
Abstract
Introduction:
Occupational therapists and physiotherapists routinely assess Hand grip Strength (HGS) to evaluate hand function. This study explored the experiences of clinicians who regularly assess and evaluate HGS including the testing protocol utilised, evaluation methods and the influence of various biological and functional factors.
Method:
This exploratory survey (n = 49) was distributed online to members of the Australian Hand Therapy Association. The questionnaire asked recipients to identify HGS testing protocols, evaluation methods, use of normative data, reasons for assessment and the influence of biological and functional factors on HGS. Demographic data was also collected.
Results:
Sixty-four percent of respondents were occupational therapists and 59% had over 10 years’ experience assessing HGS. The standardised American Society of Hand Therapists (ASHT) testing protocol was consistently adopted by only 67% of respondents . Variations in contraction time, scoring and evaluation methods were identified. Gender, age, employment and lifestyle were considered the functional and biological factors which influence HGS.
Conclusion:
This study details how and why occupational therapists and physiotherapists in Australia assess and evaluate HGS. Use of the ASHT testing protocol is not universal. Clinicians rely on the reason for assessment, clinical experience and practice context to determine how they assess and evaluate HGS.
Introduction
Hand Grip strength (HGS) is a simple and objective measure which provides a quantifiable evaluation of hand and upper limb function (Bhat et al., 2021; Günther et al., 2008; Larson and Ye, 2017). Hand function is required to participate in everyday life to complete self-care, work and leisure activities. Due to its versatile application, HGS testing is used across a wide variety of practice settings by a range of health professionals including occupational therapists and physiotherapists (Reuter et al., 2011).
HGS can be utilised to assess work capacity, to measure outcomes following trauma or surgery and as a baseline measure to track rehabilitation progression (Matheson et al., 2002; Reuter et al., 2011). The testing protocol used to assess HGS can influence the scores obtained and subsequently how a clinician interprets an individual’s hand strength and upper limb function (Innes, 1999; Richards et al., 1996). The adoption of a standardised HGS testing protocol developed by the American Society of Hand Therapists (ASHT) in 1981 was thought to allow for improved reliability when monitoring rehabilitation progress in a quantifiable manner (Fess and Moran, 1981).
HGS is also used to compare an individual’s ability in relation to normative data from the general population (Bohannon et al., 2006; Larson and Ye, 2017). To allow accurate comparison to normative data, the HGS testing protocol must be consistent with the testing protocol used to develop the normative data (Innes, 1999). A study by Myles et al. (2022) found both HGS assessment and evaluation can vary according to clinical experience and practice context and requires other factors to be considered in combination with the standardised testing protocol.
The influence of biological (age, gender, anthropometric characteristics) and functional (hand dominance, occupation, lifestyle) factors on HGS has been explored across various populations (Bhat et al., 2021; Eidson et al., 2017; Nicolay and Walker, 2005; Rostamzadeh et al., 2019; Saremi and Rostamzadeh, 2019). Age and gender have been identified as the strongest factors to influence HGS with men being stronger than women and HGS increasing from early adulthood into the third decade before declining with age (Abe et al., 2016; Agnew and Maas, 1982; Dodds et al., 2014; Günther et al., 2008; Mathiowetz et al., 1985). Conjecture remains regarding the significance of the influence of other biological and functional factors such as work and lifestyle (Günther et al., 2008; Lo et al., 2020; Mohammadian et al., 2015; Rostamzadeh et al., 2020). However, given the significance placed on HGS as an evaluation of overall upper limb function, consideration of the influence of biological and functional factors provides increased context and confidence when interpreting HGS scores. Few studies have examined how and why clinicians assess and evaluate HGS. This study expanded on previous qualitative research to include physiotherapists along with occupational therapists working within Australia (Myles et al., 2022). The aim of this study was to explore how and why occupational therapists and physiotherapists assess and evaluate HGS. A further aim was to determine the factors that influence HGS based on their clinical experience.
