
Abstract
Introduction:
Parents of individuals with autism face various difficulties, among which are decreased resilience and heightened stress. OT-Parentship is an intervention for parents of adolescents with autism that aims to promote parental resilience and enhance adolescents’ participation in daily life. This study examines OT-Parentship’s feasibility and explores the improvement of parental resilience and child and parent occupational performance following intervention.
Methods:
A mixed methods pre-post and follow up study. Fourteen parents (six mothers and four couples) of adolescents with autism participated in a series of 13 individual weekly sessions of 90 minutes each. Study results were analyzed before, after, and 3 months post intervention.
Results:
All parents completed treatment, with 100% adherence to sessions. Therapist’s treatment fidelity was estimated at 95–97% and parent homework completion was 85%. Preliminary efficacy findings show significant improvement in mothers’ and adolescents’ occupational performance and improvement in maternal resiliency.
Conclusion:
Research results support the feasibility of the OT-Parentship as a family centered, strength-based, intervention program that leads to improvements in adolescent participation and parental resilience.
Introduction
The transition to adolescence for individuals with autism spectrum disorders (ASD) with low support needs (level 1) is characterized by increasingly restricted participation in life roles, including self-care, major life areas, and social/community life (Pugliese et al., 2016). Limitations in activities include challenges in hygiene routines, peer, and sexual relationships (Cridland et al., 2014), meal preparation, room organization, class assignments (Rispoli et al., 2019), and sleep functions (Ismael et al., 2018). In addition, adolescents with autism with low support needs are more aware of their difficulties, experience social rejection, bullying, feelings of sadness, and anxiety (Fisher and Tailor, 2016).
Raising a child with autism can adversely affect the well-being of family members (Rutherford et al., 2019). Parents of children with autism with low support needs face notably elevated levels of parental stress compared to parents of typically developing children (Baker-Ericzen et al., 2005). Moreover, parents of adolescents with autism express a higher burden of caregiving responsibilities and a greater sense of concern for the achievement and well-being of their children in school environments and community in comparison to parents of younger children with autism and parents of adolescents with other developmental disorders (Lee et al., 2008). Moreover, as opposed to mothers of individuals with autism with substantial support needs, mothers of children with autism with low support needs are more likely to misattribute youth’s maladaptive behaviors to intentional, non-biological factors (Taylor and Seltzer, 2011).
Resilience is considered a central outcome of adaptive and integrated positive functioning among individuals coping with lifelong stress conditions (Southwick et al., 2014). Resilience in caregivers is described in various ways, all emphasizing the ability to overcome adversity. This not only involves managing the daily challenges of caring for a family member but also entails personal growth, increased strength, greater flexibility, and improved overall well-being (Van Breda, 2001). Additional references to parental resilience encompass indicators such as parental competence, diminished stress levels, acceptance, a sense of coherence, positive family dynamics, optimism, and enrichment. Resilient parents were found to better manage the adverse challenges of raising a child with autism (Bekhet et al., 2012).
Occupation-based coaching was found to be an effective intervention to increase parental efficacy and child participation among families of children with autism (Althoff et al., 2019). This coaching process is client-focused by addressing what holds the greatest significance, relevance, and responsiveness to client needs (Baldwin et al., 2013). Dunn et al., (2012), observed that parents of children with autism modified their perceptions, objectives, and interactions with their child. They enhanced their parental competence by applying coaching principles. Moreover, Kientz and Dunn (2012), showed that adolescents significantly increased their participation in everyday activities through a contextual intervention for parents and adolescents using coaching principles and focusing on the child’s sensory processing. Despite these positive findings, a systematic review of parent-focused interventions (Rutherford et al., 2019), highlighted the lack of data in this field and emphasized the need for further controlled investigation and development of manualized, well-defined interventions for parents of adolescents with autism, which include child and parent well-being outcome measures.
The OT-Parentship protocol (Wachspress et al., 2019) is a short-term, validated, occupational therapy (OT) intervention designed for parents of adolescents with autism with low support needs. As its name implies, it is designed to create a partnership between parent and therapist in aiming to promote parental resilience and enhance adolescents’ participation in daily life (for protocol details, Table 1). The protocol is grounded in models of occupational therapy, including the Person-Environment-Occupation Model (Law and Dunbar, 2007). The PEO model conceptualizes occupational health within an ecological framework, emphasizing the interrelations between the individual (e.g., biological and psychological factors) and their surroundings/environment. In addition, the model is client-centered emphasizing individual uniqueness, personal autonomy and client involvement in decision-making. Additional underpinning models are Occupational Performance Coaching (OPC; Graham and Rodger, 2010) and the Intentional Relationship Model (Taylor, 2008). The extensive validation process for OT-Parentship evaluated the framework, content, and clarity of the protocol making it suitable to the needs of parents of adolescents with autism (Wachspress et al., 2019).
