
Abstract
Introduction:
Prompt identification of patients susceptible to falls is required by occupational therapists to initiate early falls prevention and management strategies. This study identified the intrinsic and extrinsic risk factors of patients who experience early inpatient falls (within 48 hours of admission).
Method:
A retrospective case-control study was completed at a tertiary hospital. Data were extracted from medical records. Adults aged 18 years and older, admitted with any diagnosis, to any ward within the hospital between July 2019 and June 2020 were included. Cases were identified as those who fell within 48 hours of admission and controls did not experience a fall.
Results:
The study sample included 218 patients (109 cases and 109 control patients). Most falls occurred in the patient’s room (n = 54) or bathroom (n = 47), as a result of slipping (n = 50) or while patients were toileting (n = 32). Multivariate regression analysis identified significant predictors of inpatient falls, including unassisted mobilisation (odds ratio (OR) 5.25), impaired balance (OR 7.25), reduced muscle strength (OR 5.25) and impulsivity (OR 19.57). Receiving occupational therapy reduced risk of falling by 81%.
Conclusion:
Falls risk factors that are predictive of early inpatient falls should be identified at admission and used to prioritise patients for occupational therapy.
Introduction
Globally, falls rates in hospitals typically range from three to 11 falls per 1000 patient days (Heng et al., 2020). Approximately 36% of falls in hospital result in injury with 1% resulting in severe injury (Trinh et al., 2017). Adverse psychological affects including fear of falling and anxiety frequently accompany the physical injury (Slade et al., 2017). In addition, an inpatient fall can increase hospital length of stay by 6.3 days (Melin, 2018) and in high-income countries, approximately 1% of health care costs are related to falls (Montero-Odasso et al., 2022; O’Mahony et al., 2014).
There are a range of risk factors that may contribute to inpatient falls (Najafpour et al., 2019; Royal College of Occupational Therapists, 2020). However, due to the multifactorial nature of falls, no single risk factor has been identified to predict inpatient falls (McKechnie et al., 2017). Early identification of high-risk patients by occupational therapists is essential for falls prevention strategies to be implemented in a timely manner (Hoffmann et al., 2015; Matarese et al., 2015). Hospital occupational therapists require time-efficient ways to identify patients who require intervention. A previous internal audit at Sir Charles Gairdner Hospital in 2019 found that 70% of patients who had experienced an early inpatient fall had not yet seen an occupational therapist despite routine Falls Risk Assessment and Management Plan (FRAMP) use for all patients at hospital admission.
Occupational therapy resources are limited, and services need to be directed to priority patients to ensure effective and high-value occupational therapy. Matching a patient’s need for occupational therapy is important as it can minimise patient adverse events, support successful hospital discharge, reduce the risk of unplanned readmissions and ensure responsible use of therapy time (Barclay et al., 2021; Cuevas-Lara et al. 2019). The objective of this study was to identify the intrinsic and extrinsic risk factors for patients who experience an early inpatient fall, which could support a criterion to triage patients for early occupational therapy input in the acute care setting to reduce inpatient falls, complementing existing hospital falls screening and assessment processes (Montero-Odasso et al., 2022).
Method
Study design and setting
A retrospective case-control study was conducted at an adult tertiary hospital. Data were extracted from medical records for patients aged 18 years and older who were admitted to the hospital with any diagnosis. Reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology statement for observational studies (von Elm et al., 2007).
The aim was to identify all intrinsic and extrinsic falls risk factors that put patients at risk of an early inpatient fall. An early inpatient fall was defined as any fall in the first 48 hours of hospital admission. Patients were case matched by age and gender (Mansournia et al., 2018; Pearce, 2016). A fall was defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower-level (World Health Organization (WHO), 2021).
Participants
Inclusion criteria consisted of adults 18 years and older, admitted with any diagnosis, to any ward within the hospital between July 2019 and June 2020. Cases experienced a fall within 48 hours of admission and controls did not experience any inpatient hospital falls during their admission.
Cases
Cases were identified through a review of hospital falls incident data for the study period. Inpatient falls data are routinely recorded on the hospital Department of Health Clinical Incident Management System since May 2016 (Patient Safety Surveillance Unit, 2022). Incidence of witnessed and unwitnessed falls, including faints and rolls out of bed, are recorded. A medical records audit was completed for all those meeting the inclusion criteria and who fell within the first 48 hours of admission.