Method
Design
An exploratory cross-sectional study design utilising an online questionnaire containing pre-determined quantitative questions along with select open-ended questions was employed for this study which sought to describe how and why Australian hand therapists assess and evaluate HGS. The online questionnaire was created using the interview guide of a previous focus group study (Supplemental Appendix 1; Myles et al., 2022). Ethical approval (number) was granted by (anonymous) in August 2022. This research built on a previous study examining the experiences of occupational therapists within Queensland, Australia to include both occupational therapists and physiotherapists Australia-wide with the hope of allowing for improved transferability of the findings to clinicians who evaluate HGS more broadly (Myles et al., 2022).
Participants
Participants were recruited using purposive sampling methods through the Australian Hand Therapy Association (AHTA). The inclusion criteria were Australian Health Practitioner Regulation Agency (AHPRA) registered occupational therapists and physiotherapists, who are members of the AHTA who assess and evaluate HGS as a standard part of their clinical practice in Australia. The exclusion criteria were any health professionals other than occupational therapists and physiotherapists who are not members of the AHTA and who do not assess HGS. The primary researcher sought prior approval for the research questionnaire from the AHTA which included a formal application to the research committee consisting of a copy of the ethics approval, a participant information sheet and the questionnaire questions including a link to the online questionnaire. An email inviting members of the AHTA to complete the questionnaire, including the questionnaire link was distributed via the AHTA’s email distribution list. The questionnaire was available from October 2022 to November 2022. A reminder alert was sent via the AHTA newsletter 2 weeks before the questionnaire closed.
Data collection
An online purpose-designed questionnaire was developed using Qualtrics to gather data to answer the research questions of “How and why do Australian occupational therapists and physiotherapists assess and evaluate HGS?” and “What are the factors that influence Australian HGS” (Qualtrics (https://www.qualtrics.com)). The questionnaire was anonymous, and participants were provided with an information sheet regarding the study before providing informed consent selecting ‘yes’ to participate as the first survey question. Demographic questions were formulated to describe the participants, their professional field (occupational therapy or physiotherapy), level of expertise working with HGS and geographical work location. The questionnaire grouped years of professional experience working with HGS into specific descriptors of year ranges and utilised the Australian Geography Standard descriptors to classify geographical work location (Australian Bureau of Statistics, 2021). Additionally, descriptions regarding HGS testing protocols and how HGS scores are interpreted and evaluated were collected using multiple choice questions which allowed respondents to select all that apply. The multiple choice questions and responses and the short answer questions were developed using an earlier study which explored the experiences of occupational therapists within Queensland, Australia who assess adult HGS (Myles et al., 2022). These questions were designed to allow participants to elaborate on the reasons they assess HGS and how they evaluate HGS. A ranking question was utilised to obtain the participants’ opinions regarding what biological and functional factors they believe influence HGS. The final survey included 13 questions excluding consent: five demographic questions, six multiple choice questions, one short response question and one ranking question.
Data analysis
SPSS 27 (IBM Corporation, New York, NY, USA) was used for statistical analysis of the data. Descriptive statistical analysis was utilised to explore demographic data of the participants including educational background (occupational therapy or physiotherapy), years of experience working with HGS, educational level and geographical location. Only questionnaires which had responded to all multiple choice, short answer and 90% demographic questions were considered adequate and included within the data analysis.
