
Abstract
This study aimed to report the effect of a 6-week light-active versus moderate-active physical activity intervention embedded in a multimodal day treatment program on selected measures of cognitive control (i.e., response inhibition, error processing, and cognitive interference) and trait impulsivity. A randomized controlled design was implemented, including male multi-problem young adults (aged 18–27) assigned to either light-active (N = 12) or moderate-active physical activity lessons (N = 11). A repeated measures design was used to examine treatment effects between the two groups over time on response inhibition, error processing, and cognitive interference (measured respectively with a Go/NoGo task, a Flanker task, and the Stroop) and trait impulsivity (measured with the Dutch Baratt Impulsiveness Scale). Cognitive control, but not trait impulsivity, improved over time. Specifically, enhancements in inhibition and reduced cognitive interference were observed after 6 weeks. Error processing did not improve, but we did observe improved performance on an error-processing task. No interaction with physical activity intensity was found, suggesting similar treatment effects regardless of intensity. Results should be interpreted with caution due to several limitations, including the small sample size. Overall, due to current limitations (i.e., physical activity embedded in a larger treatment program, small sample size at follow-up, and low intervention adherence), it is not possible to draw any definite conclusions. However, the current findings contribute to a growing body of evidence suggesting potential benefits of physical activity (embedded in a multi-modal day treatment program) in the enhancement of cognitive control deficits in at-risk populations, independent of exercise intensity.
Keywords
Introduction
Executive functioning or cognitive control refers to a set of top-down processes critical for adaptive and goal-directed behavior, including working memory, cognitive flexibility, and inhibitory control (Diamond, 2013). Many other cognitive processes rely on this higher-order cognition (e.g., attention, learning, reasoning), and cognitive control deficits can therefore significantly disrupt these abilities (Botvinick & Braver, 2015; Fan, 2014). Executive dysfunctions have been related to antisocial and externalizing behaviors (e.g., aggression, substance use, and delinquency; (Hiatt et al., 2004; Marhe et al., 2013; Swann et al., 2009; Turner et al., 2018; Weidacker et al., 2017; Zeier et al., 2012; Zijlmans et al., 2019; Zijlmans, Marhe, et al., 2021). For example, compared to the general population, those displaying externalizing behavior have shown a relative inability to restrain inappropriate responses (i.e., response inhibition (Swann et al., 2009; Turner et al., 2018; Weidacker et al., 2017)), to adequately detect and react to errors (i.e., error processing, Marhe et al., 2013; Zijlmans et al., 2019), and to suppress an automated response in favor of a less automated response (i.e., resistance to cognitive interference, (Hiatt et al., 2004; Joyal et al., 2014).
More specifically, adult offenders meeting criteria for antisocial personality disorder (Swann et al., 2009), sexual offenders (Turner et al., 2018), and psychopathic offenders (Weidacker et al., 2017) show more deficits in response inhibition measured with worse performance (e.g., lower accuracy) on reaction time tasks including the Go/NoGo task compared to non-offending adults. Similarly, compared to healthy non-offending controls, adult substance abusers (Sullivan et al., 2019) have shown dysfunctional error processing measured as diminished post-error slowing (i.e., an increase in reaction time after an erroneous response, relating to an increase in response caution and a change in response bias: Dutilh et al., 2012). In addition, prior studies indicate worse performance measured as lower accuracy on an error processing task (i.e., Eriksen Flanker task) in adult substance abusers (Marhe et al., 2013) and in young adults (aged 18–27) displaying multiple problems including antisocial behavior (Zijlmans et al., 2019). Last, regarding cognitive interference, a meta-analytic review conducted on five studies showed significant worse performance on the Stroop task in sex offenders compared to non-offending adults from the general population (Joyal et al., 2014).
Given the widespread role of adequate neurocognitive functioning in our daily lives, it is important to search for effective interventions targeting these functions, such as increased physical activity (Álvarez-Bueno et al., 2017; Chen et al., 2020; Colcombe & Kramer, 2003; Gomez-Pinilla & Hillman, 2013; Guiney & Machado, 2013; Hillman et al., 2008; Smith et al., 2010; Stroth et al., 2009; Verburgh et al., 2014). Exploring the potential impact of physical activity on cognitive control may also contribute to our understanding of the mechanisms that link exercise and physical activity to reduced criminal and antisocial behavior adults (Holt, 2007; Meek, 2018; Nichols, 2010; Stern et al., 2019), as prior studies suggest physical activity can also be used as an effective intervention targeting antisocial behavior (e.g., van der Sluys et al., 2024). It is possible that these effects are in fact mediated through exercise-induced enhancement of cognitive control, although the effect of physical activity on antisocial behavior is beyond the scope of the current study. However, as a first step toward this possible model, it is still worthwhile to examine the effect of physical activity on cognitive control in young male adults suffering from multiple problems, including antisocial behavior.
Cognitive control can be enhanced by increased regular physical activity (Álvarez-Bueno et al., 2017; Chen et al., 2020; Colcombe & Kramer, 2003; Gomez-Pinilla & Hillman, 2013; Guiney & Machado, 2013; Hillman et al., 2008; Smith et al., 2010; Stroth et al., 2009; Verburgh et al., 2014), with the most prominent results in (healthy) sedentary children and older adults (Chen et al., 2020; Gomez-Pinilla & Hillman, 2013; Verburgh et al., 2014). Less is known about this effect in (healthy) young adults between 18 and 27 year (for similar conclusions, see: (Guiney & Machado, 2013; Hillman et al., 2008; Stillman et al., 2020; Verburgh et al., 2014). Nevertheless, one study in healthy young adults (M age 22, range 17–47) revealed positive exercise-induced effects on cognitive interference compared to no-exercise controls after 17 weeks of running (Stroth et al., 2010). This is further supported by another study where 8 weeks of aerobic and coordinative exercise during school days resulted in enhanced cognitive interference in adolescents (aged 12–15) compared to an attention-only control group (Ludyga et al., 2018). Another study found that 9 weeks of moderate aerobic exercise significantly enhanced error processing (i.e., faster reaction times on the Flanker task) in healthy young adults (aged 18–20) compared to wait-list controls (Zhu et al., 2021).
