
Abstract
Introduction
The dearth of clinical trials of individualised occupational therapy with people with a diagnosis of psychosis limits the evidence base globally for occupational therapy practice. This study evaluated the feasibility of conducting a pragmatic clinical trial.
Method
Mixed methods design using a pragmatic perspective; two-centre, one-group pretest-posttest study, at six months. POINTER Occupational Intervention Specification captured routine individualised occupational therapy. Process evaluation included recruitment, retention, intervention delivery, fidelity, adherence and outcome measurement. The primary outcome was participation in activities of everyday life, measured by Time Use Survey, Participation Scale and Utrecht Scale for Evaluation of Rehabilitation-Participation. The Canadian Occupational Performance Measure measured self-reported experience of and satisfaction with occupational performance. The Short Form-36v2 Health Survey measured health-related quality of life, a secondary outcome. Participants’ experiences were explored using a questionnaire. Intervention providers’ perspectives were investigated via the POINTER occupational intervention log and focus groups.
Results
Recruitment was (20/36) and drop-out 20% (4/20). Fidelity was 77%, and adherence was good; POINTER had validity and utility. Outcome measurement was acceptable to participants, indicating increased participation in activities of everyday life.
Conclusion
A larger clinical trial is merited; recruitment processes need further exploration, and outcome measurement needs refining.
Introduction and background information
Mental health is the largest cause of disability across European Union countries; 27% of the adult population have experienced at least one of a series of mental disorders in the past year (WHO, 2018). Psychosis is a general term for a class of mental health disorders, which includes the following descriptions: schizophrenia, schizoaffective disorder, schizophreniform disorder, delusional disorder and affective psychosis, for example, bipolar disorder or unipolar psychotic depression (NICE, 2014). The experience of psychosis: …include[s] hearing voices (‘hallucinations’), believing things that others find strange (‘delusions’), speaking in a way that others find hard to follow (‘thought disorder’) and experiencing periods of confusion where you appear out of touch with reality (‘acute psychosis’). (Cooke 2014: 10)
Disability for those experiencing psychosis – affects both peoples’ activity and participation in their daily lives (Krupa et al., 2010) – it is associated with narrowing of occupations, relationships and the places that people go to (Brown, 2011).
Occupational therapy enables individuals to improve participation in their activities of everyday life; participation in everyday life is an international research priority for occupational therapy specifically (Mackenzie et al., 2018) and as an outcome for early intervention in psychosis research generally (Renwick et al., 2018). Participation has international importance; activity and participation are core components of the International Classification of Functioning, Disability and Health (ICF) (WHO, 2001). Nevertheless, conceptual clarify is lacking (Khetani and Coster, 2007) making it problematic to research ‘participation’ as an outcome, without a clear definition. A systematic literature review and narrative synthesis focused on mental health and developed a definition for this study: ‘Participation occurs when an individual is involved in activities, within the context of their life, which provides that person with a sense of engagement’ (Bannigan et al., 2016b).
Systematic review and best evidence synthesis
As part of a programme of research underpinning this study, a separate systematic review and best evidence synthesis was conducted of occupational therapy and participation in activities of everyday life for adults with a diagnosis of psychosis (Inman, 2017). It identified four categories of occupational therapy interventions: life skills training (n = 6), individualised client-centred (n = 5), activity-based (n = 4) and cognitive (n = 3) (Inman, 2017). Of the five individualised occupational therapy intervention effectiveness studies identified and critiqued (Cook et al., 2009; Edgelow and Krupa, 2011; Katz and Keren, 2011; Lindstrom et al., 2012; Mairs and Bradshaw, 2004), only one had high methodological quality (Cook et al., 2009). All were tailored to individual needs using a structured format, that is, Occupational Therapy Intervention Schedule (Cook et al., 2009), Action Over Inertia (AOI) (Edgelow and Krupa, 2011), Occupational Goals Intervention (OGI) (Katz and Keren, 2011), Occupational Therapy Intervention Process Model (OTIPM) (Lindstrom et al., 2012) and Manual of Case Formulation Approach (Mairs and Bradshaw, 2004). Three studies delivered training in the intervention for those providing it; however, fidelity to the treatment interventions was measured in only two studies (Cook et al., 2009; Mairs and Bradshaw, 2004). Adherence to treatment was measured in one study (Cook et al., 2009). There was no consensus on how to measure participation as an outcome. It was concluded that there was no evidence for the effectiveness for individualised occupational therapy on participation in activities of everyday life or quality of life (Inman, 2017). The dearth of clinical trials internationally of sufficiently high methodological quality was concerning. One approach to begin to address this was to conduct feasibility studies to support future robust clinical trials. Feasibility studies are conducted before a main study to ensure the study implementation is practical, reducing threats to the validity of findings (Tickle-Degnen, 2013).
