
Abstract
Introduction
Research suggests stroke negatively affects sexuality yet is rarely addressed by healthcare professionals. This study aims to explore occupational therapists’ perceptions of addressing sexuality post stroke with service users and whether they perceive it to fit into their scope of practice.
Method
A qualitative study was undertaken following an inductive reasoning approach. Three occupational therapists working within stroke rehabilitation were purposively recruited. Data were gathered through semi-structured interviews and analysed using inductive thematic analysis to generate four significant themes.
Findings
Findings generated the following themes: (1) Acknowledging the impact stroke has on sexuality. (2) Consideration of the appropriate stage of the stroke journey to address sexuality; identifying home/community environments to be more appropriate, utilising a multi-disciplinary approach to facilitate this. (3) Barriers to addressing sexuality, including staff’s personal feelings, inexperience, limited resources and ageism. (4) Facilitators to addressing sexuality, including approaching the topic appropriately and utilising the role of occupational therapy and resources.
Conclusion
This study highlights the gap in the stroke journey where sexuality lies and the role occupational therapists can play in closing this gap. Utilising facilitators such as resources and a multi-disciplinary approach can overcome barriers to practice including embarrassment, prejudice and inexperience.
Introduction
The incidence of stroke across Europe and the United States of America ranges from 95 to 269 per 100,000 (Mukherjee and Patil, 2011) and is the biggest cause of disability in the United Kingdom, with two-thirds of people in Wales who experience a stroke leaving hospital with some form of disability (NHS Wales, 2018). Research shows having a impacts on sexual health and a large population of stroke survivors experience sexual dysfunction which is rarely addressed by healthcare professionals (McGrath et al., 2018). The World Health Organization (2006) recommends adopting a positive and respectful approach to sexuality that enables safe sexual experiences. The American Occupational Therapy Association (2020) recognises sexuality as an activity of daily living (ADL), contributing to quality of life, implying sexuality is in the scope of occupational therapy (OT). UK National Stroke Guidelines (2016) recommend stroke survivors should be asked if they have any concerns around sexuality following their stroke. There is currently limited research into the role OT plays in addressing sexuality post this research aims to explore it.
McGrath and Sakellariou (2016) explored occupational therapy practice in relation to sexuality, advocating sexuality as an important part of occupational identity. Encompassing a range of occupations including self-care, intimacy and sex, sexuality impacts on well-being and quality of life yet are overlooked by occupational therapists. McGrath et al. (2018), Nilsson et al. (2017) and Thompson and Ryan (2009) conducted separate qualitative studies into stroke survivors’ experience of the impact stroke has on relationships. Participants reported sexuality was hindered by stroke-related deficits, including weakness, fatigue and sensation. All three studies concluded participants experienced relationship changes, with partners facing a shift to a carers’ role resulting in reduced intimacy, creating emotional distance. Participants suffered identity loss, reduced self-esteem and changed relationships with their bodies, negatively impacting on sexuality (McGrath et al., 2018).
Seymour and Wolf’s (2014) cross-sectional study explored changes in sexual participation following a stroke. Utilising standardised outcome measures including Quality of Sexual Function Scale and Patient Health Questionnaire-9 increased validity and reliability of results due to the ability to repeat methods with consistent procedure and scoring (RCOT, 2017a). The study found levels of sexual dysfunction correlated with higher depression scores. Participants report medication and fear of experiencing another stroke as reasons for reduced desire for intimacy (McGrath et al., 2018; Seymour and Wolf, 2014; Thompson and Ryan, 2009). Dusenbury et al.’s (2017) systematic review into determinants of sexual dysfunction found similar results, in addition to fatigue, pain and depression, as reported by Nilsson et al. (2017). All studies reported participants received little to no advice on sexuality from healthcare professionals (Dusenbury et al., 2017; McGrath et al., 2018; Nilsson et al., 2017; Seymour and Wolf, 2014; Thompson and Ryan, 2009).
