
Abstract
Introduction:
Motor imagery (MI) may be an effective tool for improving activities of daily living (ADL) post-stroke. However, no review to date has examined ADL independence when investigating training effectiveness. This review aimed to evaluate the quality of evidence and the effectiveness of MI training for improving ADL independence post-stroke.
Method:
Randomized controlled trial (RCT) studies comparing MI to conventional therapies were reviewed. Methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) scale.
Results:
Thirteen articles met inclusion criteria. The overall quality was considered moderate to good, with a PEDro score ranging from 3 to 8. Most studies (9 out of 13) were considered good quality, with one rating of poor quality and three of fair quality. The primary findings suggest that MI training is a low-risk tool that may facilitate ADL independence. Audio-based MI training seems to improve ADL independence when paired with other rehabilitation methods, but the results should be interpreted with caution.
Conclusion:
To our knowledge, this is the first systematic review to examine RCTs investigating MI effectiveness in improving ADL post-stroke. Results support the use of MI to facilitate ADL independence. However, more research is needed to establish practice guidelines for implementing MI training post-stroke.
Introduction
Around half of stroke survivors experience long-term impairments in their ability to perform activities of daily living (ADL) (Miller et al., 2010). ADL fall into two categories: basic activities of daily living (BADL) and instrumental activities of daily living (IADL). BADL refer to the fundamental skills needed to manage one’s physical needs, such as toileting, eating, bathing, and mobilizing within one’s environment. BADL are often assessed using the Barthel Index (BI) and the Functional Independence Measure (FIM) (Schepers et al., 2006). Assessment scores capture the extent of assistance needed by the patients to complete different tasks, providing a measure of ADL independence. IADL are a set of more complex skills needed to live independently, such as cleaning, cooking, and money management, which are usually measured by performance tests (e.g., Liu et al., 2009).
Occupational therapy is essential to facilitating ADL independence following stroke (Steultjens et al., 2003). Treatment from an occupational therapist may include the training of lost performance skills or the teaching and practice of strategies that compensate for the stroke survivor’s new functional baseline (Steultjens et al., 2003). Both strategies enable patients to complete ADL as safely and independently as possible. Occupational therapy often involves task-oriented training, or the repeated physical practice of the target task to improve its performance (Steultjens et al., 2003). However, several factors can limit intensive physical task practice, including patient symptoms of pain, fatigue, or severe hemiplegia and systemic constraints that restrict dedicated therapy time (Luker et al., 2015).
One consideration is supplementing physical task repetitions with motor imagery (MI) or the mental rehearsal of movement without its physical performance. Regular use of MI facilitates motor skill acquisition in healthy and athletic populations (Ruffino et al., 2017). This facilitation is particularly significant when MI is paired with physical task practice (Ruffino et al., 2017). Brain imaging studies provide a possible explanation for these benefits, with MI training shown to induce both short- and long-term reorganization of sensorimotor cortices (Ruffino et al., 2017). This restructuring is proposed to facilitate other processes that rely on these networks, such as motor execution (Ruffino et al., 2017).
It has been demonstrated that MI training paired with physical practice is more effective at improving upper extremity function post-stroke than physical practice alone (Barclay et al., 2020). The effect of MI training on ADL independence is comparatively unclear. In two recent review studies, Guerra et al. (2017) and Barclay et al. (2020) reported that MI training may not improve ADL independence post-stroke. However, the results were based on a small sample of studies (e.g., 3 out of 32 studies in Guerra et al., 2017; 4 out of 25 studies in Barclay et al., 2020). High study heterogeneity and risk of bias also limited confidence in the documented null results (Barclay et al., 2020; Guerra et al., 2017).
Furthermore, for MI to be effectively implemented in stroke rehabilitation, one factor to consider is the instruction mode of MI training (Schuster et al., 2011). Patients may receive MI training through direct therapist instruction during in-person treatment sessions. Training can also be completed outside of direct therapist supervision through pre-recorded audio or visual-based instructions. This approach enables patients to participate in low-risk activities outside of time-restricted treatment sessions. The majority of MI training interventions in the rehabilitation literature have been delivered via pre-recorded instructions (Schuster et al., 2011). How different modes of instruction impact MI effectiveness on ADL independence has never been systematically reviewed.
To the best of our knowledge, no review has used ADL independence as its primary outcome measure when investigating the effectiveness of MI training in stroke rehabilitation. Given occupational therapy’s established role in facilitating ADL independence, an investigation into treatments that may reduce patient dependency on ADL is highly relevant to the profession (Steultjens et al., 2003). We thus carried out a systematic review with two objectives (1) to examine the quality of evidence investigating the effect of MI training on ADL independence post-stroke and (2) to evaluate the effectiveness of MI training on ADL independence post-stroke, with modes of MI instruction taken into consideration.
