
Abstract
Women who use violence represent one of the fastest growing groups within the Australian prisoner population, including Aboriginal women who are more likely to be incarcerated than non-Aboriginal women for violent crimes. Many incarcerated women report histories of adverse childhood experiences (ACEs) and intimate partner violence. This exploratory study examines baseline data from a sample of 167 women in 3 Western Australia women’s prisons enrolled in a gender-specific violent behavior program. It describes their exposure to intimate partner violence, head injury, and childhood adversities. Overall, 94% of women had experienced at least one childhood adversity (median 6), and 94% reported being a victim of physical violence by a current or former intimate partner. Aboriginal women were more likely than non-Aboriginal women to report that a family member was incarcerated as a child (p = .001). There was an association between an increased number of ACEs and head injury with a loss of consciousness (p = .008). Overall, these results present a harrowing picture of childhood exposure to adversity and violence in adulthood. Successful rehabilitation of women incarcerated for violent crimes should be cognizant of the histories of extreme violence endured by most of these women.
Keywords
Introduction
Women represent one of the fastest growing groups in the Australian prisoner population (Australian Institute of Health and Welfare, 2020). Between 2010 and 2022 female incarceration for violent offenses in Australia increased by 92% (Australian Bureau of Statistics, 2010, 2022) while the male population between 2009 and 2019 increased by 45% (Australian Institute of Health and Welfare, 2020). In the context of Australia, this trend cannot be explained as natural population growth (Australian Institute of Health and Welfare, 2020; Walmsley, 2017).
For the rest of this article, when we speak of Aboriginal women, we include those who identify as Aboriginal, Torres Strait Islander, and Aboriginal and Torres Strait Islander, and use the term interchangeably with Indigenous. Aboriginal women are significantly over-represented in Australian prisons accounting for more than one third of incarcerated females, despite comprising only ~3% of Australia’s total female population (Australian Institute of Health and Welfare, 2020; Tubex & Cox, 2020). Similarly, among men Aboriginal and or Torres Strait Islander males in prison account for 31% of the total prison population (Australian Institute of Health and Welfare, 2020). Over the past decade the number of Aboriginal women incarcerated for violent offenses increased by 66% compared with a 20% increase among non-Aboriginal women (Australian Bureau of Statistics, 2010, 2022). As a subgroup, Aboriginal woman including those who are incarcerated for violent offenses, are growing at a rapid rate compared to any other subgroup in Australian prisons (Tubex & Cox, 2020). As Tubex and Cox (2020) report, there is limited research into the trends pertaining to Aboriginal women and their increasing incarceration rates in Australia. Sullivan et al. (2019) have described that this increase may be attributed to the residual, accumulative effects of colonization and post-colonial policies and procedures including the over-policing of Aboriginal women for trivial or minor crimes. These effects continue to extend into the lives of Aboriginal women, their children, families and community, as intergenerational trauma (Atkinson et al., 2014; Sullivan et al., 2019). Whilst the experience of trauma is not exclusive to members of any given cultural, racial or religious group in Australia, trauma-related behaviors such as the use of violence and corresponding victimization is prevalent among the most disadvantaged and disconnected communities (Atkinson et al., 2014).
Although it is recognized that there are different gender pathways into criminal activity (Saxena & Messina, 2021), the literature describes that female criminogenic needs assessment modeling which underpins offending risk for women, is primarily designed through the use of male samples (Fleming et al., 2001; Wanamaker & Brown, 2022), resulting in non-gender specific recidivism reduction programs not meeting the needs of incarcerated women, particularly those at a high risk of reoffending (Fleming et al., 2001; Saxena & Messina, 2021). Prison programs addressing violence have stemmed primarily from the needs of male offenders, focusing on the discontinuation of cyclic patterns of violence predominately relating to family and sexual violence, and aggression (Rossegger et al., 2009). Notwithstanding the victimization and oppression widely experienced by those in prison (Australian Institute of Health and Welfare, 2020), there is disparity between male and female needs when addressing violence and recidivism (Craig et al., 2019; Gower et al., 2023; Jones et al., 2020; Saxena & Messina, 2021). The relationship between substance use and offending is well established (Covington, 2015; Eaves et al., 2020; Egeressy et al., 2009; Felitti et al., 1998; Loxton et al., 2021; Messina et al., 2016), where misuse is understood to be a symptom of trauma (Loxton et al., 2021; Messina et al., 2016; Saxena & Messina, 2021) and common among those who have experienced adversity during childhood (Craig et al., 2019; Eaves et al., 2020). A report undertaken by the Office of the Inspector of Custodial Services (2014) in Westerna Australia, found that standard (i.e., non-gender specific) interventions for high-risk substance use resulted in a lower recidivism rate for males, yet higher rates for women.
