
Abstract
Individuals with mental illness are significantly overrepresented in the Canadian justice system. Given the high rate of mental illness among individuals who are incarcerated, correctional facilities must implement accessible and effective mental health resources. This not only improves their health and well-being but also contributes to their rehabilitation efforts. However, evidence suggests that the care provided in prisons is inadequate. This scoping review asks, “What is known about the access and quality of mental health care services for adults who are incarcerated in Ontario?” Mental health care services included non-acute interventions and care that is provided in the institution. This scoping review followed the PRISMA Extension for Scoping Reviews methodology. Databases searched include MedLINE, EMBASE, CINAHL, PsycINFO, Criminal Justice Abstracts, JSTOR, Google Scholar, and the grey literature. The search yielded 354 titles and abstracts of which 16 met the inclusion criteria. Conducted from 2010-2022, the 16 studies included qualitative, quantitative, and mixed methods. Common themes that were identified related to segregation, mental health assessments, medication prescribing and access, opioid agonist therapy, psychiatric service access, systemic and institutional barriers, mental health perception, and the need for collaboration. Despite the significant demand for mental health care in Ontario correctional facilities, limitations to quality care are evident. Such limitations intersect and are then exacerbated, resulting in poor mental health care provision among the incarcerated population. More research is warranted regarding the access, quality, and efficiency of mental health care in Ontario prisons, and how factors including ethnicity, gender, and prison classification (provincial vs. federal) may influence mental health care and its outcomes.
Keywords
Introduction
The burden of mental health challenges among individuals incarcerated in Canada is disproportionately higher compared to the general population (Henning, 2021; Webster, 2019; Cameron et al., 2020; Kouyoumdijian et al., 2016). In fact, mental health issues are 2-3 times more prevalent in Canadian correctional institutions as compared to the general population (John Howard Society, 2020). Approximately 41% of individuals incarcerated in Ontario are estimated to experience at least one severe mental health issue during their incarceration (John Howard Society, 2020). The mental health conditions that are most observed within the prison population include depression, anxiety, substance use, and psychotic disorders (Gómez-Figueroa & Camino-Proaño, 2022).
Given the increased prevalence of mental health concerns in the incarcerated population, correctional facilities need to establish effective and accessible mental health resources to address the needs of their population. However, the current model of healthcare governance in Ontario prisons presents barriers to the accessibility and quality of care that is provided to the incarcerated population (John Howard Society of Ontario, 2016). The current model raises concern about the level of control held by the Correctional Service of Canada & Ministry of Justice in determining the nature & delivery of healthcare, as well as the providers contracted for healthcare delivery. The governance of healthcare differs based on the classification of the prison as federal or provincial. Provincial and territorial custody is for individuals with sentences of less than two years, while those in federal custody are serving sentences over two years (Lee, Ross, & Saad, 2021). Healthcare provision in federal prisons is managed by the Correctional Service of Canada, which is the ministry responsible for corrections and is separate from the healthcare system that serves the general population (McLeod & Martin, 2018). In Ontario, healthcare in provincial prisons is managed by the respective Ministry of Justice (Lee, Ross, & Saad, 2021).
Since healthcare providers are under the obligation of the Correctional Service of Canada or the Ministry of Justice, as their employees, the challenge of dual loyalty arises. This concept refers to the conflict between obligations to a patient and obligations to a third party (Lee, Ross, & Saad, 2021). Healthcare providers working in correctional settings are expected to fulfill their duties to patients in alignment with the expectations set by the College of Physicians and Surgeons of Ontario and other regulatory bodies for health (The College of Physicians & Surgeons of Ontario, 2023), while also being expected to comply with the policies and regulations of the correctional system. This can create barriers to building trust with patients in the correctional setting. Building therapeutic relationships becomes difficult and as a result, the overall quality of care is adversely affected (Lee, Ross, & Saad, 2021).
Other challenges to providing mental health care in correctional institutions have been previously reported in the literature. These challenges encompass various aspects including staff relationships (McLeod & Martin, 2018), movement restrictions (Cameron et al., 2020), and limited access to mental health professionals (Lee, Ross, & Saad, 2021; MacKenzie & Amirault, 2021; McLeod & Martin, 2018). The highest vacancy rates of correctional healthcare providers were in Ontario, with 29% of psychologist positions empty (John Howard Society of Ontario, 2016). Further, there is a lack of health resources and institutional support required for program delivery (Kouyoumdjian et al, 2018) as well as security-related concerns (i.e lockdowns, institutional searches, or physical altercations) that can hinder the accessibility and quality of mental health care in correctional institutions (Ghelani, 2020). Another challenge noted within these settings is the limited clinical independence of healthcare providers, which describes a lack of autonomy in healthcare decision-making (Lee, Ross, & Saad, 2021; Cameron et al., 2020). For individuals held in custody, unique barriers are presented due to the transient nature of the population and limited time spent in these settings. These include barriers to performing an adequate and timely assessment of health needs, initiation of treatment, and ensuring continuity of healthcare (Murphy, 2020). These issues compound, leading to a lack of mental healthcare access for the incarcerated population.