Methods
Search strategy
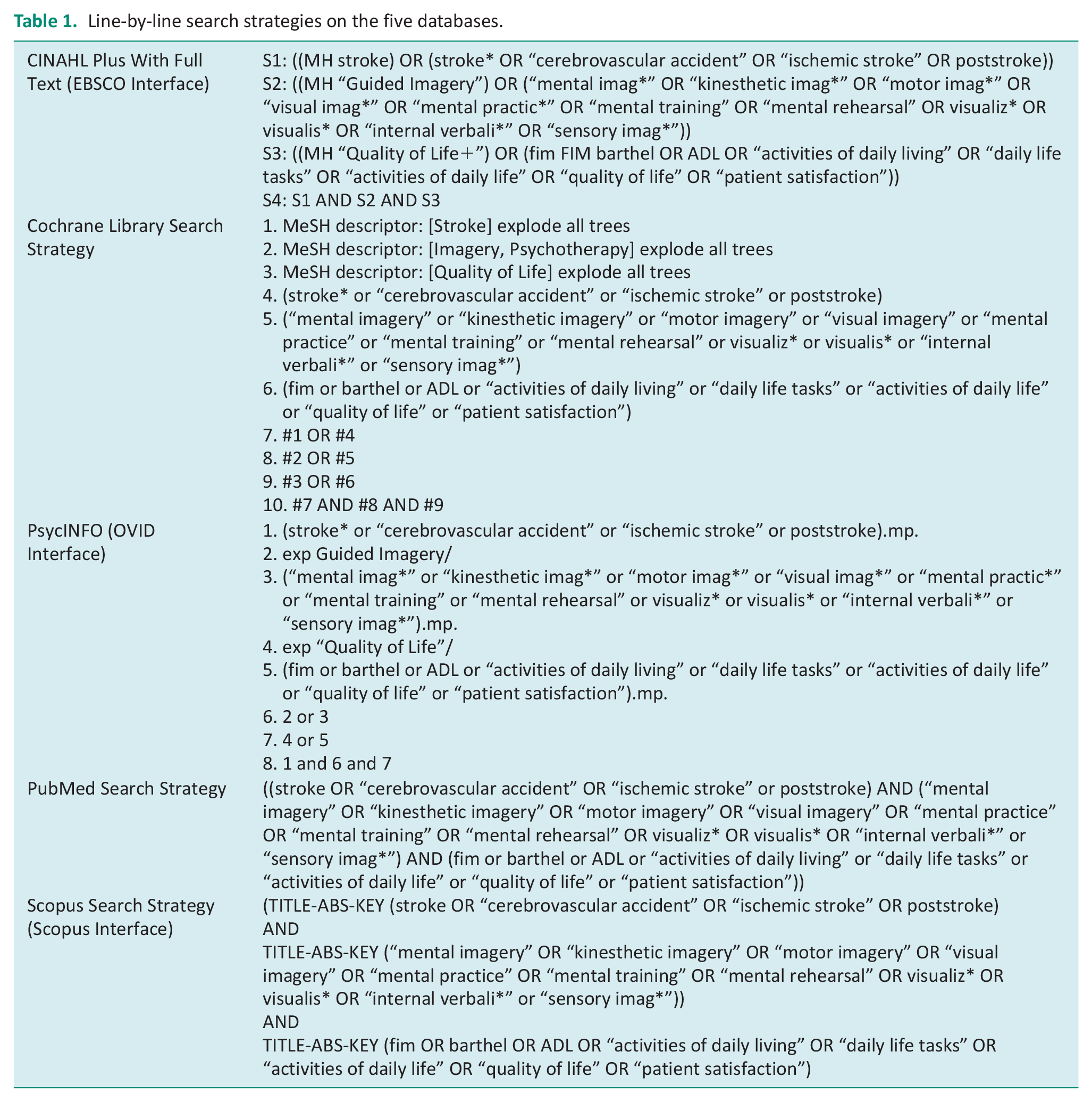
This systematic review was carried out in April 2021 and followed the guidelines recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009). The search strategy was developed in collaboration with a health sciences librarian. Searches were conducted in CINAHL, Cochrane Library, PsycINFO, PubMed, and Scopus databases (see Table 1 for search strategy details). While quality of life was included in the initial search as a potential outcome of interest, it was later determined that the review should focus solely on independence in ADL as opposed to combining both outcomes, which are conceptually distinct. No limits such as English language, specific publication dates, region, or study design were applied to the search as reviewers wanted to safeguard against incidentally omitting any mis-indexed or yet-to-be-indexed articles. Search results were exported to Covidence (https://www.covidence.org), and duplicates were removed before being screened for eligibility.
Line-by-line search strategies on the five databases.
Selection of studies
Articles were eligible for inclusion if they met the following criteria: (1) randomized controlled trial design; (2) full-text manuscript published in English in a peer-reviewed journal; (3) stroke survivors at any stage of recovery as study participants; (4) an experimental group that received MI training in isolation or in combination with conventional therapy or in combination with another experimental therapy; (5) a comparison group that received conventional therapy or the other experimental therapy, either in isolation or paired with a placebo treatment; and (6) reported results on an outcome measure that assessed level of patient independence during the performance of three or more ADL. The requirement of three or more ADL is in line with previous systematic reviews (Janaudis-Ferreira et al., 2014).
Identification of the relevant literature
Once duplicates were removed, five reviewers (KL, CH, JH, CM, and NB) screened each title and abstract for inclusion. The article was added to the full-text review if relevance was unclear from abstract screening. Each full-text article was then independently assessed for review inclusion by two of five reviewers (KL and NB). Disagreements regarding inclusion were resolved by a third reviewer (AL). Reference lists of the included studies were screened to identify additional relevant articles. Two reviewers (KL and NB) then independently extracted data from each study and organized the data into two separate tables, one for each reviewer, including the following elements: study population and setting, description of the intervention, target outcome measures, key results related to ADL independence, and study quality.
Methodological quality assessment
We used the Physiotherapy Evidence Database (PEDro) scale to assess methodological quality of the included studies (Cashin and McAuley, 2020). The PEDro scale consists of eight questions that assess the internal validity of a study and two questions that assess the study’s statistical completeness (Cashin and McAuley, 2020). It defines the quality of a survey as excellent with a score of 9–10, good with a score of 6–8, fair with a score of 4–5, and poor with a score below 4. For complex interventions, such as those commonly administered by an occupational therapist, a total PEDro score of 8/10 is considered optimal as it is often impossible to blind participants or the therapists administering treatment (Cashin and McAuley, 2020). Two reviewers familiar with the PEDro (KL and NB) independently assessed the quality of each study, with any disagreement resolved by a third reviewer (AL).