Findings
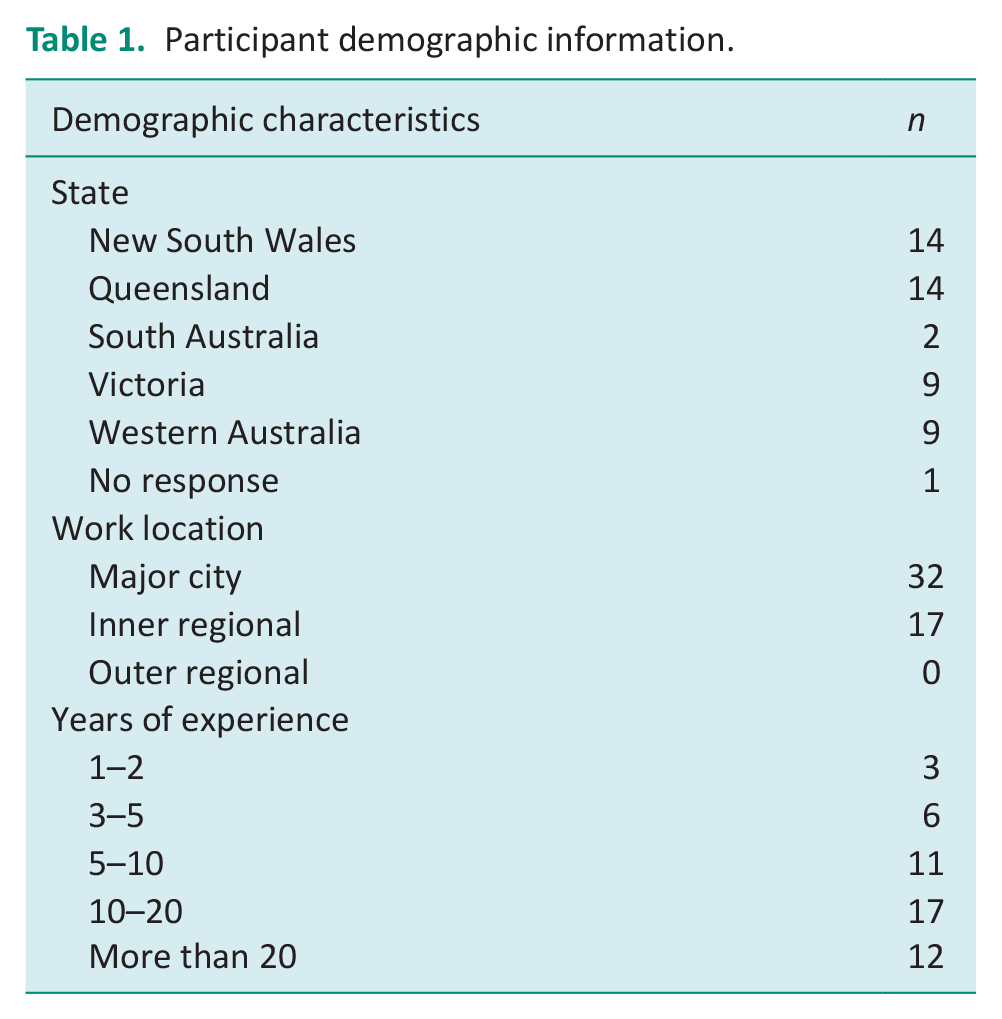
Forty-nine complete questionnaires were included within this study. An additional two questionnaires were found to not meet the completion requirements as limited data was recorded in these attempts and were subsequently not included in the study. Demographic data detailing professional field, education level, level of experience working with HGS and geographical location are presented in Table 1. Of the 49 respondents, 32 (65%) were from a major city with the remaining respondents practicing in inner regional locations across Queensland, New South Wales, Victoria, South Australia and Western Australia. Respondents identified as being highly experienced working with HGS with 29 respondents (59%) having more than 10 years’ experience assessing HGS while 40 respondents (82%) had more than 5 years’ experience.
Participant demographic information.
Data collected regarding the HGS testing identified variations in the adoption of the ASHT standardised protocol. The ASHT standardised testing position and instructions involves having the participants seated in an upright posture with both their hips and knees in 90° flexion with feet flat on the floor; testing arm at the side, not touching the body; elbow flexed at 90°, forearm in neutral, wrist slightly extended between 0° and 30° and ulnar deviation between 0° and 15°; with the non-testing arm relaxed at the side (MacDermid et al., 2015). Thirty-three respondents indicated that they follow the complete ASHT testing protocol when assessing HGS, of which 71% were occupational therapists and 61% physiotherapists. Of the respondents who identified as a qualified or qualifying Accredited Hand Therapist, 68% utilised the ASHT testing protocol. Forty-six (94%) respondents indicated they complete testing in a seated position using the second handle position. Thirty-seven respondents indicated they alternate trials between hands. Fifty percent of respondents indicated they record the mean of the three trials for each hand with the remaining 50% of respondents recording the maximum HGS score. The HGS score was determined using a short maximal contraction by 50% of clinicians with the remaining respondents utilising a sustained duration contraction.
