
Abstract
Introduction
The purpose of this study was to test the feasibility of a telehealth intervention combining computerised cognitive training and occupation-based treatment among adult cancer survivors experiencing cancer-related cognitive impairment.
Method
This was a single-arm study including six cancer survivors with cancer-related cognitive impairment. Participants completed the computerised retraining and functional treatment intervention consisting of 10 hours of computerised cognitive training (BrainHQ) and approximately 10 1:1 remote sessions with an occupational therapist using an occupation-based approach. Feasibility was measured in terms of recruitment, adherence, acceptability and potential effectiveness. Assessments were administered at baseline, post-intervention and at 3-month follow-up and included measures of occupational performance, objective cognitive functions, quality of life and mood questionnaires.
Results
From the nine participants enrolled in the study, six completed 8–13 weeks of computerised retraining and functional treatment intervention and reported high satisfaction levels. Positive and significant improvements were found in occupational performance, useful field of view and social quality of life (all P < 0.05). The positive gains were maintained at the 3-month follow-up.
Conclusion
A combined model of computerised cognitive training and occupation-based treatment delivered remotely to adults with cancer-related cognitive impairment was found feasible and may improve occupational performance, cognitive functions and quality of life.
Keywords
Introduction
Cancer survival rates have increased dramatically in recent years, causing a conceptual shift from an acute illness to a chronic health condition (Phillips and Currow, 2010). Long-term survivors face social, economic, psychological, employment and healthcare issues in addition to secondary effects caused by the treatments (Bray et al., 2018). Cancer-related cognitive impairment (CRCI) is prevalent in up to 75% of survivors from non-central nervous system (CNS) cancers, and is reported as one of the most bothersome symptoms (Lange et al., 2019). The aetiology of CRCI is multi-factorial and includes the direct neurophysiological effects of the cancer and its treatments, as well as the psychological aspects of dealing with cancer, which can lead to anxiety, stress and depression, all known to impair cognition (Vannorsdall, 2017). The nature and severity of CRCI varies between patients, although it is typically mild to moderate, and primarily involves the domains of memory, attention, executive functioning, language and speed of processing (Lange et al., 2019).
To date, computerised cognitive training (CCT) is a main treatment avenue being studied for CRCI that shows sufficient positive evidence to suggest clinical application (Allen et al., 2018). CCT is based on the assumption of neuroplasticity and involves repeatedly practising graded tasks adapted to the individual’s performance. CCT is aimed at improving, maintaining or restoring isolated cognitive functions (Nahum et al., 2013). Although CCT seems to be an acceptable and feasible intervention for improving cognitive and emotional outcomes (Allen et al., 2018), little evidence exists that CCT improves distal cognitive tasks or that it enhances everyday performance (Simons et al., 2016). Indeed, recent cognitive rehabilitation guidelines suggest integrating cognitive training together with individualised goal-directed interventions aimed at promoting occupational functioning (Cicerone et al., 2019). Furthermore, the results of several pilot studies implementing occupation-based treatment among cancer survivors found promising results (Lyons et al., 2018; Newman et al., 2019).
Our study aims to combine CCT with an occupation-based intervention targeting both cognitive and functional outcomes. It utilises the cognitive orientation to occupational performance (CO-OP) approach, a client-centred intervention aimed at enabling meta-cognitive strategy acquisition, generalisation and transfer within an occupational context. The CO-OP has been studied among adults with cognitive impairments (Poulin et al., 2017) and specifically in cancer survivors (Wolf et al., 2016). These studies found significant improvements in occupational performance and quality of life (QoL), as well as cognitive and emotional outcomes following face-to-face CO-OP treatment.
The CO-OP has been further studied using remote delivery in order to broaden the potential impact of the intervention on larger populations and allow for better scalability of the treatment (Beit Yosef et al., 2019). Tele-rehabilitation makes services more accessible to people with chronic health conditions, and provides a pragmatic solution to reduce healthcare cost, time and hospital visits. Many adult cancer survivors with CRCI are engaged in multiple life roles such as parenthood, spousal relationship, employment, and so on, and so receiving treatment that is less time consuming can be of much value for them (Corbett et al., 2018). Thus, we developed computerised retraining and functional treatment (CRAFT), combining CCT and an occupation-based remote intervention programme for adults with CRCI. The aim of the current study is to determine the feasibility of CRAFT and provide preliminary data regarding its potential efficacy in preparation for a large randomised controlled trial (RCT).
Method
Study design
The goal of this feasibility study was to prepare for a larger scale RCT. Therefore, a single-arm quasi-experimental design was applied. Participants (N = 6) received 8–13 weeks of a remote CRAFT intervention. Outcome measures were used to evaluate appropriateness for future study. Outcomes were administered face to face at three time points: baseline (T0) by interventionist, post intervention (T1) and at a 3-month follow-up (T2) by different study personnel to reduce response bias. Baseline, post-intervention and follow-up assessments lasted between 90 and 120 minutes, 60 and 100 minutes and 60 and 90 minutes, respectively. Ethics approval was obtained from the Hadassah Helsinki ethics committee.