A fundamental issue in the design of future clinical trials was how to achieve intervention descriptions in sufficient detail to enable replication and achieve international reporting standards for clinical trials (Hoffmann et al., 2014). This remains a concern for the occupational therapy profession globally. A Cochrane review critiqued occupational therapy delivered by specialists (occupational therapists) versus non-specialists for people with schizophrenia (Morris et al., 2018). Identifying the need for further research to develop the evidence base and reduce uncertainties around the best way of delivering occupational therapy for people diagnosed with schizophrenia (Morris et al., 2018). Despite extensive searching and consulting experts in the field, no pre-existing individualised occupational therapy intervention specification for individuals with a diagnosis of psychosis, living in the community, was identified that met international reporting requirements for use in clinical trials (Hoffmann et al., 2014). Subsequently, the Participation through Occupational INTervention Effectiveness Research (POINTER) Occupational Intervention Specification was developed for this purpose – separate to, and as part of, a programme of research to support this study – applying the methodology for developing, evaluating and reporting complex interventions (Inman, 2017; Medical Research Council, 2008). This was not a new occupational intervention, rather a documentation of routine best practice, incorporating best available evidence to enable it to be evaluated and replicated under robust research conditions.
The aim of the POINTER study was to assess the feasibility of conducting a pragmatic clinical trial of individualised occupational therapy for people with a diagnosis of psychosis and occupational need. Key objectives were to explore the validity and utility of the POINTER; levels and methods of measuring fidelity and adherence and valid method of measuring participation, with utility and the indication of effect of occupational therapy.
Method
Research design
An exploratory two-centre, one-group pretest–posttest feasibility study for a pragmatic clinical trial of individualised occupational therapy was conducted, investigating both participant and process outcomes. The perceptions of the study procedures, the intervention and its effect were explored from the perspectives of the participants and intervention providers (Sturkenboom et al., 2012). A pragmatic perspective was adopted exploring routine practice as this enables the results to be more applicable to clinicians’ own circumstances (Hotopf et al., 1999). The pragmatic-explanatory continuum indicator summary (PRECIS) was applied when making study design decisions (Thorpe et al., 2009).
Ethics
The Health Research Authority, National Research Ethics Service Committee North West–Lancaster (NRES Ethics reference 14/NW/1426) 2013 granted full ethical approval. Registration was made to the Research Registry (researchregistry800).
Participants
From January to March 2014, participants were recruited from two centres: a total of seven community mental health and psychosis teams, as per pragmatic principles to use normal settings (Thorpe et al., 2009). This was a convenience sample of teams who were willing to participate in the study. Eligible participants were over 18 years, living in the community, with a primary diagnosis of psychosis (dual diagnosis was acceptable) and mild to very severe occupational/functional needs. Individuals were excluded if they had an organic brain disorder or suspected organic cause to psychosis (e.g. dementia) and/or a primary diagnosis of substance misuse. The aim was to recruit 64 participants, to achieve a sample size of 60 (30 participants from each centre).
Enrolment process
Participants for the study were identified through occupational therapy referral processes in practice, as per pragmatic principles (Thorpe et al., 2009) by their care coordinator, who routinely assessed their capacity and applied this to study involvement. Occupational need was indicated by a score of two or more on question 10 of the Health of the Nation Outcome Scale (HoNOS) (Cook et al., 2009); HoNOS measures the health and social functioning of people with severe mental illness and specifically problems with activities of daily living (Royal College of Psychiatrists, 2013). Once participants gave consent to engage in occupational therapy, the study was explained, and an information sheet was provided. Research assistants obtained written consent and performed baseline measurement.
Intervention: POINTER
The intervention and delivery details are described using the Template for Intervention Description and Replication (TIDieR) as per international reporting standards for clinical trials (Hoffmann et al., 2014): Brief name: POINTER. Why: to improve participation in the activities of everyday life that were most meaningful to the participants. What (materials): the Canadian Occupational Performance Measure (COPM) and a range of daily activities meaningful to the participants. What (procedures): intervention providers (occupational therapists) followed POINTER to carry out its eight objectives: (1) assess occupational performance; (2) formulate occupational needs; (3) set occupational need goals; (4) plan occupational therapy interventions; (5) implement occupational therapy interventions; (6) reassess occupational performance; (7) review occupational need goals and (8) discharge from occupational therapy and associated key activities (e.g. Objective 7 has two key activities: (7a) review occupational need goals with the individual and (7b) reassess baseline outcome measurement) (Inman, 2017). Who provided: occupational therapists employed to work with individuals with a diagnosis of psychosis were the intervention providers; all registered with the Health and Care Professions Council (HCPC). How: mode of delivery was face to face and one to one. Where: participants’ own homes and communities. When and how much: intervention dosage was weekly – two weekly for up to 6 months. Participants could receive other health and social care interventions (these were recorded). Tailoring: the occupational intervention was tailored to each participant, collaboratively setting their unique occupational need goals and plans, expecting and permitting variation in delivery, frequency and sequencing of objectives and key activities. Modifications (during the study): reported in results. How well (planned measurement of adherence and fidelity): fidelity to the intervention was measured for the study duration, as a percentage rating based on details about what was provided in each session compared to the objectives and key activities in POINTER. All objectives and key activities must have been carried out with the participant, before the end of the six-month period to achieve full fidelity. Adherence was measured using the intervention providers’ ratings on a scale of 0–10, after each session (final rating was the mean rating score). Participants rated their level of adherence once at the end of therapy on a scale of 0–10. How well (actual intervention adherence and fidelity in study): reported in results.