Despite high rates of mental illness among the incarcerated population, limited research has been conducted on the accessibility and quality of mental health services in prisons. This scoping review addresses the question “What is known about the access and quality of mental health care services for adults who are incarcerated in Ontario?” Guiding questions for this review included: i) How accessible are healthcare services? ii) What are the factors that affect mental health care access? iii) What is the quality of healthcare services and what influences this? and iv) Are there differences in mental health service access based on the classification of the prison as provincial vs. federal?
The scoping review focused on Ontario, the most populated province in Canada (Statistics Canada, 2023), with a larger incarcerated population than other provinces (Statistics Canada, 2023). The significant population size may present unique challenges to providing healthcare in correctional facilities. Also, as previously stated, Ontario still manages correctional healthcare through the Correctional Service of Canada or the Ministry of Community Safety and Correctional Services for federal and provincial prisons, respectively, rather than the Ministry of Health and Long-term Care, which oversees health for most of the province (Sapers et al., 2017). This differs from other Canadian provinces including B.C., Alberta, and Nova Scotia, where correctional healthcare has been transferred from correctional organizations to their respective ministries of health (Lee, Ross, & Saad, 2021). This setup presents an opportunity to study the current healthcare structure in Ontario prisons and its efficiency in terms of ensuring access and quality healthcare. The insights from this study can then inform future research efforts and policy reform.
Methods
This scoping review followed the PRISMA Extension for Scoping Reviews methodology (Tricco et al., 2018). A protocol does not exist for this review.
Inclusion and Exclusion Criteria
This review included studies with adult participants (18+) incarcerated in Ontario provincial and/or federal correctional facilities. Studies that discussed mental health care services taking place outside of correctional facilities were excluded. Examples of such services include acute mental health services, such as emergency psychiatric care and hospitalization. Studies evaluating interventions that did not address mental health conditions, such as sex offender and batterer programs, were not considered for this review. Multi-site studies that did not distinguish results from Ontario correctional facilities or did not specify location were also excluded.
Search strategy
The PICOS scheme is a model used to frame and answer a clinical or healthcare-related question. PICOS stands for Patient/Population, Intervention, Comparison, Outcomes, and Study Design (O’Connor et al., 2008). Keywords related to the research question and their index terms were identified using elements of the PICOS scheme, focusing on the Population and Intervention components. Keywords included: convict, criminal, prisoner, inmate, offender, mental health service, mental health care, psychiatric service, cognitive behavioral therapy, therapy, psychotherapy, pharmacological treatment, Ontario, and other synonymous terms. A complete list of the terms used is recorded in the search strategies included in the appendix.
The search strategy was used to find published and unpublished studies in English from January 2010 to December 2022. This period was selected to obtain recent data reflecting the current state of mental health service access and quality in Ontario prisons. Relevant articles were identified from searches of electronic bibliographic databases including MedLINE (OVID), Embase (EMTREE), PsycINFO, CINAHL, Criminal Justice Abstracts, and JSTOR. The search for unpublished studies included an Internet search of reports published by Correctional Service Canada (CSC), the Office of the Correctional Investigator of Canada, Ontario Human Rights Commission, John Howard Society of Ontario, Council of Elizabeth Fry Societies of Ontario, institution-specific reports and Google Scholar (first 20 pages of results). Reference lists of eligible literature were also examined. Quality assessment of the studies was not performed.
Study selection
After the search, citations were combined and imported into Covidence where duplicates were removed (Covidence systematic review software, 2020). The first selection was from title and abstract screening and the second selection was from full-text screening. The search strategy retrieved 374 hits, and the removal of 75 duplicates resulted in 299 records for title and abstract review. Of the 299 records screened, 232 were excluded following the inclusion and exclusion criteria. Sixty-seven articles were included for full-text review, of which 16 met the inclusion criteria (Figure 1). Please view the PRISMA diagram for reasons for the exclusion of 51 articles.