Despite these (limited) studies on healthy young adults, to the author’s knowledge, very little is known about the effect of regular physical activity on cognitive control in young adults displaying externalizing behavior, regardless of the cognitive control deficits associated with this type of behavior (Jackson & Beaver, 2018). Results from acute exercise interventions show that a single bout of exercise can be effective in enhancing inhibitory performance in adults displaying externalizing behavior (e.g., violent offenders and substance abusers), measured respectively as improved performance on a Stop-Signal task (Yu et al., 2022) and improved performance on a Go/NoGo task (Wang et al., 2015). Related, studies are showing a decrease in antisocial behavior following regular physical activity interventions, including reduced aggression in youth (Harwood et al., 2017), reduced externalizing problems (e.g., aggressive and delinquent behavior) in adolescents (Spruit et al., 2016), and increased abstinence rate in adult substance abusers (Wang et al., 2014).
These improvements in externalizing behavior in youth and adults may be the result of the enhanced ability to regulate and restrain one’s behavior (i.e., exercise-induced neurocognitive changes; Boat & Cooper, 2019; Holley et al., 2017), such as increased cerebral oxygenation (Goenarjo et al., 2020), increased cortical thickness in the frontal lobe, and increased frontal gray matter volume (Stern et al., 2019). However, these effects are not fully understood in young adults (Stillman et al., 2020), and more research is needed in this age population. Young (emerging) adulthood is being viewed as a critical and distinct developmental period with unique challenges including an increased emphasis on self-sufficiency (Arnett, 2000) and maturation of the prefrontal cortex (Diamond, 2000). Simultaneously, they are at their peak cognitive functioning, possibly affecting any treatment effects (Bialystok et al., 2012). As such, it is important to focus on young adults as a separate age population, rather than grouping them with adults (Arnett, 2000).
To gain a better understanding of the effects of physical activity interventions on cognitive control, more rigorous study designs are needed, such as randomized controlled trials (RCTs). RCTs are considered the gold standard to measure treatment effectiveness, as they have multiple advantages over other experimental designs, including high internal validity and the possibility to examine cause-effect associations. In addition, the randomization minimizes the likelihood of confounding variables by balancing characteristics between groups (Hariton & Locascio, 2018). To date, however, very little RCT research includes socially vulnerable or at-risk populations, despite the increased interest in exercise and sports programs to foster positive personal development, decrease antisocial behavior, and increase cognition in youth and young adults (Holt, 2007; Meek, 2018; Nichols, 2010; Stern et al., 2019). The aim of this study is therefore to report the first findings of an RCT on the effect of 6 weeks of light versus moderate physical activity embedded in a multimodal day treatment program, on selected measures of cognitive control in a sample of male multi-problem young adults (Zijlmans, van Duin, et al., 2021). Trait impulsivity, associated with externalizing behavior including antisocial personality disorder (Swann et al., 2009), was added as an additional measure of inhibitory control (Leshem, 2016) because this related trait might also benefit from increased physical activity (Ghahramani et al., 2016).
To the author’s knowledge, there are no studies examining the effect of regular exercise intensity on cognitive control and trait impulsivity in young adults, as most dose-response studies focus on acute exercise rather than regular (e.g., Davranche et al., 2015). Yet, prior observational studies in older adults indicate a positive dose-response relationship between physical activity intensity and general cognition (Angevaren et al., 2007; Brown et al., 2012). Moreover, a 12-week intervention study in older adults demonstrated greater improvements in cognition after regular high-intensity exercise compared to moderate-intensity exercise or a control group who only performed stretching (Kovacevic et al., 2020). Based on these (scarce) findings, it is hypothesized that 6 weeks of moderate embedded physical activity leads to more improvements in cognitive control (indexed as response inhibition, error processing, and cognitive interference) and higher decreases in trait impulsivity compared to light physical activity.
Methods and Materials
Participants and Treatment Setting
Participants were multi-problem young adult males (aged 18–27) recruited at the start of a multimodal day treatment program called De Nieuwe Kans (DNK; translated as “New Opportunities”). For more information on the treatment program, see: (Luijks et al., 2017; Van der Sluys et al., 2020). The multi-problem young adult males were contacted by a trained researcher at the facility within the first 2 days of their entry into the day treatment. A total of 144 young adult males were assessed for eligibility (Figure 1). Of these, 88 were randomized to the physical activity intervention, of which 48 completed baseline testing (see Table 1 for an overview of descriptives). Half of these young adult males (n = 24) completed the follow-up 6 weeks later. One additional participant was excluded from the RCT-group analysis due to being judged by the coaches and researcher as being too inactive (did not participate in any of the activities) during the physical activity intervention. The final sample was therefore N = 12 for the young multi-problem adults receiving the light-active physical activity and N = 11 for those receiving the moderate-active physical activity lessons. See Figure 1 for the CONSORT flow diagram containing a description of exclusion reasons broken down per phase per experimental group (light-active versus moderate-active).