Childhood physical and sexual violence and abuse, neglect, and household dysfunction feature prominently in the backgrounds of incarcerated women across all cultures (Egeressy et al., 2009; Fleming et al., 2001; Friestad et al., 2014; Loxton et al., 2021; Messina et al., 2016; Messina & Zwart, 2021). Such exposures have been termed “adverse childhood experiences” (ACEs), and represent well documented risk factors for poor education and employment outcomes, health risk behaviors including alcohol and other drug use, health conditions including heart disease and mental illness, homelessness, victimization, and acts of violence into adulthood (Craig et al., 2019; Friestad et al., 2014; Jones et al., 2018, 2020; Loxton et al., 2019; Messina & Calhoun, 2021). ACEs include witnessing or directly experiencing physical, emotional and sexual abuse; physical and emotional neglect; witnessing violence in the home; residing with a family member suffering from a mental illness or who has attempted suicide; the separation or divorce of parents; exposure to household members using alcohol and illicit substances and having a family member be incarcerated (Felitti et al., 1998). ACEs may have a profound and lasting negative impact on individuals’ abilities to successfully function and flourish from childhood into adulthood (Stensrud et al., 2019).
A recent study into the health behavior of 8,607 young Australian women (Loxton et al., 2021), identified that in those aged between 20 and 25 years, 41% reported no adverse events at all, 26% reported one ACE, 23% experienced between two and three, and 10% experienced more than four ACEs during childhood. ACEs are not uncommon in the general population, especially if limited to three or fewer ACEs (Jones et al., 2020; Loxton et al., 2019, 2021; Stensrud et al., 2019). Up to 90% of incarcerated female populations in the United States are reported to have experienced childhood adversity at elevated levels (Jones et al., 2018, 2020).
Previous studies describe a dose-response relationship between ACEs, socio-economical vulnerabilities and negative health impacts (e.g., substance use) as well as victimization in the form of domestic and intimate partner violence (Dube et al., 2002; Loxton et al., 2019; Messina et al., 2016; Stensrud et al., 2019). Cyclic patterns of victimization, beginning in childhood and repeated throughout adult relationships, are considered a contributing factor for female anger and aggression (Kubiak et al., 2017; Messina & Calhoun, 2021).
Importantly, research indicates that the accumulation of ACEs and victimization throughout childhood extending into adulthood in the form of domestic and intimate partner violence, lays the foundation for female aggression and perpetration of violence (Craig et al., 2019; Friestad et al., 2014; Messina & Calhoun, 2021). Ma et al. (2019) report the negative effects of adversity during childhood development and corresponding anatomical structural changes in the brain. These changes are described as alterations in the development of regions of the brain associated with both cognitive and emotional function including executive functioning, increased hypervigilance, and impulsivity (Ma et al., 2019; Whittle et al., 2013). The accumulation of ACEs may increase anti-social behaviors resulting in an increased risk of injury, including victimization leading to traumatic brain injury (Brewer-Smyth et al., 2016; Ma et al., 2019; Schofield et al., 2006).
These predominately gendered factors pose significant challenges for the way females are managed on entry into the justice system, supported and rehabilitated in Australian prisons (Craig et al., 2019; Friestad et al., 2014; Messina & Calhoun, 2021). The literature is limited on female use of violence and childhood trauma (Saxena & Messina, 2021; Tubex & Cox, 2020), and historically interventions have been developed to address the needs of incarcerated women who are both victims and perpetrators in the prevention of violence (Kubiak et al., 2016; Messina et al., 2016). Yet growing evidence suggests that programs developed which privilege the female experience of victimization and their unique criminogenic needs, are demonstrating improved outcomes extending beyond the reduction in recidivism by comparison to gender-neutral interventions (Kubiak et al., 2016; Messina & Calhoun, 2021; Messina & Zwart, 2021). While there is some existing evidence illustrating the prevalence of ACEs among Australian prisoners more broadly (Egeressy et al., 2009), little information exists regarding the burden of ACEs among incarcerated females in Australia incarcerated for violent offenses. Further, national data and literature examining the confluence of gender, ACEs, cultural status (Aboriginality), and the use of violence, is limited (Tubex & Cox, 2020). This baseline exploratory study examines the prevalence of ACEs, sociodemographic characteristics, and criminogenic factors in a sample of Aboriginal and non-Aboriginal women in Western Australian prisons, who use violence.
Methods
Study Design
We used data from a sample of females incarcerated for current or historical (˂5 years) violent offenses, who participated in a gender-specific manualized trauma-informed intensive intervention in Western Australia, as described by Covington (2015). Modifications were made prior to, and during the initial pilot phase to adapt the program for the Australian context and ensure it is culturally safe for Aboriginal women.
Ethics
This research received ethics approval from Curtin University (HR88/2016); the West Australian Aboriginal Ethics Committee (Ref. 704).
Setting
Beginning in October 2017, both Aboriginal and non-Aboriginal women were recruited from three adult women’s prisons in WA to participate in the intervention.
