
Abstract
Research suggests that multimodal programs may support positive outcomes among perpetrators of intimate partner violence (IPV), extending beyond recidivism reduction to improvements in emotional regulation and relationship skills. However, few studies have examined their impact on underlying factors associated with IPV perpetration, such as aggression. This study aims to explore the impact of the Promotion and Intervention Program with Batterers (PPRIAC) on aggression and its components (i.e., physical and verbal aggression, anger, and hostility). A sample of 55 male IPV perpetrators in Portugal was assigned to one of two conditions: the intervention condition (IC; n=38) and the waiting list control condition (WLCC; n =17). Self-reported aggression was assessed at baseline, post-test, and at a 6-month follow-up. Participants in the IC showed clinically significant reductions in overall aggression and all aggression components from baseline to post-test. These gains were maintained at the 6-month follow-up, with a further reduction in physical aggression. Moreover, the IC demonstrated significantly greater reductions in aggression than the WLCC at both pos-test and follow-up. These findings emphasize the effectiveness of the multimodal intervention program in reducing aggression among IPV perpetrators and influencing specific factors associated with IPV.
Plain Language Summary
Intimate partner violence (IPV) is a serious issue, and programs that address different needs, called multimodal programs, have been shown to help reduce repeat offenses. However, we still know little about how these programs affect specific behaviors, like aggression, which often play a role in IPV. This study looked at whether a specific multimodal intervention—the Promotion and Intervention Program with Batterers—could help reduce aggression in men who had committed IPV. A total of 55 men took part. Some received the intervention (38 men), while others were placed on a waiting list and did not receive the program during the study (17 men). Participants completed questionnaires about their aggression before the program, right after it ended, and again six months later. The men who took part in the intervention showed a significant drop in all types of aggression, such as physical aggression, anger, and hostility. These improvements lasted for at least six months, and physical aggression dropped even further over time. Importantly, men in the intervention group showed significantly greater reductions in aggression than those in the waiting list group at both the end of the program and the six-month follow-up. These results suggest that the multimodal intervention was effective in helping reduce aggression in IPV perpetrators. By addressing aggression, the program may help lower the risk of future violence.
Keywords
Introduction
Intimate partner violence (IPV) is a significant public health concern that transcends all settings and affects diverse socioeconomic and cultural groups (World Health Organization [WHO], 2023). IPV affects millions of people each year (Sardinha et al., 2022), with women disproportionately impacted, as nearly one in three women worldwide have experienced physical and/or sexual violence by an intimate partner at least once in their lifetime (WHO, 2021). In Portugal, where the present study was conducted, the most recent Annual Homeland Security Report documented 30,221 police-reported domestic violence incidents in 2024 (Sistema de Segurança Interna, 2024). In addition, a study by Capinha et al. (2022) using self-report measures found a past-year IPV victimization prevalence of 64.4% and a lifetime prevalence of 74.6%.
IPV has serious psychological and physical consequences for victims and their families, both in the immediate aftermath and over the long term (Stubbs & Szoeke, 2022). Given its severity and widespread impact, addressing IPV is a public health priority. Secondary and tertiary prevention programs, in particular, are recognized as crucial for reducing harm and mitigating long-term consequences (Breiding et al., 2014; Caridade et al., 2021).
Perpetrator intervention programs (PIPs) align with the critical prevention efforts needed to mitigate IPV. However, ongoing debate persists regarding their overall effectiveness (e.g., Arce et al., 2020; Babcock et al., 2024; Wilson et al., 2021). Recent research suggests that for PIPs to effectively reduce future IPV, they must implement strategies that enhance participant retention and promote long-term change (Friedman et al., 2022; Velonis et al., 2016). In line with this, the present study aims to examine the effectiveness of a multimodal intervention program in addressing aggression—including physical and verbal aggression, anger, and hostility—among IPV perpetrators in Portugal.
Perpetrator Intervention Programs
Given the extensive impact of IPV, the need to prevent it, and the necessity to improve victims’ safety, multiple penal measures (e.g., arrest and prosecution policies; protective and restraining orders; incarceration and probation; court-mandated perpetrator intervention programs) have been introduced. PIPs are amongst one of the most popular penalties to deal with IPV (Cunha & Caridade, 2023; Murphy & Richards, 2022). PIPs are designed to address IPV by aiming to reduce recidivism and promote victim safety (Cunha & Caridade, 2023). These programs focus on changing pro-violent and irrational thinking, increasing awareness of gender roles, and improving communication and conflict resolution skills. Over the years, PIPs have undergone significant changes in both their underlying philosophy and intervention approaches (Cannon et al., 2016). One of the earliest initiatives was the Duluth model, which conceptualizes IPV as rooted in patriarchal structures and male socialization processes (Pence & Paymar, 1993). Within this framework, violence is regarded as a means by which men assert dominance and maintain control over their partners (Pence & Paymar, 1993). As a result, Duluth-inspired interventions adopted a gender-based perspective, most often delivered through psychoeducational strategies designed to confront and transform men’s beliefs and attitudes toward women (Butters et al., 2021; Gannon et al., 2019). Although predominantly educational, the Duluth model also integrated cognitive-behavioral elements (Bohall et al., 2016). Later, cognitive-behavioral therapy (CBT) emerged as an alternative, aiming to reduce aggression by addressing hostile cognitive biases, strengthening emotional regulation, and fostering interpersonal skills such as assertiveness, communication, and problem-solving (Beck, 1970; Butters et al., 2021; Cunha & Caridade, 2023).
There is a plurality of PIPs. Specifically, a study conducted in the USA and Canada identified 238 PIPs, the majority of which were delivered in group format. Among the 238 PIPs, approximately one-third followed the Duluth model, and another third used the CBT approach (see Cannon et al., 2016). Data from recent systematic reviews covering programs at the international level have reinforced that approaches based on the Duluth Model and CBT are the most prevalent (see Arce et al., 2020; Gannon et al., 2019; Sousa et al., 2024).
However, research has shown that PIPs yield inconsistent results regarding their effectiveness in reducing IPV (e.g., Babcock et al., 2024; Karakurt et al., 2019; Travers et al., 2021). Some meta-analyses indicated that, while PIPs produce changes, the effect sizes were small (Arce et al., 2020; Wilson et al., 2021) or medium (Fernández-Fernández et al., 2022; Gannon et al., 2019). Moreover, statistically significant effects emerged only in the studies by Arce et al. (2020) and Gannon et al. (2019). When analyses focused on specific intervention approaches, the evidence remained inconsistent. For instance, Babcock et al. (2004) and Gannon et al. (2019) found that the Duluth Model was associated with significantly larger, medium-range effects, while Arce et al. (2020) reported that CBT yielded higher effect sizes than other therapeutic modalities, suggesting greater effectiveness. More recently, Babcock et al. (2024) found that interventions such as Acceptance and Commitment Therapy (ACT) and Circles of Peace demonstrated the largest effect sizes when directly compared to Duluth Model groups. It is important to note that early studies often reported more promising results, whereas more recent evaluations, which employ stricter methodologies such as randomization and control groups, tend to show smaller effects (e.g., Cheng et al., 2019).