Intervention providers’ enrolment, training and supervision
All intervention providers were selected via a convenience sample, and they volunteered to take part and provided written consent. All had existing clinical caseloads, and new participants commenced occupational therapy when the intervention provider had caseload capacity to work with them, as per clinical practice and pragmatic trial principles (Thorpe et al., 2009). They received a half day training session on the POINTER study protocol, and all completed Good Clinical Practice (GCP) NIHR research online training, engaged in monthly professional supervision and were invited to participate in the focus groups.
Study outcome measurement
Baseline participant demographic data measured was age, gender, diagnosis, time since diagnosis, employment status, occupational need and previous experience of occupational therapy. To enable evaluation of intervention providers’ characteristics, data were collected on their age, gender and length of time as a qualified occupational therapist.
Process outcome measurement
Process evaluation was considered from the perspectives of the participants and intervention providers qualitatively focussing on recruitment, retention, intervention delivery and utility of the methods to measure adherence, fidelity and outcome measurement. A participant questionnaire and POINTER occupational intervention log – to capture the delivery of the intervention, nature of contact, location, duration, objectives and key activities, participant adherence, interventions provided by others, occupational goals, COPM outcome measure scores and overall effectiveness and enablers and barriers – were based on the structure used by Sturkenboom et al. (2012). The participant questionnaire aimed to capture participants’ experiences of the occupational intervention and being involved in the study, largely made up of closed questions to minimise participant burden. It was reviewed by service users through the CRN Mental Health FAST-R (Feasibility and Support to Timely recruitment for Research) Service, National Institute for Health Research (NIHR).
A fidelity checklist was created for POINTER; fidelity was supported and monitored during the study through monthly professional supervision and using the checklist.
A focus group intervention provider conversation guide was developed by the primary researcher to explore experiences of being involved in the study and how occupational therapy enabled participants to increase their participation in activities of everyday life. This was critiqued by the CRN Mental Health FAST-R Service , NIHR to support validity. At the end of the study, the primary researcher facilitated a focus group in both centres.
Outcome measurement
Part of the purpose of this feasibility study was to identify the primary outcome measure for a future pragmatic clinical trial; three measures of participation in activities of everyday life were utilised. The definition of participation created for this study was applied to review the content validity of different measures of participation relevant to mental health (Bannigan et al., 2016b) and found there was no reliable and valid measure of the primary outcome of participation in activities of everyday life (Bannigan et al., 2016a). Of the measures reviewed, the Participation Scale (P-Scale) (Brakel, 2010) and the Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-P) (Zee et al., 2010) had the strongest face validity, utility and acceptability amongst service users. In such circumstances, the criterion validity can be tested, by examining the outcome measures relationship with a robust measure of the primary outcome or one of its constructs (Saks and Allsop, 2007). ‘Time use’, that is, an individual’s involvement in activities, is a key construct of participation. Having a diagnosis of psychosis has been associated with low total time use in activity (Leufstadius and Eklund, 2008). Therefore, changes in ‘time use’ in this study would be expected to have a positive correlation with participation. ‘Time use’ has been measured using the UK 2000 Time Use Survey (TUS), developed by the Office for National Statistics to measure the amount of time spent by the United Kingdom population, on various activities and was designed, where possible to provide results comparable with other European studies (Short, 2006). An adapted version of the UK 2000 TUS (Short, 2006) was used in a study with individuals with a diagnosis of psychosis, and no issues regarding the utility were identified (Fowler et al., 2009). This was used as the primary outcome measure; the Fowler et al. (2009) survey was not available, so the UK 2000 TUS (Short, 2006) was adapted in a similar way. The same two summary measures were used: hours in ‘Constructive Economic Activity’ and hours in ‘Structured Activity’ per week (Fowler et al., 2009).
The P-Scale is an interview-based scale measuring participation restriction; a score of 12 and below is considered to be ‘normal’, and higher scores indicate more severe restrictions (Brakel, 2010). The USER-P is a questionnaire assessing three aspects of participation: frequency, experienced restrictions and satisfaction of ‘vocational activity’ and ‘leisure and social activity’ (Zee et al., 2010). Higher USER-P total scores indicate higher levels of participation (Zee et al., 2010).
The Short Form-Health Survey (SF-36 v2) was used to measure health-related quality of life; normative data are available for the healthy population of the United States (Maruish, 2011). It measures eight domains of health-related quality of life (HRQOL) and self-evaluated transition (SET) which compares their health now to one year ago (Maruish, 2011).
The COPM has utility in clinical research for individuals with a diagnosis of schizophrenia (Cresswell and Rugg, 2003). It measures self-reported experience of occupational performance and satisfaction using a scale of 1–10, and a change in rating of two points or more is considered to be clinically significant (Law et al., 1998).
Data collection
Baseline demographic data including outcome measures were collected from participants prior to intervention commencement by research assistants. At completion of the intervention (or at 6 months), outcome measures and the participant questionnaire were completed with participants by the research assistants. All measures completed by the research assistants were timed to assess participant burden. All research assistants received full training. Intervention providers (occupational therapists), socio-demographic and work experience data, and consent were collected by the primary researcher.