Participants and procedure
Participants were recruited from an oncology centre in Jerusalem, Israel. Patients were referred to the study through medical staff who were notified about the study or by response to flyers placed in the waiting room. Interested individuals were screened through their medical records, and eligible individuals were contacted by study staff to schedule a baseline visit. The first meeting included written informed consent, additional screening and baseline assessment.
Inclusion criteria: (a) age 18 years or older; (b) subjective concerns about decline in cognitive functioning related to the diagnosis of cancer and/or cancer-related treatment. This was obtained by providing the answer ‘yes’ to the question: ‘do you have concerns about your memory or other thinking abilities following cancer treatment?’; (c) completion of active treatment for non-CNS cancer between 6 and 60 months prior to recruitment; (d) mild cognitive decline as assessed by the Montreal cognitive assessment (19< MOCA <26) (Nasreddine et al., 2005); (e) daily access to a computer and internet facilities.
Exclusion criteria: (a) unstable psychiatric condition (according to medical file); (b) history of a brain tumour or other severe neurological disorders; (c) pregnancy, due to the assumption that childbirth during the study might disrupt complete participation in the 6-month study protocol.
The CRAFT intervention
The intervention included a combination of two remotely delivered treatments: Computerised cognitive training (CCT): we used five training exercises from the BrainHQ training program by Posit Science; divided attention, target tracker, double decision, freeze frame and eye for detail (www.brainhq.com). To date, BrainHQ has been used in several studies for treating CRCI offering encouraging results (Meneses et al., 2018; Wu et al., 2018). The BrainHQ training suite in the current study targeted the cognitive domains of attention, speed of processing and working memory. Participants logged in using a personal, password-protected login, to start their daily schedule. On each task, training progressed in an adaptive, individualised manner, ensuring that every participant was optimally challenged and that the success rate for each block in a task was about 80%. Study staff were available to troubleshoot any issues that came up during the training. Cognitive orientation to occupational performance (CO-OP): the CO-OP (Dawson et al., 2017) was delivered remotely by video conferencing. We used https://doxy.me, a free, HIPAA-compliant telemedicine platform previously used in clinical research (Bunnell et al., 2020). The initial CO-OP session included information regarding the CO-OP approach followed by education about CRCI. In all following sessions the main executive strategy – goal, plan, do, check (GPDC) was used as the main problem-solving framework to facilitate skill acquisition. After setting each goal, a plan to achieve the goal was formed. Rather than providing the participant with a certain strategy or solution, the therapist facilitated the plan formation process with questions and feedback. Between each session the participant was guided to do the plan. The following session included monitoring the execution of the plan and checking if the plan worked. If the goal was not achieved, the participant and therapist analysed what went wrong and identified a new potential ‘plan’ and the process was repeated (Dawson et al., 2017). Throughout all sessions, the therapist encouraged generalisation of skills and strategies to the natural environment and transfer to novel skills (Houldin et al., 2018). Each participant addressed at least three goals during their participation in the study. In addition, two goals were not addressed (untrained goals), and were used to assess transfer of treatment gains.
The CRAFT intervention was delivered by two occupational therapists (TM and AH) that were CO-OP certified and knowledgeable in the BrainHQ program. Participants were guided to complete 2–2.5 hours per week consisting of three CCT sessions (approximately 25 minutes each) and a single remote CO-OP session (45–60 minutes). The intervention lasted a minimum of 8 weeks or until at least three goals were achieved.
Instruments
Recruitment, retention and adherence
Information regarding the number of eligible participants, recruitment procedure and retention were documented in therapist logs. Adherence was measured separately to the assessment procedure, for CCT and for the CO-OP. Full adherence to the assessment was considered attending three assessment sessions and completion of all questionnaires and tests. Full adherence to the CO-OP included completing a minimum of eight sessions or achieving three goals (Beit Yosef et al., 2019) as documented by the therapist. Completing 8 or more hours of CCT was considered full adherence (Meneses et al., 2018), as was confirmed using data from the log portal.
Acceptability
Satisfaction was measured using a questionnaire designed for the current study and a short interview. The questionnaire addressed general satisfaction, satisfaction from the CCT and the CO-OP sessions, the remote administration, the therapist and the impact the intervention had on their daily life. Items were scored on a five-point Likert scale (1 = strongly disagree, 5 = strongly agree). The interview was used to understand the participants’ experience from the intervention and its implication on their daily lives. The interviews were administered as part of the post-intervention assessment. Participants were asked three open-ended questions: (a) describe positive aspects of the intervention; (b) describe negative aspects of the intervention; and (c) describe changes in your daily life following the intervention. The interviews were audio-recorded and later transcribed.
Potential effectiveness
All outcome measures were administered in validated Hebrew versions.