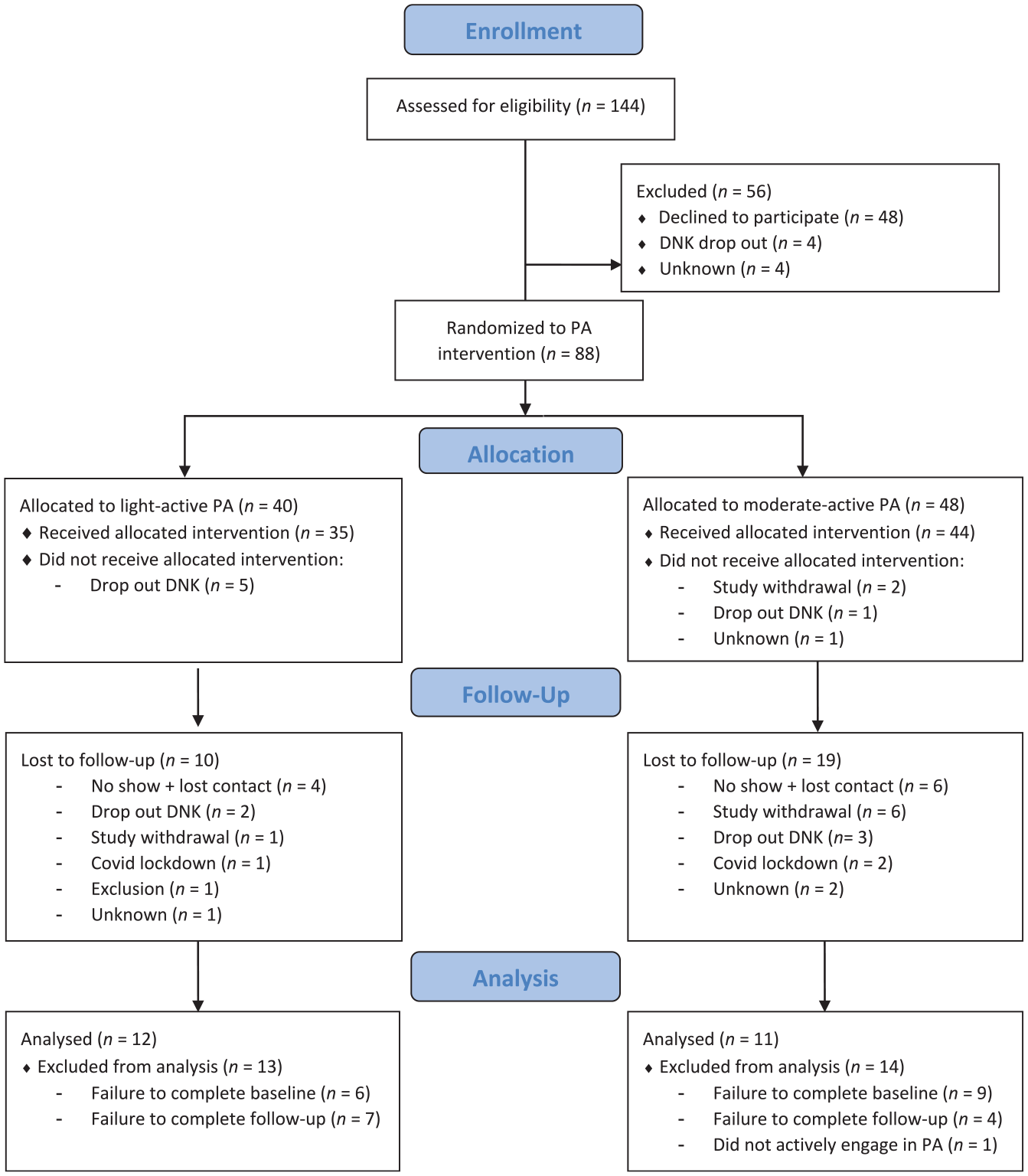
CONSORT 2010 flow diagram.
Descriptives Split Per Physical Activity Intensity (N = 23).
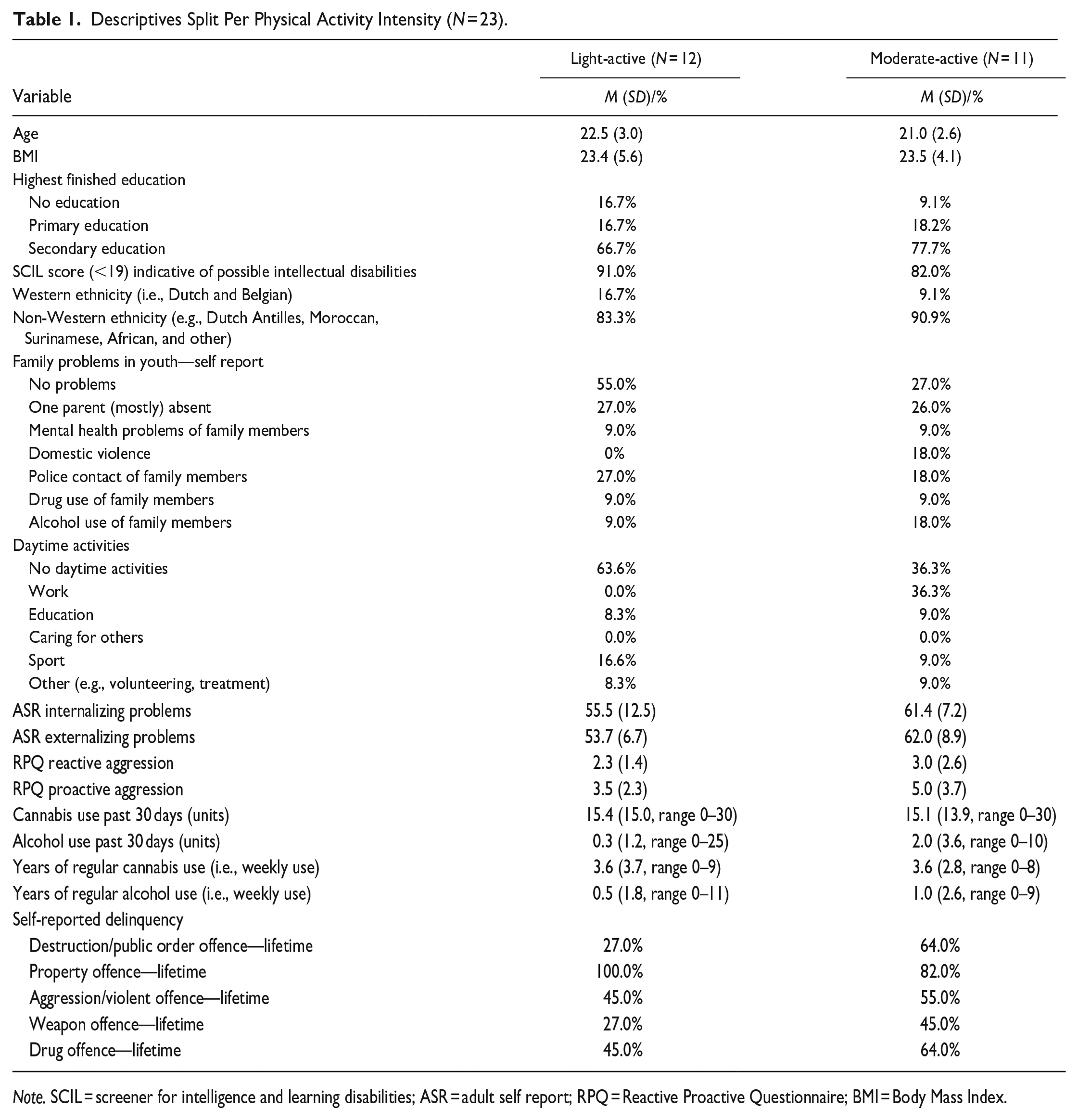
Note. SCIL = screener for intelligence and learning disabilities; ASR = adult self report; RPQ = Reactive Proactive Questionnaire; BMI = Body Mass Index.