Data analysis
As a feasibility study, the data analysis strategy used descriptive statistics, qualitative analysis and the compilation of basic administrative and physical infrastructure data (Tickle-Degnen, 2013); this was triangulated to evaluate the study outcomes. The primary researcher conducted the analysis, and this was peer reviewed by the second and third authors to increase trustworthiness. Descriptive statistics illustrated baseline characteristics of participants and intervention providers, changes in outcome measure scores, participant experiences and intervention delivery. No statistical testing was possible of the construct validity of the participation measures due to the sample size. Qualitative evaluation of the focus group data was analysed using content analysis (Elo and Kyngas, 2008).
Results
Participants
From 36 potentially eligible service users, twenty were enrolled, and 16 participants completed therapy. The drop-out rate was 20% (n = 4) (see Figure 1), and full data sets were available for 14 participants. Enrolment and participant flow diagram.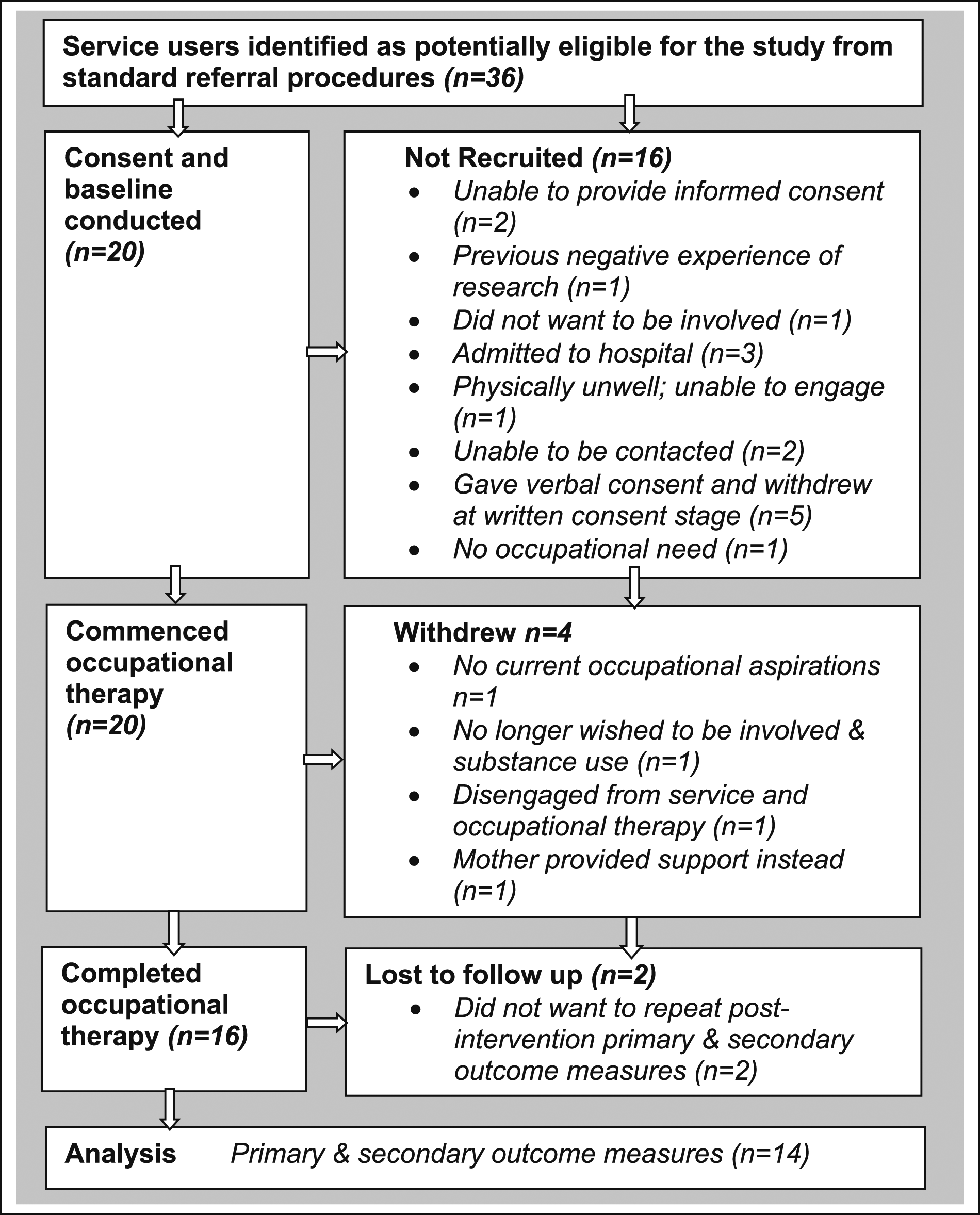
Participants’ baseline characteristics.