Mellor et al. (2013) explored healthcare professionals’ views on discussing sexual well-being post stroke with service users, including occupational therapists, nurses and doctors. In a qualitative study generalisable to UK practice, participants reported feeling it was not appropriate or a priority. Participants in McGrath et al.’s (2018) study felt healthcare professionals not addressing sexuality contributed towards sexual difficulties post stroke. Stroke survivors feel unprepared for the impact stroke has on their sexuality and are unsure where to access support, leading to reduced sexuality correlating with depression and poorer quality of life (Hamam et al., 2012; McGrath et al., 2018; Seymour and Wolf, 2014). Research reveals stroke survivors’ views differ on when to discuss sexuality; some feel the acute stage is too early (Seymour and Wolf, 2014) and others feel they would value the discussion before discharge (Nilsson et al., 2017).
Research suggests healthcare professionals do not identify discussing sexuality to be within their role, feeling other professions are more equipped, reporting a lack of training and feeling ill-equipped to answer questions (Mellor et al., 2013; Thompson and Ryan, 2009). Healthcare professionals’ embarrassment reportedly contributes towards silencing sexuality believing it is taboo (Guo et al., 2015; Hamam et al., 2012; McGrath et al., 2018; Mellor et al., 2013). Mellor et al. (2013) report healthcare professionals felt discussing sexuality was inappropriate with people who live alone, in nursing homes, or widowed, cognitively impaired or ‘older’ people. Healthcare professionals were either unaware of available resources or did not use them; Hamam et al. (2012) analysed educational materials for sex after stroke, concluding resources use negative terminology, focussing on problems rather than solutions. Stroke survivors receive rehabilitation for most activities of daily living, involving goal setting and specialised equipment, yet the approach to sexual rehabilitation following stroke is entirely different, appearing to be a forgotten meaningful occupation (Guo et al., 2015; Hamam et al., 2012).
Following concerns of the role being passed between healthcare professionals with no ownership, occupational therapists in Guo et al.’s (2015) study developed a script to normalise the subject, offering to listen to service users concerns and inform them of available resources. 100% success rate of addressing sexuality with service users within 9 months was achieved, indicating change is possible. Nilsson et al. (2017) call for an holistic, person-centred approach to sexual rehabilitation and that occupational therapists identify addressing sexuality within their scope of practice (Guo et al., 2015; Mellor et al., 2013).
Research aim
To explore occupational therapists’ perceptions of addressing sexuality post stroke with service users and whether they perceive it to fit into their scope of practice.
Research objectives
1. To explore occupational therapists’ perceptions of addressing sexuality post stroke with service users and how it fits into their role 2. To explore the barriers to addressing sexuality post stroke 3. To explore the facilitators to addressing sexuality post stroke
Methodology
An empirical design was adopted due to the specificity of the subject and as it is predominantly used within social science to research experiences (Punch, 2006; Thomas, 2017). A qualitative design aided understanding of the descriptive, in-depth data collected from OTs’ experiences (Walliman, 2018). A quantitative approach could have been used to gain numerical, measurable data (Punch, 2006); this was considered to explore how often sexuality is addressed by OTs; however a qualitative approach was decided upon to gain descriptive, in-depth answers and to understand the ‘why’ rather than the ‘how many’.
Recruitment
An exploratory sample was used rather than an experimental sample due to the small scale of the research and the fact the topic has limited past research into it (Denscombe, 2010). Specific participants meeting the inclusion criteria were selected, using purposive sampling to produce the most accurate data (Denscombe, 2010; Thomas, 2017). The inclusion criteria were occupational therapists working in Wales with at least one year’s experience working with people who have experienced a stroke. Two gatekeepers identified appropriate participants meeting the inclusion criteria and emailed participant information sheets and consent forms to the sample. This research had a limited time frame of 6 months due to submission deadlines; therefore, only three participants were chosen through quota sampling (Denscombe, 2010). Participants were selected from different geographical areas, with varying levels of experience of working with people who have experienced a stroke with an aim to improve representation (Thomas, 2017). Participant 1 (P1) worked in a hospital rehabilitation setting not specific to stroke, Participant 2 (P2) worked across a stroke-specific hospital and community settings and Participant 3 (P3) on stroke-specific acute and rehabilitation wards.
