
Abstract
Objective
Injuries can have a long-lasting effect on ability to return to work, but there is little research on which outcomes are most important to patients. This study aims to identify and prioritise return-to-work outcomes important to patients for evaluating vocational rehabilitation interventions.
Methods
Nominal group technique focus group with trauma patients.
Results
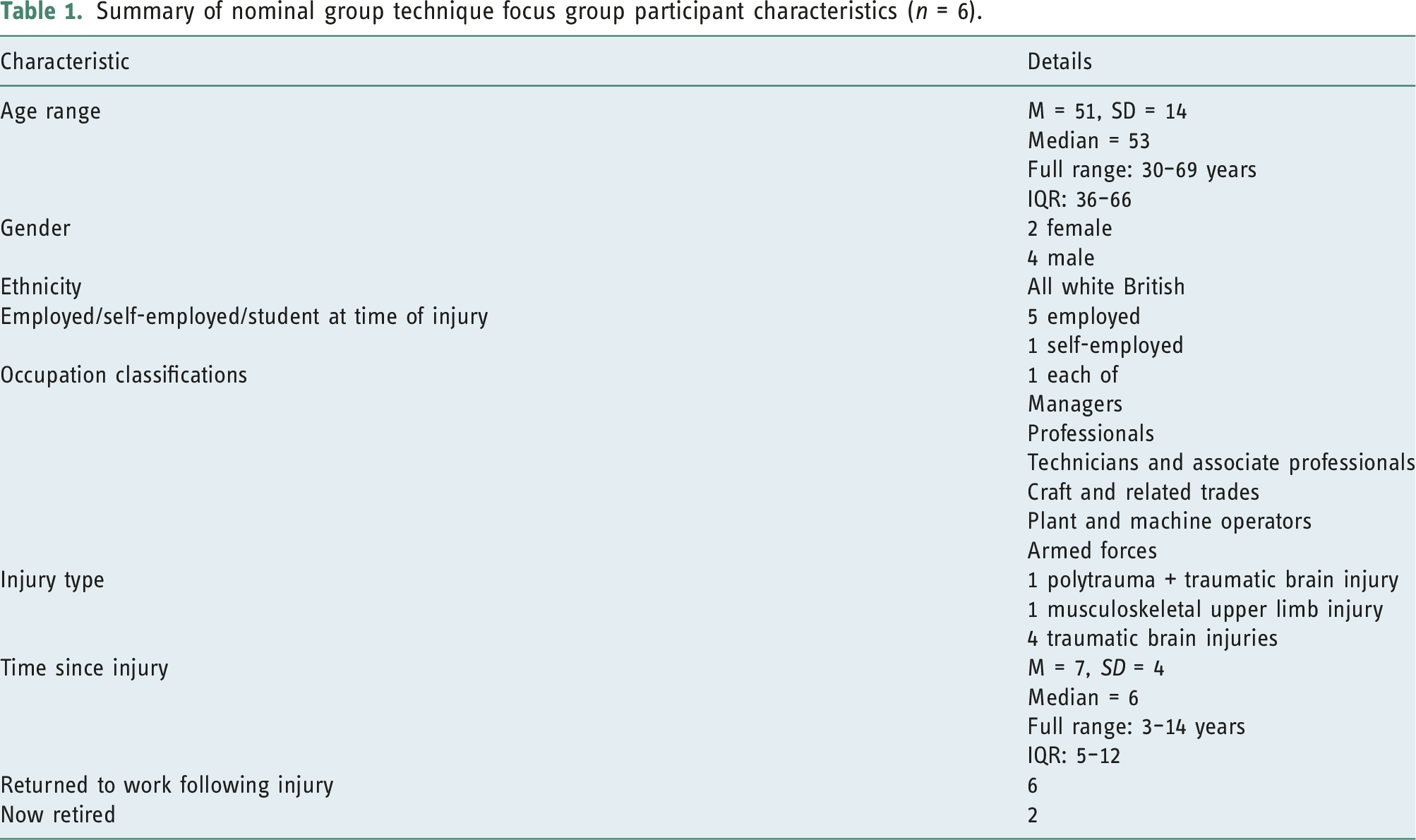
Focus group participants (n = 6) included mostly traumatic brain injuries, a range of occupation types, ages and both genders. Participants identified and prioritised their eight most important outcomes which were: sense of purpose and life satisfaction, understanding the impact of injury, assessment of readiness to return to work, using SMART (specific, measurable, achievable, relevant and time-bound) goals, facilitated reintegration to work, assessing capacity to return to work, collaboration between key stakeholders and improved employer and employee knowledge. Many of these were measures of the process of, rather than change outcomes of vocational rehabilitation.