Furthermore, these inconsistent findings may be partially explained by the fact that traditional intervention models often fail to address key individual and contextual factors associated with IPV perpetration, such as lack of motivation, mental health issues, and core underlying mechanisms like emotion dysregulation, aggression, anger, or hostility (Babcock et al., 2016, 2024; Cunha & Caridade, 2023). Importantly, these factors are also recognized as significant risk factors for IPV recidivism (McDonagh et al., 2025). In fact, IPV is a complex and multidimensional phenomenon shaped by individual characteristics, relational dynamics, and broader contextual influences (Cunha et al., 2022; Kaufman-Parks et al., 2023). Accordingly, effective PIPs must be tailored to reflect this complexity and respond to the specific needs of IPV perpetrators (Cunha & Gonçalves, 2013; Hilton & Radatz, 2018; Radatz & Hilton, 2025; Radatz & Wright, 2015). In line with the Principles of Effective Intervention (PEI)—specifically the Risk-Need-Responsivity (RNR) model (Bonta & Andrews, 2023; Radatz et al., 2021; Radatz & Hilton, 2025; Radatz & Wright, 2015)—such programs emphasize treatment over punishment and target criminogenic needs, or those factors most closely linked to criminal behavior, including aggressive tendencies, poor emotional regulation, and limited problem-solving skills (Bonta & Andrews, 2023). PIPs that specifically address criminogenic needs—such as anti-social personality, attitudes/values, anti-social behavior, family dysfunction, substance abuse, and poor self-control/problem-solving skills–have demonstrated promising outcomes (Friedman et al., 2022). Supporting this, a meta-analysis by Travers et al. (2021) found that RNR-based treatments for IPV perpetrators showed positive effects in the short-to-medium term.
Additionally, research suggests that integrating various therapeutic approaches may enhance program effectiveness (Bates & Graham-Kevan, 2020). This is supported by a robust body of literature (e.g., Berghuis, 2018; Zarling & Russell, 2022) highlighting the effectiveness of multimodal interventions—that is, programs that integrate multiple therapeutic methods to address diverse goals and treatment targets. These approaches have been shown not only to reduce recidivism (the primary intent of PIPs) but also to improve additional outcomes (e.g., self-esteem, acceptance of personal responsibility for violence; Capinha et al., 2023; Cunha, Silva et al., 2023; Friedman et al., 2022). Motivational interviewing techniques (MIT) have also been incorporated into multimodal programs, given that readiness and motivation to change are well-established predictors of treatment effectiveness among IPV perpetrators (e.g., Pinto e Silva et al., 2023; Santirso et al., 2020). The integration of MIT has demonstrated promising results in enhancing the overall effectiveness of intervention programs (see Pinto e Silva et al., 2025).
Perpetrator Intervention Programs and Aggression
Aggression is commonly defined as a behavioral tendency characterized by social dominance, threatening actions, and hostility, which may manifest as a stable personality trait in some individuals (American Psychological Association [APA], 2018). Building upon the critical role of individual risk factors highlighted in the RNR model, the literature underscores that components of aggression—namely physical and verbal aggression, anger, and hostility—understood as a broader psychological construct, not only serve as predictors (Clements et al., 2018) but also function as mediating mechanisms in IPV perpetration (Cunha, Cruz et al., 2023). For instance, individuals who exhibit hostility in their interpersonal interactions, particularly with friends and partners, are more likely to report engaging in IPV perpetration (Vagi et al., 2013). A substantial body of research (e.g., Cunha, Cruz et al., 2023; Eckhardt et al., 2008) consistently supports the association between aggression and IPV perpetration, with numerous studies indicating a higher prevalence of trait aggression among IPV perpetrators (e.g., Clements et al., 2018; Cunha, Cruz et al., 2023; Cunha et al., 2021). Additionally, IPV perpetrators often demonstrate elevated levels of hostility and anger (Eckhardt et al., 1997; Norlander & Eckhardt, 2005; Ontiveros et al., 2023; Stith et al., 2004). These findings are further reinforced by evidence showing that both anger and hostility are reliably linked to IPV perpetration (e.g., Birkley & Eckhardt, 2015; Dannisworo et al., 2019; Eckhardt et al., 1997; Stith et al., 2004) and IPV recidivism (Lila et al., 2019; McDonagh et al., 2025). Specifically, physical aggression has been identified as a mediating factor in the pathway from exposure to interparental violence to IPV perpetration (Cunha, Cruz et al., 2023).
From a theoretical standpoint, General Strain Theory (GTS; Agnew, 2006) offers a complementary framework for understanding how certain life stressors may contribute to IPV perpetration. GST posits that individuals exposed to significant strains—such as financial hardship, substance use, jealousy, or interpersonal conflict—are more likely to experience negative emotional states, particularly anger and frustration. These emotions can overwhelm an individual’s coping resources and increase the likelihood of maladaptive responses, including aggression and IPV (Cunha et al., 2024; Graham et al., 2022). This theoretical framing is particularly relevant to PIPs, as it highlights the importance of addressing both the emotional and contextual precursors to violence—an approach that aligns with RNR’s emphasis on tailoring interventions to individual needs and responsivity (Bonta & Andrews, 2023). Integrating GST into the understanding of IPV perpetration strengthens the rationale for interventions that move beyond behavior modification to include emotion regulation, stress management, and problem-solving strategies as key components of treatment.
Given the robust empirical and theoretical links between aggression-related traits and IPV perpetration—either as a direct mechanism or a mediating factor (Cunha, Cruz et al., 2023)—there is a compelling need to integrate strategies into PIPs that enhance emotional recognition and regulation, problem-solving, and adaptive coping skills (Friedman et al., 2022). Strengthening these skills may assist individuals with higher aggression traits in regulating and expressing their cognitions and emotions more adaptively, ultimately reducing IPV (Cunha, Cruz et al., 2023). These considerations highlight the need to include such psychological variables as key indicators of both intervention success and behavioral change.
