
Abstract
Mental health diversion pairs mental health treatment with court oversight as an alternative to incarceration. We conducted a qualitative exploration of the applicability of a patient-centered care framework—typically applied in healthcare contexts to center the experience of a patient in their own care—to mental health diversion. This study examines (1) if the principles of patient-centered care are experienced by mental health diversion clients and (2) how these principles apply to hybrid healthcare-legal system intervention like mental health diversion. We interviewed 15 diversion clients from 6 counties in California. Findings suggested that patient-centered care is relevant to diversion clients, including client access to care, relationships with trusted professionals, and respect for preferences. However, the patient-centered care framework requires adaptation for the mental health diversion context, in which both therapeutic professionals and legal professionals play key roles.
Plain Language Summary
Patient-centered care frameworks focus on the respect for each individual patient and their wants and needs. They have often been applied in research and practice in health care settings. There are increasingly programs that look to provide mental health treatment -- a type of health care -- to individuals involved in the legal system. One such type of program is mental health diversion, in which people have the opportunity to complete a treatment program in exchange for their charges being dismissed. However, although these programs provide clients with treatment, they are located within the court system, where the focus is typically on compliance with requirements and adherence to the law. This study focused on whether patient-centered care principles are relevant in the context of mental health diversion programs. We interviewed 15 mental health diversion clients to learn more about their experiences, and explored the application of patient-centered care principles to their experiences.
Introduction
In California, pre-trial mental health diversion programs are a community-based alternative to incarceration that allow clients with mental health concerns to engage in needed treatment. If successful, they have the opportunity for their charges to be dismissed. Mental health diversion is, in many ways, a legal system intervention, as diversion decisions involve justice partners, including defense attorneys, prosecutors, and judges. But ultimately, the goal of these programs is to provide treatment and give clients a chance to reintegrate into society without a conviction on their record. With this study, we explored the perspectives of mental health diversion clients on their experiences with diversion. To gauge the nature and quality of these experiences, we applied a patient-centered care framework. Though typically used in healthcare settings, not legal system settings, we explored the extent to which patient-centered care principles were present in mental health diversion setting, with the goal of determining how well this framework applied to this hybrid healthcare-legal system intervention and to guide recommendations for future implementation.
Mental Health and the Criminal Legal System
An estimated 64% of people in jails and 50% of people in prison have some indication of a mental health disorder, including reporting a history of mental health conditions or current symptoms of serious psychological distress (Bureau of Justice Program Statistics, 2017). As a result, correctional facilities in the United States have become de facto “mental health treatment facilities,” despite the limited resources to treat these individuals while incarcerated. Furthermore, individuals released from incarceration without community support, such as connections to treatment and other supportive services, remain at greater risk for future legal system involvement (Visher et al., 2017).
Nationally, these concerns have led to a focus on alternatives to incarceration for those with mental health and substance use disorders. For example, drug courts and mental health courts provide individuals the opportunity to complete community-based treatment with regular court oversight, allowing them to receive treatment and avoid incarceration (Liu & Redlich, 2015). However, these collaborative court models often require people to serve a probation term while they complete the program, leaving criminal charges on their records. Recently, there has been greater focus on upstream options, such as pre-trial diversion, which often allow clients the opportunity for their charges to be dismissed if they complete program requirements (Brooks Holliday et al., 2024; Reinhart, 2016).
Benefits of Pre-Trial Mental Health Diversion
Pre-trial mental health diversion offers clear health and legal advantages. Related to health, these programs provide a formal pathway for individuals to access community-based mental health treatment, which can be difficult to find, especially for marginalized racial and ethnic groups (Mongelli et al., 2020) and low-income populations (Rapfogel, 2022), which are overrepresented in the legal system (Ghandnoosh, 2023; Rabuy & Kopf, 2015). Additionally, diversion clients can avoid incarceration, and the deleterious health effects associated with incarceration (National Academies of Sciences, Engineering, and Medicine, 2014). Compared to individuals who have never been incarcerated, current and former inmates experience higher rates of communicable diseases, chronic health conditions, and psychiatric and substance use disorders (Fazel & Baillargeon, 2011). These health problems often persist even after release (Massoglia & Pridemore, 2015) and can put individuals more at-risk for having a reduced life expectancy (Patterson, 2013).
Pre-trial diversion can also help individuals avoid the other collateral consequences of incarceration. For example, only 55% of formerly incarcerated individuals earn income the year after release, and those who find employment often hold low-wage jobs with poor benefits and no health insurance (Looney & Turner, 2018). This lack of income makes it difficult to afford rent, medical care, food, and utilities, which also can negatively affect health. These barriers can lead individuals to re-offend due to limited opportunities outside of crime (Acker et al., 2019). Some evidence suggests that diversion programs can reduce the likelihood of future arrest and days spent in jail, and potentially be less costly than traditional prosecution, though findings are mixed (Heilbrun et al., 2015).
Providing Mental Health Treatment in Court Contexts
Though there can be clear benefits to participating in mental health diversion, there are some unique considerations related to providing mental health treatment to diversion clients. These programs exist at the intersection of the legal system and the healthcare system. This means that, although clients do receive treatment through community-based service providers, there is still court oversight of treatment. Moreover, there are clear consequences for failure to complete treatment: diversion clients can face traditional prosecution if they do not fulfill the terms of their diversion (Heilbrun et al., 2015).