Seventy-six percent of respondents who have more than 10 years’ experience evaluating HGS stated they utilise the ASHT testing protocol with 52% of these same respondents also indicating the use of normative data to interpret HGS scores. By contrast, only 55% of clinicians with less than 10 years’ experience stated they utilise the ASHT testing protocol during HGS assessment and 45% of these less experienced clinicians refer to normative data to evaluate HGS.
The most frequent reasons for assessing HGS were ranked in the following order: to evaluate rehabilitation progression (baseline assessment) (98%), to work towards a client’s goal (96%), for return to work and following injury/surgery (96%).
When evaluating HGS scores, 49% of respondents indicated that they utilise normative data for comparison, with the normative data set by Mathiowetz et al. (1985) as the most commonly referenced. Other means of evaluating HGS scores identified included comparing affected to unaffected or right to left sides (96%) and recording progression over time (96%). Qualification as an accredited hand therapist did not impact the use of normative data with approximately 50% of accredited (or in the process of becoming accredited) and non-accredited clinicians reporting the use of normative data to evaluate HGS scores.
The most influential biological factors identified in rank order by the respondents were: gender (19 respondents), age (13 respondents), hand dominance (three respondents), forearm circumference (one respondent), height and hand length. The most influential functional factors which influence HGS were ranked as employment (seven respondents) and then lifestyle (three respondents).
Discussion
The current study aimed to build on an earlier qualitative study which explored the experiences of occupational therapists within Queensland, Australia who evaluate adult HGS (Myles et al., 2022). The current study was expanded to explore how and why occupational therapists and physiotherapists who are members of the AHTA working within Australia assess and evaluate HGS. Members of the AHTA were included in the study as HGS testing is an inherent requirement of their job role within their practice context as hand therapists. The specific research questions of “how and why do occupational therapists and physiotherapists who are members of the AHTA working within Australia assess and evaluate HGS” and “what factors influence HGS” based on their clinical experience. These topics were explored using questions around the reasons why HGS is assessed, the HGS testing protocol utilised, how HGS scores are interpreted and evaluated along with the influence of biological and functional factors on HGS.
HGS testing protocol
Commonalities and variances were identified in the HGS testing protocol developed by MacDermid et al. (2015) and used as standardised by the ASHT. Variations to the testing protocol were outlined by the respondents. Seventy-one percent of occupational therapists and 61% of physiotherapists confirmed the use of the complete ASHT testing protocol when assessing HGS. The majority of respondents (94%) had the client complete the test in a seated position and used the second handle position of the dynamometer when performing HGS testing. Research states that the use of a standardised testing protocol results in improved test-re-test reliability (Lagerström and Nordgren, 1996). Additionally, variations from the standardised testing position can impact HGS scores (Innes, 1999; Richards et al., 1996). Roberts et al. (2011) found that considerable variation in equipment and methods used for assessing HGS can in turn impact the scores recorded. Without consistent testing protocols, small changes in body position can result in altered HGS scores (Richards et al., 1996). Myles et al. (2022) suggested educational training, clinical experience and prior experience with HGS inform the HGS testing protocol utilised. The current study found clinicians with more than 10 years’ experience more commonly used the ASHT testing protocol for HGS assessment and referred to normative data for evaluation of HGS scores. The standardised ASHT testing protocol in 1981 was developed to provide uniformity and consistent guidelines and language between health professionals (Fess and Moran, 1981). The results of this study suggest clinicians with more experience find the improved test re-test reliability of using the ASHT testing protocol along with the ability to interpret the HGS score in comparison to normative data of great benefit. The assessment and evaluation of HGS is determined by complex factors including clinical training and professional experience and the development of a standardised testing protocol has not resulted in a universal testing procedure. The study by Woods and Lilly (2018) found that certified hand therapists who indicated use of the complete ASHT testing protocol were all occupational therapists, who were highly experienced with over 21 years’ experience assessing HGS. It could be suggested that clinicians who have completed undergraduate training at different points in time may have received different instructions as to how to assess and evaluate HGS.