Current Study
The present study examines the effectiveness of a multimodal intervention program, implemented in Portugal, that incorporates CBT, psychoeducational strategies, and MIT in addressing aggression, including physical and verbal aggression, anger, and hostility, among individuals engaged in IPV. This research holds significant importance for several reasons. Firstly, the effectiveness of interventions for IPV perpetrators is a subject of ongoing debate, with conflicting findings in the literature (e.g., Arce et al., 2020; Cheng et al., 2019; Fernández-Fernández et al., 2022; Wilson et al., 2021). Therefore, evaluating interventions employing distinct approaches and techniques (e.g., CBT, MIT, and psychoeducational strategies) is crucial, given evidence suggesting their substantial impact on changing violent behaviors (e.g., Cunha, Almeida et al., 2023; Cunha, Silva et al., 2023; Friedman et al., 2022; Murphy & Richards, 2022). Secondly, while most studies evaluating intervention effectiveness tend to focus primarily on outcomes such as recidivism or reassault reduction (Friedman et al., 2022; Velonis et al., 2016), they often overlook the mechanisms that drive behavioral change (e.g., beliefs supportive of IPV, responsibility for violence, problem-solving skills; Cunha, Almeida et al., 2023; Cunha, Silva et al., 2023; Friedman et al., 2022; Skeem et al., 2009) align with the RNR model (Bonta & Andrews, 2023). Recent literature has highlighted the need to address the underlying factors contributing to IPV perpetration (Velonis et al., 2016) and to better understand the processes that support behavioral change (Skeem et al., 2009). In addition, emphasis has been placed on the importance of addressing the diverse needs of perpetrators and measuring more immediate changes—such as shifts in attitudes and the development of interpersonal skills—which offer valuable insight into the change process and into key variables associated with reduced recidivism (e.g., Friedman et al., 2022; Misso et al., 2019; Murphy & Richards, 2022; Velonis et al., 2016). Additionally, there is a dearth of studies in Portugal assessing the effectiveness of programs that integrate CBT, psychoeducational strategies, and MIT in addressing IPV and its impact on aggression and its components (e.g., Karakurt et al., 2019; Sousa et al., 2024).
The primary aim of this study is to examine whether a multimodal intervention program—the Promotion and Intervention Program with Batterers (PPRIAC; Cunha, Almeida et al., 2023; Cunha & Gonçalves, 2015; Cunha, Silva et al., 2023)—results in changes in aggression among IPV perpetrators. Specifically, the study examines variations in physical and verbal aggression, anger, and hostility, and assesses changes in individual scores over time by computing the Reliable Change Index (RCI).
Method
Participants
The study's sample consisted of 55 male IPV perpetrators, either court-referred or voluntarily participating in a community-based PIP in Portugal (e.g., Cunha et al., 2022; Cunha, Almeida et al., 2023; Cunha & Gonçalves, 2015; Cunha, Silva et al., 2023). Inclusion criteria consisted of adult males who had perpetrated criminal acts (e.g., physical, sexual, psychological violence) against a female intimate partner or ex-partner and possessed the ability to read and write. Exclusion criteria included individuals with psychotic disorders, cognitive impairments, psychological or personality disorders, or substance use disorders, as determined through a review of each individual’s case file (when available)—including clinical records—and information gathered during the clinical screening interview.
The participants had an average age of 45.07 years (SD = 11.26), ranging from 23 to 63. Most were married or cohabited with the victim at the time of the intervention (n = 29, 52.7%), with an average relationship length of 18.95 years (SD = 12.15). Most participants completed the 4th grade (n = 16, 29.1%) or the 6th grade (n = 18, 32.7%). All the individuals identified as Caucasians. More than half of the participants (56.4%, n = 31) were self-referred. This group of participants included individuals referred by child protection services or family support agencies who chose to attend the intervention voluntarily (n = 19; 61.3%), as well as those who sought help on their own initiative (n = 12; 38.7%). The majority had no previous criminal record (n = 51, 92.7%). The groups demonstrated similarity across all sociodemographic and juridical variables. Table 1 provides a concise overview of the main sociodemographic and juridical characteristics of the participants.
Sociodemographic and Juridical Characteristics.
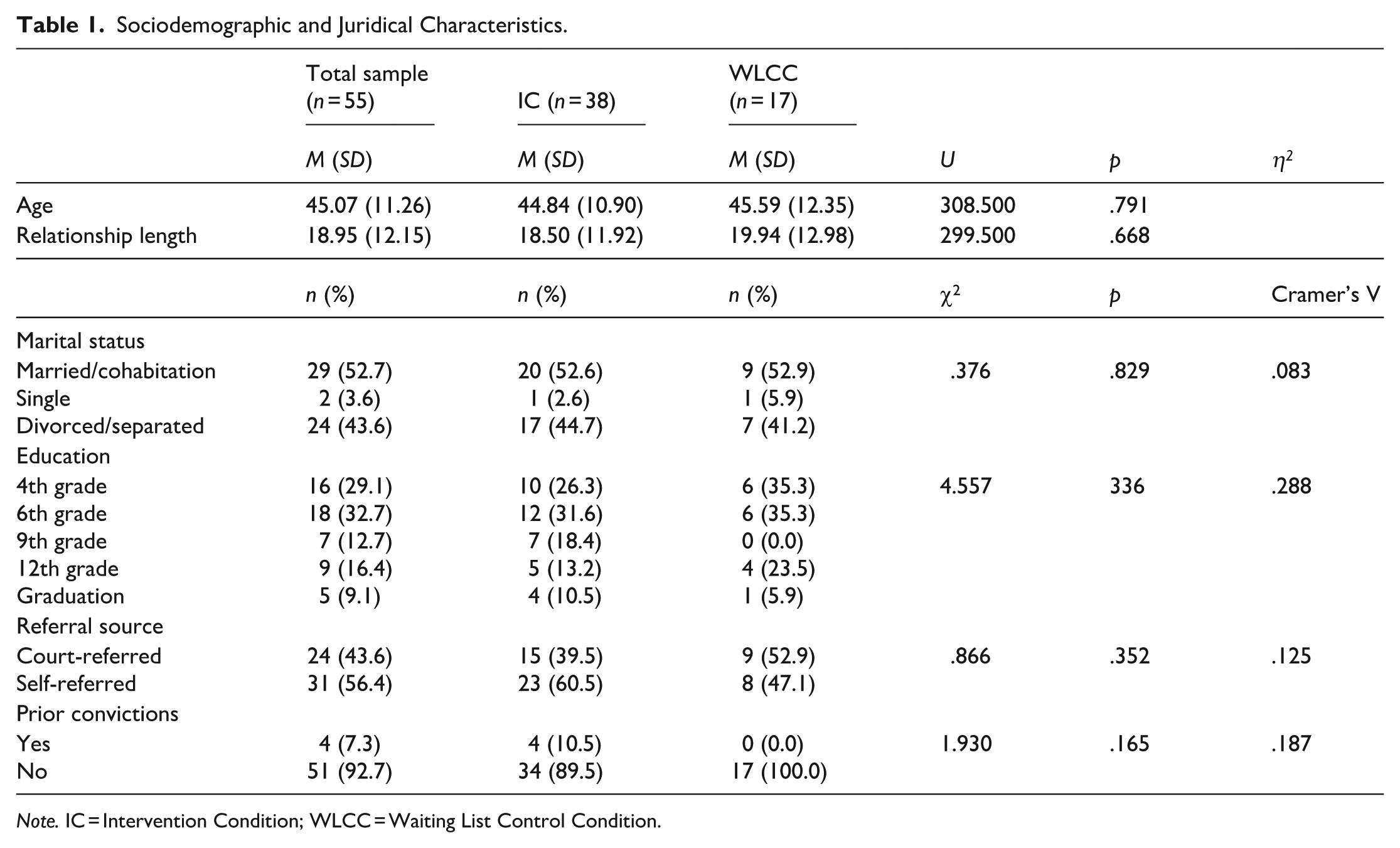
Note. IC = Intervention Condition; WLCC = Waiting List Control Condition.