Diversion programs are not the only type of program that navigate this unique context. For example, mental health courts, drug courts, and other collaborative courts are similarly situated at the intersection of community-based treatment and the legal system. These courts often follow principles that were initially established for drug courts, which highlight the ways that these courts are different than typical legal proceedings. For example, the principles highlight the use of a non-adversarial approach (Bureau of Justice Assistance, 1997). In addition, the principles briefly address the importance of providing treatment that is comprehensive, accessible, and sensitive to the needs of individual clients. However, in general, these principles are more oriented toward themes such as monitoring abstinence, promoting compliance and addressing non-compliance, and ensuring ongoing interactions between the judge and participants (Bureau of Justice Assistance, 1997). As a result, these principles can feel more oriented toward the legal system, rather than the intersection of the mental health and legal systems.
An alternative way to conceptualize these types of interventions is to draw on models typically used in healthcare contexts—models that focus on treatment and centering the patient experience, rather than punishment and consequences. This is especially the case for pre-trial diversion programs when the goal of these programs is to give clients an opportunity to clear the charges from their record.
Patient-Centered Care
Patient-centered care frameworks, broadly speaking, focus on the respect for each individual patient and their wants and needs (Epstein & Street, 2011). The concept of patient-centered care has been in existence for decades and initially grew from observations that the traditional disease-centered model was not sufficient for identifying and understanding all illnesses, especially chronic diseases (McCracken et al., 1983). First introduced in the late 1960s (Håkansson Eklund et al., 2019; Langberg et al., 2019), advocates for patient-centered care believed that practices that help physicians understand an illness from the patient’s perspective were more effective than using the disease-centered model alone (Engel, 1977). Patient-centeredness became influential in the decade after it was first introduced and by the late 1970s the World Health Organization was advocating for widespread adoption of patient-centered care (Håkansson Eklund et al., 2019). However, early efforts to promote patient-centered care were not accompanied by a clear and consistent definition of what patient-centered care entailed, or how it should be implemented (Langberg et al., 2019). Researchers have worked to further clarify and define patient-centered care (Constand et al., 2014; Jayadevappa & Chhatre, 2011; Langberg et al., 2019; Rathert et al., 2013; Yudkin, 2022), and how it differs from other centeredness approaches including person-centered care which emerged as an alternative to patient-centered care in the 1990s (Håkansson Eklund et al., 2019; Hughes et al., 2008).
Over the past 30 years, patient-centered care frameworks have been used in healthcare research to explore questions related to patient satisfaction, quality of care (Beattie et al., 2015), and healthcare outcomes in a variety of care settings and populations (Bertakis & Azari, 2011; Meterko et al., 2010; Rocco et al., 2011). Studies have been conducted in diverse care settings including primary, specialty, and inpatient care (Bertakis & Azari, 2011; Meterko et al., 2010; Rocco et al., 2011), and in countries including Sweden, China, South Korea, and Switzerland (Haller et al., 2011; H. N. Park et al., 2022; Wolf et al., 2012; Wong et al., 2011). Patient populations studied include veterans, gynecology patients, cancer patients, psychiatric patients, and those with Parkinson’s disease (Findeklee et al., 2019, 2020; Scanferla et al., 2023; Tsvitman et al., 2021; van der Eijk et al., 2011; Weiner et al., 2013). Findings have been mixed across contexts and study designs; however, systematic reviews suggest that patients who receive patient-centered care are more satisfied and experience better health outcomes, including improved treatment adherence and reduced healthcare utilization (Doyle et al., 2013; Khiari et al., 2021; M. Park et al., 2018).
Numerous patient-centered care frameworks have been used to guide clinical and research efforts. A scoping review of frameworks found three core components featured across frameworks: effective communication, partnership, and health promotion (Constand et al., 2014). However, these principles are fairly broad, and care providers could benefit from a framework that includes more detail about what patient-centered care might look like in practice (e.g., what constitutes effective communication?).
The Picker Principles of Person-Centered Care is a widely used framework developed in the late 1980’s out of a research initiative funded by the Picker Foundation and the Commonwealth Fund (Beatrice et al., 1998) that measures patient experiences related to eight specific dimensions (Jenkinson et al., 2002; see Table 1). The principles are an effective implementation road map for providers that provide a clear operational definition of communication and partnership, and health promotion. The Picker Principles have been used in a variety of research contexts. For example, the Picker Patient Experience Questionnaire, a validated measure based on these principles, has been used with patients with a variety of conditions, including acute myocardial infarction (Meterko et al., 2010), neurological disorders (Heslop et al., 2019), and cancer (Reid et al., 2024). Moreover, these principles have been used in qualitative studies of patient experiences (Pateman et al., 2023; Shrivastava et al., 2019).
Picker Principles of Patient-Centered Care.