Controls
Descriptive statistical analysis was completed on the age and gender data of patients in the case group to inform the sampling criteria of the control group. Controls were selected from the hospitals’ digital patient record using stratified sampling to match the age range and gender of the cases. Control group patients with multiple admissions within the study period had the most recent admission audited.
Audit tool and data variables
A data collection tool based on available falls literature identifying known falls risk factors was developed by the researchers (Supplemental Appendix 1). The data collection tool was hosted within Qualtrics, allowing password-protected storage of data for cases and controls (Qualtrics, Provo, UT, USA). Variables collected for both cases and controls included patient demographics, the reason for admission, co-morbid conditions as classified using the International Classification of Disease Version 11 (WHO, 2018), mobility status, prescribed medications, falls risk factors including cognitive impairment and falls history. Falls prevention interventions provided by occupational therapists such as environmental modifications, education, equipment provision and functional retraining, etc. were also recorded (Supplemental Appendix 1). Additional variables recorded only for patients who experienced a fall included place, date, time and location of fall and activity during the fall (Supplemental Appendix 1).
A FRAMP was also completed on all patients admitted as per standard hospital care (Western Australian Department of Health, 2015). The FRAMP consists of four (yes/no) screening questions: (1) had a fall in the past 12 months; (2) unsteady when walking/transferring or uses a walking aid; (3) confused, known cognitive impairment or incorrectly answers any of the following: age, date of birth, current year and place; (4) had urinary or faecal frequency/urgency or nocturia? (Australian Commission on Safety and Quality in Health Care (ACSQHC), 2022; Western Australian Department of Health, 2015). The FRAMP results were extracted from the medical record with each ‘yes’ recorded as a positive response. Scores for the FRAMP could range from zero to four.
Four researchers undertook the medical records audit and to ensure inter-rater reliability, researchers audited at least five patient files together using the data collection tool at two time points to ensure consistency of audit tool use (Vassar and Holzmann, 2013).
Analysis
Data for case and control groups were exported from Qualtrics into Microsoft Excel, cleaned and imported into IBM® SPSS® version 20 (IBM Corp, Armonk, NY). Descriptive statistics, including mean, frequencies and standard deviation, were completed to describe the study sample and factors present at the time of fall. Pearson chi-squared analysis was completed to identify the significance of categorical patient characteristics, which included gender, age group, mobility status, FRAMP screen result and if admission occurred secondary to a fall. A Kolmogorov-Smirnov test was completed to determine if continuous data were normally distributed, and significance was assessed using a parametric independent t-test. Statistical significance was defined as p ⩽ 0.05. The strength of the relationship between a potential risk factor and falling was quantified using the odds ratio (OR) and a 95% confidence interval (CI). Univariate logistic regression was completed to investigate associations of variables between control and case groups. Variables found to be significant through univariate analysis were included in multivariate logistic regression. Multivariate backward elimination regression was conducted to identify the most significant falls predictors, adjusting for age and gender. Variables were included where significant.
Ethical considerations
Ethical approval was granted by Curtin University Human Research Ethics Office (HRE2021-0011-01) and by the Sir Charles Gairdner Osborne Park Health Care Group (QA40548). All patient data was de-identified and analysed in aggregate form to protect participants’ privacy and maintain confidentiality. As this was a retrospective medical records audit, the need for written participant consent was waived by the Human Research Ethics Office and Institutional Review Board.
Results
Participant selection and baseline characteristics
A total of 839 patients were identified to have fallen in hospital between July 2019 and June 2020 of which 109 were identified to meet the inclusion criteria and experienced a fall within 48 hours of admission. As such the study sample included 218 patients, 109 patients who experienced a fall within 48 hours of admission in the case group and 109 patients who did not experience a fall in the control group. The mean age of patients in the case group was 64.1 years (SD 21.8) and 63.2 (SD 20.7) in the control group. Men accounted for 52.3% of patients in the case group and 51.4% of patients in the control group. There were no statistically significant differences between groups for age or gender (Table 1). Forty seven percent of patients in the case group and 37.0% of patients in the control group could independently mobilise without an aid (p = 0.30). There were 24 patients in the control group admitted to the hospital due to a fall, compared to 19 patients in the case group (p = 0.36). Overall, the groups were similar at baseline with no significant differences observed (Table 1).
Cases and controls baseline participant characteristics.