Procedures
The intervention took place at the Psychology Service of the University of Minho, with participants referred to by various institutions such as the court, child protection services, victim support, family support institutions, probation services, or self-referral.
Potential participants underwent a clinical screening interview, during which all procedures were thoroughly explained, emphasizing their voluntary nature. Those meeting the inclusion criteria—excluding individuals with severe mental illness, cognitive impairment, personality disorder, or substance use disorders—received invitations to participate. Ten individuals declined to join the study. Participants who agreed to take part signed an informed consent and completed a set of psychological measures. No incentives or compensation were provided.
Participants were then assigned to either the intervention condition (IC; n = 38), receiving the immediate intervention, or the waiting list control condition (WLCC; n = 17), placed on a waiting list with access to the intervention in one year. This allocation followed a 2:1 ratio determined by the order of referral to the program. Participants in the WLCC who were court-ordered received the standard treatment provided by the Portuguese Prison System. Five intervention groups were formed to deliver the group-based treatment intervention.
The choice for a waiting list design aimed to ensure that all eligible participants could eventually benefit from the intervention, while allowing for a non-intervention assessment (Cunningham et al., 2013). A 2:1 ratio was preferred to maximize intervention access, considering the potential positive impact on victims' safety. Data were collected at three points: pre-test (beginning of the intervention), post-test (end of the intervention), and follow-up (six months after the intervention). Participants individually completed instruments in a paper-and-pencil format under the supervision of a psychologist. In the IC, 10 participants dropped out from pre- to post-test, and four from post-test to follow-up; in the WLCC, one participant dropped out from pre- to post-test, and three from post-test to follow-up.
Ethical procedures regarding data protection, as established by Portuguese legislation and the Helsinki Declaration, were strictly adhered to. The study received approval from the Subcommittee on Ethics of Social and Human Sciences at the University of Minho.
Instruments
A Sociodemographic and Juridical Questionnaire was used to collect data on the main sociodemographic (e.g., age, educational level, marital status, socioeconomic level) and juridical variables (e.g., recidivism, referral source). This information was primarily gathered through self-report, with some data also verified against the official record whenever available. In cases where information from the two sources did not match, the official record was used. This data was collected at the intake and updated in the posterior assessments.
The Buss and Perry Aggression Questionnaire (BPAQ) (Buss & Perry, 1992; Cunha & Gonçalves, 2012) is a self-report comprising 29 items designed to assess aggression. Respondents rate items on a 5-point Likert scale, ranging from 1 (extremely uncharacteristic of me) to 5 (extremely characteristic of me). The BPAQ provides an aggregate measure of overall aggression and evaluates four distinct dimensions of aggression: Physical Aggression (e.g., “I have threatened people I know), Verbal Aggression (e.g., “I can’t help getting into arguments when people disagree with me”), Anger (e.g., “I flare up quickly but get over it quickly”), and Hostility (e.g., “I wonder why sometimes I feel so bitter about things”). A higher score indicates elevated levels of aggression. Both the original and the Portuguese adaptation of the BPAQ have demonstrated good psychometric properties. In the present study, the pre-test exhibited internal consistency values of .82 for the total scale, .65 for physical aggression, .47 for verbal aggression, .71 for anger, and .64 for hostility. For the post-test, these values were .86 for the total scale, .74 for physical aggression, .58 for verbal aggression, .70 for anger, and .71 for hostility. At follow-up, the internal consistency was .88 for the total scale, .72 for physical aggression, .52 for verbal aggression, .80 for anger, and .81 for hostility.
The Intervention Program
The PPRIAC was created in 2010 to address adult heterosexual male IPV perpetrators, whether self-referred or court-referred (Cunha, Almeida et al., 2023; Cunha & Gonçalves, 2015; Cunha, Silva et al., 2023) (NCT05484440).
The program is manualized and follows a multilevel structure, addressing different intervention needs in a specific sequential order to ensure that participants progress through each stage of the intervention as intended. It includes four to six individual sessions (60 minutes each) and 18 group sessions lasting between 90 to 120 minutes (depending on how the session unfolds and the participants’ progress toward meeting the objectives established for each session), delivered weekly over a period of 22 to 24 weeks. The program adopts a multimodal approach, since it integrates MIT (Miller & Rollnick, 2022), CBT (Beck, 1970), and psychoeducational techniques (Cunha & Gonçalves, 2011, 2015), addressing different needs and outcomes (e.g., attitudes and beliefs supportive of IPV, communication and problem-solving skills, self-management and coping strategies, decision making, development of positive intimate relationships, end/reduce IPV). The PPRIAC aligns with the principles of the RNR model by targeting criminogenic needs as identified by Bonta and Andrews (2023). These include procriminal attitudes (e.g., attitudes and beliefs supportive of IPV), antisocial personality patterns (e.g., development of problem-solving, self-management, anger management, and coping skills), and marital factors (e.g., reducing IPV and fostering positive intimate relationships). The program also addresses participant responsivity by incorporating evidence-based approaches such as CBT and MIT, and by applying a defined set of inclusion and exclusion criteria. Additionally, the program adheres to the risk principle, as it is specifically designed for individuals with low to moderate risk of recidivism. Its primary objectives include (a) cessation of abusive behavior towards women, (b) taking responsibility for such behavior, (c) modifying irrational beliefs and attitudes related to IPV, (d) fostering respect for women and encouraging healthy relationships, (e) developing personal and social skills, and (f) promoting a violence-free approach to problem-solving. Various therapeutic techniques, such as cognitive restructuring, the ABC model, self-instructions, assertiveness and communication skills training, and problem-solving training were implemented. Additionally, a range of methods, including role-play, homework assignments, videos, power and control wheel, equality wheel, and brainstorming were utilized.