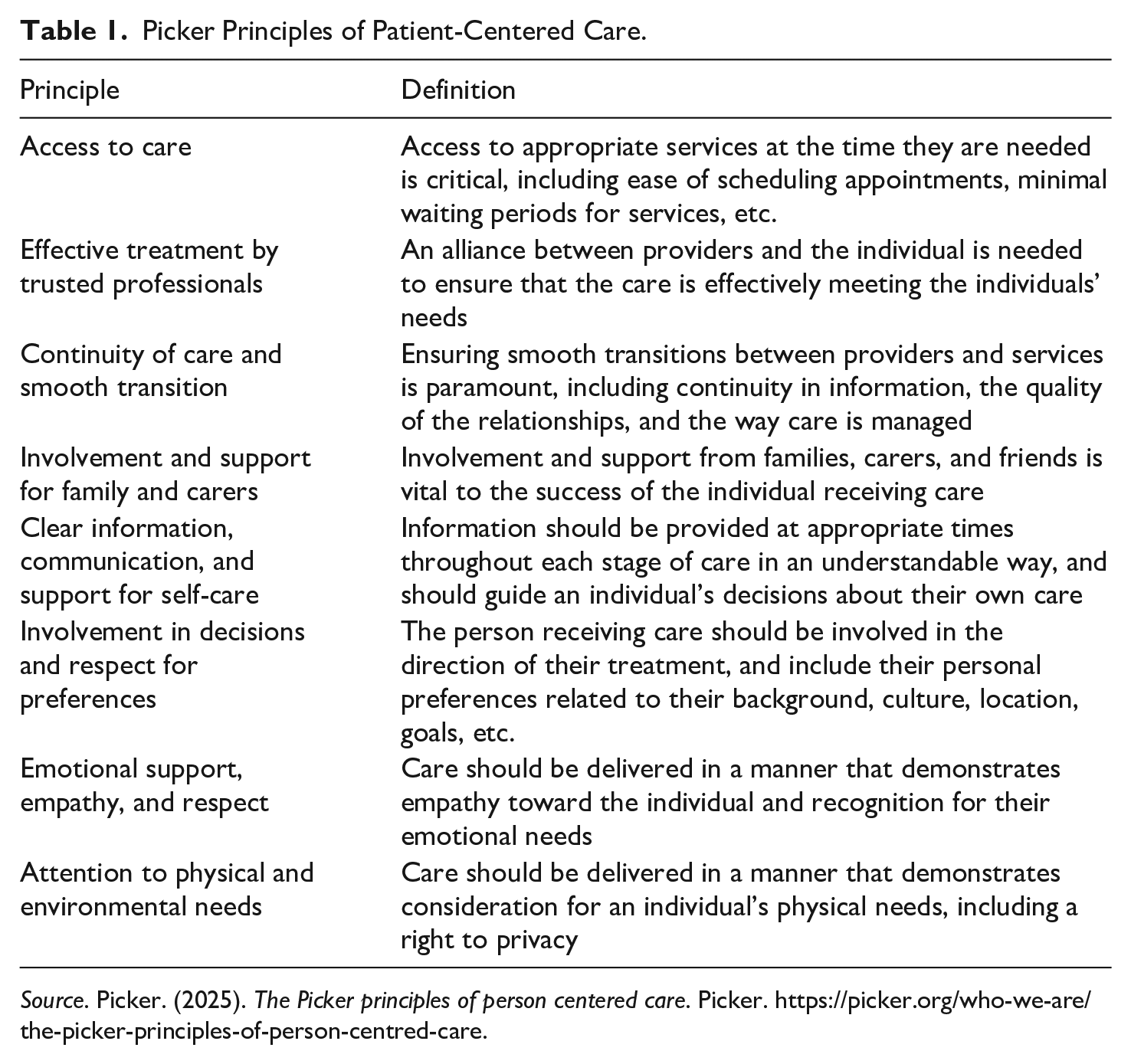
Source. Picker. (2025). The Picker principles of person centered care. Picker. https://picker.org/who-we-are/the-picker-principles-of-person-centred-care.
The present study utilizes the Picker Principles to explore patient-centered care in the context of mental health diversion. Although there are differences between receiving mental health care outside the legal system and as a result of legal involvement, incorporating patient-centered practices may enhance diversion programs as well as client outcomes.
Present Study
In 2019, California passed Assembly Bill 1810, which was codified in the state penal code under section 1001.36. This statute established pre-trial diversion for people who have a mental health or substance use disorder, and whose diagnosis had a role in the charges that they faced (note that this requirement has since been amended but was in place at the time this study was conducted). If these individuals successfully complete a treatment program of 1 to 2 years, depending on the severity of their charges, then their case is dismissed.
The aim of this study was to understand the experiences of pre-trial mental health diversion clients in six counties in California. We interviewed clients to explore how they learned about diversion, the nature of their treatment plan, their communication with relevant professionals (e.g., attorneys, treatment providers), and perceptions regarding the effectiveness of the program. The interviews were part of a larger study to understand how mental health diversion is being implemented in California (a previous phase of this study focused on the perspectives of staff and providers involved in diversion implementation; Sizemore et al., 2024). Our research questions were:
Were principles of patient-centered care present in the experiences of mental health diversion clients?
How applicable are these principles in a hybrid healthcare-legal system intervention like mental health diversion?
Given the qualitative and exploratory nature of this study’s goals, we did not have an a priori hypothesis.