Data analysis and synthesis
The two extraction tables organized by KL and NB were then compared and the data synthesized to create a single data table. The effectiveness of MI was further analyzed by categorizing the studies according to modes of MI instruction. A traditional meta-analysis was not conducted due to the small number of studies within each category and the heterogeneity of measurements used in the studies. Instead, this review applied a narrative synthesis approach to review MI effectiveness and included a calculation of effect size (ES) on outcomes relevant to ADL independence in each of the studies. This approach is supported by the Cochrane Handbook, especially when heterogeneity in measurement is a concern (McKenzie and Brennan, 2020). The advantage of using ES to support narrative synthesis is that it allows the comparison of MI effects on a uniform scale to facilitate the quantification and interpretation of treatment effects. The ES was calculated by dividing the differences in mean scores post-intervention between the two comparison groups by the pooled baseline standard deviation; ESs of 0.8, 0.5, and 0.2 are considered large, medium, and small, respectively (Cohen, 2013).
Results
The search results are presented in the PRISMA flow diagram (Figure 1). The initial search yielded 647 titles and abstracts. After the removal of 221 duplicates, 426 titles and abstracts were screened, 114 articles were included full-text screening, and 101 articles were excluded as they did not meet inclusion criteria. A total of 13 articles met the inclusion criteria and are summarized in Table 2. Included studies were carried out in Hong Kong (Liu et al., 2004, 2009), the Netherlands (Braun et al., 2012), Scotland (Ietswaart et al., 2011), China (Pan et al., 2019; Yin et al., 2022), South Korea (Ji et al., 2021; Nam et al., 2019; Park, 2015, 2020; Park et al., 2015), and two in unspecified locations (Ahmad et al., 2014; Kulkarni and Sureshkumar, 2018).
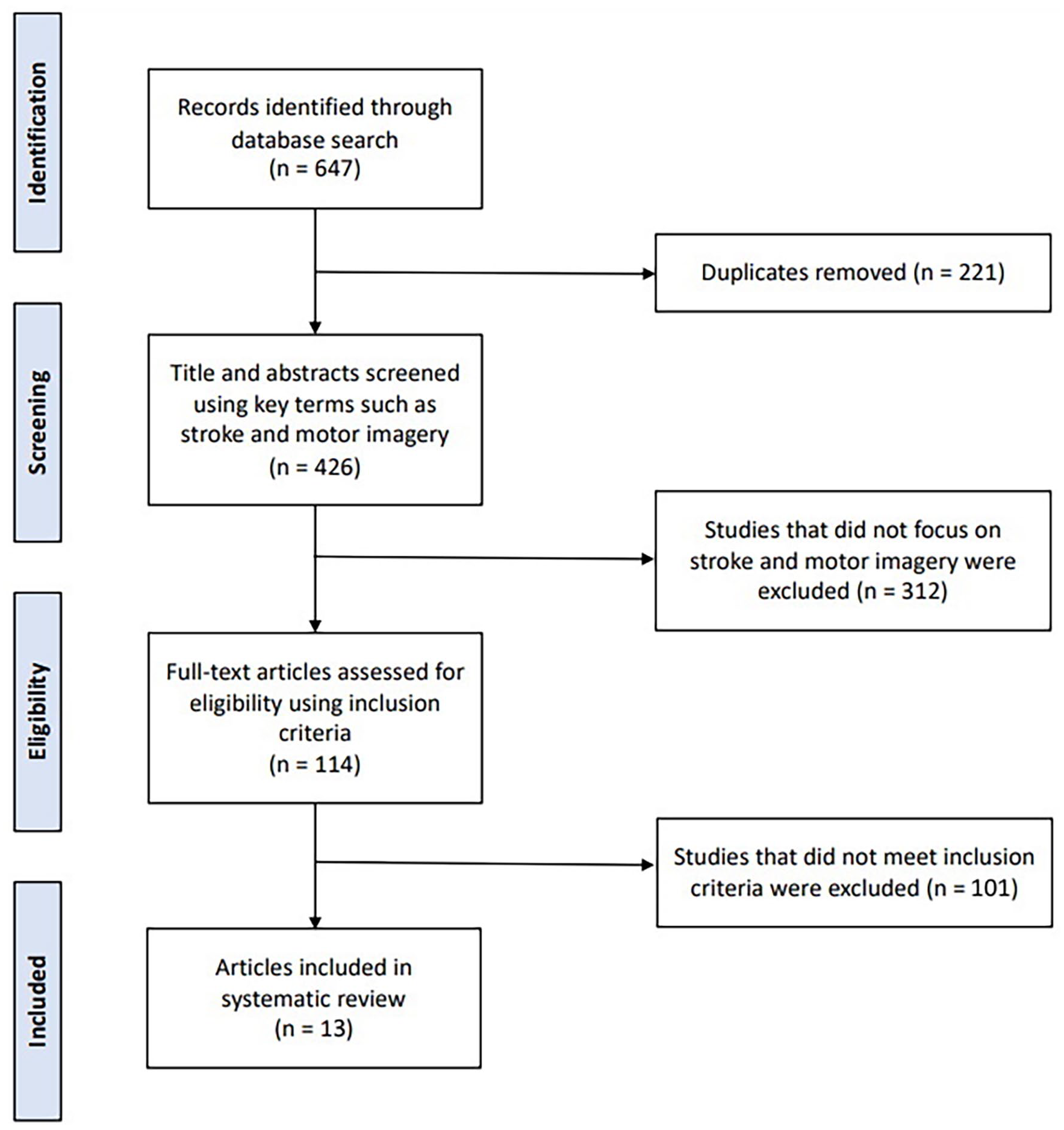
PRISMA flow diagram of the article screening process.
Descriptive summary and the Physiotherapy Evidence Database (PEDro) score of reviewed studies.