The most common variations to the testing protocol related to the type of contraction performed during the assessment and the score recorded. Fifty percent of respondents indicated that they ask the client to sustain the duration of the contraction instead of performing a short maximal contraction. This variation in testing protocol could significantly influence the scores obtained during the assessment as a sustained versus short maximal contraction may cause increased fatigue when performing three trials on each hand. Previous research found good reliability for momentary strength after 1 second, after 4 seconds and after 5 seconds, but not in the 10-second test (Kamimura and Ikuta, 2001). Therefore it is reasonable to question the suitability and purpose of performing a sustained maximal contraction particularly as sustained maximal contractions also increases blood pressure and heart rate which may be relevant considerations if completing multiple trials in short periods of time (Innes, 1999).
When noting the HGS score, 50% of respondents recorded the mean of three trials for each hand as opposed to the maximum trials for each hand. Previous research has identified the preferred methods to obtain maximum HGS is to use the mean of three trials as this was found to produce the highest reliability (Mathiowetz et al., 1984). Use of the mean score also allows for increased consistency when assessing maximal effort as opposed to a single trial (Trossman and Li, 1989). A study by Haidar et al. (2004) found approximately 25% of participants achieved a maximum HGS score on the second or third trial. Therefore, only conducting one HGS trial may not offer a thorough evaluation of an individual’s HGS compared to the mean of three trials.
The reason for assessing HGS may influence the testing protocol used. If the purpose of HGS assessment is to compare with an individual’s previous scores or to work towards a client’s functional goal, the use of the ASHT standardised testing protocol may be less critical. However, it is crucial for any comparison of scores whether over time to track progression or when comparing affected to unaffected upper limbs that a consistent approach to the testing procedure is used not only for research purposes, but also for clinical practice (Sousa-Santos and Amaral, 2017).
A study by Woods and Lilly (2018) among Certified Hand Therapists found 93.8% of respondents used the standardised testing position for at least 75% of attempts when assessing HGS. This study found 68% of qualified or qualifying Accredited Hand Therapists utilised the ASHT testing protocol. Woods and Lilly (2018) speculated that as the ASHT guideline book is only available to current members, this is likely to have affected access to the guidelines as it is not a requirement for CHTs to be members of the ASHT. It could therefore be suggested that qualified CHT would have increased professional experience compared to uncredentialled CHT assessing HGS and easier access to the standardised testing protocol which may have influenced the high usage of the ASHT guidelines. The study by Woods and Lilly (2018) did not explore the reasons for assessing HGS or the practice setting. To the authors knowledge, there is currently limited research examining years of professional experience, the reason for assessing HGS and the use of standardised testing procedures. Differences in testing protocol may not only impact reliability of the HGS scores, but also the ability to compare the scores to normative values which have been developed using the ASHT testing protocol.
Interpretation and evaluation of HGS scores
The method for evaluating HGS can vary based on the practice setting and the clinical reasoning of the assessor who determines the most appropriate method of evaluation. Comparison to normative data allows for evaluation of an individual’s performance in relation to the general population (Larson and Ye, 2017; Myles et al., 2022). Consideration of the reasons why a clinician assesses HGS may offer insight into how HGS is interpreted and evaluated including the use of normative data for comparison. Sixty-nine percent of respondents stated that they assess HGS for reporting purposes while only 33% stated they assess HGS as part of a pre-employment or functional capacity assessment for which reference to normative data is crucial. In contrast, the majority of respondents identified the reason for assessing HGS was to evaluate rehabilitation progression (baseline assessment) and/or work towards a client’s goal or for return to work purposes. If the main reason for testing HGS does not require formalised evaluation such as comparison to normative values this evaluation process may be seen to be irrelevant or less valuable than other evaluation processes which are individualised to the client.