The individual sessions, conducted prior to the group sessions, were grounded in MIT and aimed to enhance motivation for change. The subsequent group sessions were designed using a collaborative framework that encouraged active participant engagement. Each session adheres to a structured format: (a) revaluation, involving a recap of the most significant elements from the previous session and the past week; (b) reflexive activity, which encouraged participants to engage in exercises related to the session’s theme; (c) reflection/content exposure; and (d) finalization, highlighting the positive aspects and takeaways from the session (Cunha & Gonçalves, 2015). The individual sessions were conducted by a single therapist—consistently the same professional for each participant—while the group sessions were facilitated by a team of two therapists. The therapist who led the individual sessions also participated in the group sessions, ensuring continuity and building the therapeutic rapport. All therapists were trained in interventions with IPV perpetrators (see Cunha & Gonçalves, 2011, 2015).
Data Analysis
Statistical analysis was conducted using SPSS version 29. Baseline comparisons between the intervention (IC) and waiting list control conditions (WLCC) were performed using Mann-Whitney tests. Within-group differences in outcome measures at post-treatment and follow-up were assessed using Wilcoxon tests. Mann-Whitney tests were used to compare the two conditions at post-test and follow-up. Effect sizes were determined through Eta Squared (η2).
Intra-subject clinical change was evaluated using the Reliable Change Index (RCI) developed by Jacobson and Truax (Jacobson & Truax, 1991). Individuals with scores exceeding .84 were categorized as experiencing "global improvement" (GI), those with scores below -.84 were classified as belonging to the "global deterioration" (GD) group, and individuals with scores between these values were assigned to the "no change" (NC) category (Brazão et al., 2015). Chi-square tests were employed to compare the groups in clinical change categories, and effect sizes were computed using Cramer's V.
Results
Baseline Assessment
Results revealed that groups did not differ in the main variables, except for the subscale physical aggression of BPAQ (see Table 2).
Baseline Differences in Aggression (Physical and Verbal Aggression, Anger, and Hostility).
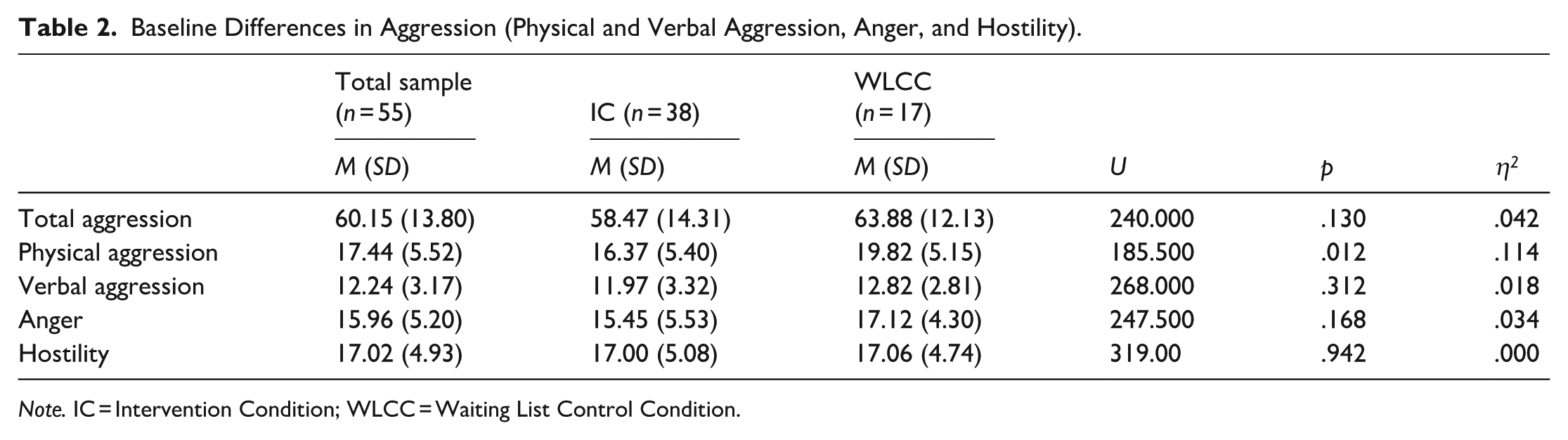
Note. IC = Intervention Condition; WLCC = Waiting List Control Condition.
Post-Test Assessment
Results regarding post-test analysis for IC and WLCC are displayed in Table 3.
Within-Group and Between-Group Analyses of Change in IC and WLCC at Post-Test.
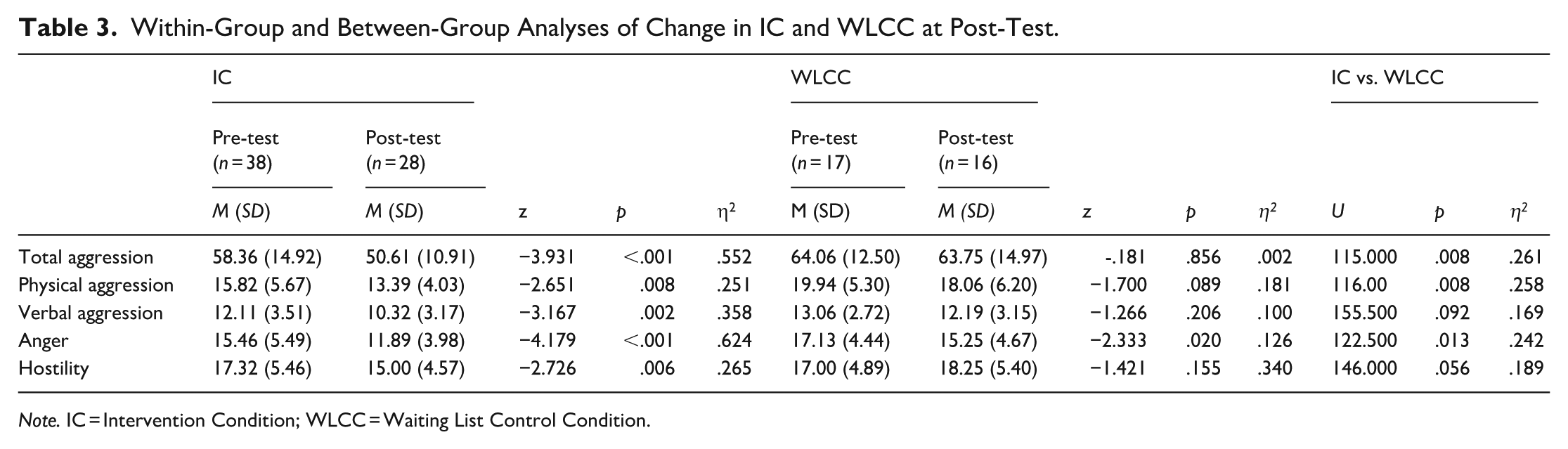
Note. IC = Intervention Condition; WLCC = Waiting List Control Condition.
Twenty-eight participants of the IC completed at least 75% of the intervention program sessions, indicating a success rate of 73.7% and a dropout rate of 26.3%. Individuals who dropped out attended an average of 7.88 (SD = 3.76) sessions, including both individual and group sessions. No other differences were found between dropouts and completers (see supplementary files).