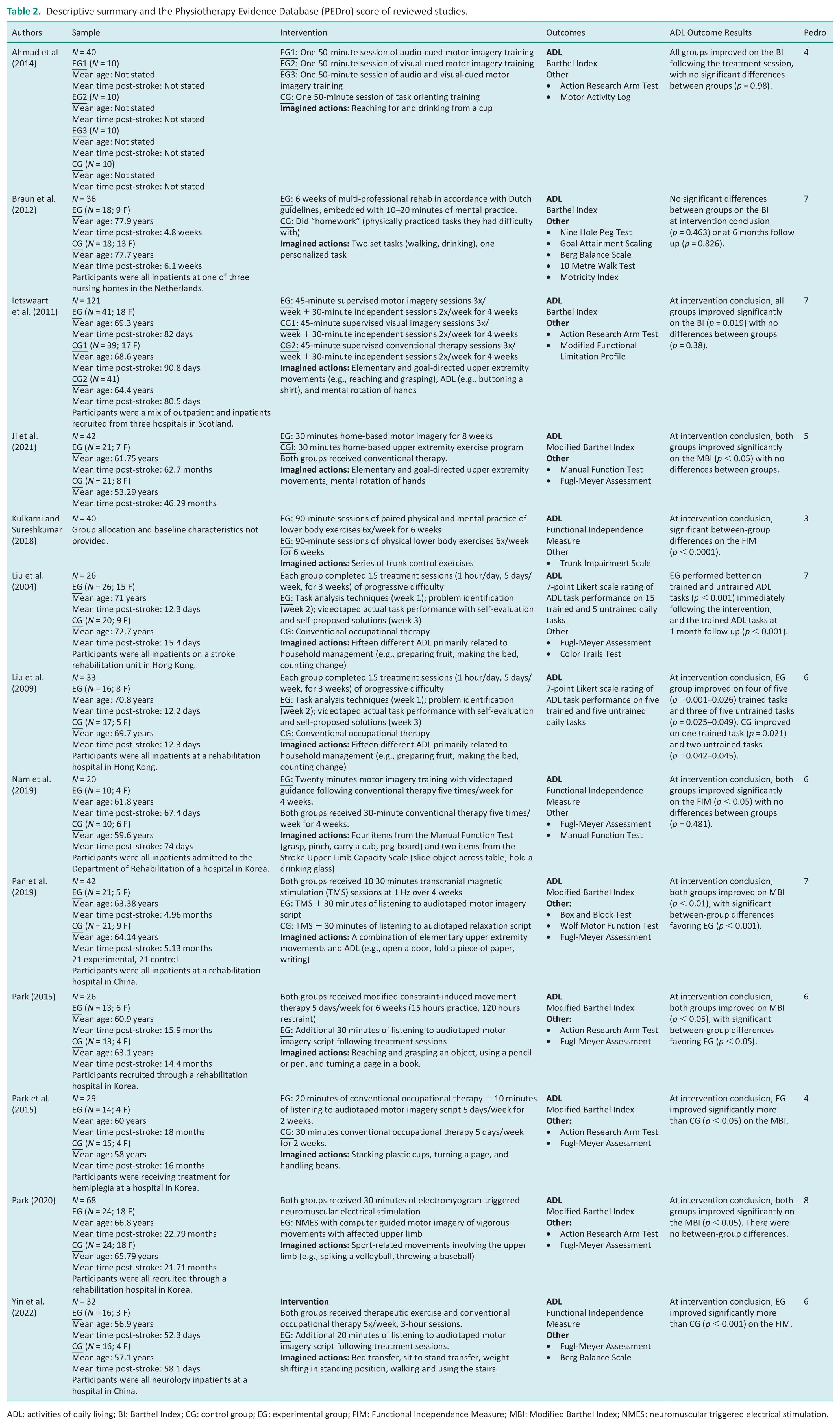
ADL: activities of daily living; BI: Barthel Index; CG: control group; EG: experimental group; FIM: Functional Independence Measure; MBI: Modified Barthel Index; NMES: neuromuscular triggered electrical stimulation.
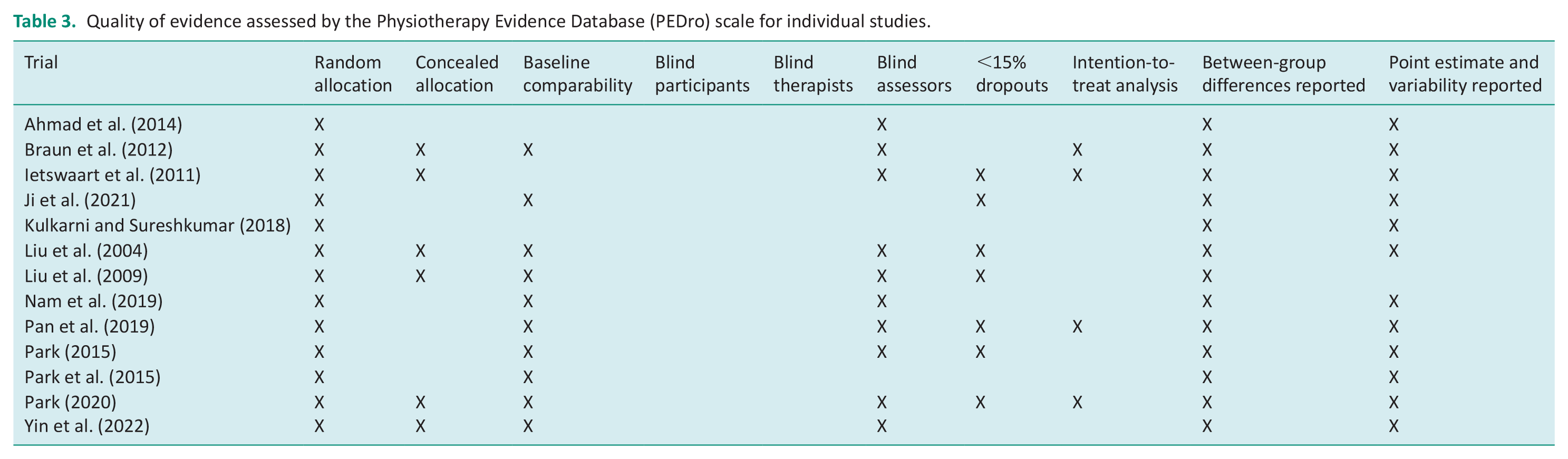
In terms of quality, the PEDro score indicated that one study was rated poor, three rated fair, and nine rated good. A summary of the articles and their PEDro scores were presented in Table 2, and details of the quality of evidence were presented in Table 3. The most common sources of bias were lack of blinding (n = 13), intention-to-treat analysis (n = 10), and concealed allocation (n = 7).