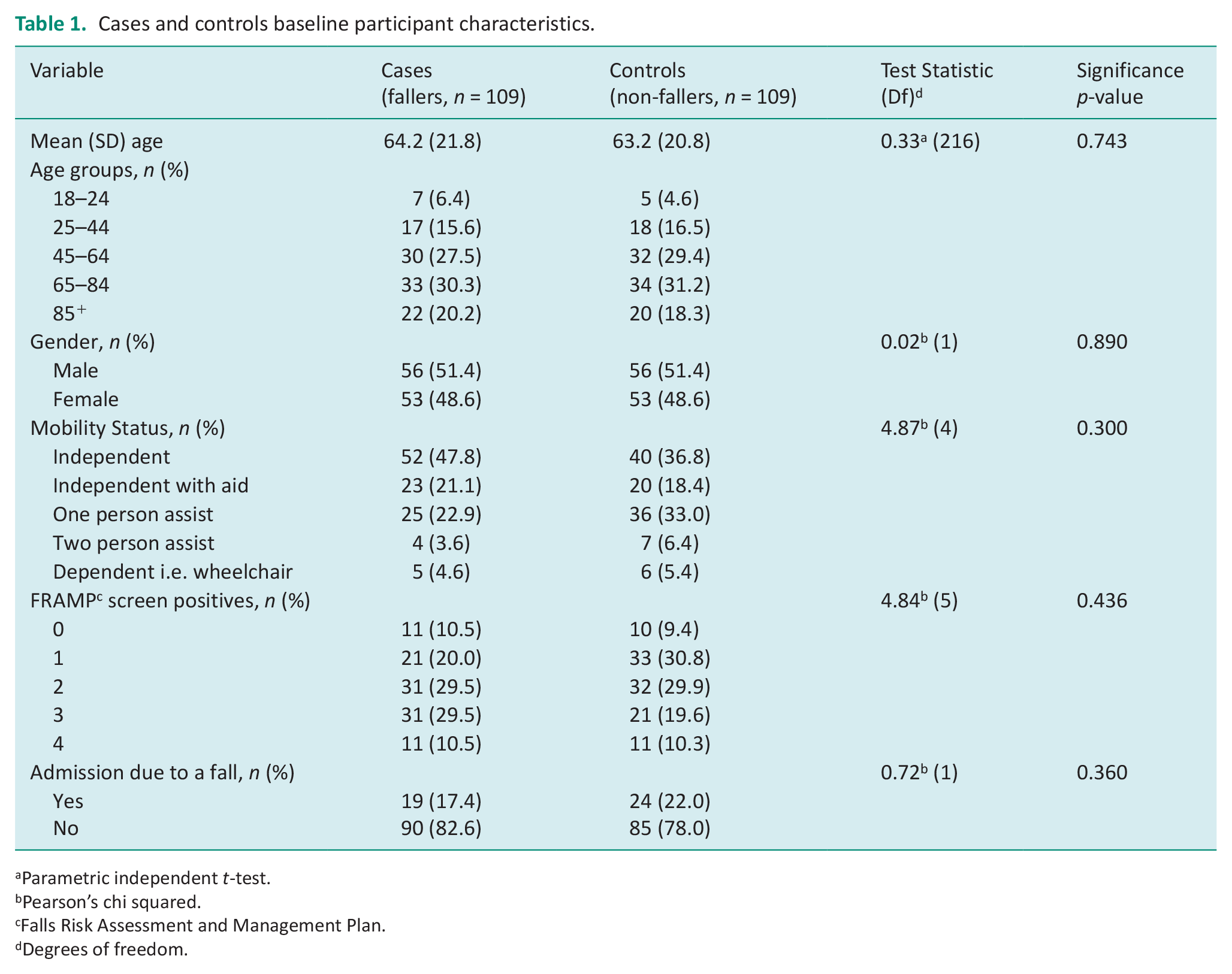
Parametric independent t-test.
Pearson’s chi squared.
Falls Risk Assessment and Management Plan.
Degrees of freedom.
Characteristics of falls
Most falls were evenly distributed throughout the day with 35.8% (n = 39) falling during the day, 33.0% (n = 36) in the evening, and 31.2% (n = 34) overnight. Most falls occurred on a Thursday (30.3%, n = 33) and the least number of falls occurred on a Wednesday (4.6%, n = 5) or a Sunday (4.6%, n = 5). Patients most commonly fell while toileting (29.3%, n = 32) and ambulating (25.7%, n = 28). Slipping was the most common mechanism for falling (45.9%, n = 50). Most falls occurred in the patient’s room (21.1%, n = 54), and of these, 21.1% (n = 23) occurred at the patient’s bed; 10.1% (n = 11) fell while exiting a bed with bedrails in place, and 4.6% (n = 5) while rolling on the bed. The second most common fall location was the bathroom (43.1%, n = 47), with 16.5% (n = 18) falling at the toilet and 9.2% (n = 10) falling in the shower. Most falls were unwitnessed by staff (61.0%) (Table 2).