Conclusions
The range of outcomes identified by trauma patients highlights the complex process of return to work and the need for vocational rehabilitation evaluations to incorporate a broader range of outcomes. Measures of the process of vocational rehabilitation are also important to trauma patients and should be included in such evaluations.
Introduction
Traumatic injuries are a worldwide health problem, with an estimated 56 million hospital admissions annually (Haagsma et al., 2016). For many working age adults, return to work is delayed by the injury effects, with one third of patients admitted to hospital after injury not having returned to work 12 months later (Kendrick et al., 2017). Return to work has many benefits including improved finances, self-esteem, social connection and quality of life (Waddell and Burton, 2006). Vocational rehabilitation (VR) (Escorpizo et al., 2011) interventions improve return-to-work rates for conditions including brain or spinal injuries and mental health problems (Cancelliere et al., 2016; Donker-Cools et al., 2016; Roels et al., 2016).
Generating evidence of the effectiveness of VR interventions requires consideration of which outcomes (i.e. changes brought about by the intervention or those relating to VR processes) should be measured and evaluated. However, selecting outcomes is difficult because specific work-related outcomes (e.g. work status and sickness absence) or broader outcomes (e.g. quality of life), may not capture the complexity of return-to-work processes (Wasiak et al., 2007) or the wide range of potential mediators or moderators of return to work affecting VR interventions (Saltychev et al., 2013). The choice of outcomes that capture the complexity of return-to-work processes is poorly informed by existing evidence as reviews of return-to-work following traumatic injury show absence of good quality Randomised Controlled Trial (RCT) studies and outcomes (Saltychev et al., 2013). Evidence highlights the importance of using a biopsychosocial approach to inform and evaluate VR interventions (Condon et al., 2019), which should be reflected in outcome measurement. Evidence also highlights the need to capture the heterogeneity of the lived experiences of patients, the priorities of different stakeholders (Wasiak et al., 2007) and the importance of social relations between stakeholders for return to work (Tjulin et al., 2010). Additionally, research advocates investigating further return-to-work process outcomes which capture priorities for patients (Hees et al., 2012; Roels et al., 2016; Vogel et al., 2011) that are distinct from change outcomes such as productivity, pay and time off work (Young et al., 2005). In fact, capturing the views of patients with lived experience is essential not only to inform intervention development but also the methods of evaluating its effectiveness (Skivington et al., 2021).
Our study aimed to identify and prioritise return-to-work outcomes of importance to patients (both in terms of change and processes) to inform an evaluation of a VR intervention delivered by occupational therapists and clinical psychologists to patients admitted to UK major trauma centres (Kendrick et al., 2021). The VR intervention (approved by NHS Ethics Committee) adopts a biopsychosocial approach and has been developed to work at both remedial (treating physical and psychological problems which may impact on return to work) and the social and environmental levels (adapting the work environment, job, role, responsibilities and changing the trauma survivors, co-workers’ and employers’ attitudes and confidence through education and supported self-management).
Methods
Research design
A nominal group technique (NGT) (Delbecq et al., 1975) focus group was used to identify and prioritise return-to-work outcomes important to trauma patients. The NGT is inclusive of all participants’ experiences, generating rich data, achieving consensus and allowing data prioritisation in a relatively short time period through the voting process.