Quality of evidence assessed by the Physiotherapy Evidence Database (PEDro) scale for individual studies.
The studies included a total of 555 participants. The average time since the participants experienced their stroke ranged from 2 weeks in Liu et al. (2004) to over 5 years in Ji et al. (2021). Imagined actions varied in complexity, with some studies involving imagery of elementary movements, such as opening and closing a fist (Nam et al., 2019), while others had participants imagine completing household management activities (Liu et al., 2004, 2009). Interventions ranged from a single session (Ahmad et al., 2014) to five sessions per week for 8 weeks (Ji et al., 2021). The cumulative dose of MI training ranged from 50 minutes (Ahmad et al., 2014) to 1680 minutes in Ji et al. (2021).
Three studies used the BI to measure independence in BADL (Ahmad et al., 2014; Braun et al., 2012; Ietswaart et al., 2011), while the Modified Barthel Index (MBI) was used in five studies (Ji et al., 2021; Pan et al., 2019; Park, 2015, 2020; Park et al., 2015). Independence in ADL was measured in two studies using the full FIM (Kulkarni and Sureshkumar, 2018; Nam et al., 2019). Yin et al. (2022) used the transfer and locomotion subscales of the FIM as opposed to the scale in its entirety. An original outcome measure was employed in two studies (Liu et al., 2004, 2009). In this measure, participants were observed performing different IADL, with the level of support needed for them to successfully perform the task rated on a 7-point Likert Scale.
The primary mode of MI delivery included direct therapist instruction (Braun et al., 2012; Ietswaart et al., 2011; Liu et al., 2004, 2009), pre-recorded audio scripts (Pan et al., 2019; Park, 2015; Park et al., 2015; Yin et al., 2022), video recordings (Nam et al., 2019), text instructions presented on a computer screen (Park, 2020), and images shown on a computer screen (Ji et al., 2021). These studies were categorized into modes of MI instruction for further analysis, thus leading to the generation of three categories: therapist-directed MI (n = 4), audio-guided MI (n = 4), and visual-guided MI (n = 3). The calculated ESs of studies are available in Figure 2. ESs were calculated from the original BI, 2 out of 10 studies; the MBI, 4 out of 10 studies; the FIM, 3 out of 10 studies; and an original task observation assessment, 1 out of 10 studies. Two fair-quality studies did not provide any information on the mode of MI instruction (Ahmad et al., 2014; Kulkarni and Sureshkumar, 2018). These two studies were therefore not categorized, and their ESs were not calculated. The ES of one study in the therapist-directed MI category was not calculated as the manuscript did not contain measures of variability for the target outcome measure (Liu et al., 2009). Below are the findings organized according to the mode of MI instruction.
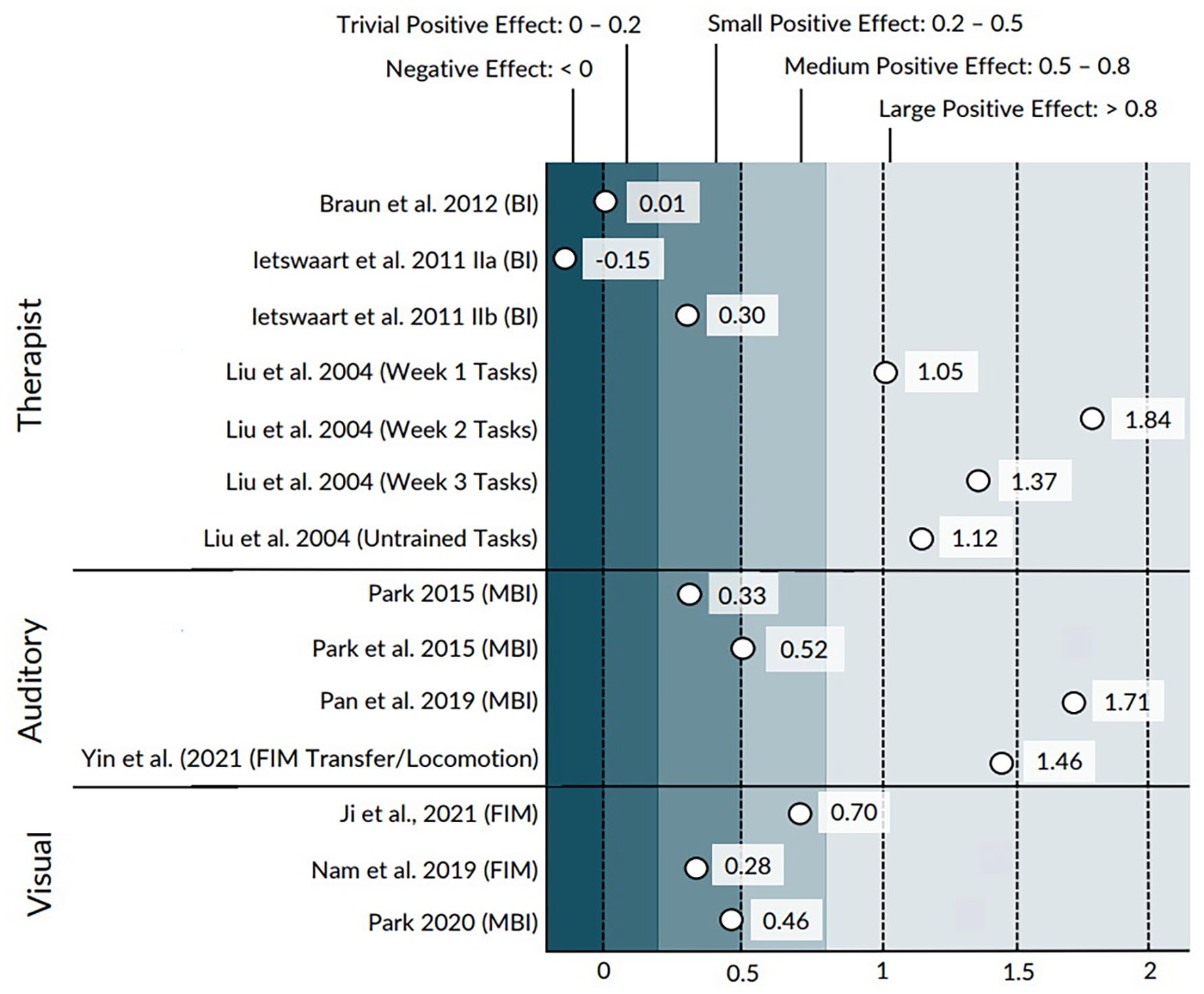
Effect sizes for each study, separated by mode of training delivery. Outcome measures are displayed in parentheses.