Common reasons to be lost after initial randomization included failure to complete baseline testing within the first 2 weeks (n = 15), dropping out of the multimodal day treatment program during the intervention period (n = 11), failure to complete follow-up testing (n = 11), not responding to communication after setting an initial testing date (n = 10), and not wanting to continue with the intervention (n = 9). Other reasons were the Covid-19 lockdown (n = 3), not actively engaging during the physical activity intervention (n = 1), and having an insufficient understanding of the Dutch language (n = 1). Data on the reasons for non-response were lost for a small number of participants (n = 4).
Young male adults at DNK suffer from a variety of problems, including lack of daytime activities (such as work and education), no income, no housing, behavioral and psychological problems, substance use, and a history of delinquency (Zijlmans, van Duin, et al., 2021). This treatment program is specifically designed for young male adults with several complex issues (e.g., behavioral, psychological, and financial problems (Luijks et al., 2017; Van der Sluys et al., 2020). The goal of the intervention is to aid the multi-problem young male adults with their reintegration into society, by guiding them to education or employment and by increasing their self-sufficiency. To achieve this outcome, DNK applies a multidimensional approach including cognitive behavioral therapy, coaching, observation, and practical support. Although the program is group-oriented, they also focus on individual needs and personal goals (Luijks et al., 2017). Participants are required to follow the complete multimodal treatment for 4 days a week (9:30 AM -2:30 PM). On average, they need about 5 to 6 months to successfully obtain education or employment, thus ending the program. In some cases, the program ends with a referral to specialized (mental) health care, if this is deemed necessary and with the participants’ consent.
Study Design
The present study was a single-blind RCT design where participants, but not trainers or researchers were unaware of the treatment allocation. Participants were selected based on voluntaryism. All multi-problem young male adults starting treatment at DNK were eligible if they were physically able to follow the physical activity lessons, did not suffer from color blindness, and had sufficient knowledge of the Dutch language.
Study participants were randomly allocated to either light-active physical activity lessons (e.g., table tennis, table soccer, walking; N = 12) or moderate-active physical activity lessons (e.g., weightlifting, fitness circuit, running; n = 11). Data was collected between October 2018 and March 2020 (first lockdown due to Covid-19). All participants received physical activity lessons twice a week lasting on average 1 hr per session as part of their compulsory day treatment at DNK. Due to the complexity and severity of the problems experienced by the treatment-seekers at DNK, we chose not to withhold day treatment for a subsample of participants. It was therefore not possible to examine the effect of physical activity without day treatment. Lessons for both groups were administered at the same time but at different locations (e.g., the fitness room of DNK, outside, or the fitness center in the adjacent building). Two trained sports coaches, both staff members of DNK, delivered the lessons. The coaches were counterbalanced every 2 weeks to minimize any possible trainer effect on the RCT groups. No standardized fitness program was used as this was not compatible with the current curriculum where classes are tailored to the individual needs, but the coaches were given a list of light-active and moderate-active activities based on estimated intensity. Light-active activities included walking and cycling at a slow pace, ball games such as soccer, and recreational activities such as table tennis and table soccer. Moderate-active activities included running and cycling at a moderate pace, and circuit training (e.g., a combination of weightlifting and light to moderate cardio including dumbbell curls, squats, and shadow boxing at a moderate pace). A subgroup of the study participants (n = 20) was required to wear a Polar A360 activity tracker on their wrist during the physical activity lessons to measure heart rate. Due to financial constraints, it was not possible for all participants to wear an activity tracker.
The study has been approved by the Medical Ethical Committee of the VU University Medical Center (registration number 2013.422—NL46906.029.13). Participants provided written informed consent. They received reimbursement of 20 euros for study participation (i.e., completing the computerized cognitive control tests and questionnaires at baseline and follow-up).
Procedure and Study Outcomes
All outcome variables were measured within 2 weeks of the start of the multimodal day treatment (baseline measured as the first day of entry, median days between entry and testing = 8 days, N = 35) and 6 weeks later (follow-up). Limiting this to the final sample of 23 participants shows a greatly reduced time between entry and baseline testing, with a median of 3.5 days, suggesting a possible selection bias with participants motivated to follow the multimodal day treatment program. None of the participants received any physical activity lessons before their baseline measurements. Participants were tested in their free time between classes or at the end of the day when their mandatory classes and treatment at DNK were finished. All measurements were performed in one setting, in a quiet room at DNK. Laptops were used to administer the cognitive control experiments and the questionnaires.