Characteristics of inpatient hospital falls.
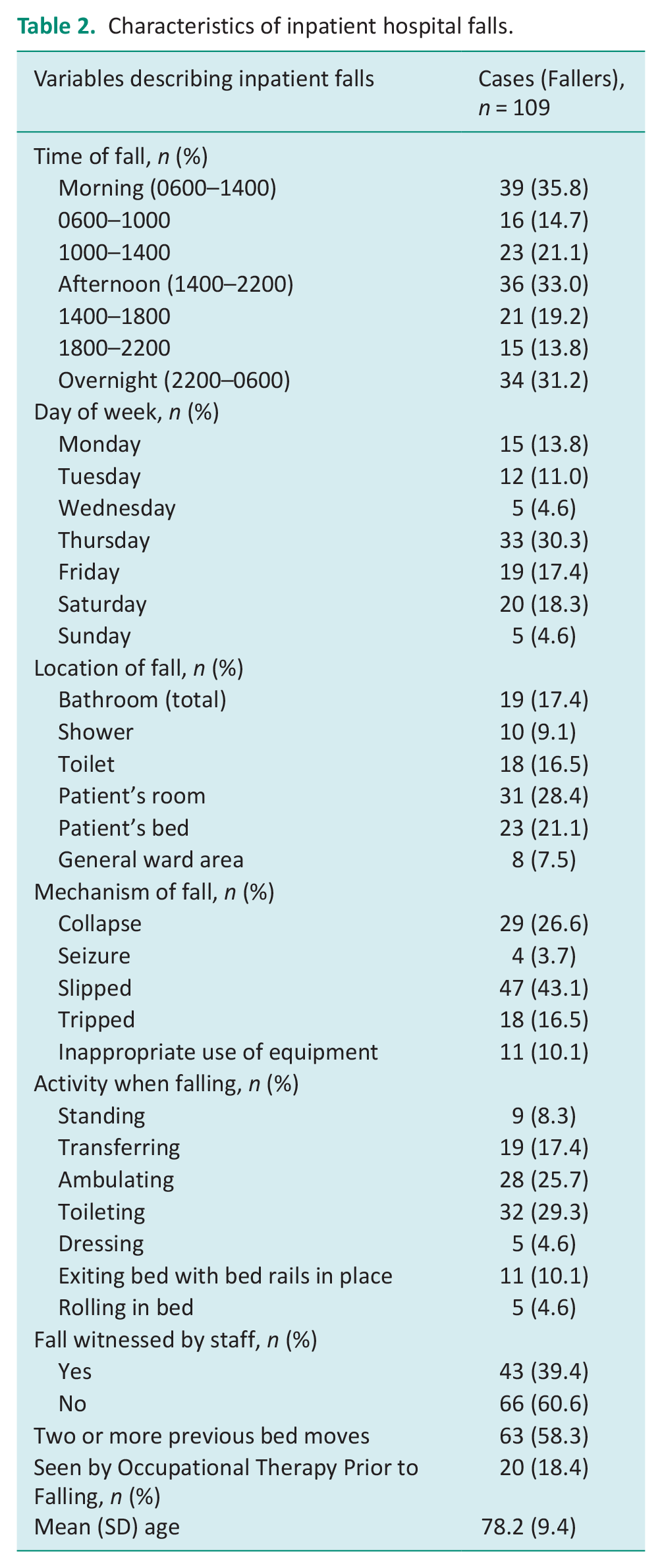
Eighteen percent (n = 20) of patients in the case group were seen prior to their fall by an occupational therapist for either assessment or intervention. Those seen by an occupational therapist were older, with a mean age of 78.2 years and with an equal gender distribution. Patients who were seen by an occupational therapist prior to their fall most commonly had co-morbidities including diabetes, heart disease, stroke, arthritis, musculoskeletal limitations and experienced polypharmacy (Table 2).