Data collection
Semi-structured individual interviews were used, allowing the researcher to guide the conversation, to ensure relevance, maintain flexibility whilst enabling participants to elaborate (Denscombe, 2010). Bias was reduced by using a reflexive approach and asking open questions to avoid influencing the data (Walliman, 2018). Interviews loosely followed a structure of exploring what the participants’ knowledge was of the impact stroke has on sexuality, what experience they had personally with discussing sexuality post stroke with service users, any barriers and facilitators they had faced when discussing sexuality post stroke and how they felt about discussing sexuality as an occupational therapist, connecting this to perceptions on how it fits into the role of occupational therapy.
Interviews were conducted in a room of the participants’ choice in their place of work, minimising work disruption, lasting 20–35 min (Jamshed, 2014). Following consent, data were recorded on an audio recording device and transcribed verbatim. The researcher’s positionality was considered in relation to personal experience, knowledge and how this may impact data interpretation (Thomas, 2017). The researcher was an occupational therapy student, with skills obtained through university to plan and implement research for their dissertation. The researcher has a personal connection to the topic from working in stroke departments.
Data analysis
The data were analysed systematically and rigorously to provide transparency, yielding trustworthy, meaningful results (Nowell et al., 2017). The researcher immersed themselves in the data by transcribing the interviews and reading and re-reading the transcripts. Inductive thematic analysis was used to generate codes and significant themes from the transcribed data (Braun and Clarke, 2006) drawing conclusions to the research aim. Each step of the analysis process was discussed with the research supervisor, as well as being clearly explained in reflective logs and placed into a portfolio documenting the research process to ensure transparency and rigour (Braun and Clarke, 2006; Nowell et al., 2017). Thematic analysis was chosen for its ability to analyse participant perspectives, finding commonalities and differences, making links and providing insight into qualitative data (Braun and Clarke, 2006; Nowell et al., 2017). Reflexivity was used to separate personal experience when analysing data, reducing bias (Warwick, 2020). The research supervisor monitored the data analysis process further reducing bias and improving credibility (Nowell et al., 2017).
Ethics
Ethical approval was obtained from the University Research Ethics Standing Committee, ensuring the Nuremberg Code and Declaration of Helsinki ethical principles were met and the study posed no harm to participants and provided some benefit (Ghooi, 2011; RCOT, 2017b). Approval was gained from the health board (RCOT, 2017b), and two gatekeepers were identified, who ethically approved access to the sample and research environment (Denscombe, 2010). The research process was explained to the gatekeepers and sample. This facilitated trust by suppling information for participants to give informed consent (Denscombe, 2010; RCOT, 2017b). Participants reserved the right to withdraw from the study at any point. Confidentiality was maintained at all times with no demographics divulged on recordings or transcribed data (RCOT, 2017b); these were stored on an encrypted USB and deleted when no longer needed, in line with Data Protection Act (2018).
Findings and discussion
Importance occupational therapists placed on addressing sexuality