Cognitive Control
Cognitive control (indexed as response inhibition, error processing, and cognitive interference) was measured with three commonly used reaction-time experiments using E-Prime 3.0 software (Psychology Software Tools, Pittsburgh, PA) and a QWERTY keyboard.
Response inhibition was measured with a Go/NoGo task (see Luijten et al., 2013; Zijlmans, Marhe, et al., 2021 for more information). In short, participants were required to press the spacebar in response to a vowel (Go trials) and refrain from any response if the vowel was a repetition of the previously shown vowel (NoGo trials). Participants were shown a total of 927 trials of which 12% (110) were NoGo trials. Jitter was introduced in the number of Go trials between the NoGo trials (M = 7.25, range 3–16), to present the NoGo trials unpredictably. The experiment consisted of five blocks, divided by 15 s rest periods. The stimuli were presented at 1 Hz (i.e., every second). The duration of the stimulus presentation was 700 ms. The stimulus did not disappear after a response. This was followed by a blank screen (300 ms). The response window was set at 1000 ms (stimulus presentation + blank screen). NoGo accuracy (percentage of correctly refrained responses on NoGo trials) was calculated as a conventional behavioral measure of response inhibition (e.g., Aron & Poldrack, 2005; Luijten et al., 2011; Zijlmans, Marhe, et al., 2021). Higher accuracy on NoGo trials is interpreted as better response inhibition.
Error processing was measured with a Flanker task previously described in Zijlmans et al. (2019). To summarize, participants were shown letter strings (HHHHH, SSSSS, HHSHH, SSHSS). They were instructed to press the h or s, corresponding to the middle letter of the string. A total of 400 trials (200 congruent, i.e., HHHHH, SSSSS and 200 incongruent, i.e., HHSHH, SSHSS) were presented at random, divided into five blocks with 15 s rests in between blocks. One trial consisted of 52 ms stimulus presentation, followed by 648 ms blank screen. Participants could respond during the stimulus presentation and the blank screen (i.e., response window set at 700 ms). The stimulus did not disappear after a response. The inter-stimulus interval was 1000 ms. Post-error slowing (post-error reaction time—post-correct reaction time) and correctness effect (reaction time correct trials - reaction time incorrect trials) were calculated as measures of error processing, with higher scores indicating better error processing. Total accuracy was collected as a measure of performance.
Interference or Stroop effect was measured with a Stroop Color-Word task (see also: van der Sluys et al., 2022). This measure represents the difference between reaction time on trials with incongruent color of ink and written words and the reaction time on trials with congruent ink and written words, and it is commonly used to assess the ability to inhibit cognitive interference (Scarpina & Tagini, 2017). Participants were required to react to the color of the ink (red, blue, yellow, green) whilst ignoring the written words (red, blue, yellow, green). Color and words were congruent (48 trials: ink and written word match) or incongruent (144 trials: ink and written word do not match), presented in random order, and divided into two blocks. Participants reacted by pressing a letter (d, f, j, k) corresponding to the colored ink. The trial started with a fixation cross (250 ms), followed by the stimulus (shown until the participant pressed a letter, with a maximum stimulus presentation of 3000 ms). Interference effect was calculated with the following formula: reaction time incongruent trials—reaction time congruent trials. A higher score is interpreted as increased (worse) cognitive interference.
Questionnaires
Questionnaires were administered by trained researchers in the form of a structured interview using Castor EDC (Castor EDC, 2019). Impulsivity was measured with the total score on the Dutch Baratt Impulsiveness Scale (BIS-11; Lijffijt & Barratt, 2005; Patton et al., 1995). The total score has a Cronbach’s alpha of .71 and sufficient construct validity, as measured in a male forensic population (Haden & Shiva, 2008). Furthermore, we conducted several questionnaires to describe the multi-problem character of the sample. These included a socio-demographic questionnaire to measure age, weight, height, ethnicity, highest finished education, family problems, and daytime activities (Table 1). Second, a screener for Intelligence and Learning Disabilities (SCIL 18+; Nijman et al., 2018) was used to screen for mild to borderline intellectual disabilities. The total score was included, with a score of 19 or lower indicating the possible presence of intellectual disabilities. Internal consistency for the total score as expressed with Cronbach’s alpha is good (.83: Nijman et al., 2018). Third, psychopathology was measured with the Internalizing Problems score (e.g., anxiety and depression) and the Externalizing Problems score (e.g., rule-breaking and aggressive behavior) from the Adult Self-Report (ASR: Achenbach & Rescorla, 2003). Cronbach’s alpha for these scales is around .85 (de Vries et al., 2020). Fourth, two subscales of the Dutch Reactive Proactive Aggression Questionnaire (RPQ: (Cima et al., 2013; Raine et al., 2006) were included to measure reactive (e.g., premediated) and proactive (defensive) aggression. The internal consistency of the Dutch version is good, with Cronbach’s alpha’s for the two subscales being .84 and .86, respectively (Cima et al., 2013). Fifth, regular cannabis and alcohol use (i.e., the number of years of weekly usage) and the number of units consumed in one month were assessed with Measurements in the Addictions for Triage and Evaluation Questionnaire (MATE: Schippers & Broekman, 2014). The MATE has good inter-rater reliability ranging between .75 and .92 and adequate validity (Schippers et al., 2010). Lastly, we included the WODC Self-reported Delinquency Questionnaire (Kruissink & Essers, 2004) to measure lifetime number of self-reported acts of delinquency on multiple domains. The percentage of young adults reporting at least one instance of delinquent behavior is reported. To the author’s knowledge, there are no psychometric properties for this instrument available.