IC participants revealed a significant decrease in overall aggression and its components, namely physical and verbal aggression, anger, and hostility, with large effect sizes. In WLCC, no significant differences were found, except for anger. Comparing both conditions, results also showed significant differences in overall aggression, physical aggression, and anger, with large effect sizes. Marginal differences were found between IC and WLCC participants in verbal aggression and hostility. IC participants revealed the lowest scores.
Follow-Up Assessment
Follow-up results are presented in Table 4. In general, the results showed that IC participants maintain the gains achieved after the end of their participation in the program.
Within-Group and Between-Group Analyses of Change in IC and WLCC at Follow-Up.
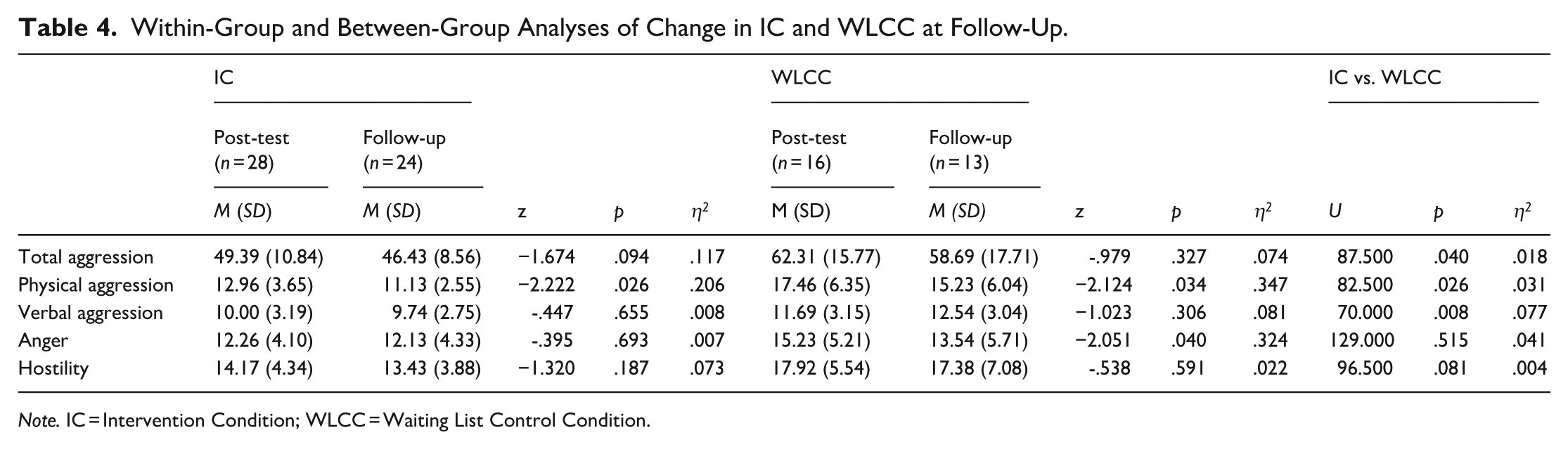
Note. IC = Intervention Condition; WLCC = Waiting List Control Condition.
IC participants revealed a significant decrease in physical aggression, with a large effect size, and a marginal decrease in overall aggression. WLCC participants also revealed significant decreases in physical aggression and anger, with large effect sizes. However, comparing the groups, significant differences in overall aggression and physical and verbal aggression, and marginal differences in hostility were found, with IC participants revealing the lowest scores.
Clinical Change in Aggression After Intervention Completion and Follow-Up
Data on clinical change at post-treatment and follow-up are presented in Table 4. Post-test results showed significant differences between the groups in the distribution by clinical change categories for total aggression, verbal aggression, anger, and hostility. The number of individuals falling into the global improvement category was higher for the IC. In contrast, the number of individuals in the global deterioration category was higher for WLCC.
Follow-up results only revealed significant differences between conditions in the distribution by clinical change categories for verbal aggression. A higher number of IC participants fall into the global improvement category, while a higher number of WLCC participants fall into the deterioration category (Table 5).
Reliable Change Index (RCI) for Aggression (Physical and Verbal Aggression, Anger, and Hostility) at Post-Test and Follow-Up.
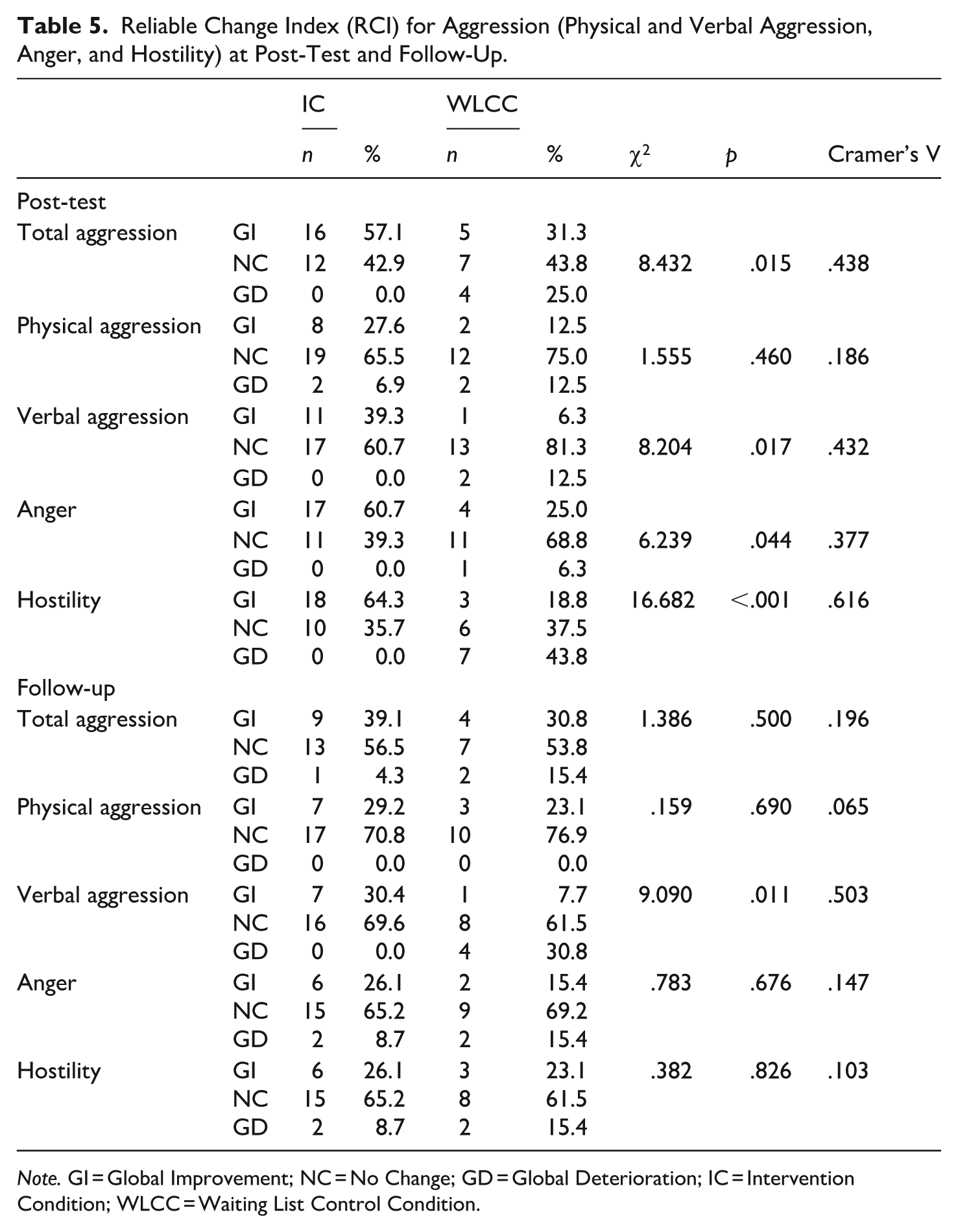
Note. GI = Global Improvement; NC = No Change; GD = Global Deterioration; IC = Intervention Condition; WLCC = Waiting List Control Condition.