Recruitment
One hundred sixty-seven participants were recruited between October 2017 and June 2021. Inclusion criteria required women to have at least one prior conviction for a violent offense, as classified by the Australian and New Zealand Standard Offense Classification codes 01-06 (01 homicide and related offenses; 02 acts intended to cause injury; 03 Sexual assault and related offenses; 04 dangerous and negligent acts endangering persons, 05 abduction, harassment, and other offenses against the person, and 06 robbery, extortion and related offenses), have a minimum of 3 months remaining on their current sentence, willing to have a baseline interview upon entry into the program, and able to provide informed consent. Exclusion criteria included severe mental illness or profound cognitive impairment, an inability to communicate in English, and subject to deportation upon release. Participants were initially identified for the program by WA Corrective Services staff, and subsequently approached by research officers to establish a willingness to participate and to be screened for eligibility. Recruitment also occurred through promotional posters and word-of-mouth within the three prisons. Offending was objectively verified through the administrative Total Offender Management Solution (TOMS) database held by WA Corrective Services.
Data Collection and Measures
Baseline structured screening and interviews were conducted by research officers employed by the study with individuals in a private setting within the prison complex. Interviews typically took between 45 min and 2 hr to complete. Interviews included standardized self-report questionnaires covering socio-demographic characteristics, and histories of violence perpetration and victimization; criminogenic risks including educational attainment, juvenile offending history, substance use, child protective services involvement and family removal (many Aboriginal and/or Torres Strait Islander children were forcibly removed from their families as a result of government policies that spanned more than 60 years from 1910 into the 1970s; and family and intimate partner violence including head-injury and non-fatal strangulation. Non-fatal strangulation screening was introduced to the baseline questionnaires as a separate self-reporting questionnaire after it emerged as a significant issue on the Intimate Partner Violence Screening Tool. The above events are not necessarily mutually exclusive however