Participants were recruited from a group of trauma patients providing patient and public involvement (PPI) input into the design and evaluation of the VR intervention (Kendrick et al., 2021). The members of the PPI group were recruited into the wider study using a variety of methods, aiming to identify a heterogeneous groups with a wide range of injury, employment, educational and socio-economic characteristics. Our PPI recruitment framework aimed for heterogeneity in occupation classification types, age, gender and type of injury to encourage diverse inputs. All PPI members were invited to take part in the NGT focus group. A time where most of those willing to take part were available, was agreed. All participants provided written consent. Participants own experience of VR support varied.
Data collection and analysis
Participants were provided with a 15-min overview of the proposed VR intervention and detailed explanation of the NGT process. Frequent reference was made to the single question guiding the discussion: What are the most important outcomes of a return-to-work intervention for people who have experienced traumatic injury? The NGT stages were: (1) Generation of Ideas: participants silently wrote their answers to the question; (2) Round Robin Discussion: audio recorded anonymous reading of generated ideas, with amalgamation of similar points (3) First Vote: participants chose and ranked their six priority outcomes (to make second ranking more manageable); (4) Discussion of First Vote: the six priority outcomes were reported to the group, and the group’s discussion was audio-recorded (eight outcomes were taken to the final vote to accommodate four pairs of equally ranked items from the first vote) and (5) Final Vote: participants each ranked the priority outcomes in their preferred order. Group ranking was calculated by summing ranked scores from individual participants (i.e. ranked first = 6; ranked last = 1).
The data collected included individually written notes, voting cards, flip charts, moderator notes, audio recordings and an Excel spreadsheet with individual rankings.
Results
Summary of nominal group technique focus group participant characteristics (n = 6).
Top 18 outcomes identified by the participants
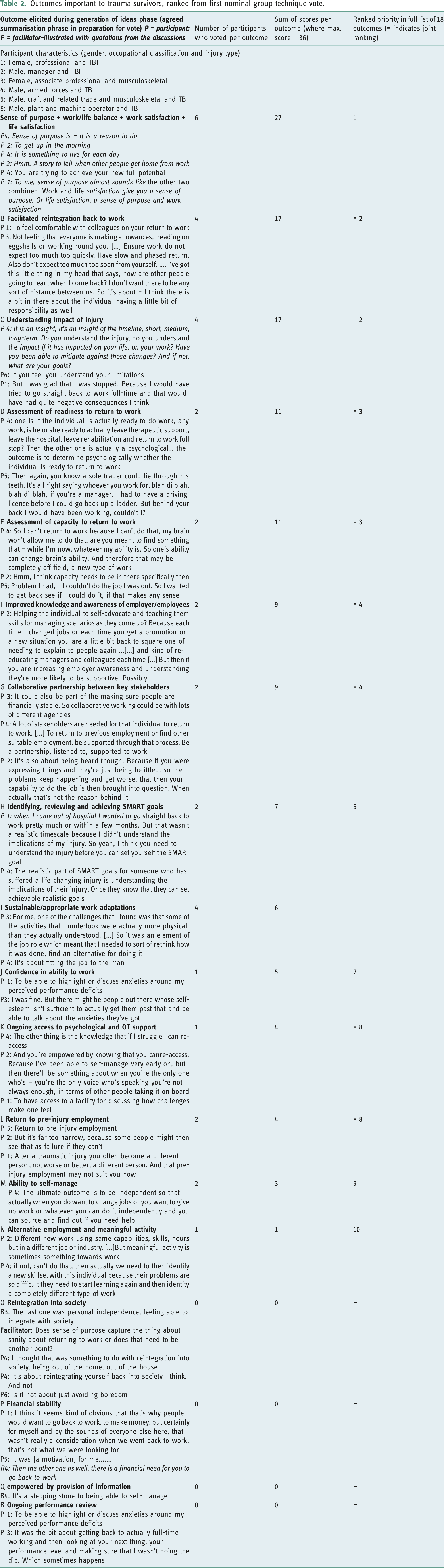