Methods
Sample
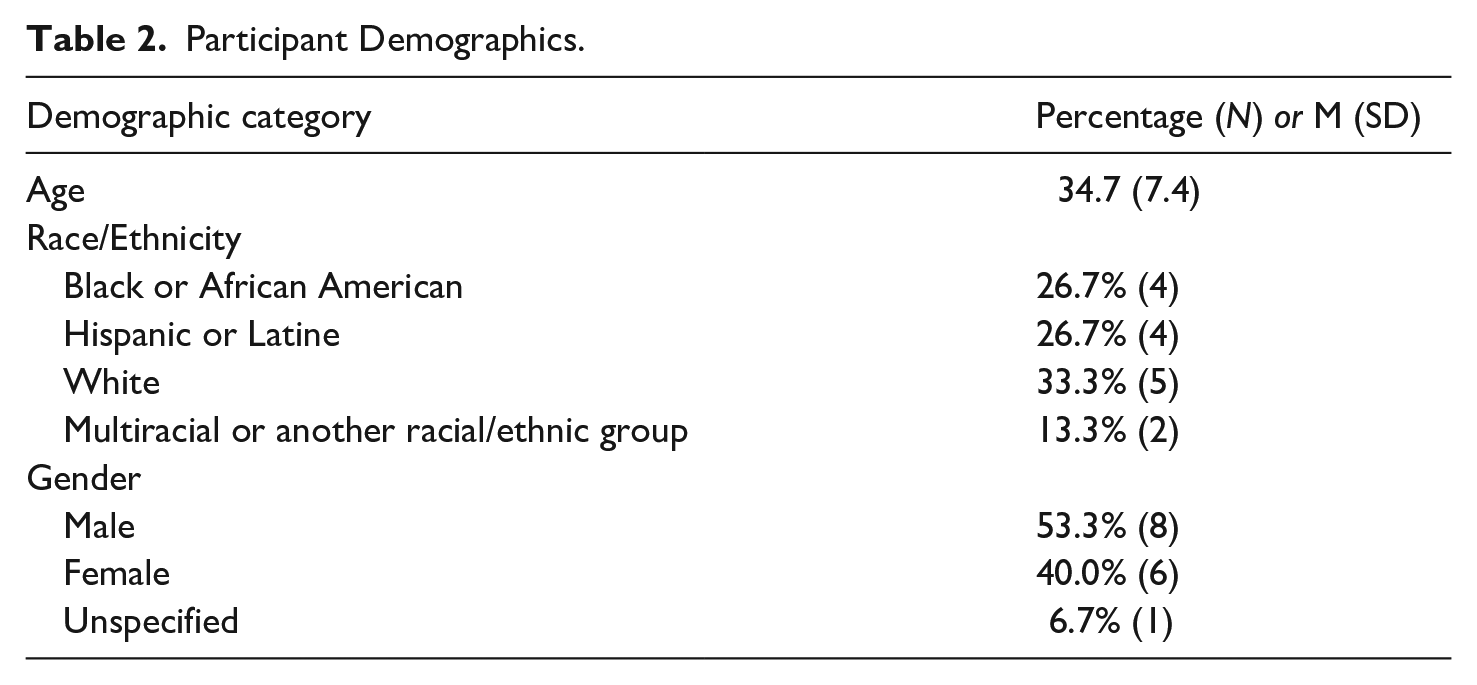
We began by recruiting nine counties across the state, focusing on counties that had implemented mental health diversion to ensure that they had started to serve clients and could share information about how diversion was implemented. We also considered factors such as county size, location, and racial/ethnic composition. To recruit participants, we began by reaching out to representatives from the primary offices involved in diversion, typically the Public Defender’s Office or county behavioral health agency, either by leveraging existing relationships in those counties or by conducting outreach to staff members identified through public-facing materials (e.g., county websites). In total, we reached out to individuals in 14 counties and 9 counties agreed to participate in the study. After an initial phase of this work, in which we interviewed staff members of the agencies involved in mental health diversion, we shifted our focus to the recruitment of current diversion clients or diversion graduates. Of the original nine counties, six agreed to assist with client recruitment. In each county, we collaborated with the Public Defender’s Office or behavioral health provider to identify potential clients who were interested in participating. In total, we received 25 names across the 6 counties, and 15 clients agreed to participate. Interviews were conducted between May of 2022 and October of 2023. See Table 2 for self-reported demographic characteristics of the participants.
Participant Demographics.
Procedure
We developed a set of interview protocols based on the client’s stage in diversion. For clients who had enrolled in diversion fairly recently and were still active in the program, we conducted a two-part interview, with the initial interview focusing on their early experiences in diversion and a second interview, approximately 6 months later, focusing on their experience in the program to date. For clients who were further along in the program or who had graduated from diversion, we conducted a single interview focused on their full diversion experience, from enrollment to completion. However, all versions of the protocol were drawn from the same question bank, ensuring consistency in content across the interviews. Clients received a gift card for their participation. A table summarizing the major domains of the interview protocol and sample questions appears in the Supplemental Materials. Interviews were recorded and professionally transcribed with the permission of participants. All procedures were approved by the RAND Institutional Review Board, and participants provided verbal informed consent for participation.
Analysis
To analyze the data, we began by developing a codebook. The parent codes for the codebook were identified in a largely deductive manner based on the interview questions. Coding was conducted in Dedoose, a qualitative and mixed methods analytic software. In total, there were 17 interviews with 15 clients (because two current clients participated in a two-part interview). Of the 17 interviews, 2 were triple-coded while calibrating the codebook and the remainder were single coded. Our research team met regularly throughout the coding process to ensure interrater reliability and consistent application of codes. All coding decisions and updates to the definition of each code were recorded in a data dictionary throughout the course of the project.
After coding the transcripts, we conducted a second stage of analysis to map our codebook onto the Picker Principles of Patient Centered Care. A single member of the research team mapped the codes to principles, and then we discussed the mapping among the research team until we reached a consensus.
We then analyzed the interview excerpts using these principles as a framework to examine whether implementation of diversion was consistent with principles of patient-centered care. Table 2 summarizes the crosswalk between each Picker Principle and the codes. The results section describes our findings in relation to five of the eight principles: Access to Care; Effective Treatment by Trusted Professionals; Continuity of Care and Smooth Transition; Clear Information, Communication, and Support for Self-Care; and Involvement in Decisions and Respect for Preferences. It is important to note that the Picker Principles were not used to develop the interview protocol; therefore, there were some principles that did not have associated codes.