screened for separately. Adverse events in childhood (defined as an adverse event occurring before the age of 18 years) across the domains of abuse, neglect, and household dysfunction were measured by the Adverse Childhood Experience Questionnaire (Friestad et al., 2014; Jones et al., 2018). Some respondents did not complete all the questionnaires and were omitted from the analysis where applicable.
Analysis
Sociodemographic characteristics, incarceration history, and substance use at baseline, as well as screening data on the prevalence of adverse childhood experiences, intimate partner violence and injury, were summarized by descriptive statistics. Differences between Aboriginal and non-Aboriginal women and grouped ACE data in categorical variables were assessed using Fisher’s exact and chi-square test of association with 95% confidence intervals (95% CI) calculated around each estimate. Continuous variables were presented as medians with interquartile range (IQR) and p-values calculated from the Wilcoxon–Mann–Whitney test using Stata BE Version 17.0. (StataCorp, 2021). Statistical significance was set at two-sided, p < .05.
Demographics
Overall, 167 women (68% Aboriginal) were included in the baseline study. The median age of the sample at baseline was 33 years (IQR 29–40) (Table 1). Eleven percent of Aboriginal women were removed to a mission and placed in care as a child, with over half reporting that a family member or relative had been removed to a mission. Unstable housing (sleeping rough, shifting between relatives, in crisis accommodation) prior to their incarceration was reported by 30%. Eighty percent of women had at least one child, however, 59% of them reported that their children were not in their care prior to prison. Over 40% had a history of being in juvenile detention, with 18% reporting that their current incarceration was a result of breaching an existing order. Non-alcohol substance use was widespread among participants (69%), with stimulants (87%) and cannabis (64%) identified as the most used substances. Seventy-six percent of participants reported ever injecting substances.
Sociodemographic Characteristics of Female Participants (n = 167) Screened for Participation.
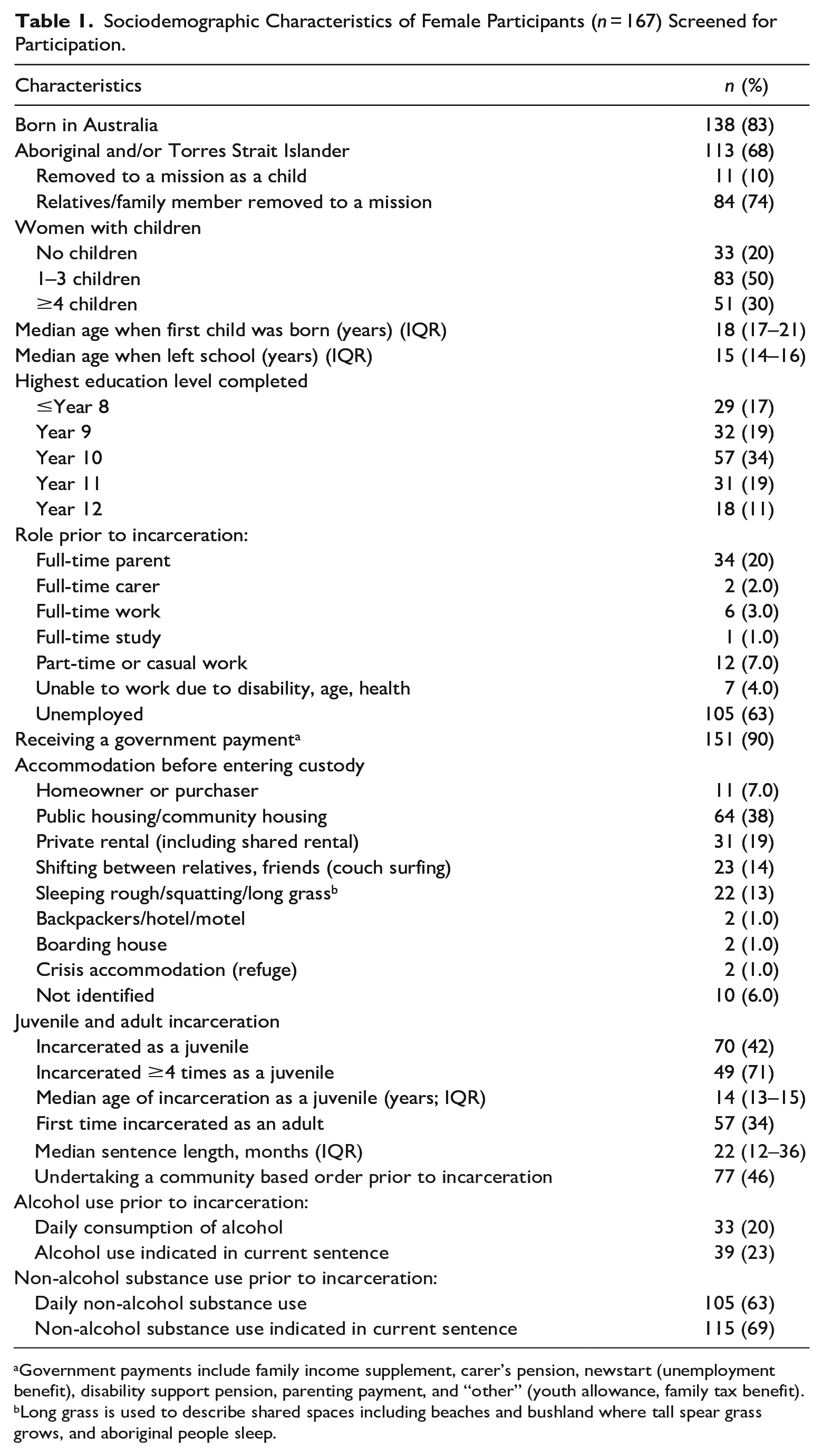
Government payments include family income supplement, carer’s pension, newstart (unemployment benefit), disability support pension, parenting payment, and “other” (youth allowance, family tax benefit).