Intrinsic and extrinsic falls risk factors predictive of falls
As shown in Table 3, univariate regression identified predictive and protective factors for falls. The intrinsic factors significantly associated with increased early inpatient falls included a diagnosis of neoplasms or cancer, reduced muscle strength, impaired balance, dizziness, malaise and fatigue, and impulsivity. Extrinsic risk factors significantly associated with early inpatient falls were lack of appropriate equipment and unassisted mobilisation (i.e., patients mobilising without awaiting assistance). Conversely, patients with polypharmacy were 57.0% less likely to fall (OR 0.43; 95% confidence interval (CI) 0.24–0.76; p = 0.004), and those consuming benzodiazepines were 49.0% less likely to experience a fall (OR 0.51; 95% CI 0.27–0.97; p = 0.04). Additionally, patients with endocrine, nutritional and metabolic diseases and nervous system disorders (including Parkinson’s Disease) were less likely to have early falls. Patients that received early occupational therapy and had falls prevention interventions were also less likely to experience falls (Table 3).
Univariate logistic regression for associated falls risk factors.
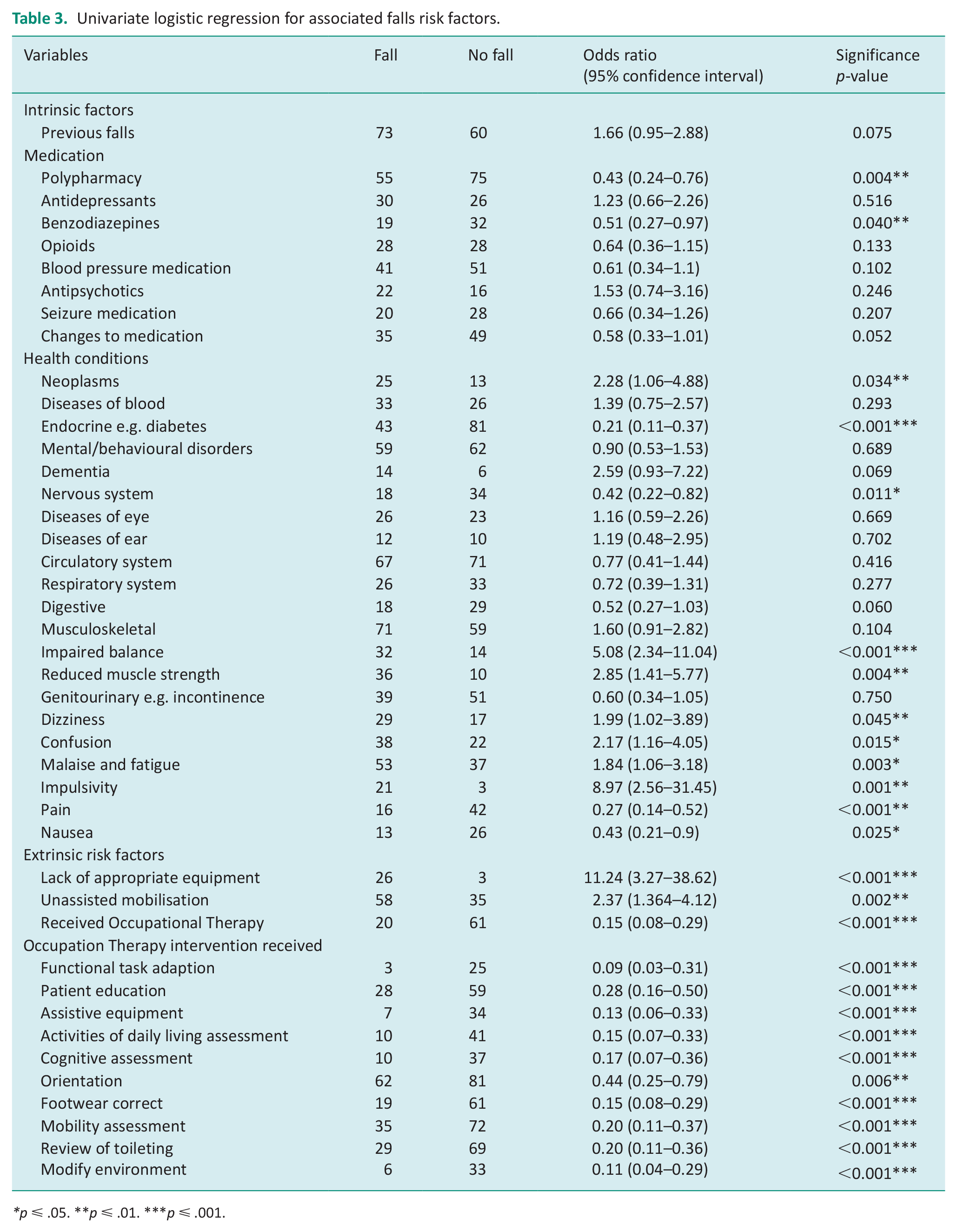
p ⩽ .05. **p ⩽ .01. ***p ⩽ .001.