The Canadian occupational performance measure (COPM) (Law et al., 2014) is a semi-structured interview used to assess performance changes by measuring the clients’ perceived performance and satisfaction with their level of participation rated on a scale ranging from 1 to 10. Higher ratings indicate better performance and increased satisfaction on predefined occupational goals. The COPM is a reliable, valid and responsive tool. A change score of 2 or more points is interpreted as clinically significant (Carswell et al., 2004). The COPM has been used with adults with CRCI (Newman et al., 2019; Wolf et al., 2016).
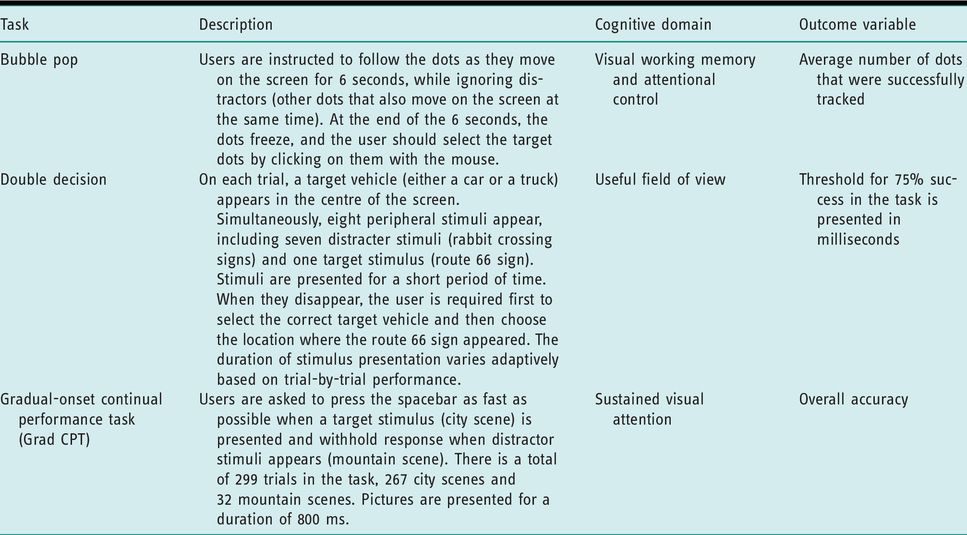
Computerised cognitive assessments (BrainHQ) see Table 1. The functional assessment of cancer therapy – general (FACT-GP) (Cella et al., 1993) is a validated patient reported QoL questionnaire in cancer survivors. The tool consists of 21 statements on which the respondent is asked to think of the previous week and determine his level of agreement on a five-point scale. Higher scores indicate greater QoL. The statements are grouped into four domains with individual scoring and a total score: physical, social, emotional and functional wellbeing.
Computerised cognitive assessments (BrainHQ).
The patient health questionnaire (PHQ-9) (Kroenke et al., 2001) is a widely used self-report screening tool aimed to assess the severity of depressive symptomatology. The nine items in the questionnaire regard the frequency of symptoms within the past 2 weeks and are rated on a four-point scale. The total scores range from 0 to 27, with higher scores indicating a more severe level of depressive symptoms. The PHQ-9 has been shown to perform well in testing depression in cancer patients in a wide range of age and cancer diagnoses (Götze et al., 2020).
The generalised anxiety disorder (GAD-7) (Spitzer et al., 2006) is a standardised self-report measure used for the screening and severity of generalised anxiety disorder. It includes seven items describing the severity of the patient’s anxiety over the past 2 weeks on a four-point scale (each item scored from 0 to 3). The sum score ranges from 0 to 21, with values of 5, 10, 15 indicating mild, moderate or severe anxiety symptoms. The tool is widely used in clinical practice and research among multiple adult populations and is recommended for cancer patients (Plummer et al., 2016).
The ruminative response scale (RRS) (Treynor et al., 2003) is a self-report questionnaire used to assess rumination among adults. The RRS includes 22 items describing responses to depressed mood. Items are rated on a four-point scale (each rated between 1 and 4) with the final scores ranging between 22 and 88, higher scores indicating more rumination.
Data analyses
Descriptive statistics using counts and percentages were utilised to assess recruitment, retention, adherence and acceptability. In addition, satisfaction interviews were transcribed and content analysis was performed. Due to the small sample size, non-parametric statistics were used. Outcome measures were described using medians and interquartile ranges and the Wilcoxon signed rank test was used to analyse potential changes over time (pre-post, post-follow-up). The significance level was set at P < 0.05. In addition, we presented the effect size (ES) of non-parametric statistics: r = z/√n, representing the following magnitude of change: r ≤ 0.10 small ES, r = 0.30 medium ES, r ≥ 0.50 large ES (Fritz et al., 2012). Given the exploratory nature of the current study multiple testing corrections were not performed in the statistical analysis.
Results
Sociodemographic and clinical characteristics
Sociodemographic and clinical characteristics are presented in Table 2. The sample included six participants (five women), whose ages ranged from 41 to 66 years (average 52.8 ± 9.97) all were married. The cancer type varied across participants, as well as the time from active cancer treatment completion (7–33 months).
Participant characteristics, adherence and acceptability (n = 6).