Long grass is used to describe shared spaces including beaches and bushland where tall spear grass grows, and aboriginal people sleep.
Results
Adverse Childhood Experiences
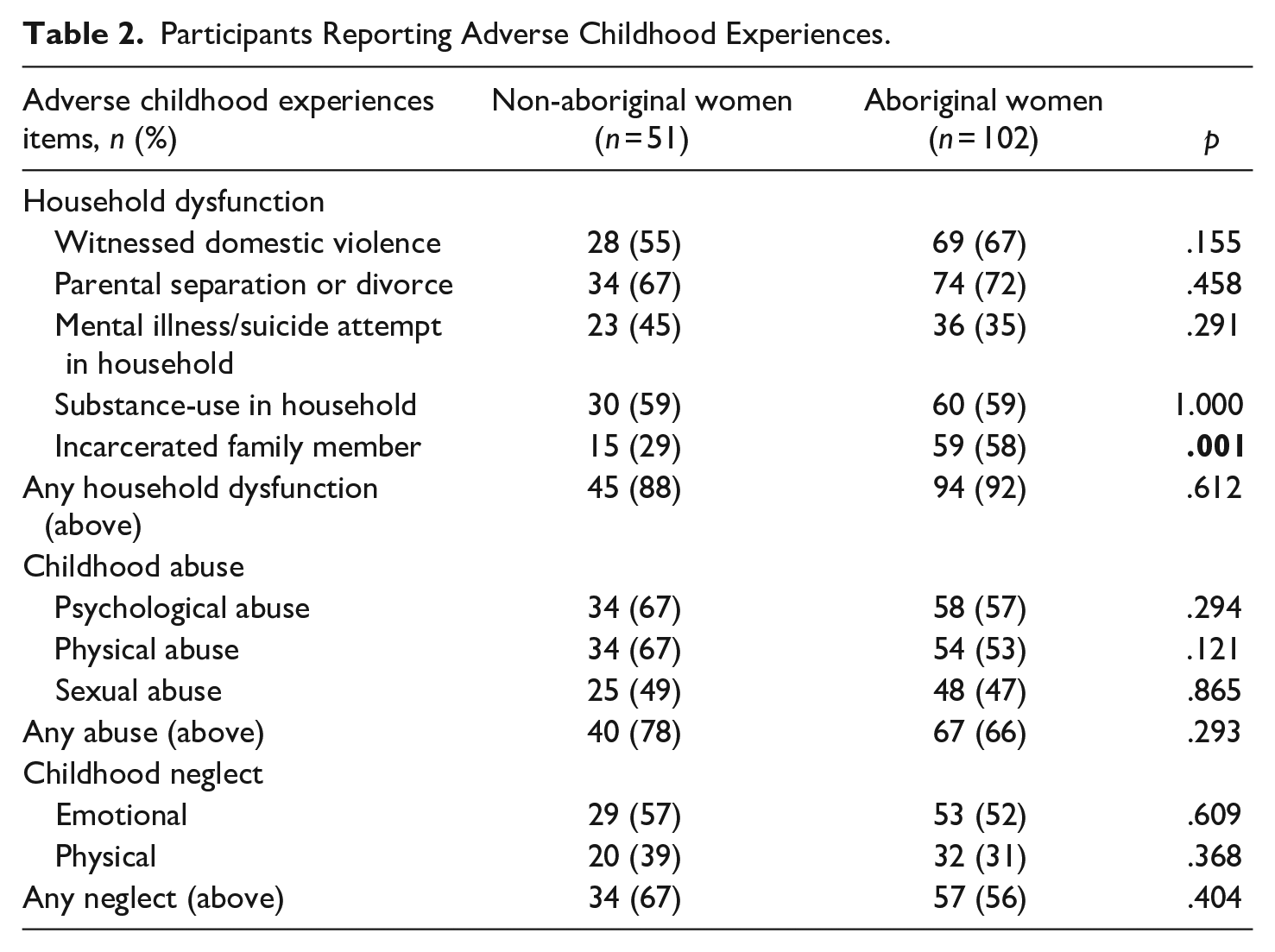
A total of 153 women completed the Adverse Childhood Experience questionnaire of whom 102 (67%) identified as Aboriginal (Table 2). Household dysfunction due to parental separation or divorce was the most common ACE reported (n = 108), followed by witnessing family or domestic violence (n = 97). Overall, 94% (n = 144) reported to have experienced at least one childhood adversity, with a median of 6 ACEs reported (IQR 3–8). Aboriginal women were more likely to have a family member being incarcerated during childhood compared with non-Aboriginal women (58% [95% CI 47, 67] vs. 29% [CI 14, 43]; p = .001). Any form of neglect was experienced by 59% (n = 91) of women. Close to half of the women (n = 73) reported sexual abuse as a child.
Participants Reporting Adverse Childhood Experiences.
Exposure to Violence
Of the 159 women screened for intimate partner violence (Table 3), 66% (n = 105) identified as Aboriginal. Overall, 94% of all women reported experiencing physical violence perpetrated against them by their current or former intimate partners. Eighty-seven percent of all women reported threats of harm, including threats to kill them. A significant number of women (n = 108) indicated that they had experienced choking, strangulation, or suffocation by a current and or former intimate partner (NFS events are not mutually exclusive however screening specifically for NFS was introduced later into the program). In the context of intimate partner violence, 77% of women reported that they fought back in response to violence.
Violence and Injury Characteristics of Participants.
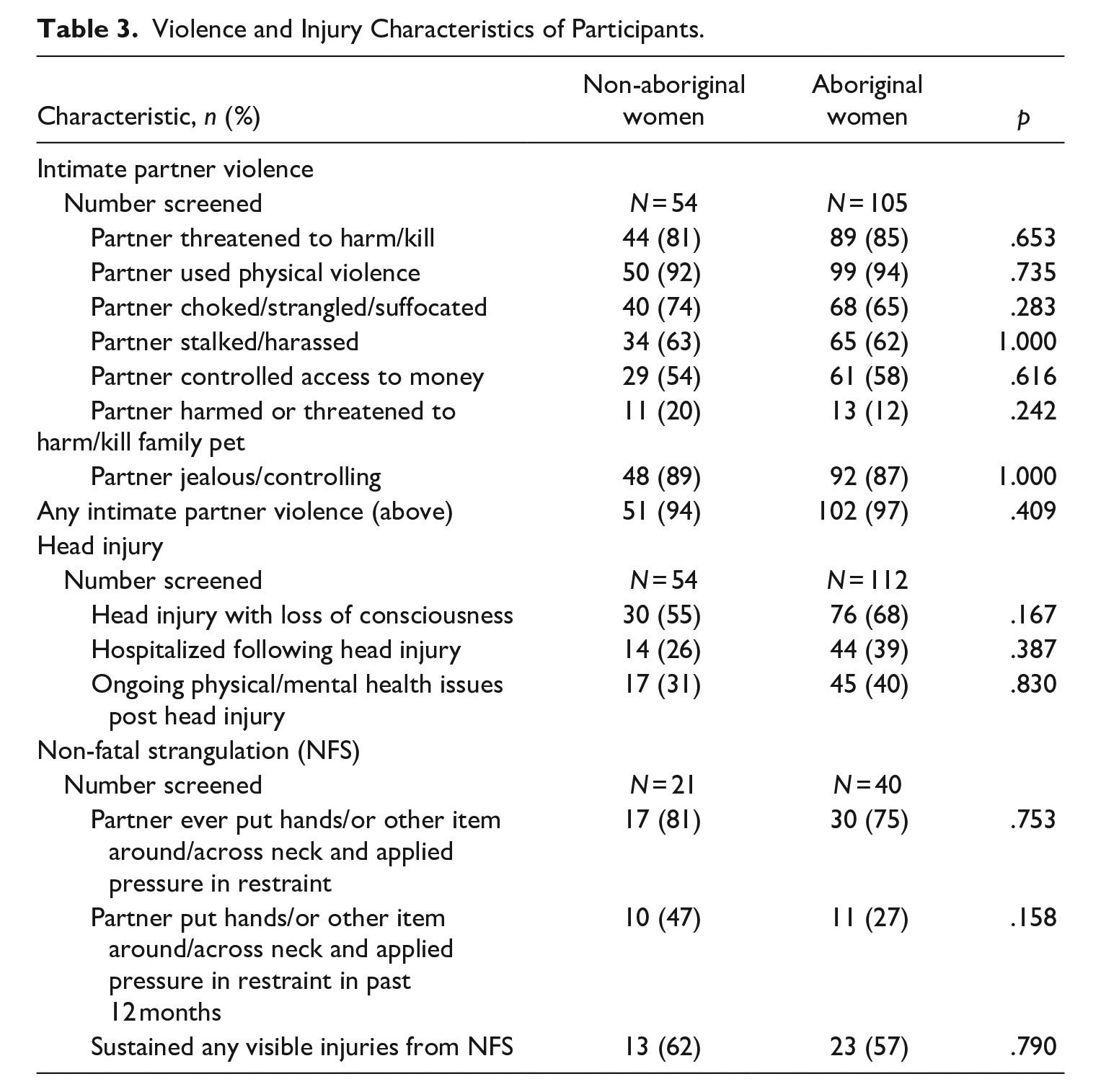
Of the 166 women screened for a head injury, 106 (64%) reported sustaining a head injury with a loss of consciousness. For 49 women the head injury and subsequent loss of consciousness was due to intimate partner and or family and domestic violence. Of the 106 women who reported loss of consciousness 46% (n = 49) reported that this has occurred several times. Overall, 58% of women (n = 62) reported ongoing health impacts following head injury including: mental health issues (31%) (including depression and PTSD), headache or migraine (26%), loss of sensory processing including loss of vision and balance (17%), and continuous pain (11%). In screening for non-fatal strangulation (NFS) 77% of women (n = 47/61) disclosed that their current or former partner had applied pressure in restraint around/across their neck, with 59% reporting sustained visible injuries.