Participants acknowledged the significant impact stroke-associated deficits have on sexuality supporting findings (McGrath et al., 2018; Nilsson et al., 2017; Thompson and Ryan, 2009), including weakness, communication, fatigue and sensation (Figure 1). the lack of sensation… they might not be able to get the sensation to build up the sexual relationship (P3. L33-34) Thematic analysis map.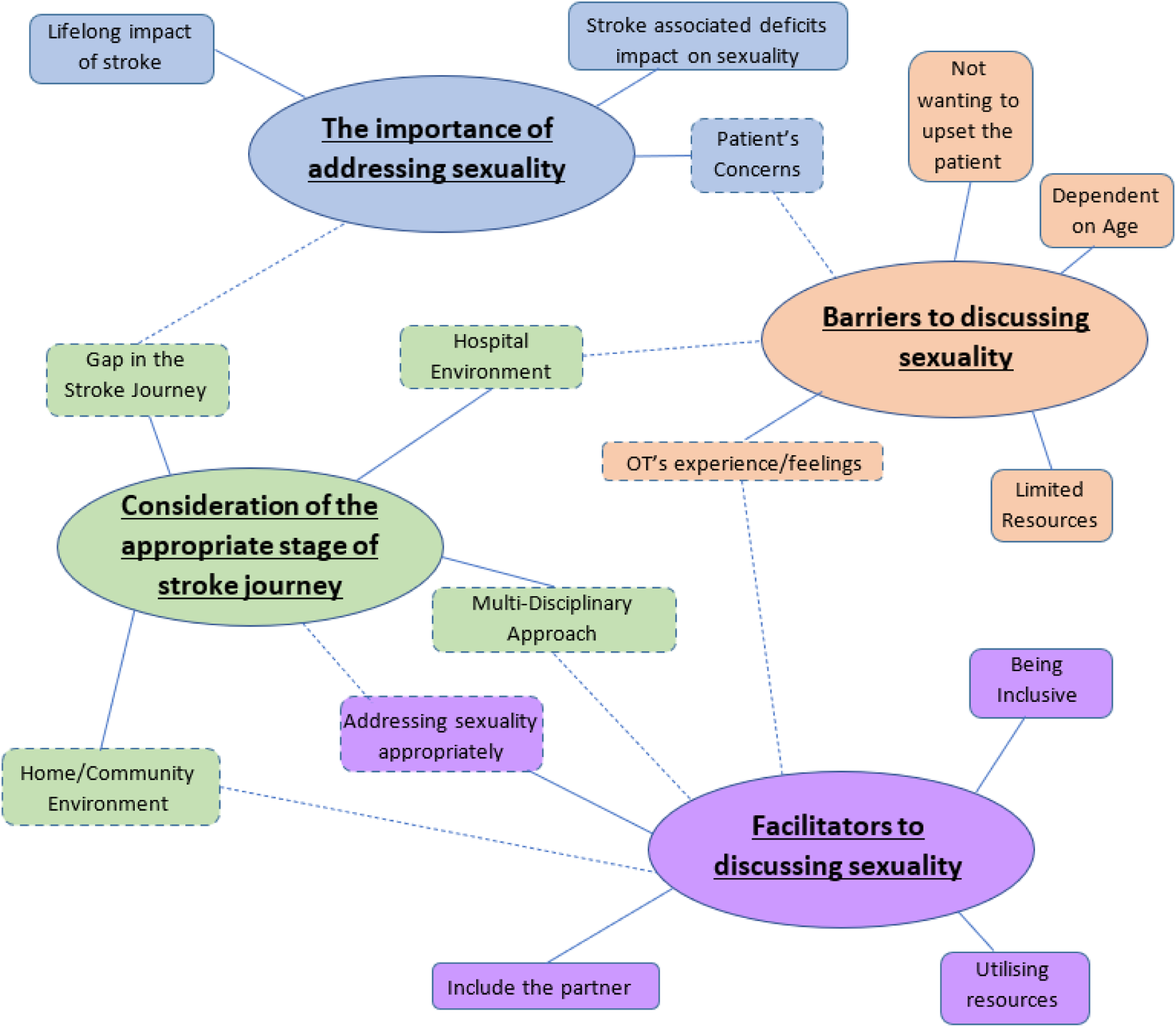
Discussing the effects self-esteem and depression have on libido related with Seymour and Wolf (2014), who found sexual dysfunction correlated with high rates of depression. Participants explained frontal lobe strokes may cause behavioural changes leading to increased sexual drive, requiring intervention to manage, supporting Mellor et al. (2013). people have had frontal lobe strokes and their personalities have changed and their inhibitions are lowered, so they’re sexually inappropriate (P2. L39-40)
Two participants discussed the unpredictable nature of stroke recovery; a stroke is a lifelong impacting event disrupting normal life. As a result, patients are left with concerns including worries of having another stroke, as reported in existing research (McGrath et al., 2018; Seymour and Wolf, 2014; Thompson and Ryan, 2009). it’s not just…when you fracture a hip, you get a new one and you know they’re going to heal in a few weeks (P2. L156-167)
For these reasons, participants expressed the importance of addressing sexuality, supporting (Hamam et al., 2012 and Guo et al., 2015) stating sex is a meaningful occupation for occupational therapists to address as holistic professionals. It is important that we address it… we’re holistic (P2. L136) for some people it will be the most meaningful… we have to acknowledge that (P2. L152-163)
Participants acknowledge the importance of addressing sexuality; however, this is not often reflected in their practice. made me realise that we’re not addressing it (P3. L16) I wouldn’t say it’s something that we’ve asked them specifically at that time (P1. L14-15)
Consideration of the appropriate stage of stroke journey to address sexuality
Participants identify a gap in the stroke journey due to occupational therapists and other members of the multi-disciplinary team not addressing sexuality, reported in research to contribute towards inability to resume normal life (McGrath et al., 2018; Nilsson et al., 2017; Seymour and Wolf, 2014). I do feel that there is a gap out there in the stroke journey (P2. L42)
Acknowledging this gap, participants considered the appropriate stage to address sexuality. All three participants felt home/community environments facilitated addressing sexuality, describing it as more appropriate. This reflected findings of Seymour and Wolf (2014) and Mellor et al. (2013), reporting patients have not considered sexuality as an issue before returning home, highlighting the need to support patients upon discharge. people often think that if they can get past the barrier of going home then they’re going to be alright, but that’s often when reality sets in (P2. L178-180)
Expanding on this, participants supported (Mellor et al., 2013), identifying the hospital environment as a barrier to discussing sexuality, considering it inappropriate and not a priority as service users are focussing on basic and essential needs. We don’t think of it as a priority, especially in rehab or in hospital (P1. L36-37) in acute we’re talking about basic needs… the ADLs [activities of daily living], toileting, washing, mobilising (P3. L194-196)