Results
Access to Care
The access to care principle focuses on the importance of clients being able to access appropriate services when they are needed. This can include factors like how easy it was for clients to schedule appointments, and short waiting periods for services. In our interviews, we explored the types of services that clients received through diversion, as well as the barriers and facilitators to accessing them. Behavioral health treatment is required under the state mental health diversion statute, and this included individual and group therapy, substance use disorder treatment (e.g., 12-step programs, outpatient treatment, residential treatment, sober living facilities), and medication management. Twelve clients described receiving additional services as well, such as case management, life skills courses, income and employment support, and connection to essential resources (e.g., transportation, food, and housing).
There were some barriers to accessing and remaining engaged in mental health diversion. Two clients said the restrictive nature of some programs was a challenge. One interviewee reported that the program they enrolled in has policies on how free time is used: “When you first get out . . . they have it on a schedule, on phases. On phase one, you can’t go anywhere, but to the appointments, and then you go up in your phases, then you get to leave more.” Five interviewees described the location of services as a barrier, two said the timing of services made it difficult for them to engage in the program, and two said the amount of time they spent engaging with the program was burdensome. In one instance, an interviewee said they quit their job because they were unable to maintain employment while actively participating in the different appointments and commitments involved in their diversion program.
In addition, two interviewees described delays of 3 months to a year in receiving services due to limited-service provider capacity. One interviewee described the wait saying, “[i]t was during COVID, and they just didn’t have the availability that they said they did. They said it’d be about a three-month wait, but then it turned out to be over a year.” Other barriers included limited access to resources like transportation, housing, and technology, as well as limited computer literacy.
However, clients also described several factors that facilitated their participation in diversion. Some of these facilitators were features of the diversion programs, for example, offering a convenient location, flexibility in the timing of services, and the option to receive services remotely. Some diversion programs allowed clients to continue seeing existing providers, which made it easier for them to engage in services (and is consistent with the “continuity of care” principle described below). Clients also drew on other factors, such their support network and their own self-motivation, to remain engaged in diversion. One interviewee described the role of self-determination in following through with diversion requirements, saying, “diversion fits everyone but it starts with the person who wants to change.”
Effective Treatment by Trusted Professionals
This principle emphasizes the need for a positive therapeutic relationship between providers and the individual, to ensure that the care effectively meets their needs. Twelve clients reported having a positive relationship with their mental health treatment providers. Some program staff were described as especially engaging and supportive, helping create accountability mechanisms for program participants to facilitate their engagement in diversion. Given racial disparities in the criminal justice system, we specifically probed as to whether clients felt that their providers were prepared to work with someone from their background. Nine clients indicated that their providers were culturally competent; however, three clients explained that they had encountered providers that were not prepared to work with clients from racially diverse backgrounds. For example, one client stated that they did not feel their provider understood their previous experiences of racial trauma in a way that was conducive for a strong therapeutic relationship with them.
In mental health diversion, the “trusted professionals” providing services go beyond the mental health treatment provider and can also be conceptualized as including the individual’s attorney, judge, and other court personnel. Twelve clients said they had a positive relationship with their attorney, and nine felt their attorneys were culturally competent. However, two clients mentioned how “busy” their attorney appeared to be, and seven clients reported switching attorneys/public defenders several times from when they first enrolled in the diversion program one client spoke briefly about their experience in this regard: “I’ve changed public defenders at least three times now. I assume she’s been comfortable with handling my case. To me, there’s a story behind how that incident really occurred. That’s something that I haven’t been able to share with my public defender in order to understand where we stand together on this. As far as I’m concerned, she’s just doing her job to help me with the changes I’m trying to make today.”
When clients described their experience in court, six said they felt that they received fair treatment and four described scheduling accommodations that the court made for them due to illness, transportation issues, and bad weather. One client described his experience in court, saying, “When my public defender read my progress report, the judge always makes a smile and just listens. Very, how to say, peacefully. So, I feel support from her, my judge, yes.”
Continuity of Care and Smooth Transition
This principle focuses on the importance of smooth transitions between providers and services. As described above, seven clients had multiple defense attorneys and four clients described staffing changes in the behavioral healthcare providers over the course of their time in diversion, which for misdemeanors charges was 1 year and for felony charges, 2 years. Four interviewees experienced staffing changes in their assigned case manager, sometimes experiencing as many as three to four staffing changes. One interviewee said that frequent staffing changes made it difficult to build strong relationships with these providers, though most did not describe this as adversely affecting their experience. Another interviewee described the challenges of intermittent contact with his attorney, saying, “[I] don’t really have one. I mean, public defender . . . he’s there sometimes at the court when I go there, other times it’s somebody else from their office. I don’t know. I appreciate the program . . . It’s a good option, but I kind of think somebody needs to get more of an idea of each individual person.”
For this study, we extended the application of this principle to include transitions that occur even after the diversion program ends. When clients complete diversion, ongoing access to treatment or other supportive services is not guaranteed. However, five clients continued receiving services after completing the program (including four who continued seeing the same provider), though two clients experienced a break in services upon graduation and were searching for new mental health providers Similarly, clients had mixed experiences with having their criminal records cleared after completing their diversion programs. Seven interviewees reported having their records cleared, while one program graduate described a clerical error that resulted in their record not being cleared, which created immigration and employment complications.