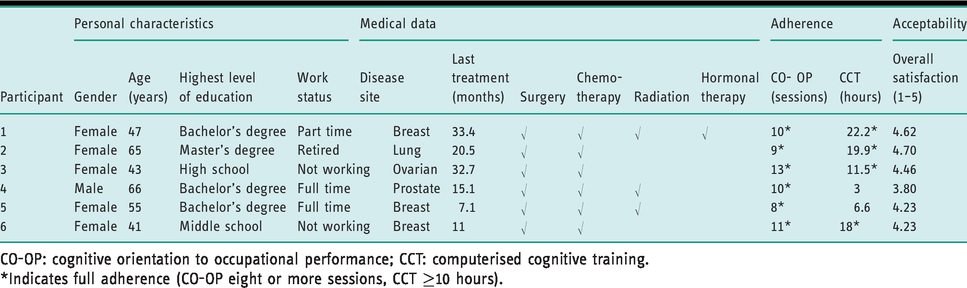
CO-OP: cognitive orientation to occupational performance; CCT: computerised cognitive training.
*Indicates full adherence (CO-OP eight or more sessions, CCT ≥10 hours).
Recruitment, retention and adherence
Study recruitment took place between November 2018 and January 2019 (recruitment rate of three to four participants per month). Figure 1 shows a flow diagram of study recruitment. Thirty-four potential participants were identified. Eleven participants completed the baseline assessment, from which two dropped out before beginning the intervention due to technological difficulty in setting up the intervention. From the nine participants who began the intervention, three dropped out during the process (after 1–4 weeks), therefore the retention rate was 66%. One participant did not complete the follow-up assessment due to return to active cancer treatment. All data were collected according to schedule, indicating full adherence to the assessment procedure. Overall, positive responses to the assessment procedure were noted in the therapist logs. Two participants asked for short breaks during the procedure.
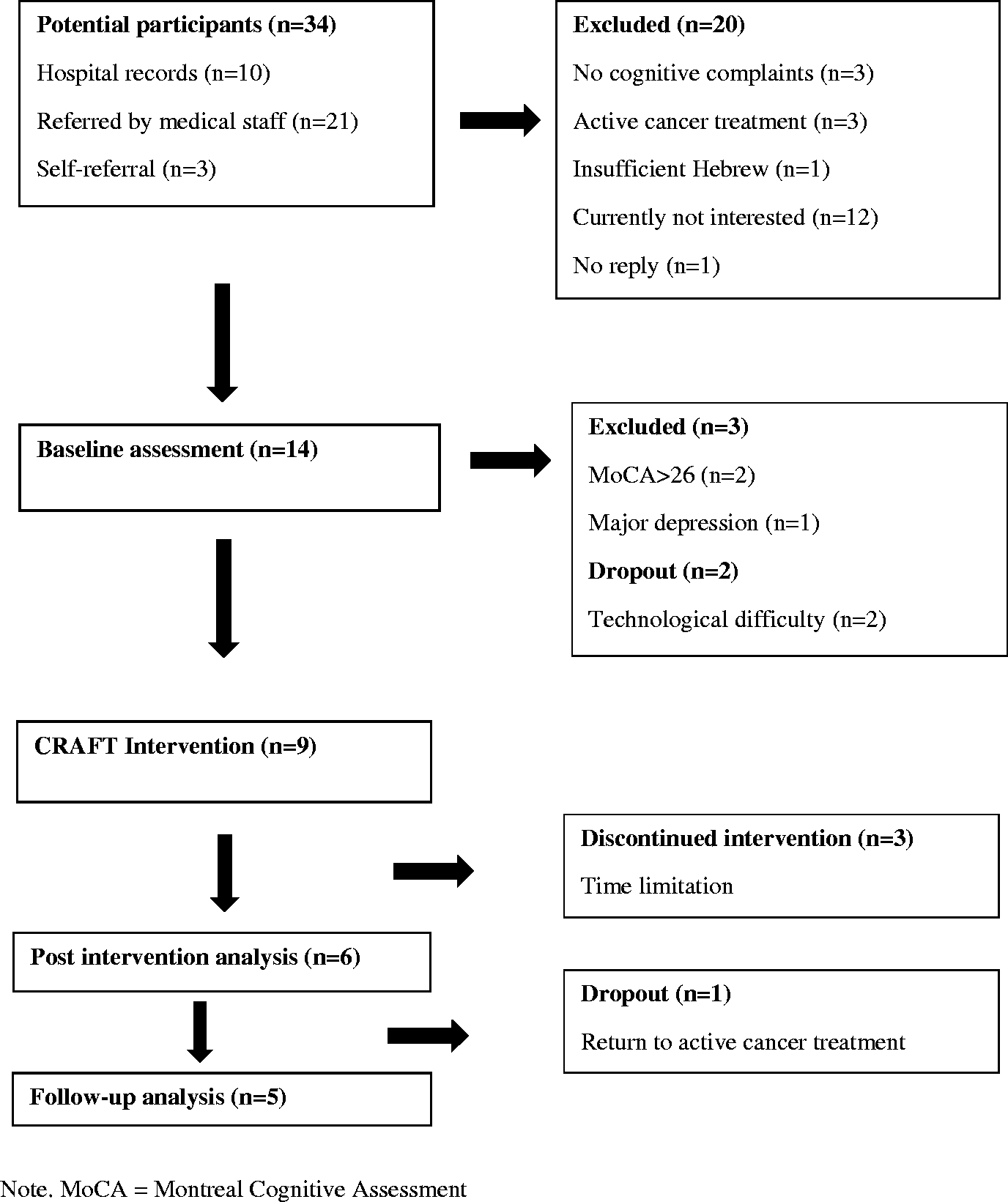
Process flow. MoCA: Montreal cognitive assessment.
