
Abstract
Introduction
Engaging with risk is a certain and unavoidable part of occupational therapy. Intermediate care services are mostly accessed by older people with complex needs, yet little is known in the literature about the extent, type and nature of risk involved in these services.
Method
A scoping review was systematically conducted to map the common areas of risk (risk domains) from an occupational therapy perspective. Thematic analysis was conducted in order to identify the risk characteristics related to the literature reviewed.
Results
25 journal articles were identified and arranged into 10 risk domains: Falls, discharge, practice errors, activities of daily living, pressure care, frailty management, patient handling, loneliness, nutritional care and language barriers. Three risk characteristics were identified: (1) Risk awareness and identifying risk, (2) decision-making under risk and (3) improving safety.
Conclusion
Occupational therapists play a diverse role in migrating risk for older people which is not fully explored beyond addressing deficits in functional ability and hazardous environments. The process of how risk is controlled and reconciled with occupation and how positive risk-taking is facilitated are implicit and not directly addressed within the literature reviewed. The findings reveal gaps in knowledge and provide a foundation for further research.
Introduction
Intermediate care is a short term intervention that occurs between primary and secondary care and is mainly accessed by older adults with complex needs. It is internationally recognised as a healthcare model and is predominantly focused on maintaining a person’s independence in their home by avoiding unnecessary hospital admissions and premature residential care (NHS Benchmarking Network, 2017). Intermediate care can include inpatient facilities which offer rehabilitation and convalescence as a step to transitioning to home or other care arrangements. As part of its provision, it prevents and reduces risks, errors and harm as part of patient safety. Patient safety is a healthcare discipline that is concerned with services provided during the provision of healthcare (NHS, 2021). Post such provision requires the management of risk through an occupational therapy risk enablement plan so that a person can carry out and benefit from their activities safely (RCOT, 2017).
Risks are normally associated with harm and whether considered or unconsidered they are everywhere; at home, at work and in both activity and inactivity (Carson and Brain, 2008). Morgan (2004 p. 18) defines risk as ‘the likelihood of an event happening with potentially beneficial or harmful outcomes for self and others’, thus emphasising both positive and negative aspects of risk-taking. In occupational therapy, negotiating the safest approach to risk-taking is an intrinsic part of a service user’s progress (RCOT, 2017).
Determining the nature of a risk and the opportunity it may or may not present is a cognitive process which includes subjective viewpoints (Gallagher, 2013; Breakwell, 2007). These cognitive processes also include some less obvious psychological factors which are related to how we make judgements in conditions of uncertainty, namely, the effect of heuristics and biases (Breakwell, 2007; Trimpop, 1994). Clinical and professional reasoning involves making judgements on risk-prone situations and occupational therapists use informal theories and tacit knowledge in their decision-making (Carrier et al., 2010). Heuristics can provide a mental shortcut to problem-solving, thereby reducing cognitive burden, but it can also lead to unhelpful bias like risk avoidance which can encroach on the ethical principles of autonomy, beneficence, non-maleficence and justice (Carson and Brain, 2008; Schell and Schell, 2008). There is a duty of care to support clients to take measured risks in occupational therapy (RCOT, 2017), this is sometimes clouded by fears of accountability and blame (Morgan, 2004). Carson and Brain (2008) contends that failing to support risk-taking can lead to serious consequences for those receiving care and avoiding risk-taking where there is a duty of care is not a guaranteed way to avoiding a harmful outcome or liability.
Effective risk management is achieved as a result of, and attention to, its preceding factors, which commonly include awareness, identification, assessment, action, communication and review to ensure harmful risk is minimised and positive therapeutic benefits are enhanced (Gallagher, 2013; Haxby et al., 2011; RCOT, 2017). The risk management process becomes particularly challenging when those with complex needs transition between higher dependency care to lower dependency care arrangements or where higher dependency care can be avoided in favour of more suitable support (National Institute for Health and Care Excellence, 2017). Additionally, the therapeutic use of risk is subject to client agreement and those that have mental capacity can choose their level of compliance or refuse such interventions which mitigate risk. Engaging in activity that presents a significant risk of harm where risk cannot be reduced to a reasonable level also presents complexity for occupational therapists. As such, refusing to support such an activity can be appropriate providing a person is made aware of all the risks and the activity is made as safe as possible. Making decisions like these is also subject to determining a client’s mental capacity and where there is a belief that capacity is lacking, risk-taking should be approached on a decision per decision basis and proportional to the level of understanding of the service user (RCOT, 2017). Such challenges are commonplace in intermediate care delivery.
In the United Kingdom, intermediate care and reablement provision are divided between home-based, reablement, bed-based and crisis-response services (National Institute for Health and Care Excellence, 2017). These services are accessed mostly by older people aged between 79 and 90 years (NHS Benchmarking Network, 2017). Demand for intermediate care is increasing as the 85+ age group is the UK’s fastest growing population and is set to double to 3.2 million by mid-2041 and treble by 2066 (NHS Benchmarking Network, 2017; ONS, 2018). As age increases, so does the likelihood of incurable long-term illness such as diabetes, cardiovascular and chronic respiratory disease (Wright et al., 2017) and ill health arising from multi-morbidity, frailty, dementia, malnutrition, falls and hip fractures, mental health problems, sensory loss, loneliness and social isolation (Age UK, 2019). These considerations together with a multitude of extrinsic factors (e.g. resource availability) require complex decision-making under risk to enable safe risk-taking. In intermediate care, positive risk-taking has become a prominent risk contingency principle. Positive risk-taking is ‘…balancing the positive benefits gained from taking risks against the negative effects of attempting to avoid risk altogether’ (National Institute for Health and Care Excellence, 2017, p. 17).