Discussion
The present study aimed to investigate the effects of the PPRIAC, a multimodal intervention program for IPV perpetrators. Specifically, the study sought to assess changes in overall aggression and its components. Additionally, the study aimed to analyze the clinical change, extending and proving the effectiveness of a multimodal intervention program designed for Portuguese IPV perpetrators. This study holds particular significance in light of conflicting findings in the literature regarding PIPs effectiveness (e.g., Arce et al., 2020; Cheng et al., 2019; Fernández-Fernández et al., 2022; Wilson et al., 2021).
One of the most noteworthy findings of the study was the significant reduction in overall aggression, marked by large effect sizes, in the IC group following the implementation of PPRIAC. Beyond total aggression, there were also notable decreases in specific subdomains such as physical aggression, verbal aggression, anger, and hostility within the IC group. These reductions persisted at the 6-month follow-up, with physical aggression continuing to decrease from post-test to follow-up. Significant group differences at follow-up were identified in overall aggression, physical aggression, and anger. These results indicate that the multimodal intervention program—designed according to current guidelines associated with improved therapeutic outcomes, specifically adhering to the RNR principles (Bonta & Andrews, 2023; Radatz et al., 2021; Radatz & Hilton, 2025; Radatz & Wright, 2015)—effectively reduces aggression traits among IPV perpetrators and also impacts specific behaviors related to IPV. This reinforces the program’s effectiveness and its potential to reduce IPV, as well as the value of intervention approaches that adhere to the RNR principles. The significance of these findings is twofold. First, aggression—particularly physical aggression, anger, and hostility—has been consistently linked to IPV perpetration (e.g., Birkley et al., 2015; Cunha, Cruz et al., 2023; Cunha et al., 2021; Dannisworo et al., 2019; Eckhardt et al., 1997; Eckhardt et al., 2008; Stith et al., 2004). IPV perpetrators tend to exhibit higher levels of hostility and anger than non-perpetrators (e.g., Eckhardt et al., 1997; Norlander & Eckhardt, 2005; Ontiveros et al., 2023; Stith et al., 2004), and these factors are conceptualized as criminogenic needs (Bonta & Andrews, 2023). This aligns with literature suggesting that effective treatment for reducing recidivism, including IPV recidivism, should prioritize addressing perpetrators’ criminogenic needs (Bonta & Andrews, 2023; Friedman et al., 2022; Travers et al., 2021). In addition, aggression may act as a mediating factor in IPV perpetration (Cunha, Cruz et al., 2023), implying that certain perceived stressors, such as financial problems, jealousy, or conflicts, can heighten anger or hostility, thereby increasing the likelihood of IPV perpetration (Graham et al., 2022). Furthermore, our results underscore the significance of enhancing emotional recognition and regulation, as well as improving problem-solving and coping skills (Friedman et al., 2022)—abilities addressed by PPRIAC (Cunha & Gonçalves, 2011, 2015). These strategies prove crucial in reducing aggression, emphasizing the importance of incorporating these variables as intervention targets among IPV perpetrators and as indicators of intervention success and change. Nevertheless, further investigation is warranted to comprehensively understand the mechanisms underlying the relationship between aggression and IPV perpetration, as previous studies suggest both direct effects (e.g., Clements et al., 2018; Cunha, Cruz et al., 2023; Cunha et al., 2021) and mediating effects of aggression on IPV (Cunha, Cruz et al., 2023).
The results also demonstrated significant clinical changes in IC, with a greater number of perpetrators falling into the global improvement category at the post-test. This contrasts with the WLCC, where a higher number of individuals fell into both the no change and global deterioration categories. This pattern held true for overall aggression, verbal aggression, anger, and hostility. While no significant differences were found for physical aggression, the levels of physical aggression at post-test in both groups were low compared to the Portuguese community sample (Cunha & Gonçalves, 2012). A similar pattern emerged for clinical changes in verbal aggression at follow-up. Regarding overall aggression, physical aggression, anger, and hostility at follow-up, the effect sizes were not sufficiently robust to differentiate between the groups in terms of clinical change. However, a consistent trend was observed, with a slightly higher number of individuals from IC falling into the global improvement category, while a greater number of WLCC participants fell into the deterioration category. This finding prompts us to question the efficacy of the traditional justice system in rehabilitating or improving emotional processes, such as emotional self-control and regulation, among IPV perpetrators (e.g., Brazão et al., 2015; Cunha, Silva et al., 2023).
Our findings suggest that a multimodal program like PPRIAC, which addresses emotional skills among other factors (e.g., Cunha & Gonçalves, 2011), may play a valuable role in mitigating the tendency for these issues to worsen over time. Crucially, the lack of change and observed deterioration in the WLCC may be partially attributed to the design employed, specifically the waiting list aspect. Research indicates that such designs may lead to overestimating intervention effects (Cunningham et al., 2013), as participants assigned to WLCC may perceive an expectation to wait until receiving the intervention and consequently comply with this perceived expectation (Miller & Rollnick, 2022). Studies suggest that the allocation to the waiting list can hinder efforts at change (Cunningham et al., 2013). Nevertheless, it is important to note that a small number of individuals in the IC also exhibited deterioration at follow-up, prompting consideration of the sustained efficacy of the intervention over the long term for all individuals (Johnsen & Friborg, 2015). However, it is crucial to highlight that the majority of individuals from both groups demonstrated normative levels of aggression at follow-up, even among those classified in the deterioration category.
