job resources were explored in six studies (Ceramidas, 2010; Hardaker et al., 2011; Hayes et al., 2008; O’Connell and McKay, 2010; Scanlan et al., 2010; Scanlan and Hazelton, 2019), including the opportunities for career progression and trainings. People who want to advance in their career or seek for new challenges at work are more likely to think about quitting their job than those who don’t have that as a reason (Scanlan et al., 2010; Scanlan and Hazelton, 2019), which means if there is more progression opportunities or challenging role for MHOTs, they are more likely to stay in their role. MHOTs are also interested in receiving continued professional development (CPD) practise and having opportunities for skill development (Hardaker et al., 2011; Scanlan et al., 2010) and have a strong training need. However, this cannot be fulfilled all the time due to the heavy workloads or pressure from management or funding and other limited resources (Hardaker et al., 2011).
Theme 4: Supervision
Quality of supervision
While supervision is discussed within workplace communities and is seen as a form of professional socialization (Ashby et al., 2013), studies have focused on it differently. Simply providing supervision is not sufficient for retaining the workforce, and the quality of supervision appears to be more significant for MHOTs, particularly for those with less experience. Two studies (Abendstern et al., 2017; Ceramidas, 2010) highlight the critical impact of high-quality supervision on the likelihood of OT students pursuing work in the field of post-graduation and sustaining their job satisfaction. MHOTs in Hayes et al. (2008) reported having different supervision needs at various grades. For instance, as their grades increased, the focus on clinical issues decreased due to their increased clinical experience. Furthermore, access to supervision is a barrier for MHOTs, such as the supervisor’s lack of availability (Abendstern et al., 2017), and irregular supervision due to time constraints (Scanlan et al., 2010). Therefore, O’Connell and McKay (2010) suggested providing appropriate and timely supervision for MHOTs of all grades.
Theme 5: Staffing
Staffing level and model
Three studies have discussed staffing issues (Baker et al., 2019; Ceramidas, 2010; Phoenix and Taylor, 2023). The shortage of human resources not only affects staffing levels but also increases pressure on inexperienced OTs and adds to the workload of the remaining OTs, which can decrease their job satisfaction (Ceramidas, 2010). Thus, the terms ‘unsafe staffing’ and ‘chronic understaffing’ have been used to describe this ‘vicious circle’ (Baker et al., 2019). Moreover, a recent study showed that MHOTs working in OT-led teams had a better work experience, because this arrangement can foster a therapeutic atmosphere (Phoenix and Taylor, 2023).
Discussion
This review identifies various factors influencing retention, categorized into themes such as work well-being, organizational environment, job resources, supervision and staffing. It highlights the complex interplay between these factors and their combined influence on MHOTs’ decisions to stay or leave, offering key insights from a broader perspective. The key messages and findings for MHOTs are outlined below.
The triangular relationship of well-being at work
Central to our findings is the triangular relationship between job satisfaction, professional identity and burnout. Job satisfaction, professional identity and burnout are three aspects of well-being at work that are emphasized the most among all included studies. Job satisfaction is crucial for keeping MHOTs in their roles, and it’s greatly affected by the support they receive from colleagues and their ability to do work that is meaningful and specific to their profession.
Closely linked to job satisfaction is the concept of professional identity, which in the context of MHOTs, is tied to their ability to apply specialized occupational therapy skills. What we’ve found is that when these therapists feel like they’re losing their professional identity, they might start to feel less committed to their jobs, which could make them burn out. Conversely, a robust professional identity seems to act as a protective barrier, mitigating job stress and fostering resilience.
Burnout, a critical issue defined by Maslach and Leiter (2016) as exhaustion and disconnection from occupational values, emerging as a critical outcome of the negative interactions between job satisfaction and professional identity. This loss of connection can cause a bunch of negative outcomes, including reduced patient care quality and higher turnover rates.
Research has investigated the relationship between professional identity and burnout (Edwards and Dirette, 2010), between professional identity and job satisfaction (Scanlan et al., 2013), and between job satisfaction and burnout (Scanlan and Still, 2013; Scanlan and Hazelton, 2019). However, our review has suggested a triangular relationship among job satisfaction, professional identity and burnout. Therefore, further exploration of the interrelationships, bidirectional influences, or causal connections within the context of workplace well-being for MHOTs would be helpful to aid in the strategic support of MHOTs.