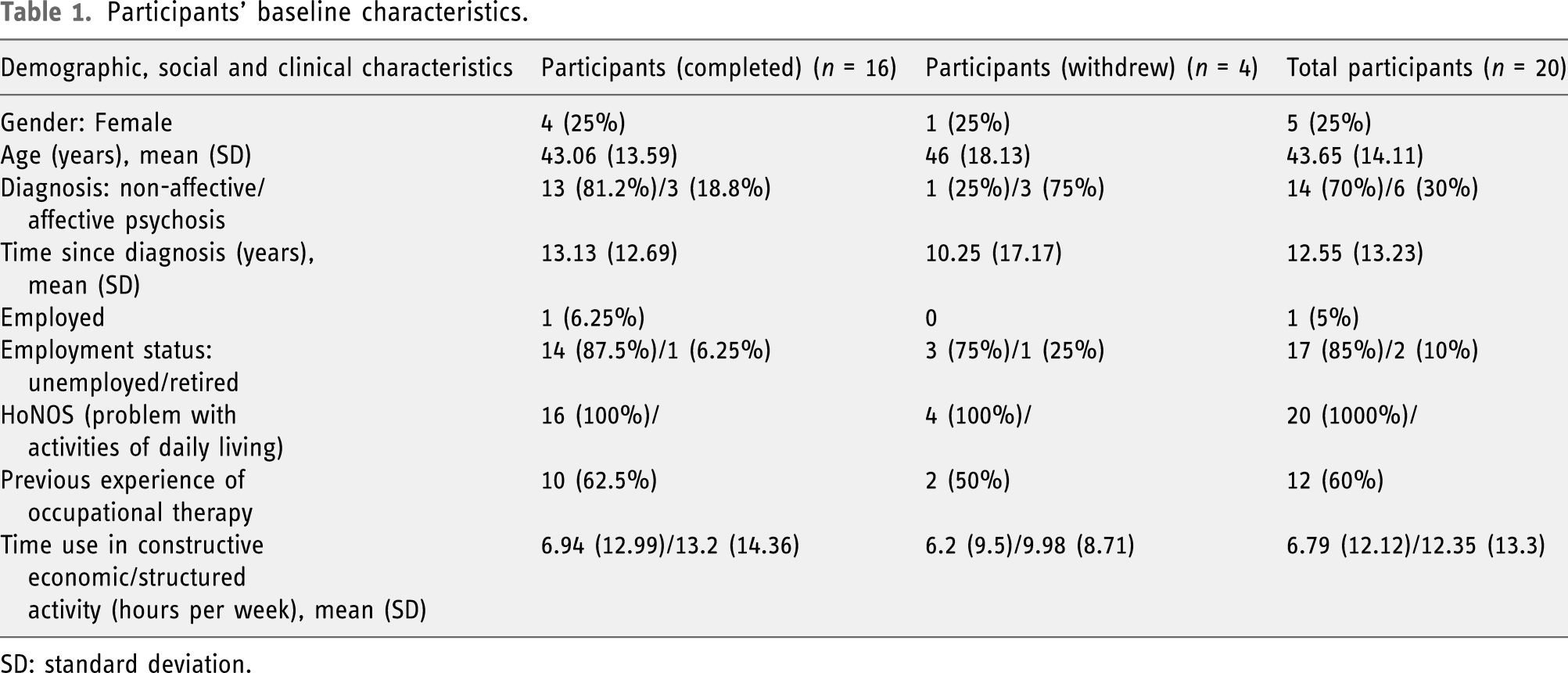
SD: standard deviation.
Process outcomes
The process outcomes show the intervention provided used the relevant items (three–twelve) of the TIDieR checklist (Hoffmann et al., 2014), inclusive of participants’ (analysed from the participant questionnaire) and the intervention providers’ (analysed from the focus groups and POINTER occupational intervention logs) experiences of the study.
Intervention provided
3. Planned materials were used fully for 14 (87.5%) participants who completed the intervention. 4. The objectives and key activities in POINTER planned procedures were utilised by the intervention providers. 5. Seven intervention providers (occupational therapists) delivered the intervention, with a mean professional experience of 13.71 (7, SD) years and 45.71 (8.9) years of age; three were male, and four were female. 6. The intervention was provided face to face and one to one. 7. One hundred and eighty-eight occupational intervention sessions were provided; 144 (76.58%) were in participants’ own homes, 33 (17.55%) in the community, seven (3.72%) in the participants’ own homes and community, telephone, two (1.06%) and CMHT, two (1.06%). 8. The mean number of sessions per participant was 11.75 (6.58, SD), the duration was 19.06 (6.79, SD) weeks and the intensity was 65.15 (23.55, SD) minutes per session, for those who completed the intervention. 9. The permitted tailoring of the intervention was carried out, demonstrated in the intervention delivery details above. 10. POINTER captured 98% of the occupational therapy provided. Modifications made in the course of the study included the provision of ‘non-occupational therapy input’. Defined as interventions provided by occupational therapists for participants, which were not specifically occupational therapy, for example, delivery of medication or care co-ordination. This input was provided in 21 (12%) of the sessions and in discrete sessions on eight occasions. 11. Fidelity and adherence were measured as planned. 12. Fidelity and adherence monitoring occurred for 62% (n = 117) of the sessions of those who completed therapy, and there was 77% fidelity to the POINTER. The highest fidelity was achieved for ‘assessing occupational performance’ (94%) and ‘setting occupational therapy goals’ (93.57%), and the lowest level of fidelity (53.13%) was achieved for ‘discharge from occupational therapy’. Participants (n = 14) were satisfied with their experience of each of the eight POINTER objectives (range 74%–93%). The mean adherence rating from participants was 6.54, and occupational therapists’ mean was 7.68 (both on a 0–10 scale). ‘Other interventions’ from the multidisciplinary team were also provided, as per usual care.