Adherence to the CO–OP part of CRAFT was complete, with all six participants completing at least eight sessions or meeting their three goals. Partial adherence was found to the CCT, with four participants completing the minimum required training (10 hours), whereas the other two participants trained for 3 and 6 hours (see Table 2 for adherence and acceptability).
Acceptability
All six participants were highly or very highly satisfied with the intervention in general, with the CO-OP component specifically and with the therapeutic relationship. Four participants were highly or very highly satisfied with the CCT intervention and with the extent to which they felt they cope better with their cognitive challenges following it. Five participants reported high or very high satisfaction with the remote nature of the treatment, and one participant was only moderately satisfied with this aspect. Despite this, when asked if they would have preferred to participate in face-to-face treatment, three participants (50%) answered ‘yes’.
When asked about the positive aspects of the intervention both components of the CRAFT were mentioned: (a) the CCT: participant 2 said: ‘It was very important for me to do the computerised training, it made me work a part of my brain that I didn’t use since I got sick’. Participant 1 stated: ‘I really enjoyed the CCT, I felt myself improving on some of the exercises and that gave me drive to continue…’; (b) CO-OP: participant 3 mentioned: ‘The [CO-OP] sessions were most important for me… I gained many tools and knowledge and can better organise my thoughts’. In addition, participant 5 said: ‘The video calls empowered me… creating a plan [to achieve a goal] was the most important, I feel more self-confident’. In addition, participant 3 noted the importance of the remote intervention for her: ‘It was meaningful for me that the therapy took place in my natural environment…’.
Regarding the challenging aspects of the intervention, two participants mentioned that the CCT was challenging for them to complete: ‘I wasn’t enthusiastic about the CCT, it was hard for me to find the time and I always felt very tired after’ (participant 5), ‘I disliked the computerised exercise with the shapes and the colours’ (participant 1). Two participants felt frustrated about not achieving goals they had set in the CO-OP. Participant 6 mentioned: ‘I had trouble working on a goal that was too big for me, like learning how to use a new computer program’. Participant 4 also expressed his disappointment: ‘I didn’t achieve my goal (regarding sexual activity) and that feels frustrating. In addition, participant 2 felt the time demands of the intervention were hard for her: ‘The scheduling was hard for me, making sure I was home by 7 pm for the phone meeting’.
When participants were asked about changes in their daily life, they mentioned using the global strategy of the CO-OP. For instance, participant 1 said: ‘I decided to work with goals, so I feel like I can achieve any goal set’. Participant 3 stated: ‘I don’t think my memory has changed; it probably won’t till I can sleep better. But I feel more put together, I try to set goals for myself’. In addition, positive changes in daily occupations were mentioned: ‘I feel a shift in my relationship with my spouse because I use our strategy’ (participant 6), ‘I returned to dance with my wife and can remember a movie I have recently watched’ (participant 4). Finally, participants stated a general improvement due to the intervention. Participant 2 stated with enthusiasm: ‘The program brought me back to life’.
Potential effectiveness
Each client set three or four goals that were addressed during the intervention, and at least two goals that were not directly addressed during treatment (untrained goals). In total, 34 occupational goals were set using the COPM at baseline, representing broad occupational domains of self-care (18 goals), productivity (10 goals) and leisure (six goals) (see Table 3).
Participants’ selected goals.
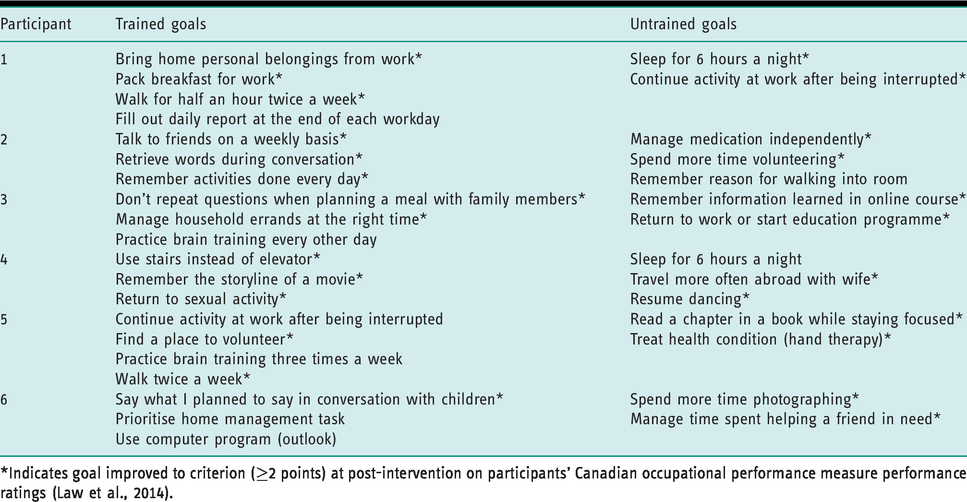
*Indicates goal improved to criterion (≥2 points) at post-intervention on participants’ Canadian occupational performance measure performance ratings (Law et al., 2014).