Table 4 outlines the intrinsic and extrinsic predictors for patient falls as indicated by multivariate logistic regression. Significant predictors for patient falls included reduced muscle strength, impaired balance, impulsivity, and unassisted mobilisation. Multivariate analysis identified that a patient was 81% less likely to fall if they had seen an occupational therapist (OR 0.19; 95% CI 0.04–0.96; p = 0.04). Additionally, the risk of falling was reduced if a patient received assistive equipment (OR 0.13; 95% CI 0.02–0.97; p = 0.04), wore correct footwear (OR 0.19; 95% CI 0.05–0.76; p = 0.01) and had a mobility assessment (OR 0.16; 95% CI 0.04–0.58; p = 0.01).
Multivariate logistic regression.
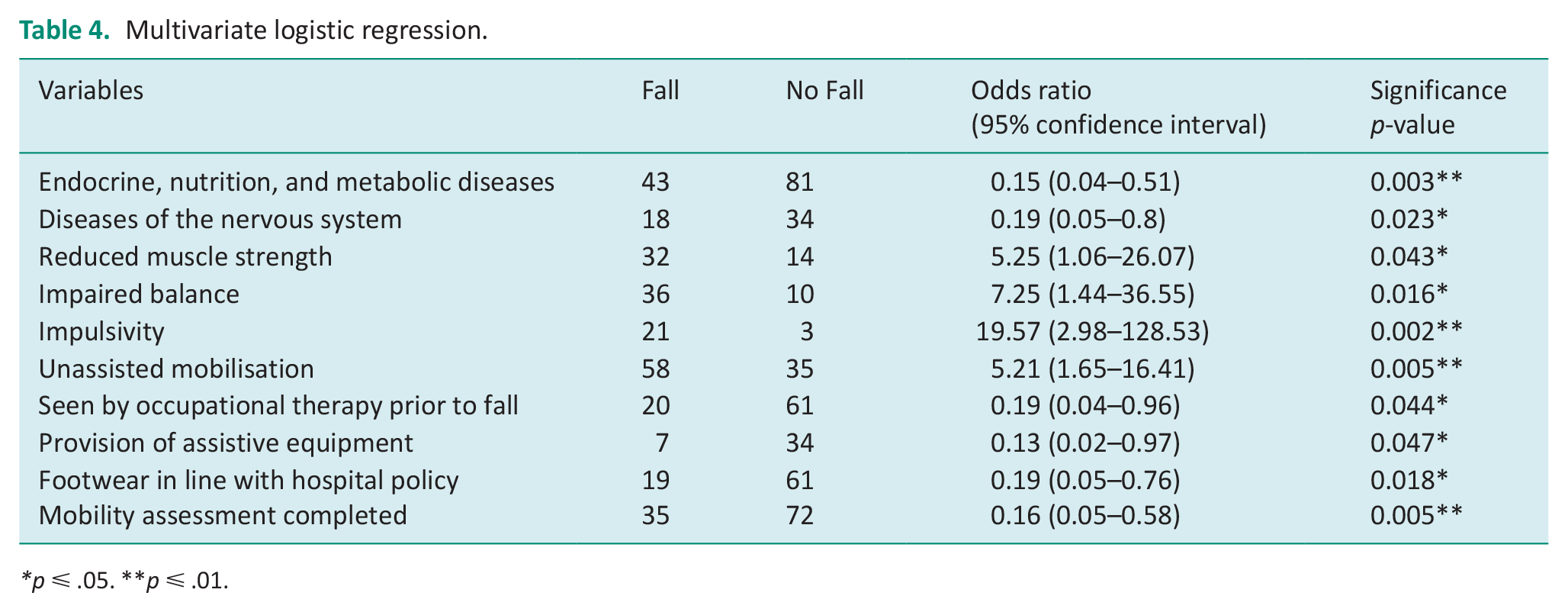
p ⩽ .05. **p ⩽ .01.