Intervention providers’ experiences
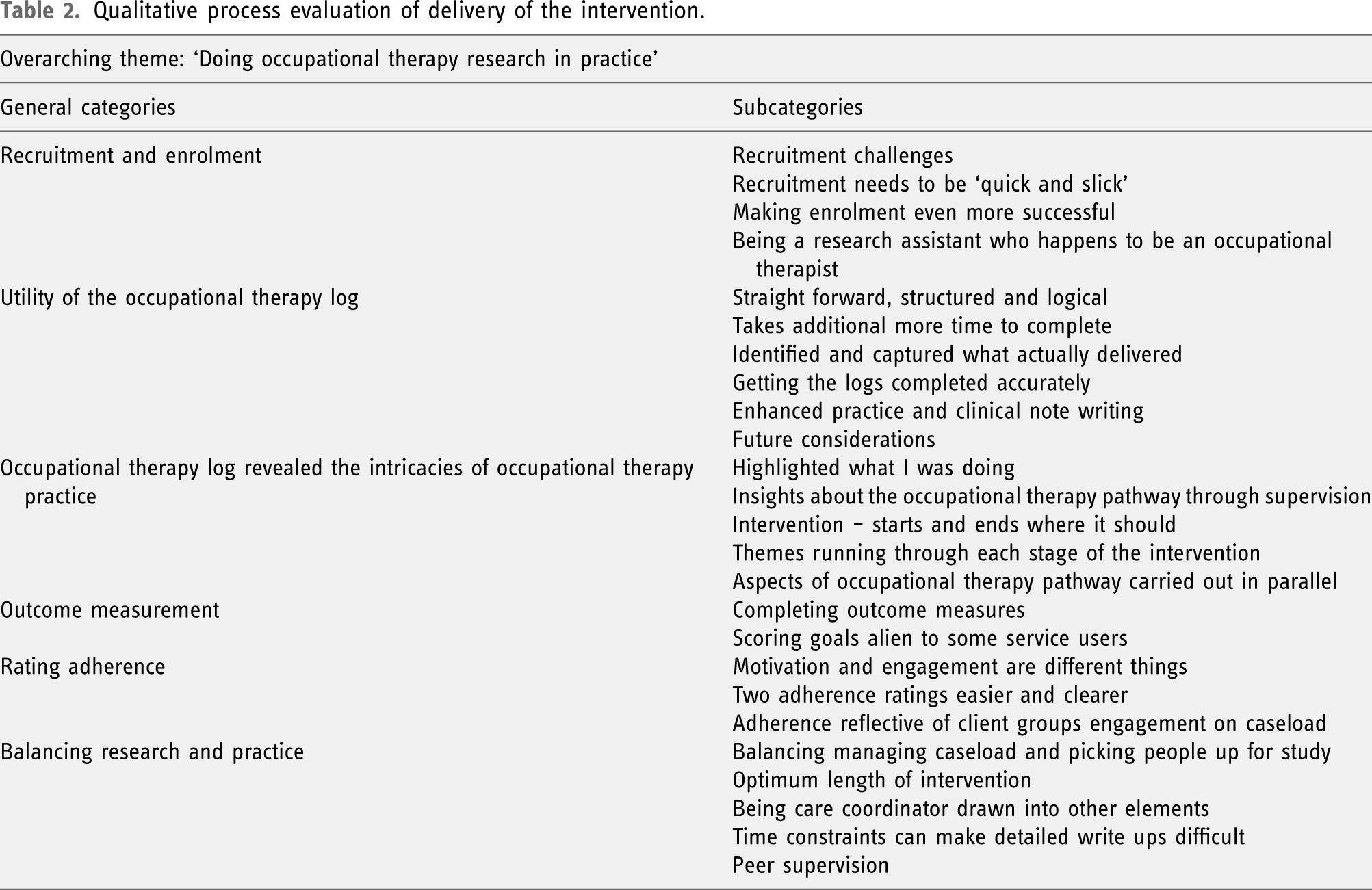
Qualitative process evaluation of delivery of the intervention.
Recruitment and enrolment
Intervention providers discussed not enough time to recruit participants and not everyone met the inclusion criteria or wanted to be involved. The research assistants also had clinical caseloads (separate to this study), identified as sometimes slowing the recruitment process. It was recognised recruitment needed to ‘be quick and slick and responsive’ (OT3C1.18). Strategies for making enrolment even more successful were suggested including having the initial occupational needs screening and conversation about the study either via the telephone or on the home visit with the care coordinator.
Balancing research and practice
The intervention providers spoke about ‘Balancing managing a caseload and picking up new participants for the study’. It was recommended to be more realistic to recruit one participant per month alongside existing caseloads, over a six-month period. The ‘Optimum length of the intervention’ was debated, and some were concerned the six-month time limit for the intervention may have negatively impacted outcomes; nevertheless, it was also recognised that, for some participants, 6 months was ample. ‘Peer supervision’ was deemed a useful mechanism for learning and support.
Utility of the occupational intervention log
Capturing and recording the occupational intervention was reported as ‘pretty straight forward to do’ (OT1C1.3), and ‘it was kind of structured, it was logical, it was a concept I was familiar with’ (OT3C1.2). It was consistently testified that the POINTER occupational intervention log captured ‘what you’ve actually delivered in that session’ (OT4C2.2). However, it also took additional time to complete, more than just doing clinical notes. Getting the logs completed accurately required practice, and some reported that they wished that they had practiced using them more before the study had begun.