Health and wellbeing involves more than just the absence of disease. Occupation is a contributing factor to wellness and is fundamental to how people realise aspirations, satisfy needs and cope with the environment (Wilcock, 1993). Mcintyre and Atwal (2005) contend that occupational therapists evaluate and assess multiple pathologies in old age together with social, psychological, spiritual and cultural factors, which present profession-specific challenges. Risks in intermediate care are complex and heterogeneous and the literature from an occupational therapy standpoint is limited. The purpose of this scoping review is to identify studies conducted in intermediate care settings which relate to occupational therapy risk management in order to pool the available research and map key concepts. This scoping review aims to 1. identify the common areas of risk in intermediate care from an occupational therapy perspective; 2. provide insight into these common areas of risk (risk domains) by establishing their volume and scope from the available research and 3. identify the nature and characteristics of the risks in the research reviewed.
Method
A scoping review was conducted in order to meet the study aims and to map the key concepts in this area, including the main types and sources of evidence available (Arksey and O’malley, 2005). The framework, in accordance with the recommendations by Arksey and O’malley (2005), was implemented using the guidance of the Joanna Briggs Institute of Applied Health Sciences and McMaster University, manual for scoping reviews. This framework and guidance assisted in identifying the research question, identifying relevant literature, study selection, charting the data, and collating, summarising and reporting results.
Identifying the research question
The research question was developed by preliminary database searching and the initial reading of relevant literature. The research question was constructed using a collaborative process between the authors and identified as: What are the common areas of risk and their characteristics found in intermediate care from an occupational therapy perspective?
Identifying the relevant literature
Search terms.
W2 and W3 = word proximity to adjacent word.
Study selection
All records identified from the databases were uploaded to EndNote X9 and duplicates were removed. To be included, articles must have originated from at least one post-registered occupational therapists’ perspective, be within the remit and/or definition of intermediate care and include an aspect of risk management. These perspectives included clinical and professional reasoning/decision-making, opinion, perceptions and reflections. The National Institute for Health and Care Excellence (2017) core guidelines, the National Audit of Intermediate Care (2019) and Grant et al. (2007) provided intermediate care definitions. Risk terminology was identified in the Royal College of Occupational Therapists, ‘Embracing risk, Enabling choice’; Department of Health’s, ‘Best Practice in Managing Risk’ and ‘Independence, choice and risk: a guide to best practice in supported decision making’ guidance (DOH, 2007; DOH, 2009; RCOT, 2017). A decision tree (Appendix 1) was developed for the purposes of applying criterion. Duplicate EndNote files were created for two authors to screen the titles and abstracts independently. The results from each of the reviewers’ screening were combined into one EndNote file and the first author completed a full text review of each study. Meetings between the reviewing authors were held to resolve screening discrepancies; three areas of exclusion were applied, as shown in Figure 1. The studies that were subject to screening discrepancies and/or required further review for inclusion or exclusion were screened by full text by the authors independently before agreeing on exclusion. Studies that did not meet these criteria or were associated solely with primary acute care discharge were excluded; however, studies that did not specify the exact discharge setting and/or included both acute care and rehabilitation occupational therapy perspectives were included. Studies were included where occupational therapists were part of multi-professional groups of participants. Studies from the perspective of occupational therapy assistants or students were only included where all the other inclusion criteria had been met. Additionally, studies were not excluded based on whether a person had a particular condition, such as stroke or dementia and/or their particular circumstances that is, prison, temporary or residential accommodation, as per Sec. 1.3.2 of the National Institute for Health and Care Excellence (2017) intermediate care core principles. The article selection process using the PRISMA flow chart (Moher et al., 2009).
Assessment of methodological quality
Study summary.
Charting the data
Included studies were organised in Microsoft Excel and the data were extracted and charted as shown in Table 2 (Joanna, 2020). The first author completed and organised the data in the following categories: • Risk domain; • Author/year; • Methodology/publication description; • Study purpose; • Location/sample; • Key findings and • Limitations (reported).
Collating, summarising and reporting results
Content analysis of all eligible studies was conducted in two stages by the first author: a descriptive analytical approach to establish frequencies followed by thematic analysis to identify themes and patterns systematically (Braun and Clarke, 2006). This method facilitated the creation of risk domains and study categorisation therein, risk domain frequency and a summary of the risk characteristics in relation to the identified risk domains. Deciding upon the risk domain categories was achieved after a full text review of each study and team meetings to help refine the risk domain criteria. Risk characteristics were identified by the first author through thematic analysis of the results, findings and discussion sections of included studies to generate descriptive codes. These codes were stored and organised in QSR International NVivo 12. Theme generation was achieved by a collaborative process between all authors before deciding upon the risk characteristics to be reported (Braun and Clarke, 2006).
Results
The database searches identified 2878 hits. After duplicates had been removed, 1862 were screened by title and abstract. A further 1820 were excluded which left a full text review of 42 studies, where 17 studies were excluded. No further studies were identified during a search of the reference lists of included studies. Three studies were unavailable resulting in 25 studies being included in this review. The search process is shown in Figure 1. All included studies were published between 2000 and 2019 and ten (60%) were published within the last 10 years. Of the included studies, 11 used qualitative study designs, eight used quantitative methods, three were literature reviews, two were mixed methods studies and one Delphi study.
Assessment of methodological quality
The qualitative studies reviewed were diverse and used a variety of study designs, including grounded theory, phenomenology and secondary data analysis. The prominent data collection methods were semi-structured interview and focus group. Four main areas presented a quality concern: those were the sampling methods used, the role of researcher, decision trial auditability and trustworthiness. The sampling methods was often not described in detail and were in most cases not related to sampling redundancy; however, it was noted that achieving data saturation in relation to recruiting a sample with flexibility may not have been an objective for these studies. The role of researcher was often overlooked in respect of their level of participation and expertise. Regarding auditability concerns, decision-making trails relating to how codes of data were identified and how they were transformed into themes was not reported in detail. The four components of trustworthiness, those being credibility, transferability, dependability and confirmability were not all addressed in the majority of the studies reviewed.