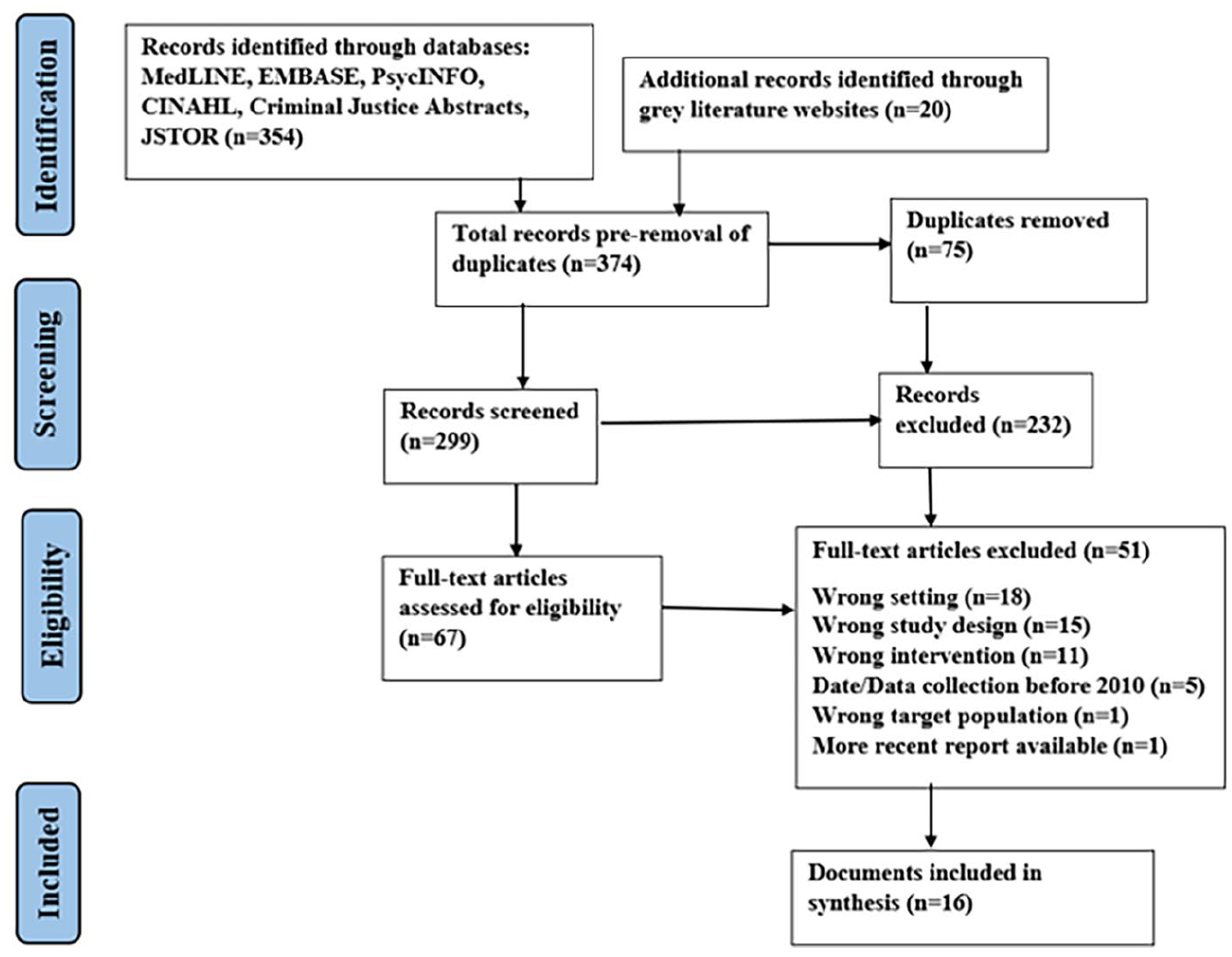
PRISMA flow diagram.
Data Extraction
Data were extracted using the Covidence software for published studies and a Microsoft Word document for unpublished texts. The items extracted from the full texts included general information (study ID, title, setting, methods, the aim of the study, study design, start and end date, funding sources, conflicts of interest, participant information, inclusion/exclusion criteria), population characteristics (age, sex, race, gender, etc.), intervention information (duration, timing, delivery, providers, etc.), outcomes, study applicability (exclusion of important populations, relevance to the research question), and additional notes. Key findings relevant to the general and guiding questions of the review were then determined.
Results
Study characteristics
The sixteen studies included were published between 2016 and 2022. The settings included six studies in provincial prisons (Murphy & Sapers, 2020; Bodkin et al., 2021; Ghelani, 2020; Hunter, 2020; Kouyoumdijan et al., 2018; Marmel & Bozinoff, 2020); one study in a women’s federal prison (Fayter & Payne, 2017), four studies in federal penitentiaries that included both incarcerated males and females (Iftene, 2019; Johnson et al., 2020; Martin et al., 2018; Russell et al., 2022); and three studies that included both federal and provincial correctional facilities in Ontario (CAMH, 2020; John Howard Society of Ontario, 2016; Sapers et al., 2017). Two papers broadly evaluated practices in Canadian correctional facilities and relevant data that specified Ontario were extracted (Correctional Service Canada, 2017; Zinger, 2020).