OT-ParentShip protocol
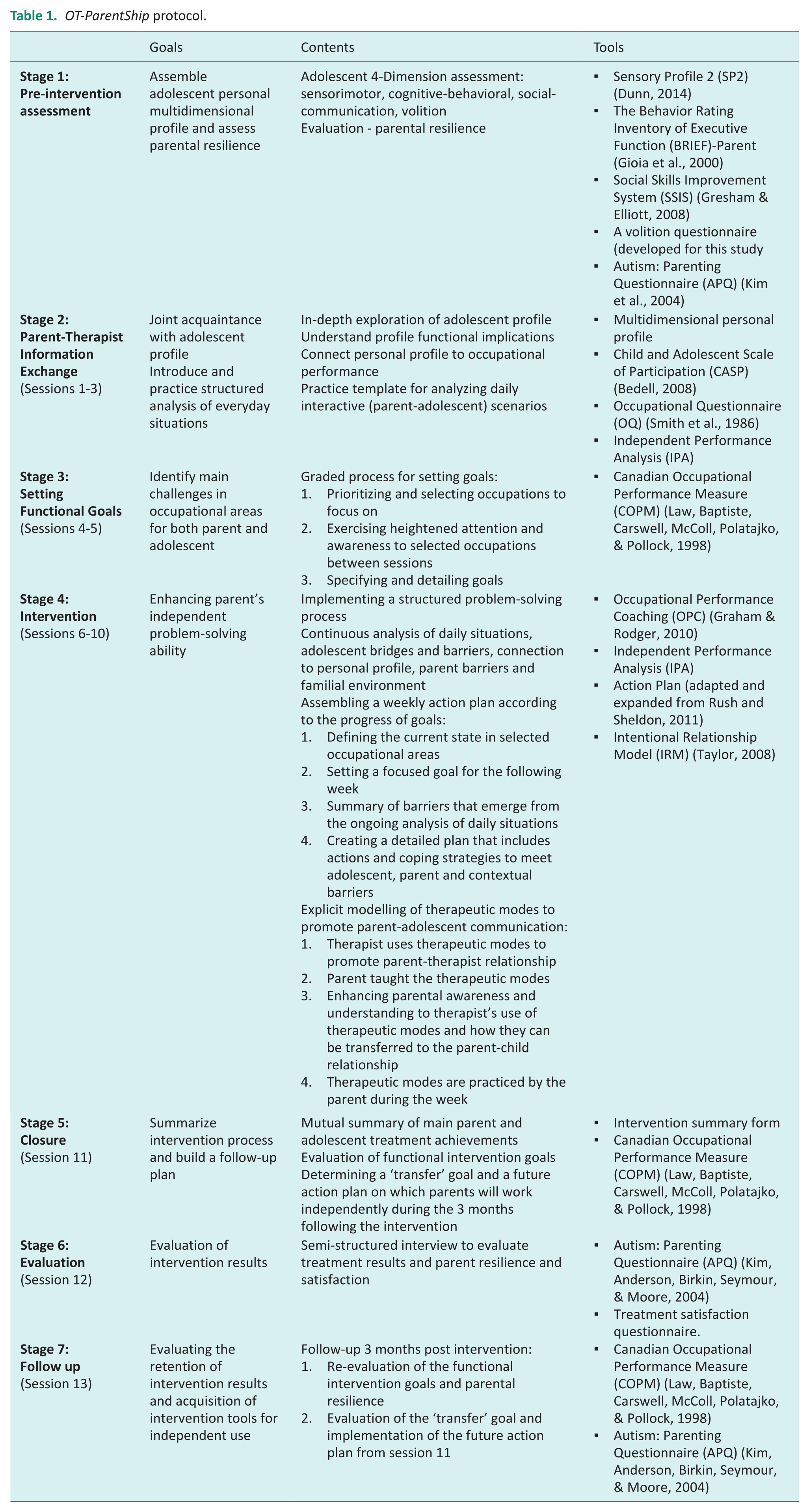
The primary goal of OT-Parentship is to lead parents into recognition and understanding of their adolescent’s sensorimotor, cognitive-behavioral, social-communicative, and motivational profile characteristics that impact their child’s daily functioning. The protocol accentuates functional outcomes resulting from the complex interactions between a person’s health condition(s) and that individual’s biological and contextual factors (environmental and personal factors). It operationalizes this goal through several stages. Parents (1) learn and become proficient with their adolescent’s personal profile; (2) analyze daily functional situations in regard to their adolescent’s unique profile; (3) identify enablers and barriers in themselves, the adolescent, contexts and task, and (4) build an action plan that addresses the identified barriers.
This article focuses on the quantitative aspect of the study which aims to (1) evaluate the feasibility of OT-Parentship to determine whether it is acceptable to parents and can be reliably delivered by trained therapists, and (2) examine the preliminary efficacy of the intervention to (a) enhance parental resilience; and (b) enable adolescent occupational performance (i.e. participation) in daily life. Establishing the feasibility of OT-Parentship is necessary to justify a large-scale randomized trial.