However, P3 suggested it could be appropriate for patients that have had a long hospital stay or have been discharged early following quick recovery; an interesting observation as participants reported acute settings to be inappropriate; however, this is a generalisation and does not take into consideration service users’ unique post-stroke journeys. we do get patients staying for 3 or 4 months so it does need addressing (P3. L197) if people go home quickly because they’ve done really well, they might need that information (P3. L88-89)
Disputing (Guo et al.’s, 2015) study who felt discussing sexuality was an occupational therapists’ job, all three participants felt it was not the sole responsibility of the occupational therapist. Participants reflected (Mellor et al.’s, 2013) findings, suggesting a multi-disciplinary approach to facilitate identifying the appropriate stage to discuss sexuality by utilising differing expertise. Two participants felt stroke nurses and Stroke Association coordinators are in appropriate positions to address sexuality within the community. P2 suggested it should depend on which healthcare professional the patient is most comfortable with. they might feel more comfortable with a physio or a speech and language therapist (P2. L122-123)
This proposes discussing sexuality should be a multi-disciplinary approach; however, P3 raised concern this risked the role being passed between team members and potentially neglected, as raised by Guo et al. (2015).
Barriers occupational therapists faced in addressing sexuality
Participants identified limited resources as a barrier to addressing sexuality in the community, associated with no access to Early Supported Discharge (ESD) and long waiting lists for Community Brain Injury Teams. Other limited resources included time, staffing and access to handouts, supporting (Nilsson et al.’s, 2017) findings. we do use [Community Brain Injury Service] for long term but their waiting list is huge, so there isn’t a lot of services out there, that’s why it’s a shame for ESD, that really helped bridge the gap (P2. L171-173)
A significant barrier raised was staff’s personal feelings towards approaching sexuality – particularly embarrassment, supporting existing research (Hamam et al., 2012; Mellor et al., 2013; Nilsson et al., 2017). Staff commonly do not feel comfortable discussing sexuality; two participants displayed these feelings and one participant identified it in others. Staff get embarrassed (P1. L35) I personally don’t want to bring it up (P3. L121-122)
This suggests a need to raise awareness and normalise the topic of discussing sexuality.
Two participants felt their lack of experience and knowledge in discussing sexuality contributed to their uncomfortable feelings, feeling ill-equipped to provide support due to no training, as reported by Mellor et al. (2013) and Thompson and Ryan (2009). I’ve had very little experience in discussing it (P3. L122)
Participants are able to identify barriers to addressing sexuality but a lack of experience is potentially one of the most significant barriers. Factors such as timing, environment and resources may be limitations; however, only one participant was able to reflect on a specific example of when they had approached sexuality with a service user. It is therefore important to take into consideration that these are perceived barriers by the participants and not necessarily based on experience. This raises concern over why more training is not provided on addressing sexuality, considering it contributes towards well-being and quality of life (McGrath and Sakellariou, 2016). Guo et al.’s (2015) research highlights that incorporating sexuality into assessments as a tick box normalised the subject for both the service user and occupational therapist, reducing feelings of embarrassment and expanding on therapists’ experience.