The quantitative studies reviewed used three prominent study designs, those being, cross-sectional, cohort and evaluative. The quality assessment of these studies alluded to potential deficiencies in three areas, which were the sample size justification, the reliability and validity of outcome measures and the methods used in data analysis. None of the studies appraised were interventional, therefore, some of the critical appraisal tool used was not applicable. Regarding the sampling method, the sample size was not justified for the studies employing inferential statistical analysis, possible selection bias was not reported, groups were not equal in size and the sample was often not described in detail. Outcome measures were not reported in terms of their empirical validity and reliability and some studies omitted whether they used a pilot study or employed a screening process to determine whether their outcome measures or psychometric scales were reliable and valid. Additionally, the rationale for using statistical testing was rarely described and most studies reported limitations to the generalisability of their findings.
Additionally, the remaining studies, mixed method (n=2) and a Delphi study also presented quality concerns in the sampling method reported. One out of the three literature reviews in this study used systematic methods and these studies ranged from 2003 to 2010 which may bring concern to their current clinical relevance in relation to this study’s research objectives. The quality assessment summary of the quantitative and qualitative studies can be seen in Appendix 2.
Risk domains
With regard to the Research Aims 1 and 2, the risk domain frequencies are Falls (n=9), discharge (n=5), practice errors (n=3), activities of daily living (n=2), pressure care (n=1), frailty management (n=1), patient handling (n=1), loneliness (n=1), nutritional care (n=1) and language barriers (n=1) as shown in Figure 2. The studies that relate to falls (36%), discharge (20%) and practice errors (12%) represent the highest frequency of risk domains and contribute to 68% of the total studies included in this review. Risk domain frequencies.