Table 4 presents the changes in study outcomes at post-intervention assessment. Significant improvements (P < 0.05) were found in performance and satisfaction ratings of both trained and untrained goals. Analysis of clinically significant improvement (CSI) in individual goals revealed that 26/34 (77%) goals improved significantly, with each participant achieving clinically significant gains in 60–83% of their goals (Table 4). Results of the neurocognitive assessments revealed a statistically significant improvement in useful field of view (UFOV) (P < 0.05). A significant improvement was found in the social wellbeing subscale of the FACT-GP. A positive trend was found on sustained attention, emotional and functional wellbeing and all mood measures. No changes were found in visual working memory and physical wellbeing. A comparison of post and follow-up assessment scores revealed no significant differences (all P>0.05). However, COPM trained goals, social wellbeing and mood outcomes show a reduction in median scores. Interestingly, non-trained goals did not show any deterioration between post and follow-up.
Changes over time from baseline to post-intervention and follow-up.
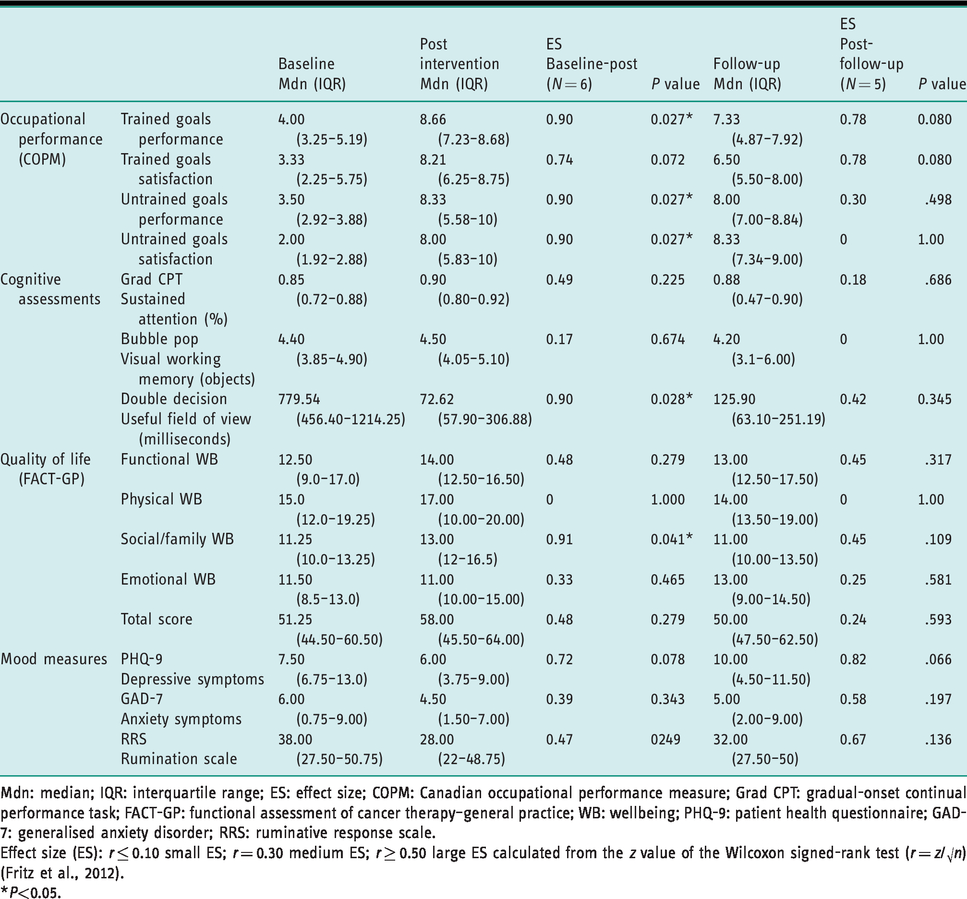
Mdn: median; IQR: interquartile range; ES: effect size; COPM: Canadian occupational performance measure; Grad CPT: gradual-onset continual performance task; FACT-GP: functional assessment of cancer therapy–general practice; WB: wellbeing; PHQ-9: patient health questionnaire; GAD-7: generalised anxiety disorder; RRS: ruminative response scale.