Practice context was not specified by the respondents. However, all respondents are members of the AHTA and likely to work in professional roles which are primarily focused on assessment and the treatment of the upper limb. Previous research found that clinicians working in hospital and private hand therapy practice settings were less likely to utilise normative data to evaluate HGS scores and more accustomed to comparing with an individual’s previous HGS scores or comparing affected versus unaffected upper limbs (Myles et al., 2022). Only 49% of respondents use normative data to evaluate HGS scores with the most commonly referred normative data set being that of Mathiowetz et al. (1985). Other methods of evaluation included comparison of affected to unaffected or right to left upper limbs (96%), recording progression over time (96%) and client feedback (30%). This speaks to the concept that interpreting and evaluating HGS goes beyond comparison to normative data and can include comparative evaluation, numerical analysis and feedback from clients based on their goals. Professional experience, practice context and clinical reasoning may be used to inform not only the HGS testing protocol but also the interpretation of the scores on a case-by-case scenario (Myles et al., 2022).
The influence of biological and functional factors on HGS
There are several biological (age, gender, height, weight, Body Mass Index, hand and forearm length, forearm circumference) and functional (hand dominance, employment, lifestyle) factors which are known to influence HGS. Respondents were asked to rank in order which factors they believed have the strongest influence on HGS. The top responses in rank order were gender, age, employment, lifestyle, hand dominance, forearm circumference, height and hand length.
It is commonly acknowledged that age and gender are known to influence HGS (Agnew and Maas, 1982; Angst et al., 2010; Mathiowetz et al., 1985). The results of this study found that the clinician’s ranking of gender was the most significant influencing factor on HGS which aligns with previous research. Studies by Eidson et al. (2017) and Moy et al. (2015) found men have higher HGS than women of the same age with gender considered to be a significant predictor of HGS. Biological differences between men and women such as an increase in muscle mass for men compared to women is likely to describe this variation between genders (Gallagher et al., 1997). This supports the continuation of segregation of normative data into gender.
Normative data is also categorised according to age. Age was selected by many respondents to have an impact on HGS. The impact of ageing sees a decline in HGS due to the loss of muscle mass (Abe et al., 2016; Agnew and Maas, 1982; Dodds et al., 2014; Mathiowetz et al., 1985). Previous studies have detailed this phenomenon of reducing HGS with increasing age as part of the normal ageing process (Agnew and Maas, 1982; Dodds et al., 2014; Günther et al., 2008; Mathiowetz et al., 1985; Moy et al., 2015).
Forearm circumference, height and hand length were selected as the most influential anthropometric characteristics on HGS. Several studies have documented forearm circumference as a strong influencing factor for HGS (Eidson et al., 2017; MacDermid et al., 2002; Mohammadian et al., 2015; Saremi and Rostamzadeh, 2019). This relationship is thought to be due to the thickness of anterior forearm muscles at this location which correlates to an individual’s muscle mass (Abe et al., 2016).
Following forearm circumference, both hand length and height were ranked higher than other anthropometric factors influencing HGS by respondents. Hand length is considered a prime criterion to estimate height (Agnihotri et al., 2008). Respondents may have been drawing on their clinical reasoning with the consideration that taller individuals have larger hands which may be seen to provide a mechanical advantage when gripping the dynamometer during HGS testing. A study by Saremi and Rostamzadeh (2019) found individuals with larger hands had stronger HGS and hypothesised that this was due to increased muscle mass.
The functional factors of hand dominance, employment and lifestyle were seen to influence HGS. Normative data for HGS is categorised into right and left hands; however, hand dominance is not considered. Previous studies have found that dominant hand strength is greater than non-dominant hand strength for men and women, particularly for right hand dominant individuals (Moy et al., 2015; Rostamzadeh et al., 2019). Lifestyle factors such as the design of tools and the set-up of the environment are generally made for right-handed individuals. This may explain the lack of difference between hand strengths in left hand dominant individuals as they may have adapted to these factors and utilise their right hand in place of their left hand (Armstrong and Oldham, 1999).