Therapist-directed imagery
Four studies, with a total of 245 participants, delivered MI training primarily through in-person therapist instruction (Braun et al., 2012; Ietswaart et al., 2011; Liu et al., 2004, 2009). Three of the studies paired MI training with physical task practice (Braun et al., 2012; Liu et al., 2004, 2009), and one delivered MI training in isolation (Ietswaart et al., 2011). All studies were considered good quality. Three of the studies received a PEDro score of 7 (Braun et al., 2012; Ietswaart et al., 2011; Liu et al., 2004), and one received a PEDro score of 6 (Liu et al., 2009). Participants were in the sub-acute stage of stroke recovery in all studies. The ESs ranged from −0.15 to 1.84, which spans from a trivial effect in favor of the control group to a large effect in favor of the experimental group (Figure 2).
Ietswaart et al. (2011) examined the effect of a MI training program on a mix of inpatients and outpatients. Therapists with a psychology or occupational therapy background delivered highly structured 45-minute sessions broken down into three components: imagery of elementary and goal-directed movements, MI guided by a mirror or video, and mental rotation of hands. Participants additionally completed two sessions of independent MI training that were guided by 30-minute audio recordings. The two control groups received either dose-matched routine care or imagery training that focused on the visualization of objects, as opposed to imagery of movements (Ietswaart et al., 2011). All groups improved similarly on the BI (Ietswaart et al., 2011).
Liu et al. (2004) and Liu et al. (2009) administered the same 3-week MI intervention. This program involved 1 hour of training each weekday on 1 of 15 household management tasks (e.g., making the bed, taking medication, washing dishes) for a total of five trained tasks per week. Working directly with an occupational therapist, participants practiced breaking down each task and identifying deficits in task performance, followed by the mental and then physical rehearsal of the task. In both studies, participants in the experimental group improved significantly more than controls (dose-matched conventional occupational therapy) on the support needed to complete both trained and untrained tasks (Liu et al., 2004, 2009). In Liu et al. (2004), these between-group differences tasks were maintained at 1 month follow up.
Braun et al. (2012) embedded MI into conventional therapy for stroke patients receiving rehabilitation at three different nursing homes. While therapists received protocol training, they were also encouraged to adapt training to the needs of each participant. Participants were trained on two set tasks (e.g., walking, drinking) and a third task of their choosing. While participants were provided with an imagery log to track independent practice, unclear participant reporting limited its interpretation. No significant differences were documented by researchers between the experimental group and controls (dose-matched usual care) on the BI, either at study conclusion or 6 month follow up (Braun et al., 2012).
When considered together, these four good-quality studies provide mixed evidence for the benefits of therapist-delivered MI training on ADL independence. The null results from Braun et al. (2012) and Ietswaart et al. (2011) (n = 157) suggest that this training does not have a significant effect on the BI, a measure of BADL independence. However, the statistically significant effects documented by Liu et al. (2004) and Liu et al. (2009) suggest that therapist-delivered training may be effective intervention if used to target independence in IADL. However, these results were drawn from a comparatively smaller sample size (n = 59) and involved the use of a non-validated measure to assess ADL independence.
Non-therapist directed
Audio-guided MI
Four studies, with a total of 130 participants, delivered MI training through pre-recorded audio scripts (Pan et al., 2019; Park, 2015; Park et al., 2015; Yin et al., 2022). MI training in all studies was standardized across participants (Pan et al., 2019; Park, 2015; Park et al., 2015; Yin et al., 2022). All studies included relaxation exercises at the start of each session and emphasized MI of ADL tasks using the affected limb (Pan et al., 2019; Park, 2015; Park et al., 2015; Yin et al., 2022). These studies were considered fair to good quality. The PEDro scores of the included studies were 4 (Park et al., 2015), 6 (Park, 2015), 6 (Yin et al., 2022), and 7 (Pan et al., 2019). The ESs ranged from 0.33 to 1.71, which spans a small to large effect in favor of the experimental group (Figure 2).
Two studies paired MI training with conventional occupational therapy (Park et al., 2015; Yin et al., 2022). In Park et al. (2015), patients more than 6 months post-stroke received 20 minutes of occupational therapy followed by 10 minutes of MI guided by audio recordings. Controls received dose-matched occupational therapy. The experimental group improved significantly more than controls on the Korean MBI. Yin et al. (2022) investigated MI training in hospitalized patients more than 1 month post-stroke. Participants completed 20 minutes of MI training in addition to occupational therapy, while controls received occupational therapy in isolation. The experimental group improved significantly more on the FIM at study conclusion than controls, who received occupational therapy in isolation (Yin et al., 2022).