Eighteen discrete outcomes important to trauma patients were elicited and agreed by the participants in the first discussion phase (described and illustrated with examples in Table 2). The outcomes can be grouped into four categories, with some outcomes relevant to more than one category: 1. Quality of life (outcomes A: sense of purpose/work–life balance/work satisfaction/life satisfaction, and O: reintegration into society), 2. support in return to work (outcomes B: facilitated reintegration back to work, C: understanding impact of injury, D: assessment of readiness to return to work, E: assessment of capacity to return to work, F: improved knowledge and awareness of employer/employees, L: return to pre-injury employment, N: alternative employment and meaningful activity and Q: empowered by provision of information), 3. ability to maintain work performance and engagement (outcomes C: understanding impact of injury, F: improved knowledge and awareness of employer/employees, H: identifying, reviewing and achieving SMART goals, I: sustainable/appropriate work adaptations, J: confidence in ability to work, K: ongoing access to psychological and OT support, M: ability to self-manage, Q: empowered by provision of information and R: ongoing performance review) 4. managing injury and related challenges (outcomes C: understanding impact of injury, G: collaborative partnership between key stakeholders, K: ongoing access to psychological and OT support, N: alternative employment and meaningful activity, M: ability to self-manage, P: financial stability and Q: empowered by provision of information). Outcomes important to trauma survivors, ranked from first nominal group technique vote.
The ranking order of the eight most important outcomes (Table 3)
Top eight outcomes important to trauma survivors, ranked from second nominal group technique vote.
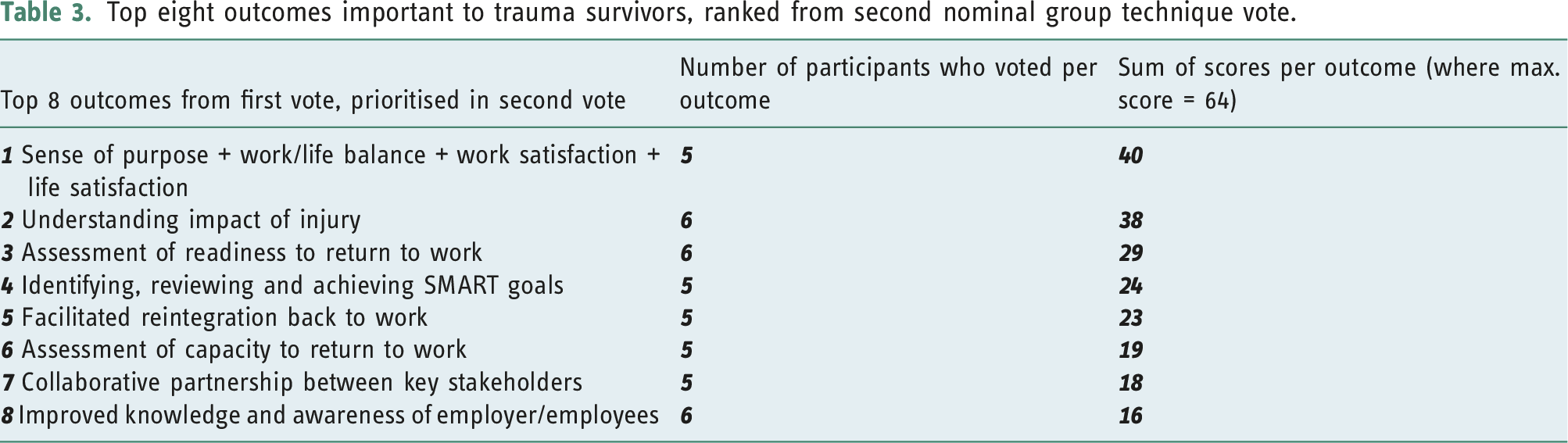
The most highly prioritised outcome (A) was an amalgamation of four separate outcomes: sense of purpose/work–life balance/work satisfaction/life satisfaction. Participants identified these outcomes in the initial-generation phase, as being sufficiently similar to group as one outcome for voting. This outcome encapsulated the importance of having a sense of purpose or meaningful work or activity (e.g. education or volunteering) which resulted in work and/or life satisfaction. This was seen to be relevant even if return to pre-injury work was not possible.