Occupational therapy log revealed the intricacies of occupational therapy practice
The POINTER occupational intervention log highlighted what occupational therapists were doing and articulated the thinking processes underpinning what felt like their intuition. Described by one as: ‘It broadly starts off where it should do, and it definitely ends when it needs to, but in the middle then there’s lots of to-ing and fro-ing and going back to the beginning and doing a bit more of an assessment…which is what happens you know in real life’ (OT4C2.5). It was acknowledged that aspects of POINTER were carried out in parallel and that the process was non-linear, just as life is not linear. Comments included: ‘More parts of the schedule were happening than I originally thought’ (OT1C1.1). ‘You almost follow the whole occupational therapy process in one session’ (OT2C2.17).
Rating adherence
One intervention provider commented ‘I think the adherence that we’re talking about is probably reflective of the client group that we are working with’ (OT2C2.14). Adherence was expressed as being affected by many factors, motivation being key and it was questioned: ‘Should it be more around motivation to engage then rather than engagement?’ (OT1C2.9). It was recommended that two adherence ratings would be easier and clearer: one for the actual intervention session and another for activities carried out as planned, in-between sessions.
Outcome measurement procedure and processes
There were challenges getting post-intervention outcome measures completed, and it was advised that incentives for participants may help to improve this response. One described the experience of scoring goals with participants: The ‘guy I was working with was very, you know, the whole idea of putting a number onto something was quite alien to him’ (OT2C1.6). It was highlighted that many participants responded more comfortably to setting small goals about their everyday living during and in-between face-to-face sessions.
With regard to participant burden, 11 (79%) participants reported being either very satisfied (n = 5, 36%) or satisfied (n = 6, 43%) with the time to complete the outcome measures for the study. The mean time to complete the outcome measures (in minutes) was TUS 22.47, SF-36v2 8.91, P-Scale 10.13 and USER-P 11.94.
Outcome evaluation
Results of primary outcome.
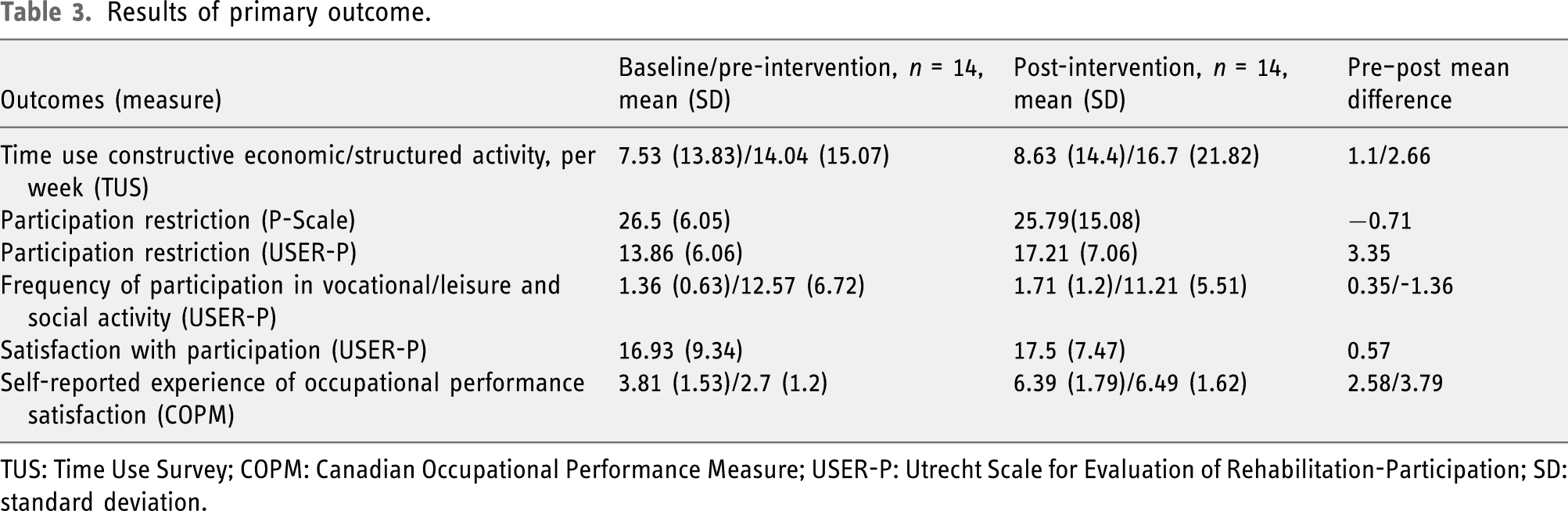
TUS: Time Use Survey; COPM: Canadian Occupational Performance Measure; USER-P: Utrecht Scale for Evaluation of Rehabilitation-Participation; SD: standard deviation.
In the health-related quality of life data, four health domains showed improvements, and four indicated increased health burden. Self-evaluated transition (SET) in health in general improved, shown by pre–post intervention mean differences (3.07, 1.3SD) to (2.38, 1.55SD).
The majority of participants (n = 10, 71%) were more satisfied with their participation in the activities of daily life most meaningful to them and that occupational therapy made it possible for them to participate more in activities and occupations that were meaningful to them. The occupational therapists mean subjective evaluation score for the effectiveness of POINTER provided was 6.36 (scale of 0 = not successful to 10 = very successful).