Physical Activity
Last, we included a self-report measure of physical activity to control for individual differences in baseline physical activity level (Gomez-Pinilla & Hillman, 2013; Verburgh et al., 2014), as measured with the International Physical Activity Questionnaire—long version (IPAQ: Hagströmer et al., 2006). Test-retest reliability of the total and activity scores are fair to good (r = 0.49-0.81) with weak to moderate concurrent validity (r = −.07 to .54).
Metabolic Equivalents (METs) minutes per week were used as a measure of physical activity level. To measure differences in intensity between the two groups, we measured heart rate during physical activity with Polar activity trackers. A weighted mean average (i.e., the relative average heart rate during the lessons taking into account the frequency and duration of the lessons) was calculated for each group.
Adherence to the Physical Activity Intervention
Adherence was defined as the percentage of completed sessions (i.e., actively engaging in the instructed light-active or moderate-active activities for at least 75% of the time of a session on average) post-treatment. This was measured using daily lesson recording sheets completed by the coaches and the researchers. Participants who were not actively engaged for at least 75% per lesson on average were excluded from the analysis. This resulted in the exclusion of 1 participant who finished follow-up measurements.
Data Analysis
All statistical analyses were conducted with IBM SPSS version 20.0 (IBM Corp, n.d.). To test for successful randomization, one multivariate analyses of variance (MANOVA) and one multivariate analyses of covariance were performed to identify any pre-intervention differences between the light-active and moderate-active group. The MANOVA compared the light-active and moderate-active group on the descriptive baseline data (N = 23) as described in Table 1. Pre-intervention group differences between the light-active and moderate-active group on the variables of interest were measured with a MANCOVA on baseline data (start of treatment) the selected indices of cognitive control (i.e., NoGo accuracy, Flanker total accuracy, Flanker post-error slowing, Flanker correctness effect, Stroop interference) and trait impulsivity (i.e., BIS-11 total score), controlling for physical activity level (i.e., MET minutes per week). Furthermore, a repeated measures (RM) MANCOVA was performed on the same set of measurements of cognitive control (i.e., NoGo accuracy, Flanker total accuracy, Flanker post-error slowing, Flanker correctness effect, Stroop interference) and trait impulsivity (i.e., BIS-11 total score), to examine any differences between the light-active and moderate-active group (between-subjects factor) with time (baseline to post-treatment 6 weeks later) as within-subjects factor, controlling for baseline MET minutes per week. Any significant MAN(C)OVA results were further examined with post-hoc univariate testing. The level of significance was set at p = .05.
Results
Participants were between 18 and 27 of age (M = 21.1, SD = 2.7). See table 1 for a detailed description of sample characteristics.
The weighted average heart rate during physical activity was 112.28 beats per minute (SD = 9.53) in the light group and 115.96 beats per minute (SD = 6.53) in the moderate group. An independent sample t-test revealed the difference was not significant (Mdiff = −3.70, p = .134, Cohen’s d = -0.468). Because of this and the relatively small sample size per group (Nlight = 12 and Nmoderate = 11), we decided to also report the main effect of time in the RM MANCOVA, to examine if there were any treatment effects in the complete sample.
Effect of 6 weeks Physical Activity
A MANOVA was run to compare the light-active and moderate-active group on all descriptive baseline variables (N = 23) including socio-demographics (i.e., age, BMI, education, ethnicity), total SCIL score, psychopathology (i.e., Internalizing Problems and Externalizing Problems score), aggression (i.e. Reactive Aggression subscale and Proactive Aggression subscale), regular substance use (i.e., years of weekly alcohol use, years of weekly cannabis, consumed units past 30 days) and several forms of self-reported delinquency. See Table 1 for a complete overview of all variables included in the MANCOVA. Results indicate homogeneous groups in terms of their descriptive and multi-problem character (F (20, 1) = 0.796, p = .724; Wilk's Λ = .059, partial η2 = .724). The MANCOVA on the dependent variables also did not show any significant pre-intervention group differences in cognitive control and trait impulsivity, after controlling for MET minutes per week (F (6, 40) = 0.567, p = .754, Wilk’s Λ = .922, partial η2 = .078), indicating successful randomization.
After controlling for baseline MET minutes per week, results from the RM MANCOVA (Nlight = 12 and Nmoderate = 11) revealed a significant main effect of time on cognitive control (F (6, 15) = 2.820, p = .048; Wilk’s Λ = 0.470, partial η2 = .530). More specifically, when looking at the individual variables with post-hoc univariate testing, we found increased NoGo accuracy (Mdiff = .05, F (1) = 5.013, p = .037, partial η2 = .200) and decreased Stroop interference effect (Mdiff = −41.4, F (1) = 11.402, p = .003, partial η2 = .363). No effect was observed on error processing, although we did find increased total Flanker accuracy (Mdiff = .05, p = .031, F (1) = 5.418, partial η2 = .213). See also Table 2 for an overview of mean scores at baseline and after 6 weeks. There was no significant main effect of group (F (6, 15) = 2.820, p = .048, Wilk’s Λ = 0.470, partial η2 = .530), that is, the treatment effect was not significantly different between the two groups. The time by group interaction was also not significant (F (6, 15) = 0.838, p = .560, Wilk’s Λ = 0.749, partial η2 = .251).
Descriptives of Main Outcome Measures Over Time (N = 23).