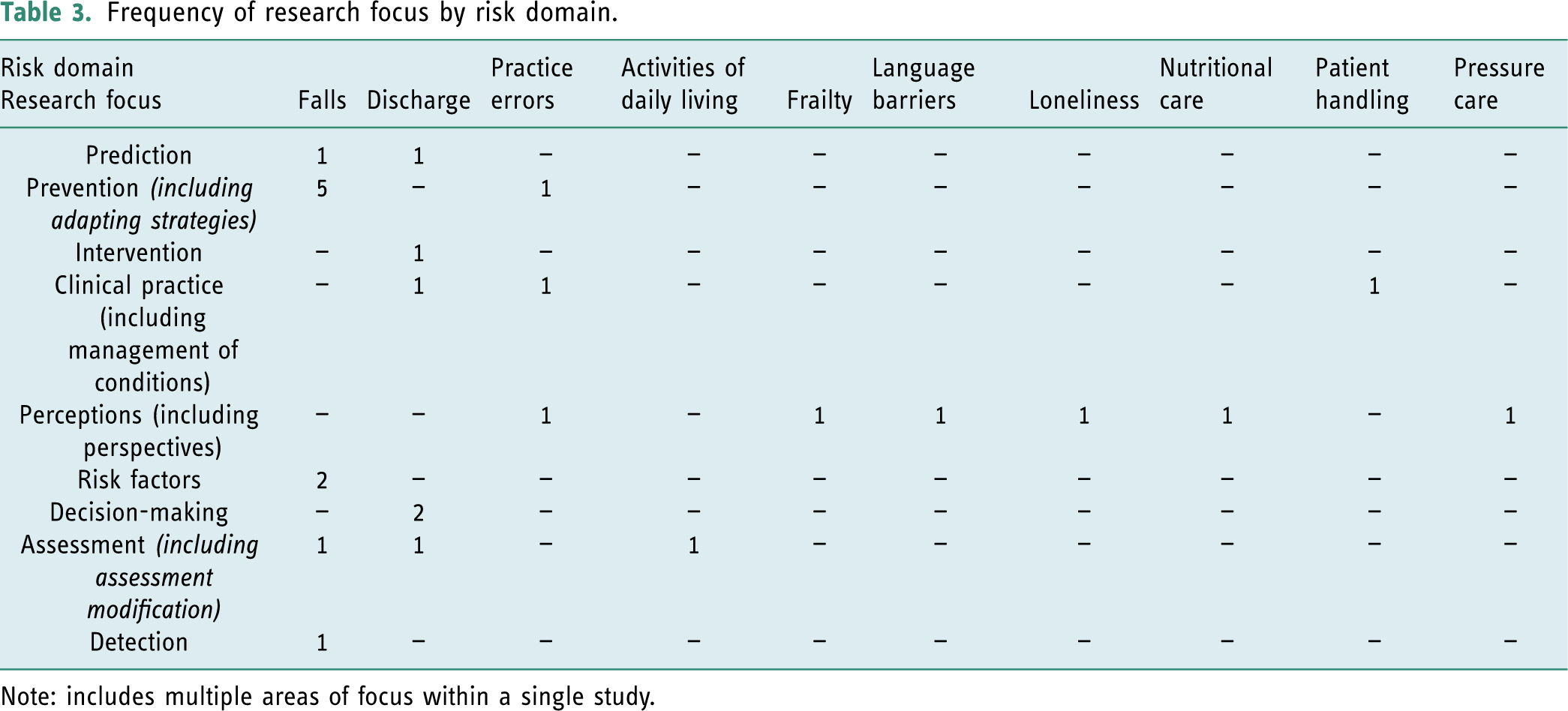
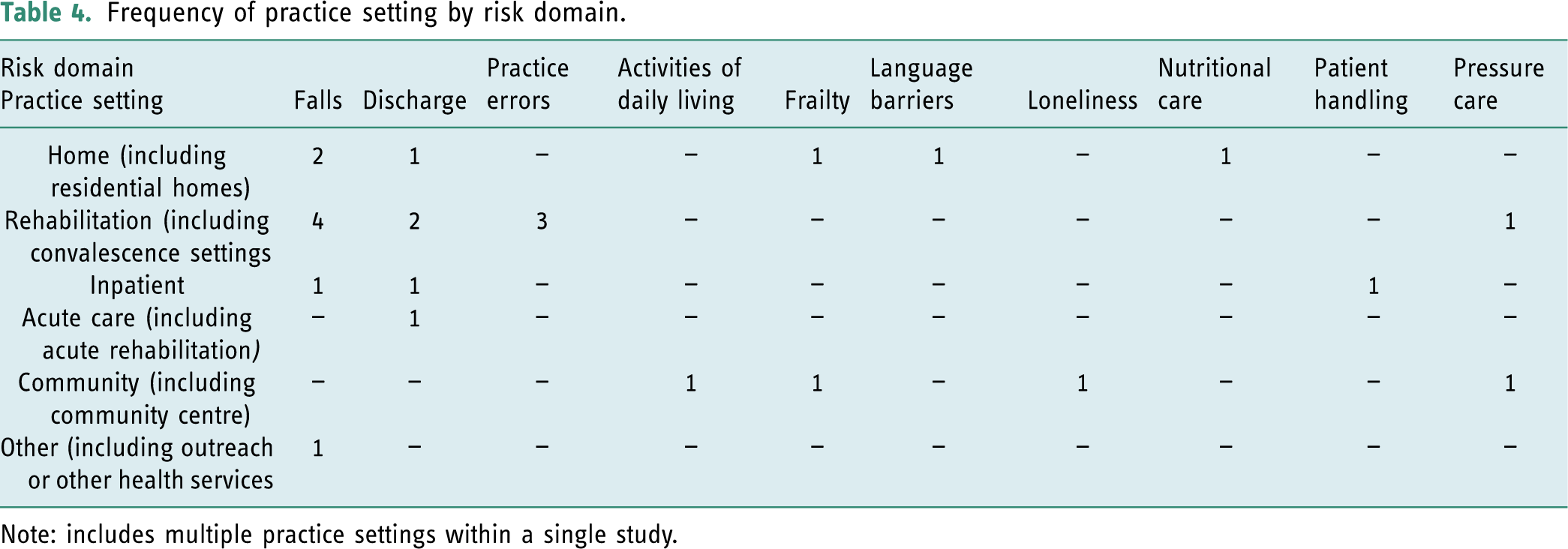
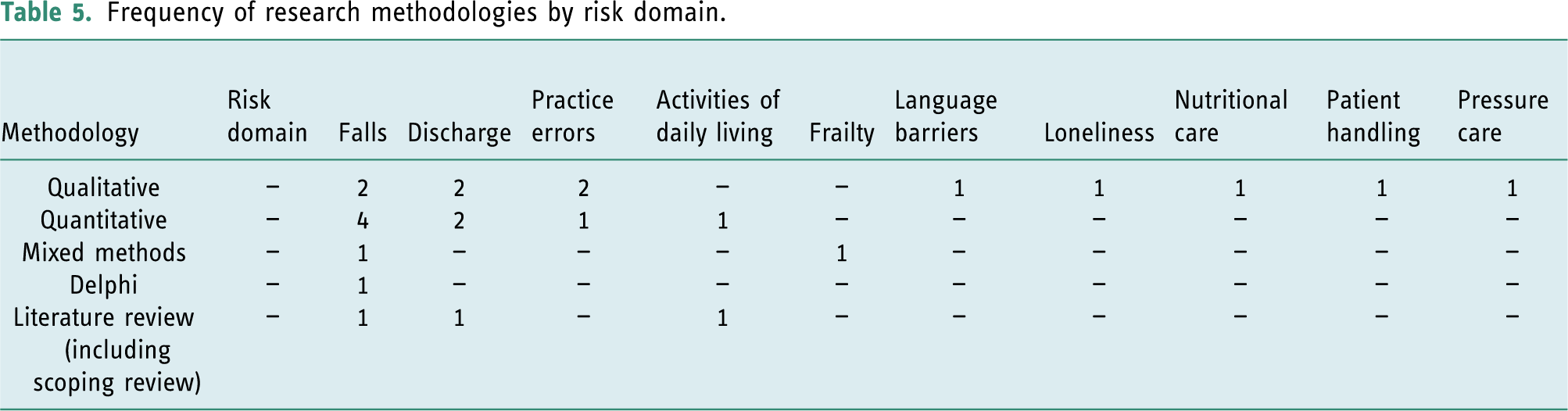
Examination of the nature and scope (Aim 2) of the risk domains was conducted to identify the research methodologies, practice settings and the focus of the research within each risk domain, as presented on Tables 3–5. In describing the common areas of risk as risk domains, three main areas of ambiguity were identified and resolved: • The ‘Discharge’ risk domain included those studies that focused on home visits prior to discharge. All home visits were initiated in the context of discharge; therefore, discharge became the area of risk and was categorised as the risk domain. • The ‘Activities of daily living’ risk domain incorporated those studies which focused on assessments, interventions and the clinical reasoning of occupational therapists in determining ability during activities necessary to remain independent, safe and to live at home. • Where multiple risk domains were identified, the aim(s) and primary focus of the study became the over-riding factor in risk domain determination. Frequency of research focus by risk domain. Note: includes multiple areas of focus within a single study. Frequency of practice setting by risk domain. Note: includes multiple practice settings within a single study. Frequency of research methodologies by risk domain.
Risk characteristics
To address Aims 2 and 3, prominent themes, and features of risk from the reviewed literature were categorised as risk characteristics. Three risk characteristics were identified: (1) Risk awareness and identifying risk, (2) decision-making under risk and (3) Improving safety.
Risk awareness and identifying risk
Risk awareness may be defined as the acknowledgement of a condition, disability, disease, patient safety issue or a risk-prone situation that when unaddressed has the potential to cause harm. Risk identification includes best practice methods for identifying risk and/or risk factors that present safety issues or inhibit wellbeing.