Effect size (ES): r ≤ 0.10 small ES; r = 0.30 medium ES; r ≥ 0.50 large ES calculated from the z value of the Wilcoxon signed-rank test (r = z/√n) (Fritz et al., 2012).
*P<0.05.
Discussion
This feasibility study aimed to assess the feasibility of CRAFT in terms of recruitment, retention, adherence, acceptability and potential effectiveness. The target population was identified easily and expressed interest in treatment. Two-thirds of the sample completed the intervention and were highly satisfied. Furthermore, positive and significant effects were found post-intervention in cognitive, occupational and QoL outcomes. In addition, all positive gains were maintained at the 3-month follow-up. Given the encouraging results we are preparing to conduct a three-armed RCT comparing CRAFT treatment to CCT only and a control group receiving treatment as usual.
Recruitment
Comparing the recruitment rate with other studies is difficult as this study combines two interventions that have not yet been studied together and are delivered in a remote manner. Therefore, we compared the recruitment to similar studies of each intervention separately. The current enrollment rate of about 40% is similar to that found by Von ah et al. (2012) implementing CCT for breast cancer survivors. On the other hand, our rate was much higher than a similar study conducted among breast cancer survivors with CRCI in which only 17 participants were enrolled out of 127 potential participants (Wolf et al., 2016). The main reason for not enrolling in the current study was participants’ lack of interest. It appears that participation in this type of intervention study does not appeal to all cancer survivors with CRCI (Wolf et al., 2016). These recruitment findings can inform the planning of the RCT considering the number of potential participants that need to be contacted in order to reach the target sample size. In addition, we plan to add an option for carrying out assessment procedures in participants’ homes to encourage participation in the study. We believe that meeting participants in their homes might also reduce drop-out rates due to technological difficulties even before the beginning of the intervention (n = 2/5) because it will allow the therapist to help set up the computer or tablet for CCT and video-conferencing.
Retention
We compared the retention rates in the current study (66%) to other studies that employed these interventions separately. Our retention rate is lower than that found for similar studies with a CRCI population using face-to-face CO-OP (82%) (Wolf et al., 2016) and CCT only (77.5%) (Wu et al., 2018). Reasons for withdrawal expressed by participants in the current study were time constraints. Therefore, we conclude that although CRAFT is a remote intervention, which allows one to save travel time and increases accessibility to treatment, it is still conceived as time consuming and requires time and motivational resources of the participants. Following this result, we added to the initial screening a confirmation regarding time availability of at least 2 hours per week.
Adherence
Full adherence was found to assessment procedures except for one participant who was excluded before follow-up due to return to active cancer treatment. This confirmed the feasibility of the assessment battery as well as the schedule. Regarding adherence to treatment we found full adherence to CO-OP sessions and lower adherence (66%) to the CCT schedule. These rates are similar to those found for the remote delivery of CO-OP among adults with acquired brain injury (Beit Yosef et al., 2019), and for CCT among adults with CRCI (70%) (Wu et al., 2018), suggesting that the combination of the treatments did not negatively affect the adherence.
Acceptability
Overall satisfaction with the intervention was high indicating the acceptability of combining CCT with CO-OP in a remote method of delivery. In line with previous studies (Beit Yosef et al., 2019; Wu et al., 2018), remote delivery did not negatively affect the general satisfaction with the intervention. However, some variance was found among participants relating to the different components of CRAFT. In particular, satisfaction with the therapeutic relationship was high, suggesting that developing and maintaining a therapeutic relationship is feasible also in a remote mode of delivery. Moreover, the option to deliver therapy in participants’ real-world contexts supported client centredness. In addition, the use of telehealth was perceived as an advantage, as it was convenient and less time consuming. However, there were some participants who would have preferred face-to-face meetings if this option was provided. We were not surprised that some participants preferred to receive therapy in its traditional face-to-face setting. On the contrary, we were encouraged that 50% of participants were satisfied with the current remote format and would not have chosen otherwise. In addition, we still found full adherence and high satisfaction of those who would have preferred face-to-face meetings, suggesting they found the remote treatment acceptable enough.
We found individual differences regarding the satisfaction and feedback on the CCT. Some participants reported that the CCT was validating of their primary presenting cognitive complaints. Furthermore, for these individuals the CCT can be conceptualised as a meaningful activity in and of itself, providing them with an opportunity to activate their minds (Moll et al., 2015). This suggestion is supported by the amount of time these participants engaged in the training, even beyond the recommended dose. On the other hand, the question regarding satisfaction with the CCT received the lowest score. Participants’ feedback, in line with previous studies (Wu et al., 2018), revealed that some tasks were not enjoyable enough and/or were frustrating. Although the likeability of tasks was not unanimous, in preparation for the RCT we plan to change the tasks that were noted as less enjoyable. This change might also add to the adherence rates to the CCT.