The joint second most important outcomes were facilitated reintegration back to work (B) and understanding the impact of injury (C). Outcome B referred to third-party facilitation of trauma patients’ re-joining the workplace that resulted in returners feeling ‘comfortable’ with colleagues. Outcome C encompassed the need for trauma patients, employers and colleagues to understand the short-, medium- and long-term impacts of injury on work and life in order to manage expectations about recovery by different stakeholders including patients, colleagues and employers.
The joint third most important outcomes were assessment of readiness for (D) and capacity to return to work (E). Participants clearly differentiated these two outcomes before voting, with readiness referring to processes to determine whether an individual was psychologically and physically ready to return to work. Capacity to return to work referred to the trauma patients’ ability to return to their pre-injury job and whether there was a need to identify alternative solutions.
The joint fourth most important outcomes were improved knowledge and awareness by employers and employees (F) regarding trauma patients’ needs and collaborative partnership (G) working between key stakeholders as part of the VR process. Key stakeholders included the family/close people, therapist, employer and other agencies such as the UK Department for Work and Pensions (responsible for welfare and pensions) and charities, for example, Headway.
The fifth most important outcome was goal identification and monitoring (H), describing the need for individually appropriate and SMART (specific, measurable, achievable, relevant and time-bound), goal setting as part of the VR process.
It is noteworthy that six of the eight most important outcomes (B, D, E, F, G and H) related to VR processes as opposed to outcomes per se.
Discussion
Main findings
The study’s primary aim was to identify patient priorities regarding return-to-work outcome measures to inform the effectiveness of a VR intervention. The NGT focus group identified and prioritised a range of outcomes relating to return to work of importance to trauma patients, which reflected their multiple needs and the complex process of return to work. These included outcomes focussing on the broader benefits of work for patients (e.g. providing a sense of purpose or life satisfaction; understanding the physical and psychological impact of injury) and on VR processes (e.g. assessment of readiness for and capacity to work, facilitated reintegration to work, improving knowledge and awareness of employers and employees, collaborative partnerships between stakeholders and identifying, reviewing and achieving SMART goals). Many of these outcomes were related to each other or were prerequisites for one or more other outcomes to be achieved.
Comparison to previous research
Previous research highlights the limited and inconsistent nature of trauma outcome measurements, especially in relation to environment, activity and participation domains (Hoffman et al., 2014). Our study supports the importance of these domains, as prioritised outcomes focus on improved work environment, creating collaborative partnerships and facilitating reintegration to work. A review of return-to-work outcomes (Wasiak et al., 2007) identified goal-setting, work readiness assessment, work satisfaction, reintegration, interaction with stakeholders and appropriateness of management to be important, consistent with our study findings. Our findings also support recent qualitative research finding outcomes of importance to trauma patients include psychological and physical recovery, purposeful life engagement and managing the expectations of key stake holders (i.e. individuals, colleagues and employers) (Bridger et al., 2021). Unlike previous research, our study did not find productivity loss or return to work to be important outcomes, while highlighting the importance of measuring process as well as change outcomes (Hoffman et al., 2014).
To our knowledge this is one of the only studies of patient prioritisation of outcomes (Radford et al., 2018) for a VR intervention for survivors of traumatic injury with a range of employment, gender and age characteristics, although the majority had experienced brain injury. Evidence shows that VR intervention commissioners and research commissioners prioritise outcomes differently from patients (e.g. short-term vs longer-term) (Radford et al., 2013). Our research has highlighted that trauma patients want reassurance that the VR they receive includes some key process features that are measured, and which serve as important interim outcomes in their recovery journey.