The retention ecosystem and the ripple effect of subtheme factors
While subtheme factors may contribute to turnover intentions and therefore impact retention, interactions among them may also play a role. Researchers have already found that the factors influencing the retention of mental health staff are complex but have an important impact on overall retention (Long et al., 2023). Each factor does not exist in isolation but rather has the potential to influence and amplify others. To better explain how these observed factors impact retention, either individually or in combination, we introduce the concept of a ‘Retention Ecosystem’ – a network where each element can initiate a chain reaction, contributing to a complex interplay of influences. It is hard to streamline every interactions within this ‘retention ecosystem’, but we still find some clues to explain them. Our findings indicate ‘impact on wellbeing at work’ consistently emerges as a core factor affecting an MHOT’s decision to stay or leave, and the triangular relationship of well-being at work acts as the foundation of this ecosystem. The subthemes factors identified in the findings influence the Retention Ecosystem, either contributing to its stability or causing disruptions. For instance, inadequate staffing does not simply increase workload, it can erode the professional identity by forcing MHOTs into generalized roles and dilute job satisfaction by creating an unsustainable work environment, thus amplifying the risk of burnout and destabilizing the ecosystem. Meanwhile, good supervision, chances to grow professionally and CPD do more than help individuals, they’re crucial for keeping this ecosystem healthy and are especially helpful for those who are new to the profession to build up their professional identity, which has the potential to create positive reaction throughout the ecosystem.
The broader implications for retention
Within this retention ecosystem framework, it’s evident that MHOTs’ desire to leave isn’t driven by a single stressor but by the combined effect of multiple factors. This insight highlights the need for specific strategies tailored to the unique experiences of MHOTs, rather than relying on generic solutions. Therefore, healthcare organizations must rethink about approaches to retaining MHOTs. In this study, we propose that MHOT retention could be improved by
(1) Development of a comprehensive support system: This involves establishing peer support groups and mentorship programmes in both structured and casual settings, as well as creating ways to foster a more positive social and emotional work environment.
(2) Development of career ladders: Clear pathways, especially the long-term career paths for professional growth can provide MHOTs with a sense of progression and future within their roles, which is essential for long-term retention. Particularly focusing on training and replacement opportunities for new OT graduates and developing strategies to offer work variety, challenges and skill development.
(3) Strategies for strengthening professional identity: Effective approaches are needed to motivate occupational therapists to use OT-specific skills, while also making sure that these skills are acknowledged and appreciated by other professions and management. It’s also important to find the right balance between specialized and general roles for mental health occupational therapists.
(4) Strategies for workload management: Effective strategies to manage workloads include delegating appropriate tasks to support staff or less-experienced team members, with proper training provided. Focus on hiring both new graduates and experienced therapists to maintain adequate staffing levels and implement flexible staffing models to adjust to changing work demands.
Study limitations
One limitation of this study is the exclusion of grey literature, which may mean that the evidence collected is not fully comprehensive. On the other hand, a strength of this review is its inclusion of studies from various countries, offering a global perspective. However, with nearly half of the papers coming from Australia, the generalizability of some findings to MHOTs working in the United Kingdom, especially within the NHS, may be limited. Another constraint is the predominant use of cross-sectional study designs. While they have identified certain factors influencing MHOT retention, the constantly evolving nature of global health environments means that these factors’ impact on retention can change over time. As a result, some factors identified in this review may not hold the same weight for today’s workforce, while others may have gained importance. Furthermore, given the variety within the mental health service sector, each with its unique therapeutic focus and patient characteristics, there is a clear need for more research. Such research should explore retention factors specific to different sectors within mental health services, to develop more targeted, meaningful and detailed strategies for the current workforce.
Conclusion
Understanding the retention ecosystem is important for healthcare organizations to improve MHOT retention. It requires a holistic approach that recognizes the interconnected nature of the factors at play. Our analysis underlines those policies aimed at improving job satisfaction, preserving professional identity and fostering a supportive work environment that is key to successfully retaining MHOTs.
Key findings
A triangular relationship within well-being at work and the concept of the ‘retention ecosystem’ has been identified.
Future research needs to consistently focus on MHOT workforce across various mental health sectors.
What the study has added
Findings from this study indicate that the retention of MHOTs is a multifaceted challenge, and there is a need to explore the retention ecosystem in order to develop more holistic strategies for the current MHOT workforce.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226241288157 – Supplemental material for Factors affecting retention of occupational therapists in adult mental health service: A systematic review with narrative synthesis
Supplemental material, sj-docx-1-bjo-10.1177_03080226241288157 for Factors affecting retention of occupational therapists in adult mental health service: A systematic review with narrative synthesis by Wenting Yan, Sally Ohlsen and Emily Wood in British Journal of Occupational Therapy
Footnotes
Acknowledgements
None.
Research ethics
Not applicable.
Consent statement
Not applicable.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EW and SO received funding from The Health Foundation (grant number 1275277).
Contributorship
WY, SO and EW designed the study and devised the search strategy. WY and SO conducted the screening. WY conducted the data extraction and analysis. WY wrote the first draft of the paper. All authors reviewed and edited the manuscript and approved the final version. EW is the guarantor.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.