Characteristics of Participants and the Experiences of Adversity in Childhood
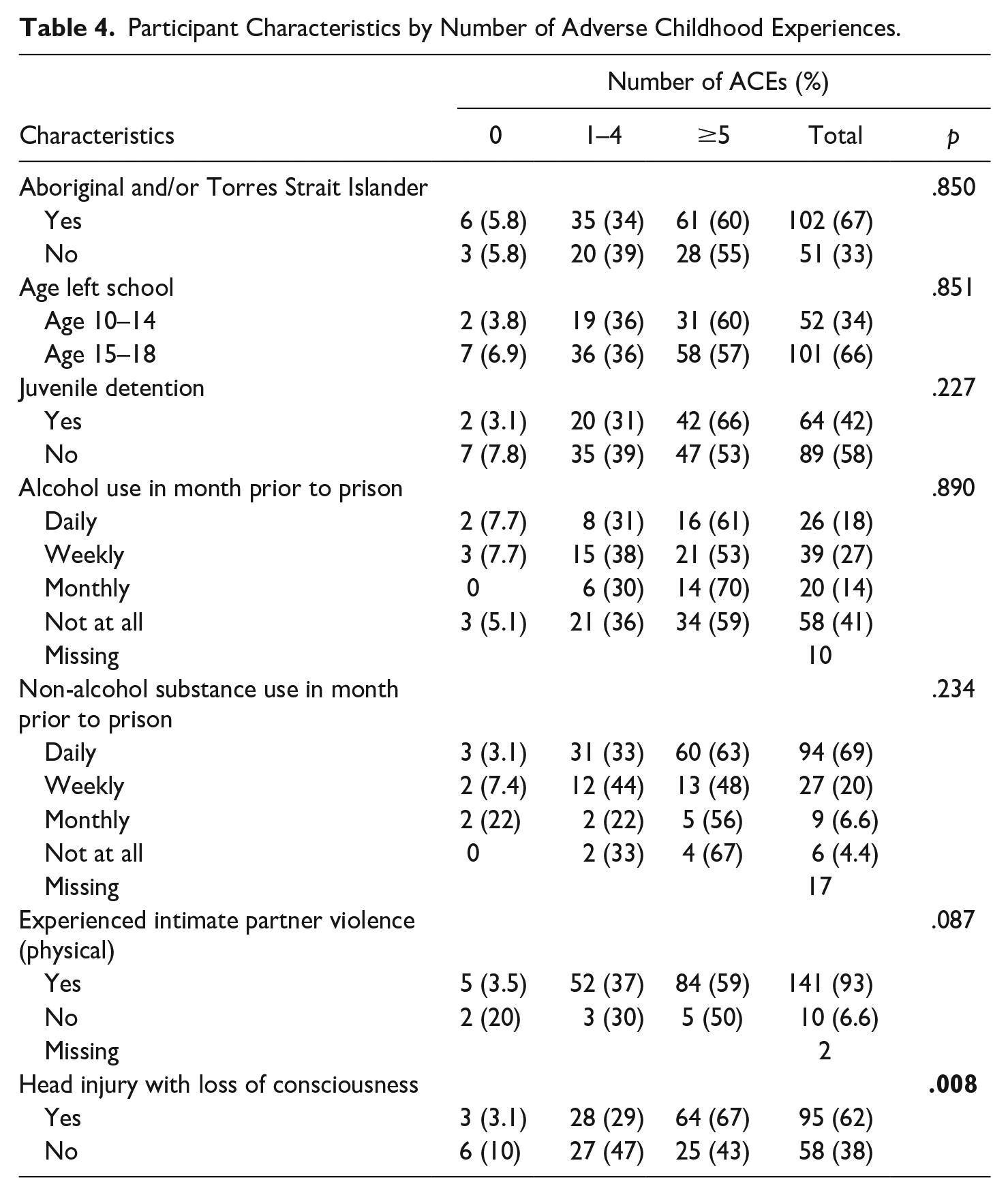
Though non-alcohol substance use (daily, weekly, monthly) and the experience of intimate partner violence (physical) were salient among this population irrespective of the level of adversity experienced during childhood, the differences were not statistically significant (Table 4). Women who had head injury with loss of conciseness were more likely to report >5 ACEs than those with no head injury with loss of consciousness (67% [95% CI 57, 76] vs. (43% [CI 30, 56], p = .008). There were no significant differences in cultural status, years of education, juvenile detention, alcohol, and non-alcohol substance use, who reported more than five ACEs and those who reported less.
Participant Characteristics by Number of Adverse Childhood Experiences.
Discussion
These findings present a harrowing picture of ubiquitous exposure to adverse childhood experiences, and violence into adulthood in a sample of adult female prisoners, underscoring the need for trauma informed approaches addressing the gendered criminogenic needs of this growing population. This study highlights that whilst this population have been convicted of violent offenses, almost all are victims themselves. It expands upon the limited research assessing the experiences of Australian women who use violence in areas of childhood adversity, substance use, and family and intimate partner violence, including victimization resulting in head injury (Jones et al., 2018, 2020; Messina & Calhoun, 2021). Indeed, only 9 women out of 153 women reported no ACEs, reinforcing the traumatic background from which many of these women come from.
Despite representing greater than half of the baseline cohort, Aboriginal women were only found to be more likely to report that as a child a family member was incarcerated, compared with non-Aboriginal women. This finding is consistent with Brewer-Smyth et al.’s (2016) results, where both Hispanic and African American female prisoners showed disproportionately increased rates of incarcerated adult family members during childhood, than their Caucasian counterparts. There were no differences between Aboriginal and non-Aboriginal women