Methods
Study design
A mixed methods pre-post and follow up pilot study without a control group was conducted.
Participants
The study was approved by the Helsinki Committee of Hadassah Medical Organization (0269-17-HMO), 2019. ClinicalTrials.gov Identifier: NCT03361787. The participants were recruited using convenience sampling from community-based autism centers and social media. All participants signed an informed consent form at the beginning of the intervention. Ten families completed the intervention: 6 mothers and 4 couples (mother–father) of adolescents with autism (level 1; 5 boys, M = 14.32 years, SD = 1.98 and 5 girls, M = 13.95 years, SD = 1.06). Most families were at an average socioeconomic level, two families were above average and one family below. Six adolescents were treated with medication for ADHD, depression and/or anxiety (for detailed demographic data, Table 2). Inclusion criteria were: (a) parents (father, mother or both) of an adolescent (male or female) aged 12–18 years; (b) adolescent’s medical diagnosis (by a neurologist or psychiatrist) of ASD (Level 1) according to DSM-5 criteria. Eight of the ten adolescents were also diagnosed based on the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2002); (c) unmet daily functional needs/difficulties reported by parents; (d) commitment of the parent/both parents to attend all sessions for a period of approximately 6 months; and (e) receiving a score indicating adolescent impairment in one or more of the following areas: sensory processing (assessed by the Sensory Profile 2 (SP2)-Parent, Dunn, 2014)/executive function (The Behavior Rating Inventory of Executive Function (BRIEF)-Parent, Gioia et al., 2000)/social-communication skills (Social Skills Improvement System (SSIS)-parent, Gresham and Elliott, 2008). Exclusion criteria were untreated neurologic or psychiatric comorbidity, having a major effect on functioning, based on parental report.
Family demographic data (N = 14).
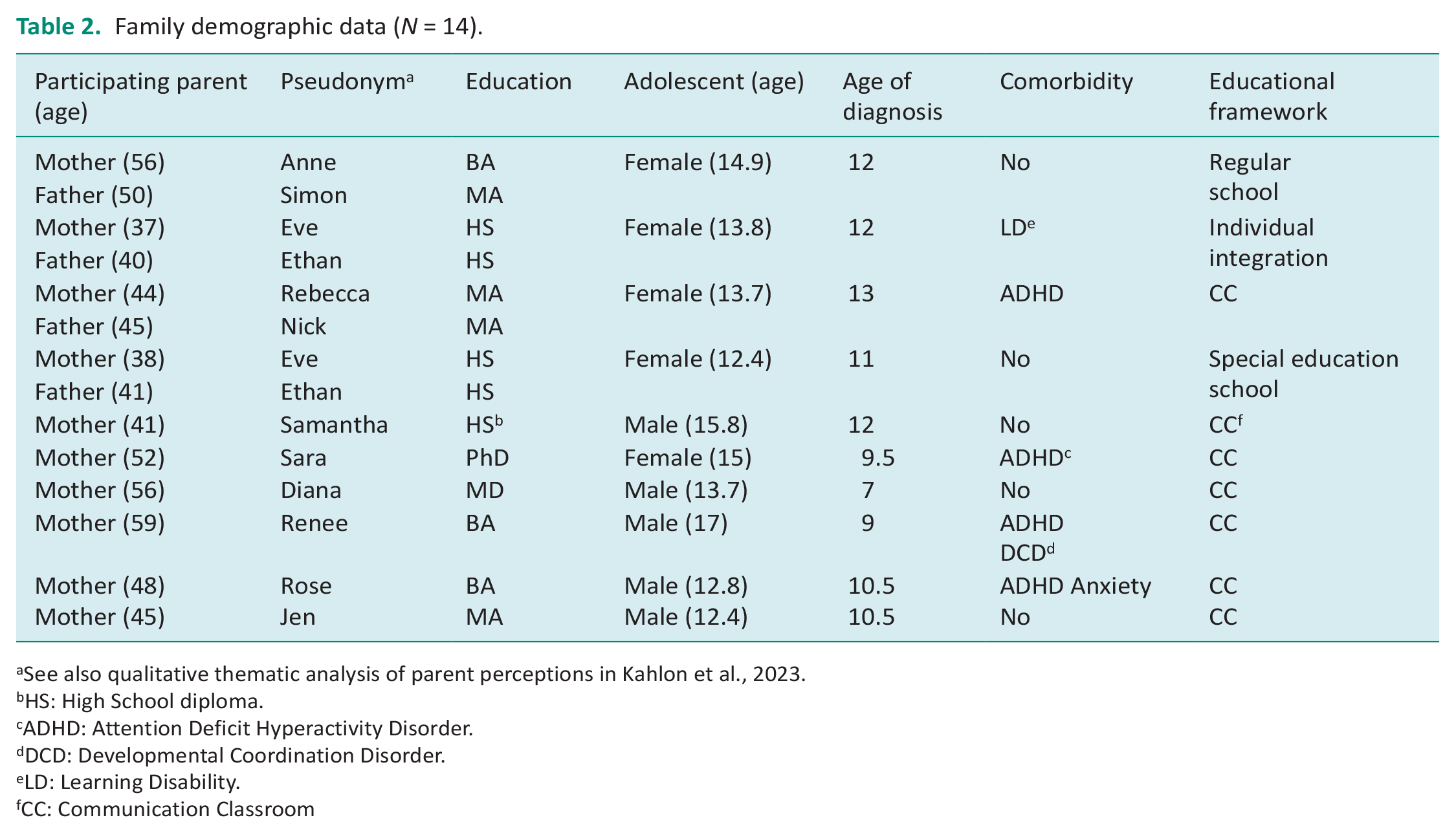
See also qualitative thematic analysis of parent perceptions in Kahlon et al., 2023.