Discussion and implications
Findings from this study highlight the intrinsic and extrinsic risk factors for patients who may be at risk of falling within the first 48 hours of hospital admission, allowing occupational therapists to prioritise patients with these risk factors for early assessment and intervention. Patients who mobilised unassisted were at increased risk of falling, as well as those with impaired balance, reduced muscle strength, and documented as impulsive. Receiving occupational therapy input and provision of falls prevention interventions was associated with reduced inpatient falls.
In this study, 50% of fallers were over the age of 65. Advanced age has frequently been reported as a major risk factor for inpatient falls (Zhao and Kim, 2015; De Groot et al., 2020). In our study patients with advanced age were found to fall more frequently; however, this was not predictive of early inpatient falls. This is comparable to other studies, where no relation between older age and inpatient falls was found (Guillaume et al., 2016; Najafpour et al., 2019). Additionally, multiple studies in recent years have identified a positive correlation between male gender and inpatient falls (Cox et al., 2017; De Groot et al., 2020; Guillaume et al., 2016; Rose et al., 2019); however we found that gender was not associated with early inpatient falls.
Patients who mobilised without assistance were found to be 5.2 times more likely to fall in this study. This finding is supported by Rheaume and Fruh (2015), who found that only one in six people called for assistance when needed. Rose et al. (2019) also concluded that 80% of patients who fell were not following their documented level of assistance to mobilise. Patients may overestimate their ability, be experiencing functional decline due to acute illness or perceive their request for assistance as burdening staff (Guillaume et al., 2016; Rose et al., 2019). As this was a retrospective audit this could not be explored further with patients. However it highlights the significant role occupational therapists have in completing functional assessments and educating patients on functional changes and how to avoid falls.
In this study nearly 50% of patients in the case group were able to mobilise independently prior to admission. Patients who are known to ambulate independently may have been a lower priority for occupational therapy; however, therapists need to consider if acute illnesses are likely to impact on a patient’s function and need for earlier intervention. Similar to existing literature dizziness, malaise and fatigue were associated with falls and reduced muscle strength, imbalance, and impulsivity were significant predictors of falls (De Groot et al., 2020; Heslop et al., 2012; McKechnie et al., 2017; Zhao and Kim, 2015). These symptoms are known risk factors for falls (McKechnie et al., 2017) and should continue to be identified by occupational therapists at hospital admission.
Benzodiazepine use and polypharmacy (prescription of 5 or more medications) was associated with decreased falls in this study. Literature has previously identified polypharmacy, particularly psychoactive drugs, as a risk factor for falls (Wedmann et al., 2019; Zhao and Kim, 2015). Heslop et al. (2012) concluded that polypharmacy of psychoactive medication might result in physiological instability and orthostatic hypotension. Although there is evidence to support the association between polypharmacy and falls, research by Najafpour et al. (2019), also found polypharmacy to have no significant association with an increased risk of falling. Benzodiazepine use has been found to increase inpatient falls risk (de Groot et al., 2020; Najafpour et al., 2019; Rheaume and Fruh, 2015). The exception is the study conducted by Wedmann et al. (2019), who concluded that only long-acting benzodiazepines are a significant falls risk, whilst short and intermediate-acting benzodiazepines are not. In our study it is likely that although known risk factors including psychoactive drug use and neurological movement disorders were not identified as predictive factors, these patients were receiving input from therapist to manage falls risk factors.
Most falls in this study occurred while patients were alone. These results are comparable to other studies, where 88% of falls were unwitnessed (Guillaume et al., 2016), and 100% of all serious falls were unwitnessed (Rheaume and Fruh, 2015). Evidence suggests that patients are at higher risk of falling when staff are needed elsewhere, and patients are unsupervised (e.g., during staff handover or educations sessions) (Heslop et al., 2012; Zhao and Kim, 2015). Najafpour et al. (2019) suggested that regular nursing rounds, placing patients in visible rooms near nursing stations and scheduled assisted toileting may be effective interventions to reduce unwitnessed falls occurring. Occupational therapists can identify patients at risk and support implementation of these strategies.
Patients were 81% less likely to fall if they received intervention from an occupational therapist. Receiving falls prevention interventions was associated with lower falls rates, indicating that occupational therapy intervention is effective in preventing falls. Effective interventions included providing equipment, ensuring appropriate footwear, and facilitating a mobility assessment which all decreased falls likelihood by 87%, 81%, and 84%, respectively.