Recent studies have begun to explore the influence of employment and lifestyle factors on HGS. A study by Myles et al. (2022) found that knowing the physical demands of an individual’s employment influenced the expectations of their HGS scores. Manual workers have been found to have increased HGS compared to non-manual workers (Lo et al., 2020; Rostamzadeh et al., 2020). However, some studies found no difference in HGS related to employment (Günther et al., 2008; Mohammadian et al., 2015). Employment forms a significant part of an individual’s daily life and thus, the impact of hand function and in turn evaluation of HGS may be important in determining suitability and sustainability to perform work demands.
Choice of lifestyle activities outside of employment was seen to influence HGS. This was supported by Myles et al. (2022) who found HGS was influenced by hobbies, sport or unpaid work which requires increased physical demands. As hand function is required to perform most daily activities whether employment-related or during leisure time it is important to consider the influence on HGS of how an individual spends their time and the demands of the activities they are engaged with.
Implications for practice
This study has provided descriptions of how and why clinicians across Australia assess and evaluate HGS.
Limitations and future research
While this study uncovered some interesting findings, it is subject to limitations. One limitation of the present study is that practice setting was not examined within the online questionnaire. The questionnaire was distributed through the AHTA who has a large membership group; however, clinicians who are members of the AHTA are generally working in practice settings specifically treating the hand and arm. Therefore, occupational therapists and physiotherapists working in alternative practice settings such as occupational rehabilitation are unlikely to be members of the AHTA and subsequently not included in the study. Therefore, it is difficult to generalise the reasons why HGS is assessed to all practice settings where HGS is measured.
Conclusion
Current research examining how and why clinicians assess and evaluate HGS is limited.
Clinicians within Australia do not consistently adopt the complete ASHT testing protocol when assessing HGS. The majority consistently perform the assessment in a seated position, using the second handle position of the dynamometer. The most significant aspects of variation are the length of the muscular contraction, either short or sustained and recording the score as either the mean of three trials or the maximum trial for each hand.
Evaluation of HGS also varies depending on the reason for assessment. Clinicians who are reviewing and tracking progression following trauma or injury may simply record the numerical scores over time to track progress or compare the affected upper limb to the unaffected. Evaluation using normative data to compare an individual to the general population was not routinely conducted as a form of evaluation. The reason for HGS testing was found to influence how clinicians assess and evaluate HGS.
Biological and functional factors were considered to impact HGS results. Future research should investigate the reasoning behind the adherence to the ASHT standardised testing protocols and evaluation methods by general clinicians working in a wide range of practice settings.
Key findings
There is considerable variation in testing protocol for HGS
The reason for testing may influence how HGS is assessed and evaluated
Consistent testing protocols within patients is needed for evaluation
What the study has added
Clinicians use a variety of testing procedures and evaluation methods when assessing HGS based on the reason for testing and their clinical experience. Consistent assessment and evaluation protocols are crucial to ensure reliability within patients when testing HGS.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226231208409 – Supplemental material for The how and why of handgrip strength assessment
Supplemental material, sj-docx-1-bjo-10.1177_03080226231208409 for The how and why of handgrip strength assessment by Louise Myles, Nicola Massy-Westropp and Fiona Barnett in British Journal of Occupational Therapy
Footnotes
Acknowledgements
None.
Research ethics
Ethical approval (H8854) was granted by the James Cook University Human Research Ethics Committee dated 25/08/2022.
Consent
Participants were provided with an information sheet regarding the study before providing informed consent selecting ‘yes’ to participate as the first survey question.
Patient and public involvement in data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was: Included in the conduct of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
All authors contributed to the study design of this project. LM completed the data collection process and wrote the first draft of the manuscript. The data analysis, interpretation of results and critical evaluation of the manuscript was completed by LM with guidance from the other authors. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.