Clear Information, Communication, and Support for Self-Care
According to this principle, information about treatment should be provided to clients in an understandable way and at appropriate times throughout each stage of care. For this study, we were particularly interested in how clients first learned about diversion, what they were told about diversion as an option in their case, and how they decided to participate. Eleven clients said they learned about diversion from their defense attorney, typically during a court hearing, while in jail, or shortly after being released. Four clients said they decided to participate in diversion because of the possibility of having their case dismissed if they successfully completed the program. However, there were other reasons that clients ultimately decided to participate in mental health diversion—not only legal reasons, but also personal reasons (e.g., being able to maintain their relationships with family members, the opportunity to receive services and support). Nine clients remembered that staff shared details with them about the potential benefits of completing a diversion program.
Involvement in Decisions and Respect for Preferences
Nine clients said that a behavioral health provider or case manager was in charge of their treatment planning process. Clients had a range of responses when asked what information was shared with them about their treatment plan. Eight clients said that they were given information about the services they would receive, such as case management, therapy, medication, cognitive behavioral therapy, intensive outpatient treatment, groups, and housing support. Two clients also recalled there being “court requirements,” such as maintaining sobriety.
About half of the clients we interviewed felt they had input into their treatment plan, though they did not elaborate on how their input was solicited. The remaining clients stated they did not have much input or had simply agreed to the services and treatment goals that were suggested. For example, one client said, “I didn’t have as much input. It was more requirements and, yeah, they pretty much require certain things, so I just had to do it and I did.”
Another aspect of this principle is that clients’ personal preferences related to their background, culture, location, and other aspects of identity are taken into consideration. When asked whether they felt their group identity influenced their experience, 12 clients said they did not believe factors such as race or gender influenced their overall experience in the diversion program in terms of whether they were offered diversion or the types of care they received. The only exception were the concerns described previously about the cultural competence of clinicians.
Discussion
The aim of this qualitative study was to understand the experiences of diversion participants in California. Overall, the responses we received were generally positive, which is noteworthy considering the variation in the execution of diversion across the state. To further analyze our results, we applied a commonly used patient-centered care framework, the Picker Principles, to our findings.
Though the purpose of mental health diversion is to connect participants with mental health treatment—a type of healthcare—the program is situated within the legal system, where the emphasis can often be on compliance and public safety rather than patient experience (Redlich et al., 2010). This can result in an innate tension between patient-centered care and mental health diversion. Patient-centered care is grounded in respecting and prioritizing a patient’s preferences and perspectives, empowering individuals to decide whether, when, and how they wish to engage with healthcare systems (Constand et al., 2014; Langberg et al., 2019). In contrast, clients involved in the criminal legal system have inherently limited agency. Mental health diversion offers an alternative to incarceration, but participants are still restricted to choosing between participation in behavioral health treatments or the potential for incarceration (Johnson & Ali-Smith, 2022; Miller, 2025). Additionally, clients who enroll but do not successfully complete the requirements still face criminal legal charges (Heilbrun et al., 2015).
Despite this tension, the principles of patient-centered care are still relevant to healthcare-legal system interventions, as a core goal of these programs is to connect clients with needed treatment. To successfully complete mental health diversion, clients must engage in behavioral healthcare treatment (Verhaaff & Scott, 2015), but providers can ensure that treatment delivery aligns with the client’s preferences. Research in other healthcare contexts has shown that patient-centered care may improve patient satisfaction and outcomes (Doyle et al., 2013; Khiari et al., 2021; M. Park et al., 2018), suggesting its potential value in diversion programs. Even small changes, such as soliciting client input on treatment plans or scheduling court dates at accessible times, can enhance clients’ sense of autonomy. These are just a few examples of how legal and healthcare professionals can help clients to shape their diversion experience, which in turn may increase successful program completion by tailoring treatment to individual needs (Trood et al., 2021).
In this section, we summarize our findings as they relate to the Picker Principles, making specific recommendations as to how diversion programs could integrate elements of patient-centered care into their operations.
Applicability of Principles of Patient-Centered Care to Mental Health Diversion
Access to Care
One key benefit of mental health diversion is that it provides participants with access to mental health care that they might not otherwise have accessed. There were some challenges to accessing services, though, such as several months elapsing between agreeing to diversion and actually receiving behavioral health services. To some degree, these factors may be outside the control of the diversion programs. For example, clients in many counties rely on the existing Medi-Cal funded system of care (Sizemore et al., 2024) or private insurance providers to access services, and there may be little the court can do to improve access to services (Herman et al., 2024). However, one way that diversion programs could address this is by clearly communicating expectations with clients at various stages of the program, which would also be consistent with other principles of patient-centered care.
Though not a standard component of all diversion programs, some interviewees described other supportive services they received while participating in diversion, such as temporary housing, food assistance, and transportation, along with standard services such as case management and mental health treatment. The clients who received these extended elements expressed that it was critical for allowing them to focus on their mental health in a way that they might not have been able to previously. The programs that offered additional services could be considered more patient-centered because doing so may improve the chances that clients can fully engage in the diversion program and benefit from treatment. This is also consistent with the patient-centered care principle of attention to physical and environmental needs, defined in Table 1.
A notable challenge that some counties experience is a lack of knowledge and resources on how to use available funding to support diversion participants, especially related to housing and expanding community-based services for those who are not eligible for Medi-Cal. Several recommendations were made in a report by The Council of State Governments Justice Center to address this barrier, including statewide trainings, resource development, and peer learning opportunities (Herman et al., 2024) which could lead to increased access to care for participants.