Another barrier identified is perceptions that addressing sexuality is dependent on age, supporting (Mellor et al., 2013). Two participants felt more comfortable addressing sexuality with younger patients, suggesting it would feel more appropriate. One participant admitted being ageist, stating they would not assume an 85-year old would be sexually active, reflecting healthcare professional’s views in Mellor et al.’s (2013) study. Two participants acknowledged it would be wrong to make such assumptions. I know this is ageist (P1. L29-30) it would be wrong for us to assume that they [older generation] don’t do anything, that’s not true, many people have active lifestyles (P2. L89-91)
Contributing to feelings of embarrassment are acknowledged taboos of discussing sexuality, as raised by two participants and reflected in research (Guo et al., 2015; McGrath et al., 2018; Mellor et al., 2013), making the conversation difficult for occupational therapists and patients. Revealing another barrier of not wanting to upset the patient, P3 was apprehensive of disrupting the therapeutic relationship by discussing sexuality, reflecting expressions by participants in Mellor et al.’s (2013) study. it’s not something I’d initiate because of fear of upsetting the patient (P3. L129)
This highlights requirements for increased confidence in staff to approach sexuality appropriately, without prejudice or upsetting patients.
Facilitators occupational therapists employed in addressing sexuality
Participants felt a multi-disciplinary approach could mitigate some barriers, utilising expertise or collaborating with more experienced occupational therapists to overcome inexperience. P2 identified their experience as a facilitator, having developed the instinct to know when the situation is appropriate. Suggesting therapists should be educated about addressing sexuality in university, supporting normalisation, as noted by Mellor et al. (2013) and Thompson and Ryan (2009). having worked with people and having been qualified for 15 years, it is different, you’re experience to know when it is appropriate (P2. L106-108)
Participants reported experience improves knowledge of addressing sexuality appropriately. They advise using the same technique with everyone is inappropriate, suggesting utilising therapeutic use of self to get the best out of the situation for the patient. P2 stated addressing sexuality should be approached like any area of practice, utilising the occupational therapy process to find out what is most important to the individual and collaboratively problem-solving. it’s how you approach it and how you interpret it in terms of what’s important for them (P2. L138-139)
Participants acknowledge building rapport facilitates approaching sexuality appropriately, feeling getting to know the person put therapist and patient in a better position for discussing sexuality. This was disputed by Mellor et al. (2013) and Nilsson et al. (2017), both reporting participants felt discussing sexuality could damage rapport. it depends on how much of a rapport – does the patient feel happy discussing it (P3. L71-72)
Two participants identified being inclusive as an integral factor; people of all ages and gender experience post stroke sexual dysfunction, supporting existing research (Mellor et al., 2013; Dusenbury et al., 2017). P3 supported (Nilsson et al.’s, 2017) findings, stating it is important to be inclusive of all, no matter age, gender, sexual orientation or marital status. People might develop a relationship when they go home, it shouldn’t matter if they’re single or in a relationship (P3. L192-193)
It is important to include the partner if the patient is in a relationship; all participants noted stroke does not solely affect the individual. Partners may have to adjust to behavioural changes or deal with emotional detachment; spouses commonly take on a carer role, moving away from the spousal role, also reported in the literature (McGrath et al., 2018; Thompson and Ryan, 2009; Nilsson et al., 2017). Occupational therapists can play a vital role reassuring patients and partners. wife will have to have those conversations and learn strategies about how to cope with that (P2. L47-48)
Participants felt the role of occupational therapy aids inclusivity by being holistic, an attribute that also facilitates addressing sexuality. While participants felt this was not exclusively an occupational therapists’ role, they identified aspects of the role that could be utilised to provide support regarding sexuality, supporting existing research (Mellor et al., 2013; Guo et al., 2015). Specific skills include task analysis of functional activities, problem solving, developing strategies to manage behaviour, providing a counselling role and collaborating with patients to achieve meaningful goals.