when examining different exposures to intimate partner violence. This finding although not statistically significant, is consistent with a paper release by Australia’s National Research Organisation for Women’s Safety (2020), which reported between 70% and 90% of women in Australian prisons have experienced intimate partner violence. Wilson et al. (2017), however, note that Aboriginal women were 35% more likely to be hospitalized for intimate partner violence related assaults, than non-Aboriginal women. In the context of Australia’s short history of colonization, Aboriginal and or Torres Strait Islander women continue to live with systemic disadvantage, cultural marginalization, and dislocation, including the forced removal of their children, or their own experience of removal as a child (Atkinson et al., 2014). The cyclic cost of colonization for Aboriginal women may be expressed behaviorally as unresolved intergenerational and childhood trauma, resulting in normalized expressions of violence and subsequent incarceration (Atkinson et al., 2014). This is linked to continued intergenerational suffering, the breakdown of family functioning and community, resulting in poor physical and mental wellbeing as well as the complex experience of violence as both victim and perpetrator (Atkinson et al., 2014; Australian Institute of Health and Welfare, 2020; Friestad et al., 2014; Sullivan et al., 2019). Atkinson et al. (2014) describe this victim-participant relationships further as a normalization of violence experienced intergenerationally and accumulatively as a child, remaining unresolved and sustained into adulthood; trauma symptomology indistinguishable from causation and effect (Atkinson et al., 2014). It is the resistance, the contestation and resilience which Aboriginal women participate that moves the narrative beyond the focus of entrenched victimization, to consider the numerous intersecting causes of violence which have resulted in their growing rates of incarceration experienced by this group (Atkinson et al., 2014; Australian Institute of Health and Welfare, 2020; Blagg et al., 2020; Friestad et al., 2014; Sullivan et al., 2019). It is possible to consider the lack of statistical significance relating to cultural status (Aboriginal versus non-Aboriginal) in terms of the accumulation of ACEs. This possibly reflects the extreme disadvantage that all women in prison endure, as well as an overall level of disadvantage among this population.