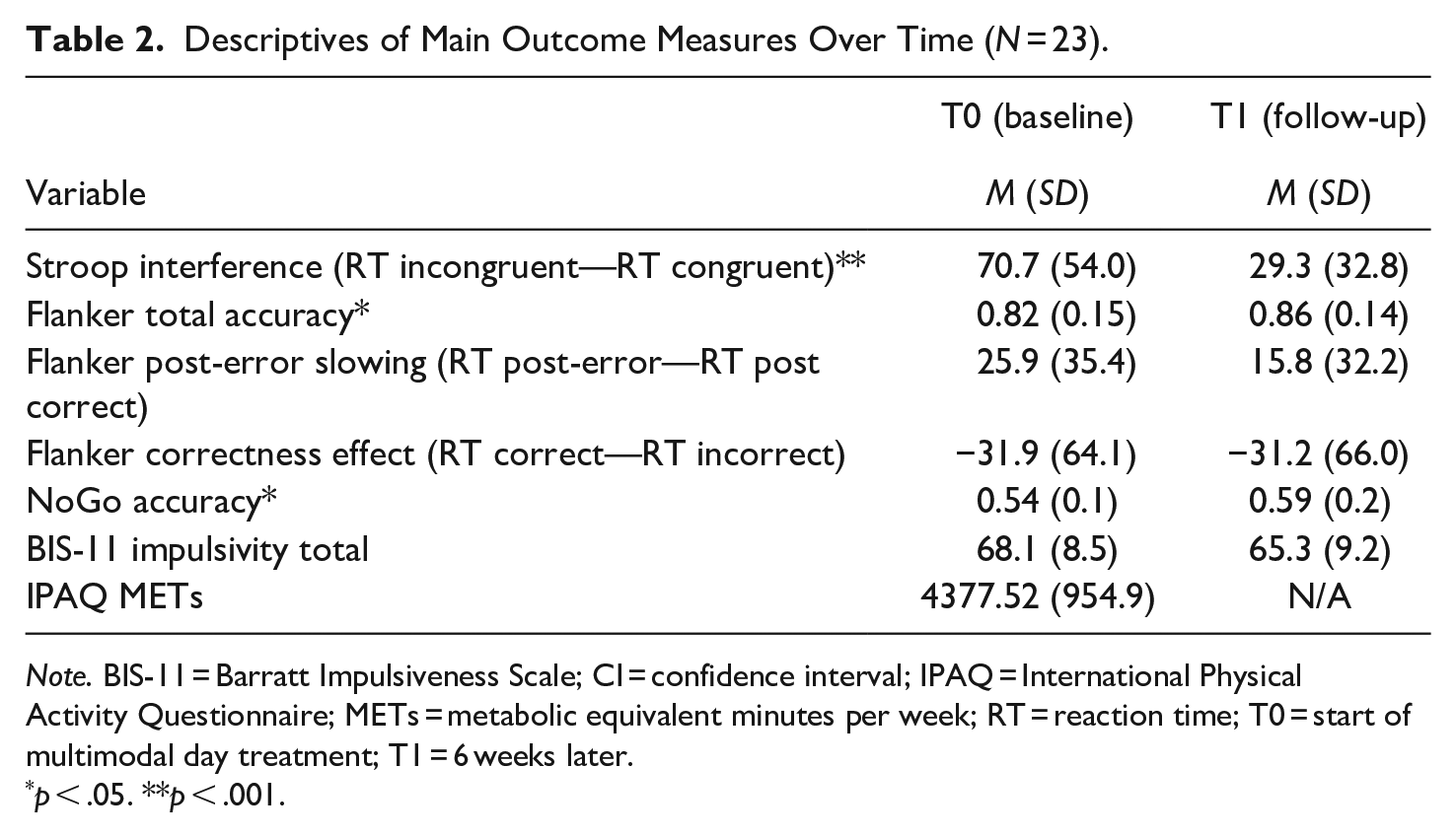
Note. BIS-11 = Barratt Impulsiveness Scale; CI = confidence interval; IPAQ = International Physical Activity Questionnaire; METs = metabolic equivalent minutes per week; RT = reaction time; T0 = start of multimodal day treatment; T1 = 6 weeks later.
p < .05. **p < .001.
These results indicate that overall, there was an improvement in NoGo accuracy, total Flanker accuracy, and Stroop interference from pre- to post-treatment, however, the effect of treatment did not differ between the light-active and moderate active group, possibly because the difference in intensity was not significant. The current findings should be interpreted carefully, taking into account the limitations (including the small sample size and the lack of a control group) elucidated in the discussion section.
Adherence to the Physical Activity intervention
The median intervention adherence from baseline to end of the 6-week intervention was 33% of completed lessons (i.e., lessons with at least 75% active participation) among the group of randomized participants (N = 88). Twenty-nine percent of the participants attended at least half (i.e., 6 or more) of the prescribed physical activity lessons, 62% attended 5 or fewer sessions, and 9% did not attend any of the sessions. Excluding participants who dropped out of the multimodal day treatment program (and thus could not continue with the physical activity intervention) did not increase the median adherence. Including only the 23 participants of the final sample used in the analysis resulted in a median intervention adherence of 50% of the lessons completed, suggesting a possible selection bias. One participant completed all the measurements yet was excluded from the analysis as he failed to participate at least 45 min on average per 60 min of lesson (i.e., 75% active participation). An independent sample t-test showed no difference in adherence rates between the light-active (M, SD) and moderate-active (M, SD) group (Mdiff = −0.55, t(61) = 0.753, p = .455, Cohen’s d = −0.190).
Discussion
The current study investigated whether 6 weeks of light-active versus moderate-active physical activity embedded in a multimodal day treatment program would improve cognitive control (i.e., response inhibition, error processing, and cognitive interference) and trait impulsivity in multi-problem young male adults. Due to several limitations (e.g., small sample size, no no-exercise control group, intervention embedded in larger program, described in more detail below), it is not possible to completely confirm or discard our hypothesis. Given these limitations, we did not observe a difference between the light-active and moderate-active on executive functioning and trait impulsivity after 6 weeks of physical activity compared to the light-active group. However, both groups demonstrated enhanced cognitive control post-treatment, specifically improved inhibition and improved (i.e., lower) cognitive interference. No effect on error processing was observed, although we did found improved performance on the error-processing task (measured as improved accuracy) in the group as a whole. We also found no improvement on trait impulsivity. It is possible that the current intervention was too short to elicit any changes on this personality trait as prior research suggest a persistent intervention of at least 18 months is needed to alter personality traits (Bleidorn et al., 2019).