HS: High School diploma.
ADHD: Attention Deficit Hyperactivity Disorder.
DCD: Developmental Coordination Disorder.
LD: Learning Disability.
CC: Communication Classroom
All the adolescents in the study had regulation difficulties as expressed in the following standardized measures. In the SSIS – eight (out of 10) adolescents received a low standard score (below 85, indicating difficulty) in social skills and nine received a high standard score (above 115, indicating difficulty) in behavior problems. The SSIS identified all ten adolescents with autism spectrum behavior level above average. In the BRIEF, nine adolescents received a total score above 65 indicating a significant clinical impairment in executive functions. One adolescent scored 64 – suspected impairment. Eight adolescents scored 2 SD from mean (indicating definite difference from the normative sample) at least on one of the four sensory quadrants of the SP2, and two scored between 1 and 2 SD from mean. Note: Dunn acknowledged the possible use of the SP2 up to 18 years. (Personal Communication, February 2017).
Measures
Demographic Questionnaire
Parent and adolescent demographic information (Table 2) as well as open-ended questions about the strengths and challenges of the adolescent and coping methods of the parent.
Feasibility outcome measures
Therapist treatment fidelity checklist
This checklist tracks therapist implementation of session goals for each of the 13 OT-Parentship sessions (11 therapy sessions, 1 interview session, 1 follow-up session). For each session, the therapist marked whether each segment of the session took place according to the protocol by marking yes/no. Treatment fidelity scores for each family are expressed in percentage by calculating the sum of the segments completed (marked as “yes”) divided by the total possible number of segments×100.
Fidelity checklist – Video data collection
We further validated the results of the fidelity checklist using video data collection. The last author analyzed 30% (similarly to Caldwell et al., 2018) of randomly selected (complete) sessions and marked whether each segment of the session took place according to the protocol by marking yes/no. Treatment fidelity scores for each family are expressed in percentage by calculating the sum of the segments completed (marked as “yes”) divided by the total possible number of segments × 100.
Recruitment, retention, and adherence
Information regarding the number of eligible participants, recruitment procedure and retention were documented in therapist logs. Parent adherence was measured by the number of sessions attended (13, 90 min. sessions, altogether).
Parent homework completion
Homework completion assessed parent implementation of assignments. We defined homework completion as none, partial or full implementation of the weekly action plan. A partial implementation meant that parents actively initiated the plan and were motivated to fulfill it, but that it was objectively impossible to implement (due to change of circumstances/context, and/or understanding that parts of the plan were irrelevant to the situation or the parent). For each family, we calculated a raw score for the number of full implemented action plans from the total number planned. The raw score was converted to percentage to enable comparisons across families.
A qualitative semi-structured interview
Assesses parental experience and satisfaction from the intervention. Contains eight open-ended questions relating to positive and negative aspects, as well as program compliance with parent expectations, changes in parental behavior and competence following their engagement in the intervention process.
Efficacy outcome measures
Autism: Parenting Questionnaire
A 25 item, self-completed questionnaire targeting six domains of autism-specific parenting competence (knowledge, communication, play, behavior management, confidence and family functioning) and one domain of parenting stress. Collectively, these domains serve as measures of parental resilience in the current study (according to the resilience indicators mentioned above; Kim et al., 2004). The APQ was developed to assess the effectiveness of an early intervention program for parents of children with ASD. However, the normative data were gathered from parents whose children spanned an age range of 2–47 years, with a mean age of 10.7 years. A correlational analysis of the normative sample showed no relationship between the age of the child and the total score. Therefore, the questionnaire can potentially be used as a general measure of parenting skills in parents of children with autism regardless of the age of the child. A higher score indicates higher parental perception of parental competence (min. 25, max.150). Internal reliability: the coefficients for subscales ranged from 0.67 to 0.82 and the coefficient for the Total Score was 0.87.
Canadian occupational performance measure
A semi-structured interview, used as an outcome measure to detect changes in self-perception of patient performance and satisfaction over time by identifying problems with daily functioning (Law et al., 1998). During the interview, the patient identifies functional difficulties in three occupation areas (self-care, productivity and leisure) and ranks them according to their level of importance. Rating is on a 10-point Likert scale (1 = low importance and 10 = high importance). An improvement of two points from one time point to the second, is a significant statistical improvement. In the current study, parents define their own level of performance as well as that of their adolescent, in 2–3 goals.