Regarding the CO-OP, very high satisfaction scores were found. Nevertheless, feedback interviews revealed that two participants expressed unachieved goals as a limitation of the intervention. It is possible that the goal-setting process in occupation-based treatment among cancer survivors may also involve a painful realisation of disease-related losses, when the parameters of realistic goals are encountered (Holt et al., 2015; Lyons et al., 2018). This feedback broadens our awareness of the impact of the occupational goal-setting and warrants careful consideration. This issue resonates with the statement of Wade (2009) that ‘the (goal-setting) process needs to establish what changes are at least possible and what changes are not possible, and what would be needed to achieve each goal and how likely the change is’ (p. 293).
Due to the small sample size the potential effectiveness results should be interpreted with much caution. That said, improvement trends were found in several occupational, cognitive and QoL outcomes as well as in mood outcomes. The improvement in COPM after CO-OP using telehealth for cancer survivors is encouraging and matches that of recent adult CO-OP studies (Beit Yosef et al., 2019; Wolf et al., 2016). Interestingly, the positive change in the transfer goals (that were not explicitly targeted in the intervention), were larger than the trained goals, and were fully maintained at follow-up. This finding supports the contention that the CO-OP includes metacognitive processes that transfer to novel contexts (Houldin et al., 2018). In a similar vein, the significant improvement in the social wellbeing in the QoL measure, a distal outcome, can be conceptualised as additional support of the transfer effect of the treatment (Houldin et al., 2018).
The results of the cognitive assessments at post-intervention and at follow-up showed significant improvements in UFOV as well as a clinically significant change from the severely impaired to the normative range. The improved performance in UFOV found in this study is in congruence with the literature on neuroplasticity-based cognitive training (Nahum et al., 2013). In particular, the current findings are in line with the evidence that 10 hours of training might be a sufficient dose for improving UFOV (Meneses et al., 2018).
The current study examined the combined effect of CCT and CO-OP. Given this design, it is not possible to tease apart the unique contribution of each component to the positive outcomes. However, it is possible that combining two interventions may have had a synergistic effect, as suggested by Wolf et al. (2019), who combined CO-OP with task-specific training. We suggest that with therapeutic guidance, the CCT can be harnessed as a client-centred treatment tool which may promote self-efficacy and self-awareness, that in turn has the potential to enhance goal attainment and strategy use. For example, one participant mentioned that: ‘after experiencing challenges in the visual attention task on the CCT, I understand the risks of driving. I think driving safely should be the next goal we work on together’. These insights are facilitated by the integrative therapeutic context, whereby the therapists intentionally link between the experiences during the CCT and occupational performance. Further controlled studies are needed to compare between CRAFT and its individual components in order to gain a deeper understanding of the active ingredients of these interventions.
Study limitations
This study has several limitations. Firstly, the sample was small and diverse, particularly in relation to cancer types and treatments. In preparation for the future RCT, the study would have benefited from separating the CCT from the CO-OP, in order to examine the unique versus combined contribution of each treatment component. This limitation also prevented us from examining the feasibility of the randomisation procedure to different treatment arms. Finally, we did not assess subjective ratings of cognitive impairments. Using the FACT-Cog instrument, which was designed for this population (Wagner et al., 2004), would have added value, as a significant client-centred outcome measure on broad cognitive functioning, beyond specific occupational goals.
Conclusion
This feasibility study supported the use of CRAFT among adults with CRCI in terms of recruitment, adherence and acceptability. Potential effectiveness was found for occupational performance, UFOV and QoL. Despite the well-established critique of cognitive remediation in occupational therapy literature for lacking transfer to daily life (Gillen et al., 2019), we found that the use of bottom-up treatment, combined with an occupation-based approach, might have worthy therapeutic benefits. These results will inform modifications in the design of a full-scale controlled trial.
Key findings
A combined model of computerised cognitive training and cognitive orientation to occupational performance delivered remotely to adults with cancer-related cognitive impairment was found to be feasible. Significant positive effects were found for computerised retraining and functional treatment on occupational performance, useful field of view and quality of life. The need for a large-scale controlled trial is warranted to test the efficacy of computerised retraining and functional treatment.
What this study adds
Findings from this study indicate that computerised retraining and functional treatment seems to be a feasible and ecological treatment option for adults living with cancer-related cognitive impairment.
Footnotes
Research ethics
Ethical approval was obtained from Hadassah Helsinki committee board on February 26, 2018 (protocol no. 0138-18-HMO).
Consent
All participants provided written informed consent to participate in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Funding for this project was received from the Israel Cancer Research Fund (ICRF) and the Israel Cancer Association (#20191362).
Contributorship
Yafit Gilboa, Mor Nahum, Chen Makranz, Tamar Peretz and Nechama Silberman were responsible for the study conception and design. Chen Makranz and Talia Maeir applied for ethical approval. Talia Maeir, Afik Hoba and Shai Netanel Nagary were responsible for ongoing study procedure, participant recruitment, treatment, and data management. Talia Maeir was primarily responsible for data analysis and drafting the manuscript with support from Yafit Gilboa. All authors critically reviewed the manuscript for content and style and approved the final version of the manuscript for submission.