Ruchinskas et al. (2001) emphasised the importance of identifying known fall risk factors to support accurate fall prediction and found cueing helped predictive accuracy and participants’ ability to identify ‘history of falls’ but not ‘advancing age’ risk factors. Ruchinskas (2003) found therapists demonstrated some predicative capability for falls, however not exceeding that of using two major predictors: ‘falls history’ and ‘presence of a neurological condition’. In contrast, Pighills et al. (2019) surveyed occupational therapists and found the majority agreed that people at a high risk of falls include those with a history of falls, visual impairment, those who are aged, have co-morbidities or had had a recent hospital visit.
Several studies have focussed on identifying and mitigating risk factors. Buri et al. (2000) found perceptual dysfunction was related to falls in older people with cognitive impairment and spatial disorientation was the most important perceptual risk factor. Xu et al. (2019) sought to adapt a falls’ prevention program for stroke survivors as they have condition-specific risk factors for falling which include hypertension medications, neurological visual disorder and post-stroke depression. Occupational therapists understand and routinely ask about pressure care needs (Mole et al., 2019) and use a client-centred approach to identify and address such issues (Rose and Mackenzie, 2010). They perceive loneliness as a psychosocial risk factor associated with higher risk of developing poor health outcomes, epitomised by social isolation, depression and physical deconditioning, lack of self-care and falls (Chana et al., 2016). Bathing for adults with physical disabilities is seen as a potential risk owing to hard, sharp surfaces and the presence of water and occupational therapists ranked the most important assessment and solution considerations as mobility, client priorities, safety factors, medical diagnosis and the availability of bathing equipment (Gooch, 2003).
Studies investigating home visits as an intervention during discharge have focused on client mobility and functional deficits, unsafe environments and risk-prone situations. Nygård et al. (2004) found that occupational therapists associate client problems during discharge home visits with inadequacies in motor, cognitive and psychological capacity and environmental hazards. Davis Aisling and Mc Clure (2019) identified home visits as potentially unsafe areas of practice for therapists, sometimes involving lone working or dangerous social situations and hazardous environments.
Best practice methods for equipment selection for safe patient handling was associated with the awareness of physical, behavioural, cognitive and perceptual characteristics of each patient, the equipment’s features, suitability and the environmental demand (Darragh et al., 2013). Barriers that inhibit patient safety and cause practice errors were investigated by Scheirton et al. (2003), Mu et al. (2011) and Corrado et al. (2014). Scheirton et al. (2003) and Mu et al. (2011) findings suggest occupational therapists consider that practice errors arise from individual and organisational failings. Corrado et al. (2014) found poor maintenance of equipment, unsuitable private therapy areas, medication errors, unrealistic time scales for services to communicate, confusion over role, inadequate organisation of workload and lack of uniformity in rehabilitation tools caused latent risk factors in organisations and their systems.
Decision-making under risk
Risk characteristics of ‘decision-making under risk’ refer to studies that include one or more risk judgements in prevention strategies, assessments, predictions and interventions to manage risk and/or delineate the clinical reasoning in decision-making.
Clinical reasoning has been found to incorporate many perspectives including using clinical experience and learning through error. Carrier et al. (2010) asserted that decision-making components used by community occupational therapists include interactive decision-making, quick formation of solutions prior to comprehensive reasoning and dimensions of clinical reasoning used simultaneously. Additionally, integrating tacit knowledge with formal knowledge were features of this decision-making influenced by internal (personal context) and external (practice context) factors. Rose and Mackenzie (2010) found that clinical reasoning in occupational therapy pressure care was multifactorial involving client diagnosis, prognosis and collaboration. Additionally, the volume of the products, cost, equipment needs and their impact were also part of the decision-making process that often led to ‘compromise’ and ‘trial and error’ methods. In assessing for frailty, Roland et al. (2011) established that therapists would look for signs of poor judgement, impaired decision-making, limited physical function and cognitive ability to recognise and articulate needs. In the over 65 age group risk, Kinn and Galloway (2000) contend the likelihood of injury increases for those who cannot rise after a fall and found clinical experience to teach clients how to rise was the only reported method used to mitigate this risk. Scheirton et al. (2003) found learning through error was considered a valued learning experience in their study of occupational therapists’ responses to practice errors.
Deficiencies in organisational processes and approaches to therapy were found to influence decision-making under risk. Mole et al. (2019) identified that organisational failings and therapist inadequacies can affect nutritional care, specifically limited time, nutritional knowledge and financial pressure to replace carers with meal delivery support. Corrado et al. (2014) found practice errors relating to wrong dose, treatment planning and functional assessment were the most frequently reported, and organisational, bureaucratic and administrative factors were important considerations in clinical risk management.
Differing approaches to assessment were seen to influence decisions relating to risk-prone activities. Gooch (2003) found assessing bathing in adults with physical disabilities was inconsistent and not always conducive with best practice methods for determining functional ability. Telephone assessments were more frequently reported than the use of standardised assessments and over half reported using their own assessment methods and when face-to-face assessment took place it was mostly conducted without water.
Enhancing standardised methods in order to improve decision-making under risk was considered in the studies by Xu et al. (2019) and Hasegawa and Kamimura (2018), where adapting fall assessment and prevention programmes were brought more in line with the client group, culture and environmental demands. Pighills et al. (2019) found environmental home assessments and modifications for falls were affected by therapists’ confidence in and awareness of guidance, key stakeholder support, misunderstanding the value of occupational therapy, financial implications and time to complete modifications and administration. Risk prediction is an inevitable component of risk management and identifying those who may fall with a degree of predictive accuracy in the over 60 age group was found to be difficult (Ruchinskas, 2003). In contrast, Simning et al. (2019) found the predictions of the occupational and physiotherapists were veridical with discharge outcomes in older adults transitioning to home.