Participants felt utilising resources including leaflets, questionnaires or the Stroke Association could mitigate the barrier of occupational therapists’ personal feelings and inexperience. P1 suggested lifestyle questionnaires may reduce feelings of embarrassment, enabling patients to raise sexuality without an occupational therapist directly asking them. This proposal supports (Guo et al., 2015), who found using a script normalised the situation for both the occupational therapist and patient. Participants found Stroke Association resources useful to aid advice when feeling underqualified to answer questions. Unfortunately, participants identified limited access to resources. P3 reported their ward had information relating to a range of areas post stroke, but nothing on sexuality after stroke, as was discovered by McGrath et al. (2018) who reported a lack of available resources to patients. All participants creatively problem-solved this, creating a patient information corner, integrating questions within the stroke screen/passport or providing questionnaires. This suggests potential options in developing appropriate resources. I think it’s easier if you introduce a booklet, then they come back to you and say I want help, it’s easier than going to them (P1. L59-61)
However, Hamam et al. (2012) concluded that available resources on sex after stroke focus on problems, not solutions. It could therefore be proposed these resources are used as a facilitator to conversations, rather than a substitute.
Implications
This research highlights a need for further education and training for occupational therapists on addressing sexuality appropriately with patients, supporting them to return to this meaningful occupation and normalising sexual rehabilitation. There has been recent development of guidelines from the Care Quality Commission on ‘relationships and sexuality in adult social care services’ (CQC, 2019). However, a lack of experience felt by occupational therapists could be addressed through specific occupational therapy guidelines from professional bodies such as the Royal College of Occupational Therapists. Additional to this, participants identified potential areas for service development in regard to the available resources on sex after stroke to aid support. This study contributes a specific occupational therapy perspective on addressing sexuality post stroke, which has not previously been explored. Findings suggest addressing sexuality does come under the scope of occupational therapy; however, a multi-disciplinary approach should be adopted. Findings corroborate existing research, demonstrating elements of generalisability and transferability to inform practice.
Limitations
Limitations included a small sample size specific to one health board. Due to the sample size, occupational therapists from community settings were not included, meaning results were biased to a hospital setting. Considering participants’ perceptions that acute settings are not appropriate, participants from community settings may have offered a counterargument to this viewpoint. A small sample also meant only female occupational therapists were interviewed, excluding views from a male perspective which may have produced a different result. These limitations are likely to cause bias results, particularly when considering occupational therapy as a female-dominant profession and stroke statistics (Stroke Association, 2018) show males are more at risk of having a stroke at a younger age putting them in a position to more likely warrant a discussion regarding sex. This relationship and feelings of discomfort between female therapists and male patients to discuss sex in an acute setting needs to be considered and could be one of multiple potential hypotheses to be explored. Further research is required into the specific role occupational therapy plays in addressing sexuality post stroke with a larger sample, including occupational therapists of both genders from multiple health boards, locations and stroke settings. Participants did not discuss the changes in roles and occupational identity that stroke survivors experience (McGrath et al., 2018); this could be a potential area for further research in relation to occupational therapy philosophy.
Conclusion
Findings support existing research identifying the importance of addressing sexuality with service users post stroke. Stroke-associated deficits significantly impact on sexuality, which is not commonly addressed by occupational therapists, leading to disrupted relationships, reduced mood and quality of life for stroke survivors. Participants identify sex as a meaningful occupation and recognise the role that occupational therapists can play in supporting patients adapt to sexuality post stroke. However, occupational therapists do not feel it is their sole responsibility and that a multi-disciplinary approach should be taken to identify the most appropriate environment, approach and time in which to address sexuality with a stroke survivor. Occupational therapists face barriers including limited resources, embarrassment, ageism, lack of training and experience, leading to feelings of being underskilled and the taboo nature of sexuality causing concern of upsetting patients. However, identified facilitators could mitigate these barriers including the use of resources, a multi-disciplinary approach, being inclusive, including the partner and the role of occupational therapy itself.
Key findings
Addressing sexuality does come under the occupational therapy scope of practice as a meaningful occupation. Barriers include embarrassment, lack of training and limited resources. Facilitators include a multi-disciplinary approach, resources and utilising the role of occupational therapy.
What the study has added
This study highlights the gap in the stroke journey where sexuality lies and the role occupational therapy can play in closing this gap by utilising facilitators to overcome the current barriers to practice. Considering existing research outcomes, there is potential for the normalisation and addressing of sexuality to increase well-being and quality of life for stroke survivors and their partners.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.