Two studies paired MI training with treatment other than conventional therapy (Pan et al., 2019; Park, 2015). Park (2015) examined the effect of MI training paired with modified constraint-induced movement therapy (mCIMT) in patients more than 6 months post-stroke. Participants in both groups received 30 minutes of therapy five times per week. The experimental group additionally listened to 30 minute pre-recorded MI scripts directly following treatment sessions. The researchers recorded significantly greater gains on the Korean MBI in the experimental group than controls, who received mCIMT in isolation (Park, 2020). In Pan et al. (2019), hospitalized patients between 3 and 12 months post-stroke listened to pre-recorded MI scripts for 30 minutes during repetitive transcranial magnetic stimulation (rTMS). Controls listened to pre-recorded relaxation scripts while receiving rTMS. Both groups received dose-matched conventional therapy outside of sessions. The experimental group exhibited significantly greater improvements on the MBI than the controls (Pan et al., 2019).
The three good-quality studies (Pan et al., 2019; Park, 2015; Yin et al., 2022) in this group both recorded significant differences between groups, with large effects favoring the experimental group. These results suggest that MI training delivered through audio recordings improves independence in ADL when added to another intervention. However, the findings must be interpreted with caution as two studies did not control for the additional therapeutic time spent listening to the pre-recorded MI scripts (Park, 2015; Yin et al., 2022). The remaining fair-quality study (Park et al., 2015) provides some additional support for the benefits of audio-delivered MI training, although ESs were small to moderate.
Visual-guided imagery
Three studies, with a total of 130 participants delivered MI training that was primarily guided through visual information (Ji et al., 2021; Nam et al., 2019; Park, 2020). The types of visual input included videos (Nam et al., 2019), text displayed on a computer screen (Park, 2020), and photographs (Ji et al., 2021). The included studies were considered fair to good quality, with PEDro scores of 5 (Ji et al., 2021), 6 (Nam et al., 2019), and 8 (Park, 2020). The ESs ranged from 0.28 to 0.70, which spans a small to medium effect in favor of the experimental group (Figure 2).
In Park (2020), participants more than 6 months post-stroke practiced MI for 30 minutes while receiving neuromuscular triggered electrical stimulation (NMES) to the forearm of the hemiplegic upper limb. The MI training was guided by written text on a computer screen and involved imagery of sports-related upper extremity movement (e.g., throwing a baseball and swinging a tennis racket). Controls received the same amount of NMES in isolation. Both the experimental and control groups improved significantly on the MBI, with no significant differences between groups.
Ji et al. (2021) adapted a graded MI training program from complex regional pain syndrome protocols for patients with chronic stroke. The home-based program was delivered daily through a smartphone over 8 weeks. Participation was limited to individuals more than 3 months post-stroke. Each 30-minute session included three components: mental rotation of hands, MI of upper limb movements guided by photographs, and mirror therapy (Ji et al., 2021). Dose-matched physical practice of the imagined tasks served as the control intervention. While no significant differences between groups were recorded, ES calculations indicated a moderate effect on the FIM in favor of the experimental group. This study received a PEDro score of 5, indicating fair quality.
Nam et al. (2019) also delivered MI training through a smartphone. Participants in the early sub-acute phase of stroke were guided through imagery by a reversed video of themselves performing the target movement with their unaffected limb, thus creating the appearance of using their affected limb during the movement. The imagined actions were basic activities taken from two post-stroke upper limb assessments (Manual Function Test, Stroke Upper Limb Capacity Scale). Participants completed the 30-minute imagery sessions following conventional therapy, which the controls received in isolation. Results indicated no significant between-group differences on the MBI
None of the three studies recorded significant differences between the experimental and control groups on measures of ADL independence. This lack of significance in two studies of good methodological quality, with supporting evidence from one fair-quality study, suggests that MI training is not an effective intervention when delivered indirectly through a visual mode of instruction if used to target independence in ADL post-stroke.
Discussion
To our knowledge, this is the first systematic review to examine the effect of MI training post-stroke using independence in ADL as a primary outcome. The included studies used several approaches to deliver MI training, with varying results. While all studies documented the benefits of MI training on the level of assistance needed to perform ADL, only half recorded significant differences between experimental and control groups.
Between-group differences occurred in all interventions that added audio-delivered MI training to other treatments (conventional occupational therapy, TMS, mCIMT). However, these differences must be interpreted with caution. The total number of participants was relatively small, and the range of documented ESs was large (0.33–1.71). Additionally, it is not possible to rule out the placebo effect in two of the studies. While more high quality research is needed in the area, the documented differences remain promising for stroke rehabilitation. Stroke patients commonly report a desire to receive rehabilitation of higher intensity and duration than currently provided in standard care (Luker et al., 2015). Inpatients frequently perceive a lack of practice opportunities outside of supervised treatment sessions (Luker et al., 2015). MI training using audio-guided scripts offers a low risk means by which patients can engage in additional therapy without relying on the presence of others.
The present review found no evidence supporting the use of visual-guided MI training delivery to facilitate ADL independence, while evidence for therapist-directed MI training was mixed. There are a few possible reasons for this mixed evidence. The two studies that recorded between-group differences following therapist-directed training contained several unique characteristics (Liu et al., 2004, 2009). Both involved using MI as a cognitive strategy to identify and problem-solve challenges related to task performance. Liu et al. (2004) and Liu et al. (2009) were also the only studies to measure independence in IADL, and did so using a non-validated measure. Finally, participants were on average around 2 weeks post-stroke, earlier than other studies using therapist-directed training (Braun et al., 2012; Ietswaart et al., 2011).
MI training is proposed to be particularly valuable in the early stages of stroke recovery when physical function of the affected limbs is especially impaired (Sharma et al., 2006). Barclay et al. (2020) documented no relationship between the stage of stroke recovery and the effect of MI training on upper extremity outcomes. In the present review, the average time post-stroke in studies that delivered MI training through audio recordings to positive results ranged from <2 to 18 months. It is thus unclear from this review if the stage of stroke recovery impacts the effect of MI training on ADL performance, or if this effect is impacted by the mode of training instruction.