Procedure
The intervention program was delivered over 11 weeks, an assessment session at week 12 and a follow-up session 3 months post intervention. The intervention was delivered by one of two occupational therapists – the first author and a certified OT who was also a graduate student at the time. The outcome measures were evaluated by a researcher who did not conduct the intervention, the last author. Study results were evaluated for each parent separately at three time points – before intervention (Time 1), immediately post intervention (week 12–Time 2) and 3 months post intervention (week 24–Time 3). The transfer goal was evaluated on week 12 and week 24. Time 1 included an assessment of the adolescent profile as well as an initial assessment of parental perception of competence. Thereafter, each parent (or couple) participated (without the presence of the adolescent) in a series of 11 individual, in-person, weekly sessions of 90 minutes each, an assessment session at week 12 (Time 2) and a follow up session at week 24 (Time 3). With the consent of the participants, the intervention sessions of 9 out of 10 families were fully videotaped. In the first three sessions, mutual recognition and learning (parent-therapist) of the adolescent’s multidimensional personal profile, and its implications on his or her participation in daily life through everyday situation analysis, were conducted. During the fourth and fifth sessions (while incorporating the Canadian Occupational Performance Measure (COPM)), parents identified two or three main challenges in one or more occupational areas, based on issues that emerged in these first sessions. Each challenge (e.g., online communication) consisted of two goals – one for the adolescent (e.g., the adolescent will initiate and respond to mobile phone messages daily) and one for the parent (e.g., the parent will coordinate regular times for sending and responding to messages with the adolescent and will maintain consistency in implementing the action plans). From the sixth session onwards, the parents and the therapist focused on enhancing parent’s independent problem-solving ability. This was achieved through continuous analysis of daily situations (independently by the parents during the week as well as jointly with the therapist during sessions), of adolescent barriers and their connection to his or her personal profile, and of parent barriers regarding their familial environment. Each session was concluded with a weekly action plan. At the end of the 11th session, an additional goal (“transfer goal”) was set by the parents for both parent and adolescent. This goal examines whether parents acquired the ability to independently implement the tools and strategies learned in the intervention.
Data analysis
Descriptive statistics using sums, means and percentages were used to assess treatment fidelity, recruitment, retention, adherence, and homework completion. Due to the small sample size, non-parametric statistics were used. Outcome measures were described using Wilcoxon signed rank tests to analyze change over time (pre-post; post-follow up; pre-follow up) and Spearman rank correlation coefficients to calculate correlations between differences (Δ) in adolescent performance, mother performance, and mother competence. Change scores were calculated between time1–2, 2–3, and 1–3 in order to examine associations between changes in mother/adolescent performance; and associations of changes in performance with mother resilience. The significance level was set at p ⩽ 0.05. We also reported effect sizes (EF) for non-parametric tests using r = z/√n (a large effect is r ⩾ 0.5, a medium effect is r = 0.3, and a small effect is r ⩽ 0.1; Fritz et al., 2012).
Results
Feasibility outcomes
Therapist treatment fidelity checklist
The maximum number of possible segments for all sessions was 40. Raw scores ranged from 37 (93%) to 40 (100%). Mean score for all families was 39 (97%).
Fidelity checklist – Video data collection
A total of 117 (9 families × 13 sessions) sessions were recorded (one family did not agree to recordings). Thirty-five sessions (30% of total sessions recorded) were analyzed. Results yielded a mean raw score of 38/40 (95%) implemented segments.
Recruitment, retention, and adherence
Study recruitment took place in two phases: between December 2017 and February 2018, and between November and December 2018. Twenty-two, self-referred, parents contacted the study coordinator, of which 20 were identified as eligible according to inclusion criteria. Since this study limited the number of participants, 10 families were recruited to the intervention (first-served basis). Retention rate was 100% – all 10 families completed the intervention and follow-up. Full adherence (100%) to all 13 sessions of the protocol were documented for all families. It should be noted that on occasion that parents were unable to attend (possible reasons were: holiday, medical issues, family commitments) the session was rescheduled to the earliest possible date. The mean time for the intervention without follow-up (12 sessions) was 16.5 weeks (median. 15.7; min. 12; max. 22).
Parent homework completion
The mean for total number of action plans was 6.6 (range: 4–9), out of which a mean of 5.6 (range: 3–7) action plans were implemented. The mean full implemented action plans for all families was 85%. Reasons for partial implementation: Time limitations, an unexpected familial situation, non-relevance of the plan to actual home context, or plan not specific enough.
A qualitative semi structured interview
All parents (N = 14, 100%) participating in the pilot study were highly or very highly satisfied with the intervention. All parents (100%) stated they would recommend the intervention to others, and 90% wanted to continue with the intervention process. A qualitative account of the thematic analysis of parental experience and satisfaction from the intervention is detailed in Kahlon et al. (2023).