To the author’s knowledge, this study is the first to examine the effect of a physical activity intervention embedded in a multimodal day treatment program on cognitive control in young male adults with multiple problems including aggression, substance use, and a history of delinquency. As we did not observe a significant difference in heart rate between the two physical activity groups, it is possible that the current activities (e.g., table tennis, table soccer, walking, vs. weightlifting, fitness circuit, running) were too similar in terms of intensity to elicit any differences in treatment effect (Kaiser et al., 2022), and more research is needed to establish if there is a dose-response association. Despite the non-significant effect of intensity, our findings point to the same direction as existing intervention studies in healthy children and older adults (Alvarez-Bueno et al., 2017; Chen et al., 2020; Liu et al., 2020), suggesting treatment programs including physical activity components may exert a positive influence on (some) cognitive functions in young male adults.
The present study is not without limitations, with the most prominent being the fact that the physical activity intervention was embedded in a multimodal day treatment program (i.e., practical guidance, lessons including culture, cooking, and cognitive behavioral therapy, Luijks et al., 2017) and the lack of a control group without physical activity. Caution is thus advised interpreting current results, as it is not possible to completely discern any possible effects of the multimodal treatment from the physical activity intervention. Although this complicates any causal statements about the isolated effect of physical activity, it also contributes to our understanding of an ecologically valid sample of treatment-seeking young male adults with complex and co-morbid problems. To the best of our knowledge, no studies have been conducted on the effects of similar multimodal treatments on cognition. However, related studies on the efficacy of cognitive behavioral therapy (i.e., one of the main components of the multimodal treatment) did not uncover a significant effect on cognitive control in adults with obsessive-compulsive disorder (Vandborg et al., 2015) or attention deficit disorder (Virta et al., 2010), suggesting this may also be the case for our multi-problem sample. Other effective approaches to increase neurocognitive functioning include mindfulness (Larson et al., 2013) which is not a part of the current treatment curriculum. In contrast, physical activity has been known to improve cognitive control in young adults (Stern et al., 2019), suggesting physical activity may have (partially) contributed to the positive effect on cognitive interference, although future studies including a no-exercise control group are needed to test this theory.
It is also important to discuss the relatively low number of participants who completed the follow-up testing (27% of the 88 young male adults who were initially randomized). We used small financial incentives (5 euros for making the appointment and 5 euros for completing the tests) and reminders to encourage participants to complete both baseline and follow-up testing (Booker et al., 2011). In addition, we collected multiple sources of contact information (Stewart et al., 2021) and tried to accommodate the young male adults as much as possible regarding the time and place of the testing. Other types of incentives or more frequent contact to stimulate bonding (Booker et al., 2011) may be more effective to maximize retention. Regardless, it is not uncommon for effect studies with similar hard-to-reach or at-risk populations to have small sample sizes ranging between 10 and 20 participants (e.g., see Lubans et al., 2012; Sanchez-Lastra et al., 2019), for example, due to frequent changing or lack of address and phone numbers, starting a new day treatment and not having enough time, and having physical and mental health problems (Fahmy et al., 2022).
Last, although the physical activity lessons were mandatory for all young male adults starting the multimodal day treatment (independent of study participation), we observed a relatively low adherence (i.e., only 29% of the initially randomized young male adults attended at least half of the lessons), indicating low compliance and/or enforcement of the compulsory nature. Although we did not question participants about their reasons for (not) participating, we observed a general lack of motivation to exercise in most treatment seekers during the multimodal day treatment (independent of study participation or allocation). Including only participants who are willing to exercise may increase adherence, yet it would also introduce bias. Another option is to increase motivation, for example through gamification (Kari et al., 2016) or physical performance goals (Gorny et al., 2021). Low adherence is a continuing problem in physical activity RCTs (Eldridge et al., 2016; Slade et al., 2016) and further research should be undertaken to investigate factors associated with low adherence, such as personality (Lewis & Sutton, 2011).
Future studies should focus on discerning the effects of physical activity with and without similar multimodal day treatment programs and with the inclusion of a no-exercise control group to establish a causal relationship between physical activity and cognitive control. Special attention should be given to overcoming barriers to adherence such as lack of motivation or time constraints, to enhance the effectiveness. Other important factors to take into account are the exploration of potential confounding factors (such as physical health, willingness to change, or affinity with sports) and their unique contribution to the treatment effect, as these were not tested in the current design. Last, it is worthwhile to explore any differences in sex, as our sample included only males and sex is known to affect treatment effects of exercise on general cognition in older adults (e.g., Barha et al,. 2017) and on attention (but not cognitive flexibility) in adolescents and young adults (Haverkamp et al., 2020), suggesting possible different effects on cognitive control in female young adults.
In sum, based on these limitations, it is hard to draw any firm causal conclusions about the effect of physical activity on cognitive control. However, together with prior promising studies, the current results are pointing to the direction that engaging in physical activity (embedded in a multi-modal day treatment program) for 6 weeks may benefit cognitive control in multi-problem young male adults, even at light intensity. Based on these findings, it is recommended to explore opportunities to integrate physical activity components within larger treatment programs for at risk-populations with executive dysfunctioning, for example in a correctional settings such as prison (Meijers et al., 2015). In addition, it is recommended to tailor these treatments to individual needs, for example by early identification of predictors of adherence and treatment outcome including motivation, as individually tailored treatments are known to have increased effectiveness (Frick, 2016; Rubin et al., 2006).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by Reclassering Nederland (the Dutch probation service) and the Arnold Oosterbaan Hersenstichting. They were not involved in the study design, manuscript drafting, data collection, or analysis.