We are unaware of any other studies that have outlined risk factors for patients that are likely to fall within 48 hours of a hospital admission. This research can improve an occupational therapist’s knowledge and ability to triage and prioritise high-risk patients based on information received at admission. Close to 90% of patients in this research screened positive to at least one FRAMP question, indicating that most are at risk of falls. However, this research can support risk grading. Effective identification of high-risk patients can enable the provision of earlier intervention to reduce the occurrence of falls or reduce the risk of injurious falls. This study highlights the need for a multicomponent approach to falls prevention, starting with occupational therapist awareness of risk factors, patient and family education, continued identification of at-risk patients, and implementation of effective falls prevention strategies.
Limitations
This study was conducted at one hospital site and the results may not be generalisable to other settings. Concerns regarding the generalisability of results from a single-hospital study were moderated by selecting a large sample size from wards across the hospital (Cox et al., 2017; De Groot et al., 2020; Najafpour et al., 2019). This study was limited by the content of medical records and how researchers interpreted the information. Steps were taken to reduce bias such as developing and piloting the audit tool to support data extraction and the use of four research assistants involved in data extraction with inter-rater reliability of audit tool use reviewed.
Future research
The risk factors identified in this study could be used to develop a criterion to triage patients for review in acute hospital settings. These criteria could be reviewed and tested in future clinical research. Additionally, a prospective mixed-methods study may be beneficial to collect valid data on risk factors not typically recorded in patient files through interviews with patients and clinicians including exploring mobilisation without awaiting assistance (Najafpour et al., 2019; Zhao and Kim, 2015).
Conclusion
This study identified intrinsic and extrinsic risk factors of patients who experienced early inpatient falls in the acute care setting. Patient characteristics associated with early inpatient falls included impaired balance, reduced muscle strength, impulsivity, and patients who had experienced a change in mobility function and were likely to mobilise without asking for assistance. These risk factors should be identified on admission to hospital and used to prioritise patients for occupational therapy. The findings also highlighted the impact of occupational therapy intervention and assessment in preventing falls.
Key findings
Occupational therapists should triage patients with impaired balance, reduced muscle strength, and impulsivity.
Early occupational therapy reduced inpatient hospital falls.
Age, gender, and pre-admission mobility status did not predict falls.
What the study has added
Key risk factors from an occupational therapy perspective have been identified which can be used to triage patients for inpatient therapy supporting existing hospital falls risk assessment and management processes.
Supplemental Material
sj-doc-1-bjo-10.1177_03080226231181019 – Supplemental material for Prioritising patients for hospital occupational therapy to reduce inpatient falls: A retrospective case-control study to identify predictive patient falls risk factors
Supplemental material, sj-doc-1-bjo-10.1177_03080226231181019 for Prioritising patients for hospital occupational therapy to reduce inpatient falls: A retrospective case-control study to identify predictive patient falls risk factors by Kristie J Harper, Emily Mast, Grace Carter, Trey Katnich, Vincent Oldham and Claire Morrisby in British Journal of Occupational Therapy
Supplemental Material
sj-docx-2-bjo-10.1177_03080226231181019 – Supplemental material for Prioritising patients for hospital occupational therapy to reduce inpatient falls: A retrospective case-control study to identify predictive patient falls risk factors
Supplemental material, sj-docx-2-bjo-10.1177_03080226231181019 for Prioritising patients for hospital occupational therapy to reduce inpatient falls: A retrospective case-control study to identify predictive patient falls risk factors by Kristie J Harper, Emily Mast, Grace Carter, Trey Katnich, Vincent Oldham and Claire Morrisby in British Journal of Occupational Therapy
Footnotes
Acknowledgements
Thank you to Melinda Williamson and Colleen O’Brien-Malone for providing feedback during manuscript development.
Research ethics
Ethical approval was granted by Curtin University Human Research Ethics Office (HRE2021-0011-01) and by the Sir Charles Gairdner Osborne Park Health Care Group (QA40548) during 2020.
Consent
As this was a retrospective medical records audit, the requirement for informed consent to participate was waived by the Ethics Committee and the Institutional Review Board.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
EM, GC, TK and VO researched literature and conceived the study with the support of KH and CM. All authors were involved in protocol development and gaining ethical approval. EM, GC, TK, VO and KH completed the medical records audit and EM, GC, TK and VO completed the data analysis. EM, GC, TK and VO wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.