Ethical considerations, client-centred decision-making and client behaviour were found to be factors in mitigating risk. Following up on recommendations to review compliance to interventions and adopting a client-centred approach were found to be important components in attempting to prevent falls for those older adults living alone (Woodland and Hobson, 2003). Moats and Doble (2006) found an association between risk-taking and client-centred practice as clinical decision-making is often guided by autonomy promotion and accepting the risk a client is prepared to take. Their findings suggest autonomy promotion is subject to conflicting ethical principles, the fear of risk-taking repercussions, socio-political values, service traditions, prejudice and/or economic directives that support risk avoidance. These factors were identified to sometimes lead to inappropriate methods of care involving persuasion, coercion and intimidation (Moats, 2007). Additionally, the findings of Nygård et al. (2004) suggest a client-centred approach is tested when a client’s behaviour increases risk and Moats and Doble (2006) found client centeredness is often abandoned when clients place themselves in danger.
Systemic organisational factors were found to influence decisions and behaviours relating to risk-prone situations. Squires et al. (2019) found preventing the miscommunication of risk in the use of interpreter services engendered proactive decisions relating to the organisation of workload to ensure harm did not result from inaccurate interpretation. Chana et al. (2016) found intermediate team members considered ‘loneliness’ a relevant issue; however, managing loneliness was a low priority within the intermediate care service caused by a propensity to work only towards symptoms and functions within a traditional medical model.
Improving safety
The ‘improving safety’ risk characteristic includes recommendations for improving risk-prone areas of practice, adaptation or modification of therapeutic tools, removal of barriers inhibiting safety, research development and organisational factors not conducive with safe practice.
Improving falls research, education, clinical supervision, and prevention programmes were seen as necessary to increase the uptake in programme participation, mitigate risk and to sustain services. Olij et al. (2017) reported the need to remove financial barriers and improve healthcare counselling and national health education. Pighills et al. (2019) called for better access to peer support and collaboration with key stakeholders. In recognition of increasing healthcare costs, Xu et al. (2019) contend that group-based falls-prevention interventions for stroke survivors such as ‘Stepping On’ could improve cost effectiveness. Hasegawa and Kamimura (2018) developed a Japanese version of the Westmead Home Safety Assessment to prevent falls in older adults and identified further research was required to improve its reliability and validity. Ruchinskas et al. (2001) and Ruchinskas (2003) contend staff education on empirically supported risk factors for falls may reduce the potential for error and improve decision-making and patient care. Kinn and Galloway (2000) found nearly half of therapists did not teach older persons how to rise from the floor after a fall. Recommendations for improvement included more teaching at undergraduate level and clinical supervision.
Factors identified to improve discharge planning and home visits included systemic organisational change, collaboration and communication between key stakeholders and client centeredness approaches. Davis Aisling and Mc Clure (2019) proposed additional time to complete visits, standardised checklists for hazard identification, further policy guidance, better transport options, occupational therapy assistant support, administrative resources and collaboration between community services and multi-disciplinary teams. Nygård et al. (2004) recommended service improvements for discharging inpatient older adults in line with their findings, which concluded the client’s wellbeing can be affected by too many workers visiting them, the adoption of follow-up visits and better communication in providing care and ordering equipment.
Alleviating inhibitive workloads and removing barriers preventing best practice, improving working relationships, assessment tools, education and research were identified in many of the studies reviewed. Roland et al. (2011) found that ameliorating the effects of a therapist’s workload could potentially improve frailty detection amongst at risk populations, facilitate prevention contingencies and response to acute cases. Squires et al. (2019) found a consensus amongst their participants that supporting clinicians to manage non-English speaking patients would potentially improve outcomes and quality of care. Chana et al. (2016) recommended improving the detection and management of loneliness within intermediate care services by addressing the following barriers: high workloads, unsatisfactory referral systems and lack of close working with social care and independent sector services. Additionally, bringing reliable brief assessments into practice, training on detecting and managing loneliness and improving working relations with key stakeholders were seen as necessary for improving services. Corrado et al. (2014) and Mu et al. (2011) recommended focusing on and advocating for systemic change which would help reduce practice errors and improve patient safety. Scheirton et al. (2003) recommended future occupational therapy research should target, explore and develop specific strategies to prevent and reduce practice errors.
Mole et al. (2019) proposed improvements in the detection and management of nutritional care including developing training aids, education on identifying nutritional risk and helping families make appropriate meal choices to prevent malnutrition. Rose and Mackenzie (2010) suggested further and clearer guidance on the occupational therapy role in pressure care for undergraduate educators and service managers to educate students and existing practitioners. Darragh et al. (2013) recommended further research relating to the development of equipment designed for therapeutic activity is crucial for therapist and client safety. Gooch (2003) found further investigation was required to determine the safety considerations for adults with physical disabilities bathing and what risk factors should be considered by occupational therapists.
Discussion
The purpose of this scoping review was to identify the common areas of risk and their characteristics in intermediate care from an occupational therapy perspective. Twenty-five articles were reviewed comprising a range of study designs and methodological approaches. The common areas of risk have been described as risk domains and three prominent risk characteristics have been identified from the literature reviewed. In terms of methodological quality, there were some areas where quality assessment items were not reported across many or all included studies. However, all studies were found to have relevant and meaningful conclusions and, therefore, worthy of attention and significant to this study.
‘Falls’, ‘Discharge’ and ‘Practice errors’ were the most prominent risk domains accounting for seventeen (68%) of the studies reviewed, and the remaining eight studies accounted for seven risk domains (see Figure 2). There is an absence of studies that focus on the components of risk management particularly outside of the ‘Falls’ and ‘Discharge’ risk domains (see Table 3), and ‘Rehabilitation’ settings followed by ‘Home’ and ‘Community’ were the most common research locations (see Table 4). The majority of research reviewed was qualitative in nature or used descriptive quantitative survey designs (see Table 5). However, many of these studies were not about risk itself but sought to understand therapists’ perspectives of a particular area of practice that is synonymous with risk. The focus of these studies was establishing conceptual perspectives, working practices, barriers to providing care and the occupational therapy role and did not explicitly focus on how risk was mitigated in these risk domains.