Another intervention characteristic of interest is training dosage. Any assessment of a dose-response relationship is limited as we were unable to determine the cumulative MI training dose of several interventions (Braun et al., 2012; Liu et al., 2004, 2009). While all studies that delivered MI training through audio recordings reported benefits of ADL performance, the cumulative dose of training ranged from 100 to 900 minutes. Recent reviews have documented no clear relationship between the dose of MI training and its effect on upper extremity function following stroke (Barclay et al., 2020; Gaughan and Boe, 2022). The absence of a clear relationship between MI training effectiveness and training dosage documented here is therefore in line with previous research.
All included studies aside from Liu et al. (2004) and Liu et al. (2009) measured ADL independence using a variation of either the BI or the FIM. The BI and the FIM are validated measures that involve rating the level of assistance an individual requires to perform different activities. The two measures have comparable psychometric properties for stroke patients (Schepers et al., 2006). The MBI was developed to address the perceived insensitivity of the BI (Quinn et al., 2011). While the original BI uses a two- or three-step scale to rate independence, a five-step scale is used for rating all tasks in its modified version. The MBI has been recommended for use over the original index in future stroke trials (Quinn et al., 2011).
Occupational therapy was directly mentioned in most studies. All four studies that delivered MI training through a healthcare professional involved occupational therapists in training delivery. Several studies paired MI training with conventional occupational therapy, including three studies that used audio recordings as their mode of instruction. Several other studies paired training with general conventional therapy that likely involved occupational therapy or interventions within the profession’s scope, such as CIMT. This prominence of occupational therapy within the reviewed literature highlights the potential relevance of MI training to the profession’s established role in stroke rehabilitation.
A key component of occupational therapy’s role is enabling patient participation in meaningful activities (Steultjens et al., 2003). As ADL are viewed by many stroke survivors as meaningful, independence in ADL is a relevant outcome measure for occupational therapists (Eriksson and Tham, 2010). For some stroke survivors, independence in ADL is valuable because it facilitates participation in other meaningful activities related to work, leisure, or social-related roles (Wood et al., 2010). Other survivors may view ADL as meaningful in and of themselves, with increased independence in these activities providing a sense of autonomy (Wood et al., 2010).
This review indicates the need for greater methodological rigor in studies that investigate MI training as a treatment for ADL independence. Blinding of participants and therapists is often challenging to accomplish in rehabilitation trials (Santaguida et al., 2012). However, challenges in meeting such criteria renders the blinding of assessors especially important to the study’s internal validity. While comprehensive blinding is difficult to accomplish in rehabilitation trials, concealed allocation and intention-to-treat analysis are comparatively straightforward to implement. Concealed allocation, which prevents selection and confounding biases, was not discussed in 8 of the 13 studies. This result is in line with previous findings that concealed allocation commonly goes unreported in stroke rehabilitation (Santaguida et al., 2012). Intention-to-treat analysis is not required when all participants receive the treatment as assigned. Providing information on treatment compliance, and statistical measures taken if such compliance is lacking, is essential to confidence in the reported results.
Limitations and future studies
The current review has several limitations. While the included studies come from a diverse range of countries, we did restrict articles to those published in English. This restriction was applied at the start of the literature search, and therefore we cannot be certain how many articles were excluded that otherwise met the review’s eligibility criteria. Second, our definition of an ADL outcome measure was reached through a joint discussion of three practicing occupational therapists and consultation with the literature. However, some may argue that our chosen definition is overly conservative and led to the unnecessary exclusion of relevant articles. For example, several excluded studies used the Motor Activity Log (MAL) as an outcome measure. In the MAL, participants post-stroke rate the use of their affected arm in the context of ADL along two scales: amount of use and quality of movement (van der Lee et al., 2004). While ADL serve as the assessment context, neither scale specifically focuses on participant independence in the target activities. We thus excluded the MAL as an outcome measure. The high heterogeneity of the included studies limits our ability to determine critical factors of successful MI training interventions. Finally, the categorization of studies based on modes of MI instruction provided additional value to this review but led to the exclusion of two lower-quality studies in the interpretation of findings. These two studies met inclusion criteria but lacked essential information about their respective training programs.
Future studies that use audio-guided training should consider incorporating a placebo treatment such as pre-recorded relaxation scripts into the control intervention to increase confidence in the effects of MI training. We also recommend that future studies include replicable MI training protocols to facilitate comparison between otherwise similarly described studies.
Conclusion
This review examined the effect of MI training on ADL independence following stroke. Audio-based MI training consistently increased independence in ADL when paired with other rehabilitation methods. The lack of supervision required for such training could provide patients with additional therapeutic activity outside supervised treatment sessions. Findings were inconsistent for MI training delivered directly by a therapist. Treatment dosage and stage of stroke recovery did not affect training effectiveness. The small number of participants included in most reviewed studies indicates a need for further research into MI training’s effectiveness in the post-stroke population. We hope that the potential benefits documented in this review, together with methodological considerations for improving the quality of evidence, will encourage further development of MI training protocols for implementation in occupational therapy practice.
Key findings
MI training delivered through audio recordings appears to facilitate ADL independence
High heterogeneity in interventions limits the ability to draw conclusions on effective treatment characteristics.
What the study has added
We examined the effects of MI training on ADL post-stroke. Findings support audio-based training as an effective adjutant tool, with more research required for therapist-delivered training.
Footnotes
Research ethics
This is a review study, and no ethical approval is required.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, patient and public involvement in the research was: Not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Contributorship
All authors researched literature and conducted screening and reviewing of the articles. CH, JH, and CM drafted the original manuscript. KL led the interpretation of study results, carried out manuscript revisions with NB, and wrote the final manuscript. AL reviewed the search results, edited the manuscript, wrote the summary of the manuscript, and made recommendations to improve the manuscript.