Strengths and limitations
Participants were recruited from a single PPI group (aiming to recruit a heterogonous membership in terms of injury, occupational and social economic characteristics) and due to unexpected cancellations, the group was smaller and had a less diverse range of injury types than planned. The number of participants was still within recommended group size for the NGT (Delbecq et al., 1975). Although our participants had experienced a range of injuries, some injuries (e.g. spinal cord injury or amputation) were not represented in our group. It is possible that other outcomes could have been identified or outcomes prioritised differently if participants with such injuries had been included. Most participants were several years into their recovery, potentially affecting recall of priorities earlier in their recovery. However, this allowed insight into medium and longer-term outcomes.
Research implications
The diverse range of outcomes identified by patients provides important knowledge for evaluating VR interventions. For example, readiness to work and/or work self-efficacy may prove useful indicators of intervention success, especially when the dichotomous outcome of return to work is not achieved within the study follow-up period or where environmental and socio-economic factors such as economic downturns limit opportunities for return to work. Measures such as a sense of purpose or life satisfaction may be useful outcomes when return to life and work as it was pre-injury might not be possible (e.g. severe injuries) or may help explain other work outcomes. Similarly, process measures (e.g. goal setting) may be useful for quality assurance of the rehabilitation process in VR evaluations and in clinical practice. Future research should explore the role of severity and type of the injury (e.g. musculoskeletal injuries) on priority of outcomes and how outcome importance varies over time. While the present research identified sense of purpose as a key outcome, it is important to explore how this impacts on recovery and return to work.
Practice implications
VR intervention trials should ensure they measure outcomes prioritised by trauma patients (e.g. sense of purpose and understanding injury impact), including process measures. Process measures can also be used to inform the design of VR services, quality assure services and evaluate the VR processes. Supporting people to participate in daily life including work is a primary focus in occupational therapy (Désiron et al., 2011) worldwide (WFOT 2012). Occupational therapists deliver VR in many settings worldwide and generating evidence of VR intervention is one of the key strategies of the World Federation of Occupational Therapists (WFOT, 2012). However, occupational therapists should ensure they measure outcomes that are relevant to their service-users, the intervention focus and the context in which VR is delivered.
Key findings
• Patients from mostly traumatic brain injuries and diverse employment contexts identified key outcomes to measure in vocational rehabilitation interventions.
• Patients prioritised outcomes which include sense of purpose, life satisfaction and key stakeholder education (e.g. patients and employers).
• Patients prioritised process outcomes (e.g. assessment of readiness to return to work) as well as typical change outcomes measured in vocational rehabilitation interventions.
What the study has added
The range of outcomes identified and prioritised by trauma patients highlights the complex process of return to work and the need for vocational rehabilitation evaluations to incorporate a broader range of outcomes. The findings also highlight the importance of involving individuals with lived experience in identifying appropriate outcome measures for a complex return-to-work intervention.
Patient and public involvement
Patient and public involvement were involved in the study design, funding acquisition, data analysis and write up.
Footnotes
Acknowledgements
This paper has been written on behalf of the wider Return to Work after Trauma (ROWTATE) team, including all grant co-applicants and members of our Patient and Public Involvement (PPI) group. The authors would like to acknowledge their support in conducting this research. We would also like to thank all participants for taking part in this research.
Author contributions
K.B. methodology, formal analysis, writing, data collection, review and editing. B.K. funding acquisition, project administration, methodology, formal analysis, writing, review and editing. D.K. conceptualisation, funding acquisition, project administration, methodology, writing, review and editing. J.K. methodology, data collection, review and editing. J.H. review and editing. S.T. methodology, conceptualisation, funding acquisition, review and editing. I.A. design and analysis. S.F. design and analysis. K.R. conceptualisation, funding acquisition, project administration, methodology and review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Reference number RP-PG-0617-20001). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Institutional Review Board Statement
Ethical approval for this study was obtained in 2019 from the University of Nottingham Faculty of Medicine and Health Sciences Research Ethics Committee (Ref: FMHS 150-1811) and Leicester South NHS Research Ethics Committee.