The most common risk domain was ‘Falls’ accounting for nine studies and many risk characteristics in this review. This reflects falls being the major cause of disability and mortality in older people in the UK (DOH, 2001). Older adult fall prevention is complex with over 400 risk factors for falls. The risk of falling appears to increase with the number of risk factors and this requires multifactorial risk assessments across different healthcare professionals to target interventions to mitigate fall risk factors (National Institute for Health and Care Excellence, 2015). The methods of fall prevention and management in the ‘Falls’ risk domain concentrated primarily on physical, psychosocial and environmental factors and the effect on occupation was not fully explored. Woodland and Hobson (2003) found occupational therapy was underrepresented in falls literature and there was a clear gap in knowledge regarding the role that occupational therapy plays in older adults fall prevention. The role of occupational therapists working with older adults to prevent and manage falls is not exclusive to those working in specialist falls services as ‘person’, ‘environment’ and ‘occupation’ considerations align with intrinsic (personal), extrinsic (environment) and behavioural (occupation) fall risk factors (RCOT, 2020). The process of how falls risk factors are reconciled with occupational routines in intermediate care remains unclear from the literature reviewed.
The ‘Discharge’ risk domain included five studies that support discharge planning as multifactorial and subject to risk. Older adults are likely to have or develop multi-morbidity which is known to increase the likelihood of hospital admission and re-admission (Age UK, 2019) and intermediate care is essential to facilitate timely and safe discharge (NHS Benchmarking Network, 2017). Nygård et al. (2004) and Davis Aisling and Mc Clure (2019) assert home visits during discharge planning are important for identifying risk associated with problems related to a client’s physical, cognitive and psychological capacity in addition to assessing their environment for hazards. In contrast, Nygård et al. (2004) found occupational therapy interventions predominantly focus on ameliorating the effect of physical impairment by prescribing assistive equipment or environmental adaptations. Moats and Doble (2006) and Moats (2007) contend discharge planning during home visits often involves autonomy versus safety considerations in balance with professional objectives, support and resource availability and the concerns of family and carers. Whilst this review has provided insight into the styles of reasoning that factor into decision-making under risk, there is a lack of information relating to how the severity, impact and likelihood of risk is assessed to safely facilitate discharge and promote independence.
Making judgements on risk to prevent or reduce the likelihood of practice errors introduces another perspective in risk management. The focus of many studies in relation to mitigating harmful risk concentrates on therapeutic activity; however, three studies catagorised in the ‘Practice error’ risk domain explore causational factors beyond that of the individual (Scheirton et al., 2003; Mu et al., 2011; Corrado et al., 2014). Organisational risk factors can be localised or systemic and they can also impact service users disproportionately. They can relate to all aspects of an organisation including policies, procedures, the actions of staff, management of resources and the availability and provision of assistive equipment (Mu et al., 2011; RCOT, 2017). These risk factors can be latent and less obvious (Corrado et al., 2014) and their potential effect cannot be overlooked or considered beyond any responsibility to take action to mitigate their potential harm. Practice errors can cause emotional responses as they are seen against professional standards (Scheirton et al., 2003); however, their inevitability also provide opportunities to improve services. Open and honest reporting will facilitate learning through error and support of a ‘whole system’ approach to mitigate their future occurrence (Scheirton et al., 2003; RCOT, 2017).
Risk awareness and identifying risk is the first step in the risk management process. Haxby et al. (2011) assert risk awareness means that individuals and organisations can potentially prevent practice errors from causing harm to patients. Likewise, identifying risk relating to clinical, operational and financial processes is fundamental in risk management and to creating sustainable, safe and effective healthcare (Haxby et al., 2011). Making decisions under risk sometimes requires using contradictory or incomplete information making the determination of risk factors difficult. Risks are quite often viewed as socially constructed and determining the likelihood and severity of any potential event is dependent on subjective viewpoints which are influenced by many factors including heuristics and biases (Breakwell, 2007). The result of such influences can act against effective decision-making and quality of care. Many factors to reduce harmful risk, support decision-making and improve the quality of care are evident in the ‘Improving safety’ section of this review; however, education and training are prominent themes which can support decision-making under risk, improve risk management skills and help create a risk enablement culture (RCOT, 2017).
Despite the scope of risk characteristics identified, the methods of how occupational therapists assess the severity and likelihood of risk, communicate it and evaluate any outcomes from interventions relating to it, are notably absent in the literature. The National Institute for Health and Care Excellence (2017) recommends occupational therapists support positive risk-taking in intermediate care. This review did not identify any studies that explicitly focus on how occupational therapists facilitate risk enablement or positive risk-taking (RCOT, 2017). However, there are many examples of the implicit approaches occupational therapists are employing to ensure occupational dysfunction is ameliorated, harmful risk is mitigated and positive outcomes are realised.
Implications
It was expected that there would be a paucity of research relating to risk management, including positive risk-taking, in intermediate care from an occupational therapy perspective which is why a scoping review with a broader focus was conducted. Possible reasons for this lack of information may reside in the diverse nature and approaches used in risk management and how occupational therapists use clinical and professional reasoning, informal theories and tacit knowledge to problem solve risk-prone situations. These techniques may be difficult to communicate and therefore difficult to investigate in research. However, examples of best practice methods including overcoming barriers to employing such risk management strategies that support policy and guidance have not been identified. This knowledge gap presents implications to occupational therapy student and clinical practice education. It is important to develop training programmes that are evidence based and are reflective of occupational therapy expertise in the delivery of intermediate care. This challenges future research to investigate the explicit methods of risk management and how positive risk-taking is facilitated in intermediate care by occupational therapists involved in its delivery and who are experts in their field.