Effective Treatment by Trusted Professionals
As described previously, this principle requires some adaptation to fit the context of mental health diversion, as the “trusted professionals” can be conceptualized as including not only the mental health treatment providers, but also the attorney, the judge, and other court personnel. Our interviews revealed at least one area that deserves additional attention from providers to ensure consistency with this principal, cultural humility. Because people of color are overrepresented in the legal system, it is essential that providers are knowledgeable about disparities and are competent to serve people from marginalized backgrounds (Kapoor et al., 2013; Primm et al., 2005; Schar, 2023; Tadros & Owens, 2021; Venable & Guada, 2014). To help ensure that services appropriately respond to patient needs, diversion programs should consider investing in client evaluations of diversion programming to identify areas that programs can make improvements. Seeking client feedback regularly throughout the participant’s enrollment in diversion can offer valuable insight into the client experience at different stages during the program.
Continuity of Care and Smooth Transition
Ensuring smooth transitions and continuity of services can be accomplished by sharing information across providers, cases are approached consistently across care team members, and that there are no breaks in services. In the context of mental health diversion, themes emerged from our interviews which related to continuity of mental health providers, as well as attorneys, with many participants reporting staffing changes in these roles. Though some clients were not necessarily bothered by these transitions, studies have shown that high turnover among behavioral health providers makes it more difficult for healthcare teams to implement evidence-based practices and may lead to lower quality services (Woltmann et al., 2008).
Changes and shortages in mental health care providers or attorneys may be inevitable, especially given patterns of high turnover among mental healthcare providers (Hutchison et al., 2021) and the relatively small number of lawyers entering public interest law (Albiston et al., 2021). Diversion programs may be able to draw from healthcare models designed to promote continuity of care across staffing changes like the Transitional Care Model (University of Pennsylvania, n.d.) which assigns one clinician who is responsible for coordinating care across contexts and providers (Naylor et al., 2018), or the Care Transitions Intervention model wherein providers repeatedly follow up after a client exits care to ensure a smooth transition (Care Transitions Intervention, 2024). Drawing from these models could benefit diversion clients by reducing the negative impact of these transitions.
This is particularly important in the unique context of diversion programs, which operate within a compliance-based framework. Although court oversight can seem at odds with patient-centered care, judges in problem-solving courts often view themselves as part of the treatment team and develop innovative strategies to work with diversion participants toward meeting the requirements, which is a different approach than in traditional court settings (Castellano, 2017; Munetz et al., 2014). Research also suggests that judges’ relationship with clients in drug courts can positively influence outcomes (Jones & Kemp, 2013). By leveraging the supportive role of judges, diversion programs may also be able to maintain stability and consistency for clients, even during periods of staffing transitions.
We also learned that some participants were able to continue seeing their mental health providers even after graduating from diversion, which is beneficial from a patient-centered perspective. Ideally, diversion programs would promote this type of continuity of care after graduation, such as through creation of an aftercare plan. If continuing to see their existing providers is not possible, this type of aftercare plan could help connect participants to new providers so that they do not experience a disruption in services when graduating.
Clear Information, Communication, and Support for Self-Care
Patient-centered care has different considerations when it comes to a legal system intervention, such as the manner and extent that information is communicated. For example, nine clients recalled being told that their case would be dismissed upon successful completion of diversion, but only seven clients remembered whether the details of the program requirements (e.g., nature and length of treatment) were also explained at that time.
The criminal justice system operates on the premise of necessary involuntariness, whereas the recovery model depends on voluntary efforts to achieve its goals (Ferrazzi & Krupa, 2016). Diversion programs, however, are situated in a gray area between these two concepts, which can raise ethical questions—especially because defendants’ legal cases remain open while participating in treatment. Although the variation in our interviewees’ responses lacks a clear explanation, it highlights the importance of explicit communication, beginning with the introduction of diversion as an option. Providing sufficient information for informed consent is a fundamental practice in any context, but it is crucial for attorneys (and other program staff, if relevant) to clearly communicate the potential benefits of the program to clients and ensure they understand the commitments involved, as the decision to enroll is often complex, influenced by factors such as financial hardship, limited access to mental health services, or inadequate healthcare coverage (Canada et al., 2020). Furthermore, research indicates that participants who feel coerced into diversion programs may be more likely re-enter the justice system within a year of enrolling (Pratt et al., 2013).
Providing a comprehensive review of the pros and cons, or risks and benefits, of the available options not only aligns with patient-centered practices but also embodies the principles of holistic defense. Holistic defense prioritizes addressing clients’ broader legal and social needs, rather than focusing solely on achieving the most favorable legal outcome, such as case dismissal (The Center for Holistic Defense, n.d.).
Diversion professionals can also draw on this principle to help clients understand the potential for changes in their diversion team (e.g., transitions in their defense attorney). Ensuring that efforts are made to explain to clients early on about the possibility of changes occurring, in addition to properly communicating when a change has been made, would reflect a more patient-centered approach, especially when it is not possible to avoid a transition in care.