No ancillary analysis was undertaken, and no harms were reported from the intervention.
Discussion
This study demonstrates the value of feasibility studies prior to clinical trials to improve rigour and reporting. This study achieved an 80% retention rate, which is an acceptable sample size for an effectiveness study with short-term follow-up (Steultjens et al., 2002). However, fewer participants (n = 20) were recruited than planned (n = 64); this was not an issue in the pilot study by Cook et al. (2009) and may be due to the pragmatic design of this study. This suggests planning more time and occupational therapists, accounting for the demands of occupational therapists’ pre-existing caseloads to ensure recruitment targets are met. Equally the recruitment in this study could contribute to a power calculation for sample sizes in future studies. The baseline differences, between those who completed therapy and those who did not, suggest the POINTER may need to include actions to engage service users with low volition and consider how occupational therapists respond to this type of diagnosis. This will need to be monitored in future studies.
In contrast to the interventions identified in the systematic review (Inman, 2017), all of the items in the TIDieR checklist (Hoffmann et al., 2014) were captured and reported within this study, which is critical to achieving a study with high methodological quality (Steultjens et al., 2002). POINTER captured 98% of the occupational therapy carried out, strengthening its validity as a description of individualised occupational therapy for people with a diagnosis of psychosis. Although the POINTER occupational intervention log did take more time to complete than only delivering the intervention, it captured what was actually delivered.
This study achieved an overall fidelity level of 77%, above that achieved by Sturkenboom et al. (2012). As well as being an acceptable level of fidelity, it indicates the utility of the method used. The participants and the intervention providers’ adherence ratings were relatively closely scored, suggesting the validity of the ratings and, therefore, the method used to measure. However, the intervention providers requested an additional adherence measure for in-between sessions which will be considered in future studies.
This was a small sample, with in-group variability, and it was always recognised these results would not be generalisable; nevertheless, the findings are promising. The majority of participants experienced occupational therapy making it possible for them to participate more in activities and occupations that were meaningful to them. The results have shown positive change scores from baseline to post-intervention on Time Use, Self-reported Experience of Occupational Performance and Occupational Performance Satisfaction, Satisfaction with Participation and Participation Restriction. In addition, the self-reported experience of occupational performance and satisfaction with occupational performance showed clinically significant improvements for those participants in the study, and the pre–post intervention mean differences are encouraging. Participants also experienced better health in general (SET) at post-intervention. Participants continued to receive other routine community mental health non-occupational therapy interventions, as is common to pragmatic clinical trials; some changes could be argued to be attributed to these. All further indications that a larger pragmatic clinical trial is merited. As this was a before–after feasibility study, no follow-up outcome assessments were carried out, and this will be incorporated into the next study when testing effectiveness.
The TUS, USER-P, P-Scale and COPM were all found to be sensitive enough to detect change with this client group and created minimal burden on participants. Despite statistical analysis of the concurrent validity of the TUS and participation measures not being possible, the results from comparing the direction of change on the face of it suggest the links are promising. Further refinement of the outcome measures is warranted, especially as there was no consensus on outcomes or measures in the systematic review.
Limitations
Not achieving the planned sample size prevented further validity testing of the measures of participation. Even so, the sample was reasonable for a feasibility study and provided useful insights into recruitment issues and the burden on the intervention providers. This study prioritised engagement and minimising burden on participants, as guided by the pragmatic perspective. However, this approach has limitations; it reduces the depth of information generated about participants’ experiences of being involved in the study and subsequently the process outcome learning.
Fowler et al. (2009) adapted the TUS (Short 2006); this was not accessible and, whilst similar adaptions were made to the TUS (Short 2006), these may not have replicated those made by Fowler et al. (2009). When analysing the SF-36v2 outcome measure data, it became apparent that there were no norm-based scores for people with a diagnosis of psychosis in the United Kingdom. The norms for the United States general population were utilised, which may have affected the validity of the results. In terms of next steps, a measure for health-related quality of life needs to be explored to include more diagnosis-specific considerations.
Conclusion
Key uncertainties involved in designing a pragmatic clinical trial of individualised occupational therapy with people with a diagnosis of psychosis and occupational need were resolved. The fundamental issue of intervention reporting that conforms to the internationally recognised TIDieR checklist has been overcome; its use will strengthen the methodological quality of a future pragmatic clinical trial (Hoffmann et al., 2014). The analysis of the study process outcome measures also highlighted how a future clinical trial could be bolstered with regard to recruitment, sample size and retention. The indication of effect of this early phase study shows promise; however, further validity testing of the outcome measures is required. Having addressed multiple research design uncertainties, alongside indicators of effectiveness from participants and outcome measure data, a larger pragmatic clinical trial is now warranted.
Key findings
The majority of participants with a diagnosis of psychosis experienced occupational therapy as enabling them to participate more in activities and occupations that were meaningful to them.
What the study has added
POINTER is a valid description of individualised occupational therapy and has been shown to have good utility to support robust reporting of clinical effectiveness research.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank all the service users and staff who were involved in this study from Lancashire Care NHS Foundation Trust and Tees, Esk and Wear Valleys NHS Foundation Trust.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Plymouth University and York St John University.