Efficacy outcomes
The goals set by the parents represent a wide array of occupational domains that challenge families of adolescents with autism with low support needs (e.g., morning routines, meal preparation, sports activity, showering, and initiating social interactions). Given the disparity in the number of participating mothers (10) and fathers (4) in the study, the descriptive data of all participants’ results are presented in Table 3. However, only mothers’ data were included in the statistics analysis.
Mother and father COPM and APQ mean scores.
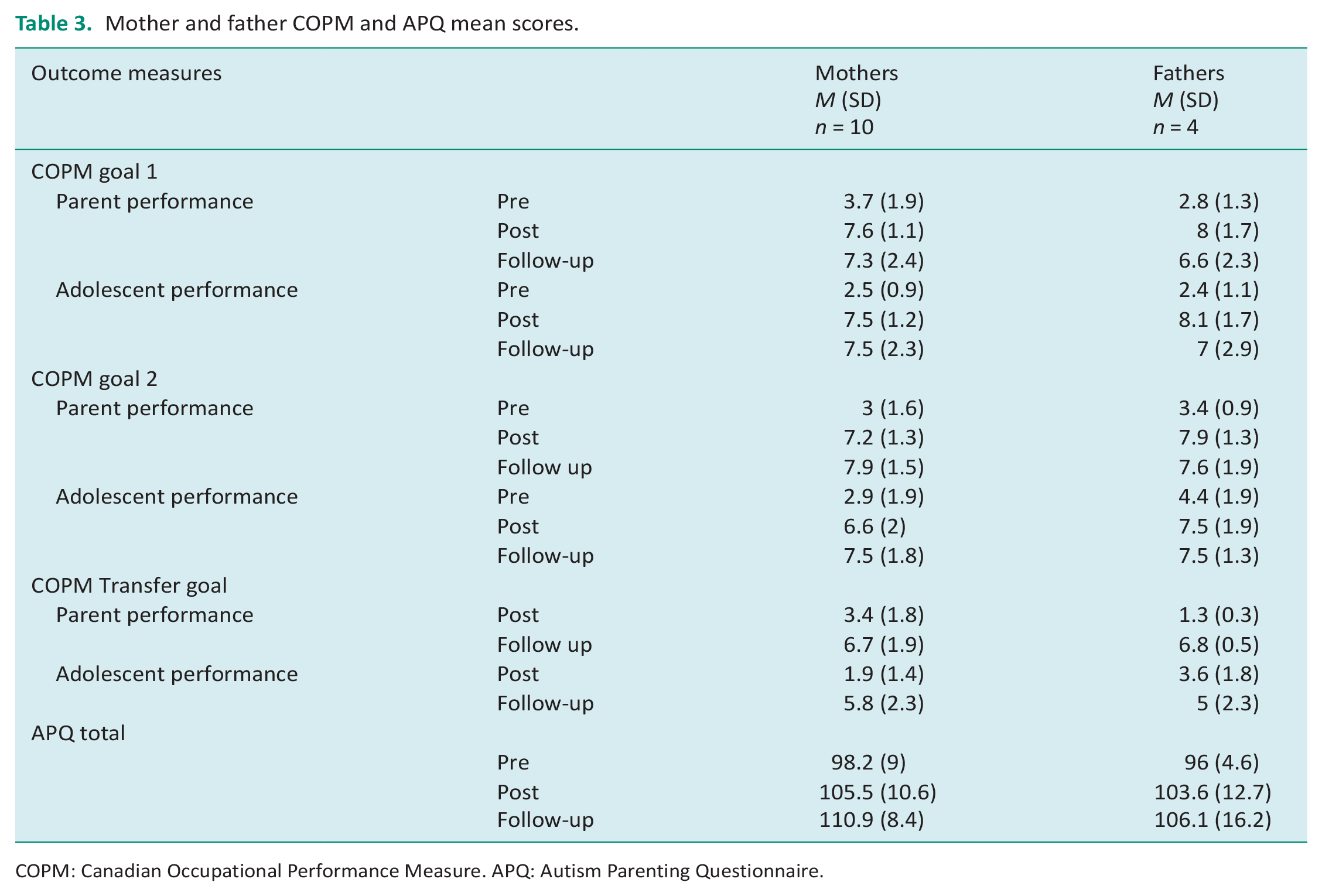
COPM: Canadian Occupational Performance Measure. APQ: Autism Parenting Questionnaire.
A significant improvement was found in COPM performance score from time 1 to time 2 for mother-related goals (Time 1: M = 3.19, SD = 1.18; Time 2: M = 7.38, SD = 0.7; Z = 2.81, p = 0.005) and adolescent-related goals (Time 1: M = 2.67, SD = 0.78; Time 2: M = 7.11, SD = 1.37; Z = 2.8, p = 0.005). Furthermore, results were maintained at time 3 as was established in the non-significant change for mothers (M = 7.63, SD = 1.2; Z = .88, p = NS) and adolescents (M = 7.49, SD = 1.17; Z = 0.72, p = NS). A medium positive correlation (non-significant) was found between change scores (Δ) of adolescent COPM performance and mother performance scores from time 1 to time 3 (rs = 0.512, p = 0.065).