Involvement in Decisions and Respect for Preferences
Because mental health diversion is a legal system intervention, there can be challenges to integrating clients into the decision-making process due to structural and procedural constraints. For example, certain facets of diversion are defined by statute, such as the length of the program, and are often influenced by factors like the availability of services and sources of funding for certain services (Edgely, 2014; Robertson et al., 2020). These limitations may restrict the court’s ability to fully incorporate clients’ preferences into the process. However, programs can still offer opportunities for clients to make decisions about their experiences, when possible, as shared decision-making can lead to better treatment adherence and outcomes (Shay & Lafata, 2015). There is precedent for this in the context of diversion; for example, a recent evaluation of a pretrial diversion program found that clients were often given the chance to provide input into their treatment plan (Brooks Holliday et al., 2024). Such practices highlight the potential for balancing the legal system’s requirements with patient-centered approaches.
Similarly, there is value in making accommodations for client preferences. For example, many interviewees expressed appreciation for being able to attend court or appointment via video conference, as it made it easier for them to attend. Of course, not all accommodations may be legally or clinically indicated; however, accommodating client preferences when possible could serve to promote engagement and increase the likelihood that clients actually complete diversion.
Limitations
There are limitations to this study that should be taken into consideration when interpreting the findings. First, participants represented just six counties in California, which were selected to include larger counties and those that had already started to implement mental health diversion, and we had just 15 participants in total. In addition, we worked with professionals in each county to recruit diversion clients, and there is a potential for selection bias (e.g., we may have spoken to people who were more engaged in diversion or had more positive views of the program). Though some qualitative research may set out to create knowledge that generalizes to other contexts, the goal of this study was not to develop generalizable findings, but rather to conduct a more in-depth exploration of client experiences and identify areas for future research (Carminati, 2018; Hays & McKibben, 2021). Therefore, though there are limitations to our small sample and potential for selection bias, it is also important to note that the purpose of the study was not generalizability.
Second, there are aspects of the diversion process that may be specific to mental health diversion in California under PC §1001.36 (e.g., the required type and length of treatment, eligibility criteria). That said, even if mental health diversion in other jurisdictions does not have the exact same features as mental health diversion under PC § 1001.36, there are aspects of the process that are likely similar (e.g., the fact that services span both the legal and mental health systems, the opportunity for case dismissal); therefore, we believe these findings are relevant to other cities, counties, and states.
It is also important to note that we did not design our interview protocol to explicitly explore all eight Picker Principles of patient-centered care. Our protocol was designed more broadly to gain an in-depth understanding of the experience of diversion clients. However, based on the themes that emerged in our analysis, there was clear relevance to the concept of patient-centered care, which is why we chose to deductively apply this framework at the stage of analysis. It will be valuable for future studies to integrate the patient-centered care framework at the stage of study conceptualization, which would also enable researchers to explore all eight principles, rather than just the subset of five principles addressed in the present analysis.
Finally, there are many different patient-centered care frameworks. We selected the Picker Principles because they include a more concrete explication of the elements of patient-centered care than frameworks that have fewer principles. We believe that having a more detailed, concrete set of principles may be helpful for professionals when trying to implement the principles. That said, there is evidence that multi-component frameworks can present different implementation challenges, such as a greater cost burden or need for more staff (M. Park et al., 2018), which should be kept in mind by programs aiming to improve their patient-centered focus when providing services. We also acknowledge the underrepresentation of certain demographic groups, such as marginalized racial and ethnic groups, in research that utilizes or validates the Picker Principles. This is a potential limitation when applying the Picker Principles to mental health diversion programs, particularly given that people from marginalized racial, ethnic, and socioeconomic groups are more likely to be involved in the legal system (Daly & Rosoff, 2022; Kang-Brown & Zhang, 2024; Muller & Roehrkasse, 2022). Our sample was too small to formally explore this question, but this is worthy of future study.
Future Directions
Though preliminary, the present study suggests that patient-centered care frameworks are relevant to mental health diversion. Future studies should aim to explore the applicability of patient-centered care in further depth, which could include studies of different diversion programs, with larger samples of clients, with mental health diversion professionals, and using quantitative measures of patient-centered care (e.g., the Picker Patient Experience Questionnaire; Jenkinson et al., 2002). It would be valuable for future research to explore what patient-centered care looks like in other legal contexts, including collaborative courts and correctional mental health care, and to conduct a more nuanced examination of how the framework could and should be adapted for different professional roles (e.g., legal professionals, mental health providers). Finally, it will be important to understand whether care that is provided in a patient-centered manner is associated with better outcomes for diversion participants, including the impact on health outcomes (e.g., improved mental health symptoms) and legal outcomes (e.g., reduced likelihood of recidivism).
Supplemental Material
sj-docx-1-ijo-10.1177_0306624X251372192 – Supplemental material for The Application of a Patient-Centered Care Framework in Mental Health Diversion: A Qualitative Study
Supplemental material, sj-docx-1-ijo-10.1177_0306624X251372192 for The Application of a Patient-Centered Care Framework in Mental Health Diversion: A Qualitative Study by Tiffany Keyes, Alex Sizemore, Chase Breaux, Nicole K. Eberhart and Stephanie Brooks Holliday in International Journal of Offender Therapy and Comparative Criminology
Footnotes
Acknowledgements
None.
Ethical Considerations
The RAND Corporation Institutional Review Board approved our interviews (Approval ID: 2021-N0698) on February 10, 2022.
Consent to Participate
All participants provided verbal consent for participation in this study.
Consent for Publication
All participants gave verbal consent for publication before starting interviews, including the use of quotes.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Robert Wood Johnson Foundation under Grant 78822.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Interview sample questions, the qualitative interview codebook, and exemplar quotes are included in the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.