All participants had a history of violent offending, with most witnessing violence in the home as a child, and over half (57%) having been victim to physical abuse during childhood. Victimization throughout childhood and subsequent use of violence as an adult has been described as the intergenerational transfer of violence occurring by way of imitation and/or tolerance of similar behaviors and experiences into adulthood (Mair et al., 2012). Regardless of the level of adversity experienced during childhood, a significant proportion (93%) of participants reported to have experienced intimate partner violence, supporting previous research findings (Jones et al., 2018; Messina & Calhoun, 2021). High rates of head injury resulting in a loss of consciousness as a direct result of intimate partner violence were reported in the sample with almost half reporting ongoing mental health issues as a consequence of the head injury. This is consistent with research indicating that head injury with loss of consciousness is found more commonly among violent female prisoner populations than those who are incarcerated for non-violent crimes (Brewer-Smyth et al., 2004, 2016). Importantly, this finding also supports the literature that the accumulation of adversity in childhood is considered to increase the risk for continued victimization into adulthood, resulting in an increased risk of sustaining a brain injury (Brewer-Smyth et al., 2016; Ma et al., 2019; Schofield et al., 2006). Numerous factors confer risk for traumatic brain injury beyond intimate partner violence such as substance use and physical assault (non-family or intimate partner violence), both of which are substantially over-represented in prisoner populations and may be a risk-factor for criminal behaviors, impulsiveness, and violence (Australian Institute of Health and Welfare, 2020; Brewer-Smyth et al., 2004, 2016; Schofield et al., 2006). Screening for head injury on entry into the justice system may provide the opportunity to divert woman away from incarceration, and into treatment programs to address the needs of those affected by head injury (Schofield et al., 2006).
Early childhood exposure to parental/carers who misuse substances represents negative parental modeling of coping skills and adaptive functioning and is a robust predictor for substance misuse in adulthood (Marotta, 2017). Many participants reported that they witnessed substance use in the household as a child (59%), yet there was no difference of significance between those who reported both alcohol and non-alcohol substance use and the accumulation of five or more ACEs. Previous research by Kubiak et al. (2017), found no direct effect of substance use on the perpetration of violence, rather the misuse of substances was considered an attempt to suppress or avoid difficult emotions relating to ACEs, leading to a greater difficulty in managing emotions such as anger, suggesting that these factors have an indirect effect on offending, yet are interconnected. The extent of trauma exposure during childhood development appears to correlate negatively with the effectiveness of interventions for substance use among women (Marotta, 2017).
These findings highlight the need for female specific programs, in addressing the complexities of ACEs, cyclic victimization including head injury and the relevance to the causality of the perpetration of violence. Importantly, the unique needs of female offenders may be currently overlooked in existing programs generalized from men.
Limitations
Limitations of the study include the reliance on self-report by the women who have suffered numerous head injuries. The lack of access to medical records to verify participant medical history, mental health diagnoses or history of victimization has relied further on self-reporting. However, a previous study by Schofield et al. (2011) found adult male prisoners to be very reliable in terms of reporting head injury. The instruments we used may have failed to ascertain both the level of adverse events during childhood due to underreporting, but some life events that might confer additional risk for substance misuse, and violence in adulthood. For example, the death of a parent or family member, economic deprivation, peer victimization, and violence in the community during childhood, have been considered to contribute to adverse consequences later in life (Jones et al., 2020; McLennan et al., 2020). In addition to establishing an ACE norm among females who perpetrate violence, further research to explore the interrelatedness of ACEs and their possible associations with specific types of crime including non-violent crimes would be valuable and lead to a greater understanding of not only female victimization, but the possible differentiation of female violence as a result of “fighting back” as previously described in the context of intimate partner violence, the role of extensive victimization, along with undiagnosed head injury. Furthermore, a recent publication on women in Australian prisons by the Australian Institute of Health and Welfare (2020), suggested that the increase in the female prisoner population for violent offenses may be attributed to an increase in the seriousness of offenses committed, which are more likely to attract a custodial sentence, or there may be a more severe response to minor offenses which would have otherwise seen community base sentences imposed.
Conclusion
The findings of this study are consistent with the limited research and literature that has identified ACEs as a possible risk factor for female violence, substance misuse, head injury and family and or intimate partner violence in adulthood. The focus of the intervention program on ACEs and the related efforts to assist female offenders with an opportunity to address and resolve the repercussions of these negative experiences on entry into the system, may well pay dividends in terms of the prevention of incarceration and reduction in reoffending in the future. We hope that with the conclusion of the intervention study from which these baseline data were drawn, we may have robust evidence to support such an anticipated outcome.
Footnotes
Acknowledgements
I would like to express my gratitude to my supervisors, Professor Tony Butler, Professor Peter W. Schofield, and Dr Mandy Wilson for their invaluable constructive guidance during the development of this work. I am particularly thankful for the generous time of Dr Jocelyn Jones in their proof reading, and of Dr Azar Kariminia, who provided me with valuable advice. We acknowledge the assistance of the WA Department of Corrective Services. Errors of omission or commission are the responsibility of the researchers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Health and Medical Research Council (NHMRC). Aboriginal and non-Aboriginal women perpetrators of violence: a trial of a prison-based intervention (Beyond Violence) Grant number: 1108115.
Data Availability
The authors do not have permission to share data.