The COPM performance score for the transfer goal also showed significant improvement from Time 2 to Time 3 for mothers (Time 2: M = 3.35, SD = 1.7; Time 3: M = 6.7, SD=1.2; Z = 2.67, p = .008) and adolescents (Time 2: M = 1.85, SD = 1.2; Time 3: M = 5.8, SD = 2.1; Z = 2.81, p = 0.005). Furthermore, a high significant positive correlation was found between change scores of adolescent COPM performance and mother performance scores from time 2 to time 3 for the transfer goal (rs = .63, p = .026).
APQ total scores showed an improvement trend (not significant) from time 1 (M = 98.2, SD = 8.9) to time 2 (M = 105.5, SD = 10.6; Z = 1.582, p = 0.114), a significant improvement from time 2 to time 3 (M = 110.9, SD = 8.4; Z = 2.143, p = .032) and from time 1 to time 3 (Z = 2.807, p = .005), all with large effect sizes (r = 0.50, 0.68, 0.89, respectively).
No correlation was found between change scores of the COPM mother performance and APQ total scores from time 1 to time 2 (rs = −0.018, p = 0.96) and from time 2 to time 3 (rs = −0.26, p = 0.468). However, there was a medium positive correlation (non-significant) between change scores of adolescent COPM performance and mother APQ total scores from time 1 to time 2 (rs = 0.491, p = 0.115) and from time 2 to time 3 (rs = 0.382, p = 0.276).
Discussion and implications
Results from this pilot study support the feasibility of OT-Parentship and its preliminary efficacy as a strength-based intervention for parents of adolescents with autism with low support needs. The intervention was acceptable to parents as evidenced by several factors: The target population was easily identified and recruited in two phases, with full (100%) retention and adherence to protocol sessions and a satisfactory rate (85%) of homework completion. All parents expressed their satisfaction with the intervention and 90% wanted to continue at its termination. Therapists delivered the protocol in a consistent fashion as evidenced by 95% fidelity on a random sample of sessions viewed by a trained/independent reviewer, and 97% fidelity on the implementation of protocol segments. The development of OT-Parentship and the process of evaluating its implementation is based on the recommendations of Persch and Page (2013) on how to maximize treatment fidelity, adherence to treatment and quality control. In short, findings from this pilot study suggest that OT-Parentship can be delivered reliably by therapists to parents with high rates of engagement and satisfaction.
Full retention and adherence to the protocol sessions was possible, in our opinion, due to OT-Parentship’s inherent flexibility and family-orientation. Factors such as flexibility in rescheduling sessions when needed, or the fact that each session was attuned to the specific needs and contexts of the family are important aspects, both technical and fundamental, lending to these high rates. Another important factor is the 90-min. units for each session. Both therapists and parents agreed that this longer-than-usual (45–50 min.) time frame allowed for a calmer and more relaxed atmosphere, which in turn allowed for in-depth sharing and processing of parents’ needs. A possible limitation of this flexibility in session scheduling was apparent in two occurrences in which there was more than a 2-week gap between sessions. In these cases, parents seem to be less compliant with the implementation of weekly action plans, perhaps influencing the moderate rates of homework completion observed.
Results demonstrated improvements with notable clinical significance (as portrayed by medium-large effect sizes) in occupational goal attainment and maternal resilience. Regarding occupational goals, significant improvements were found from beginning (time 1) to end of the intervention (time 2) for the mother’s own goals as well as the goals she set for her adolescent. Furthermore, the follow-up assessment results provide a window into generalizability of effects. It appears that therapeutic gains continued after completion of treatment as shown by improvements in transfer occupational goals, that were not specifically targeted in therapy, further improvements in resilience, and maintenance of occupational gains achieved that were targeted during treatment.
The high significant positive correlation found between change scores of adolescent COPM performance and mother performance scores from time 2 to time 3 for the transfer goal indicates that, in the transfer goal, on which the parents worked independently after the intervention ended, the degree of change in mother’s performance was related to the degree of change in adolescent functioning. These findings highlight the potential benefit of OT-Parentship beyond the immediate treatment setting, suggesting that parents acquired coping strategies that may continue to promote participation of their children and resiliency in themselves. These findings may meet the need arising from the research results of Reid et al (2019) for treatment that addresses directly the personal needs of the parent as well as their needs as parents of a child with autism. In OT-Parentship, a unique implementation of the Intentional Relationship Model (IRM; Taylor, 2008) is incorporated: The model is used as a platform for an ongoing analysis of the barriers and needs of the parent. Based on parental insights acquired through the study and practice of the model, it is consequently applied as a tool by the parent to better understand and interact with their adolescent.