Despite the favorable effects of PPRIAC on aggression and its components, a concerning issue persists: a substantial dropout rate, reaching almost 27%. While these rates align with those observed in prior meta-analyses (e.g., Cunha et al., 2024; Travers et al., 2021; Wilson et al., 2021), the elevated incidence of dropout among PIPs is a critical concern due to its association with an increased likelihood of re-offending (e.g., Lila et al., 2019; Morrison et al., 2021). The factors contributing to these high attrition rates remain unclear, particularly in this study, where no significant differences were found between completers and dropouts in sociodemographic and juridical variables and aggression levels. One plausible explanation may be related to the no-cost nature of PPRIAC (Cunha et al., 2022). Some literature suggests that, in some locations—such as California—dropout rates tend to decrease when individuals make a financial investment in their treatment (Timko et al., 2015). However, this explanation has limitations, as other studies have reported the opposite trend, indicating that financial barriers may, in fact, increase dropout rates (e.g., Friedman et al., 2022; Yorke et al., 2010). These mixed findings suggest that the relationship between financial investment and program retention is complex and likely context-dependent. Therefore, further research is needed to better understand the impact of financial investment on dropout rates, particularly within voluntary, community-based interventions. An alternative explanation centers around the timing of dropout. The relatively low average number of sessions attended by non-completers (approximately seven) suggests that most dropouts occurred early in the intervention, likely before establishing a therapeutic alliance and group cohesion (Hendricks et al., 2006). Building a robust therapeutic alliance is pivotal for client motivation and serves as a predictor of favorable clinical outcomes (Boira & Carbajosa, 2023). While MIT are integrated into PPRIAC, as the number of sessions ranges from four to six, there is a possibility that certain individuals may benefit from additional sessions to enhance their motivation for change further and increase engagement with the intervention process (Cunha et al., 2022).
Limitations and Future Directions
Despite the valuable contributions of this study, it is crucial to acknowledge its limitations. Firstly, the small size of our sample impacts on the statistical power of the analyses, thereby necessitating a cautious interpretation of the results. Future studies should strive for a larger sample to enhance the reliability of findings. A larger sample would also allow for a more detailed examination of the change process, specifically identifying which aspects of the intervention program contribute to change. In this regard, a mixed-methods approach with a qualitative focus would be particularly relevant. Secondly, the relatively short follow-up period underscores the need for extended duration to evaluate the sustained impact of the intervention program over the long term. Thirdly, as previously noted, using a waiting list design poses a limitation. While this design offers ethical advantages by providing care to participants actively seeking help, it may overestimate intervention effects (Cunningham et al., 2013). Therefore, the results should be interpreted considering the chosen design. Fourth, the absence of randomization in participant allocation to each condition is an additional limitation, emphasizing the importance of future studies employing randomized control trial designs to assess intervention effectiveness more effectively. Fifth, another limitation of the current study is that it was not designed to examine the minimum number of sessions required to effectively reduce aggression. Future research exploring the dose-response relationship could provide valuable insights into the optimal intervention length needed to achieve meaningful behavioral change, which would be crucial for informing program design, resource allocation, and policy decisions. Sixth, the exclusive reliance on self-report measures to assess aggression introduces a potential source of bias. Given the tendency for social desirability in perpetrators’ self-reports (Dutton & Hemphill, 1992), future studies should incorporate social desirability measures or lie scales. Additionally, validating results through victims' and other significant reports and in-depth interviews with participants would offer a more comprehensive understanding of the strategies employed for emotion management and problem-solving. Lastly, a significant limitation of this study is the absence of direct outcome data on IPV, including self-reports, partner reports, or official criminal justice records. This limits our ability to conclusively assess the intervention’s impact on IPV behaviors specifically, and future research should incorporate multiple sources of IPV outcome data to provide a more comprehensive evaluation of program effectiveness.
Conclusion
The study’s findings underscore the positive impact of PPRIAC in mitigating aggression among individuals involved in IPV. These results demonstrate the efficacy of the PPRIAC intervention and emphasize the crucial necessity for multimodal approaches when addressing aggressive behaviors within the complex context of IPV.
The significance of these findings extends to their potential to inform and shape future therapeutic and preventive strategies. By highlighting the success of a specific multimodal intervention, the study advocates for a nuanced and comprehensive approach essential for tackling the multifaceted nature of violent behaviors in intimate relationships. This encourages a shift towards interventions that go beyond conventional methods, considering the diverse factors contributing to IPV. Tailoring interventions to address both the overt manifestations of aggression and the underlying dynamics and triggers can lead to more sustainable and comprehensive outcomes. Furthermore, the results of this study contribute to the ongoing discourse on IPV prevention. The effectiveness of PPRIAC suggests that interventions should not adopt a one-size-fits-all approach but should be adaptable, recognizing the diverse needs and circumstances of individuals engaged in violent behavior. The study also points towards the need for further exploration into the specific components of PPRIAC that contributed to its success, paving the way for evidence-based practices and enhancing the overall effectiveness of interventions targeting IPV.
Supplemental Material
sj-docx-1-ijo-10.1177_0306624X251415371 – Supplemental material for Addressing Aggression in Intimate Partner Violence: Preliminary Findings from a Multimodal Intervention for Male Perpetrators
Supplemental material, sj-docx-1-ijo-10.1177_0306624X251415371 for Addressing Aggression in Intimate Partner Violence: Preliminary Findings from a Multimodal Intervention for Male Perpetrators by Olga Cunha, Teresa Silva, Telma Catarina Almeida, Rui Abrunhosa Gonçalves, Marta Sousa and Sónia Caridade in International Journal of Offender Therapy and Comparative Criminology
Footnotes
Acknowledgements
Not applicable
Ethical Considerations
The present research was approved by the University of Minho Ethics Commission (CE.CSH 102/2018). All procedures were in accordance with the ethical standards of the institutional ethics commission and with the 1964 Helsinki declarations and its later amendments. The trial is registered at ClinicalTrials.gov with the reference NCT05484440.
Consent to Participate
All participants were informed about the content and aims of the study and were informed about their anonymity and voluntary participation. All participants signed an informed consent.
Consent for Publication
Written informed consent for publication was obtained from all individuals who participated in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was conducted at CIPsi, School of Psychology, University of Minho, supported by the Portuguese Foundation for Science and Technology (FCT; UID/01662/2023: Centro de Investigação em Psicologia) through national funds. This study was also funded by the Foundation for Science and Technology—FCT (Portuguese Ministry of Science, Technology and Higher Education), under HEI-Lab R&D Unit (UIDB/05380/2020, https://doi.org/10.54499/UIDB/05380/2020) and project UID/4585/2025 (![]() ). It was also supported by FCT Grant SFRH/BD/66110/2009, awarded to the first author.
). It was also supported by FCT Grant SFRH/BD/66110/2009, awarded to the first author.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to confidentiality of the data but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.