Strengths and limitations
This scoping review has been conducted using a systematic and rigorous process and has benefitted from the experience of a multi-professional research team and a comprehensive quality assessment of the studies under review. Intermediate care has different definitions and therefore, a broad and inclusive criterion was adopted. This resulted in a broad focus on different areas of practice that may not be fully representative of any specific intermediate care setting. Many studies relating to discharge were screened out as they did not meet our definition of intermediate care and these studies may have added value to this review. There were studies that included perspectives from disciplines other than occupational therapy and this must be considered in the findings of this review. Three studies were not available.
Conclusion
This scoping review identified 10 risk domains and three areas of risk characteristics which are central to occupational therapy practice in intermediate care.
Occupational therapists predominantly seek to mitigate risk relating to a client’s symptoms, mobility and function within their environment but are aware of risk related to themselves, suboptimal systems and processes within organisations. Organisational policies and practices together with high demands for intermediate care services are not always congruent with mitigating risk relating to psychosocial phenomena such as loneliness. This can cause conflict between those providing care and service providers.
There are many examples of the implicit management of risk in relation to the positive effect of occupational therapy interventions in the ‘Decision-making under risk’ and ‘Improving safety’ risk characteristics. However, this review has found no explicit information relating to key risk management strategies including how the likelihood and severity of risk is assessed and how positive risk-taking is facilitated. Likewise, there is a lack of occupational focus and therefore a gap in knowledge as to how risk is embraced and reconciled with the value and need for occupation for those accessing intermediate care services. Successful positive risk-taking is dependent on effective risk management skills. Future research must focus on all aspects of risk management and how positive risk-taking is factored into occupational therapy interventions in relation to older adult intermediate care in support of the current policy and guidance.
Key findings
• 10 risk domains were identified, ‘Falls’ being the most common. • Three prominent risk characteristics were reported. • Managing occupation in relation to risk-taking strategies was implicit within the literature reviewed.
What this study has added
This study has mapped the current literature relating risk in intermediate care from an occupational therapy perspective, providing insight into risk within the service to further knowledge and research direction.
Footnotes
Acknowledgements
The authors thank the Northumbria University inter-loan library team for their support in resourcing and obtaining publications.
Declaration of conflicting interests
The author declares there are no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Northumbria University as part of a PhD studentship; no other agency is involved in the funding of this publication.
Research ethics
The ethics department at Northumbria University’s Faculty of Health and Life Sciences provided permission and ethical approval.
Screening decision tree.
A quality assessment summary of the quantitative and qualitative studies.
Key: ✓ = yes; × = no; ! = unclear or not reported and N/A = not applicable.
Quantitative
Studies
Gooch, 2003
Davis Aisling and McClure, 2019
Simning et al., 2019
Kinn and Galloway, 2000
Ruchinskas et al., 2001
Ruchinskas, 2003
Hasegawa and Kamimura, 2018
Corrado et al., 2014
1. Was the study purpose clearly stated?
✓
✓
✓
✓
✓
✓
✓
✓
2. Was relevant background literature reviewed?
✓
✓
✓
✓
✓
✓
✓
✓
3. Was the design appropriate for the study question?
✓
✓
✓
✓
!
✓
✓
✓
4. Were any bias(es) identified or considered?
✓
✓
✓
✓
✓
!
!
!
5. Was the sample/sampling process described in detail?
!
✓
✓
×
!
!
!
!
6. Was sample size justified?
×
N/A
×
N/A
N/A
×
×
N/A
7. Were the outcome measures reliable?
!
!
!
!
!
✓
✓
!
8. Were the outcome measures valid?
!
!
!
!
!
✓
✓
!
9. Intervention was described in detail?
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
10. Contamination was avoided?
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
11. Cointervention was avoided?
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
12. Results were reported in terms of statistical significance?
✓
N/A
✓
N/A
N/A
✓
✓
N/A
13. Were the analysis method(s) appropriate?
!
!
✓
✓
!
✓
!
!
14. Clinical importance was reported?
✓
✓
!
✓
✓
✓
✓
✓
15. Dropouts were reported?
N/A
N/A
✓
N/A
N/A
✓
N/A
N/A
16. Conclusions were appropriate given study methods and results?
✓
✓
✓
✓
✓
✓
✓
✓
Qualitative
Studies
Moats, 2007
Nygård et al., 2004
Buri et al., 2000
Xu et al., 2019
Squires et al., 2019
Chana et al., 2016
Mole et al., 2019
Darragh et al., 2013
Scheirton et al., 2003
Mu et al., 2011
Rose and MacKenzie, 2010
1. Was the study purpose clearly stated?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
2. Was relevant background literature reviewed?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
3. Was the design appropriate for the study question?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
!
4. Was the sample/sampling process described in detail?
✓
✓
✓
!
!
!
✓
!
!
5. Was the sampling method appropriate to the study purpose or research question?
✓
✓
✓
!
✓
!
✓
6. Was sampling done until redundancy in data was reached?
×
×
×
×
×
×
×
×
×
7. Clear and complete description of the site and participants?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
8. Clear role of the researcher and their relationship to the participants?
×
✓
✓
×
✓
×
9. Was there sufficient information to understand the data collection?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
10. Procedural rigour was used in data collection strategies?
✓
✓
!
✓
✓
✓
✓
✓
✓
✓
✓
11. Data analyses were inductive and appropriate?
✓
✓
✓
✓
✓
✓
!
✓
✓
✓
✓
12. Findings were consistent with and reflective of data?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
13. Decision trail developed?
×
×
×
×
×
×
×
×
×
×
×
14. For auditing, is the process of analysing the data was described adequately?
✓
✓
!
✓
✓
!
✓
!
!
✓
15. Did a meaningful picture of the phenomenon under study emerge?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
16. Was there evidence of the four components of trustworthiness?
×
×
×
×
×
×
×
×
✓
✓
×
17. Conclusions were appropriate given the study findings?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
18. The findings contributed to theory development and future OT practice/research?
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