Resilience serves as a protective factor, mitigating the impact of stressors on families of children with ASD (Halstead et al. 2018). Bekhet et al. (2012) identified that parents’ positive beliefs about their own resourcefulness can serve as a protective factor in managing the demands of a child with ASD (i.e., caregiver burden). An individual’s interpretation of a stressful event(s) can play a pivotal role in resilience and effective coping strategies (Ruiz-Robledillo et al., 2017). Similarly, in the current study, the increase in maternal competence from baseline to the end of intervention and follow-up may be indicative of resilient coping, the ability to cope with adverse situations in an adaptive manner. Although we found a definite trend of increased competence from Time 1 to Time 2 it was not statistically significant.
In the current study, the degree of change in parental resilience (mother) was found to be non-significantly associated with the degree of change that occurred in adolescent performance, from the beginning of the intervention to its end, and 3 months thereafter. This result, although non-significant, is important in that it echoes Iida et al. (2018) namely, that the more mothers are able to analyze and cope with their child’s behavior, the more they improve their stress coping style (an indicator of resilience Bekhet et al. (2012)) allowing for a subsequent change in the child’s behavior.
This study highlights several active ingredients which constitute the change mechanisms of OT-Parentship: (1) the adolescent profile is the end product of a thorough, multi-dimensional, scrutiny of his/her abilities and deficits. The parent learns the unique, multidimensional profile of his adolescent, and acquires the ability to identify, based on the profile, the fundamental components underlying daily challenges. Only after this basic stage is established, the therapist and parent set goals for promoting parent and adolescent functioning; (2) analysis of debilitating personal and environmental (social and physical) barriers, of both the adolescent and the parent, may improve coherence and manageability of daily life problems. The protocol couples parent and adolescent goals in a unique form – parents are encouraged to set goals that amplify their specific role in advancing the adolescent goal; (3) the therapeutic relationship and communication were enhanced by continuously using the IRM model to respond to parent’s needs during the session. These three active ingredients are consistent with the recommendations of Schoen et al. (2021) for parental involvement in the assessment process, which should include a parent–therapist discussion regarding areas of concern in daily life. This process strives for a better understanding of the relationships between body functions and occupational performance in order to promote family-centered care and for determining meaningful intervention goals; (4) In the qualitative analysis of this study (Kahlon et al., 2023), Self Determination Theory (SDT; Ryan and Deci, 2017) was found to be an adequate theoretical framework that can help in understanding treatment outcomes. Overall, it appears that OT-Parentship directly enforces parents’ three basic psychological needs, who, in turn, were able to support these basic needs for autonomy, relatedness, and competence in their adolescent with autism.
This research used a small, convenience sample of parents, limiting its external validity. Participating parents were families that answered advertisements in community-based autism centers and social media. As such, they were probably highly motivated to participate. The OT-Parentship protocol requires commitment and availability (albeit short term) on the part of parents, and therefore may not be suitable for all parents of adolescents with autism. These pilot findings should be examined in the future in a broader, randomized and controlled study, possibly enabling a more balanced perspective of both mothers and fathers.
Conclusion
OT-Parentship intervention led to a significant improvement in adolescents’ participation and the performance of parents in promoting this participation. The intervention outcomes indicate a potential for increasing parental resilience. Results support its feasibility as a strength-based family centered OT intervention program that provides parents of adolescents with autism with low support needs with a deep understanding of their adolescent’s unique profile, an opportunity to analyze everyday situations, and promotes them in acquiring practical tools and strategies for coping with everyday functional challenges. This is a thorough, well-defined, manualized intervention that adds data to the wanting field of parent-focused interventions (Rutherford et al., 2019).
Key findings
OT-Parentship facilitates direct and structured engagement with parents, aiming to enhance the participation of adolescents with autism.
OT-Parentship emphasizes a collaborative process between parents and occupational therapists promoting parental resilience.
What this study adds
OT-Parentship is a feasible intervention that provides a practical approach for parents of adolescents with autism, addressing both their and their adolescent’s occupational performance while enhancing parental resilience. Nonetheless, further research is needed for stronger evidence.
Footnotes
Acknowledgements
The authors would like to extend their gratitude to Einav Kahlon for her assistance in data collection.
Correction (February 2025):
Article updated to correct Table 1. See DOI: 10.1177/03080226251318928.
Research ethics
The third and last author designed and supervised the study. The first author completed the data collection. The second author supervised the ethics application process and served as medical advisor. The first and last author drafted the manuscript and all authors critically reviewed and approved the final version.
Consent
The study was approved by the Helsinki Committee of Hadassah Medical Organization (0269-17-HMO), 2019. ClinicalTrials.gov Identifier: NCT03361787. All participants signed an informed consent form.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by a student research grant from the Hebrew University Autism Center.
Contributorship
The third and last authors designed and supervised the study. The first author completed the data collection. The first and last authors conducted the quantitative data analysis. The second author supervised the ethics application process and served as medical advisor. The first and last authors drafted the manuscript, and all authors critically reviewed and approved the final version.