Study designs included four qualitative studies (Bodkin et al., 2021; Fayter & Payne, 2017; Kouyoumdijan et al., 2018; Marmel & Bozinoff, 2020), one mixed methods (Russell et al., 2022), and two quantitative (Johnson et al., 2020; Martin et al., 2018). One narrative review (Murphy & Sapers, 2020), one letter to the editor (Ghelani, 2020), one dissertation (Hunter, 2020), one book chapter (Iftene, 2019), and five reports from organizations were also included (Zinger, 2020; CAMH, 2020; Correctional Service Canada, 2017; John Howard Society of Ontario, 2016).
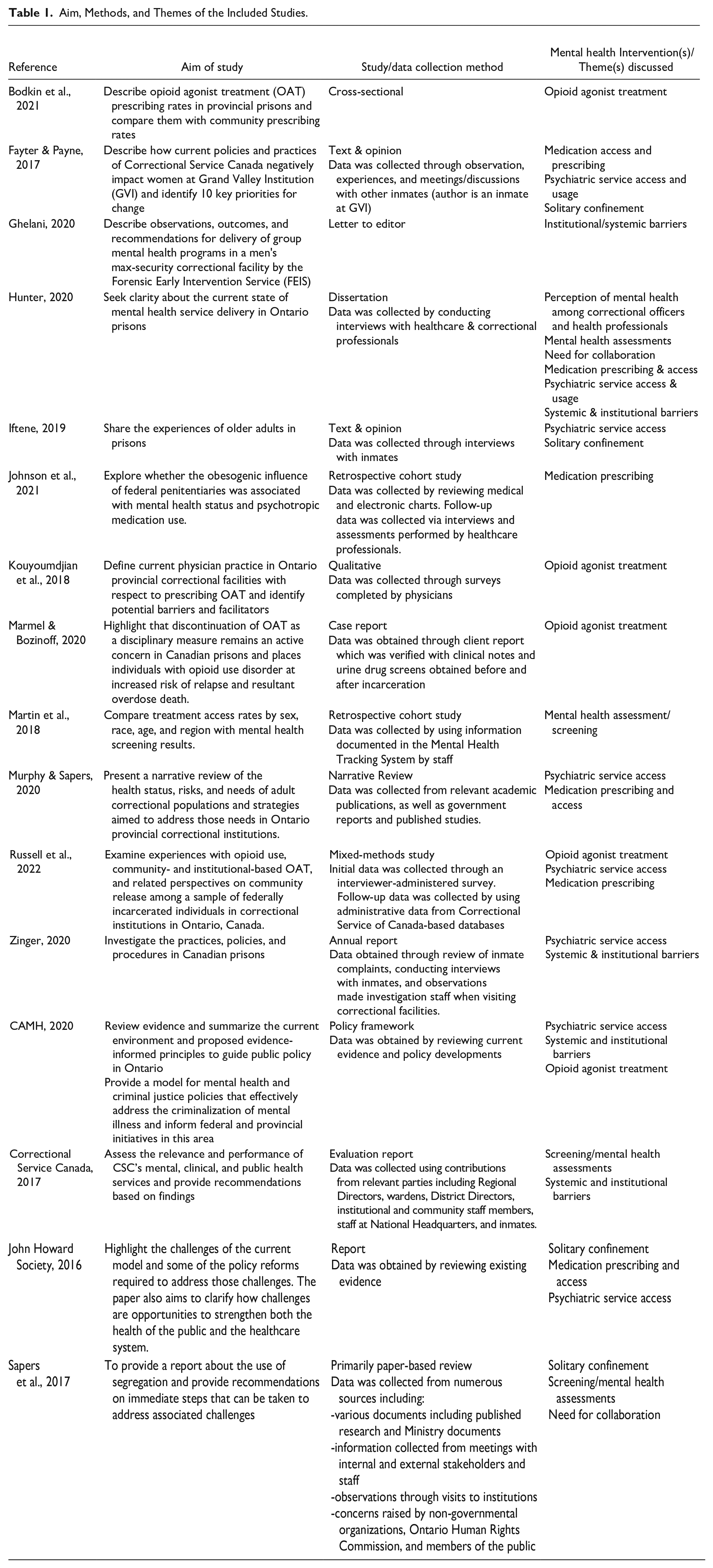
The studies varied in aim and intervention type, or theme discussed (Table 1). Key themes identified included segregation, screening/mental health assessments, medication prescribing and access, opioid agonist therapy, psychiatric service access and usage, systemic/institutional barriers, insufficient clarity regarding mental health perception, and the need for collaboration. The key subthemes found for each major theme are highlighted in Figure 2.
Aim, Methods, and Themes of the Included Studies.
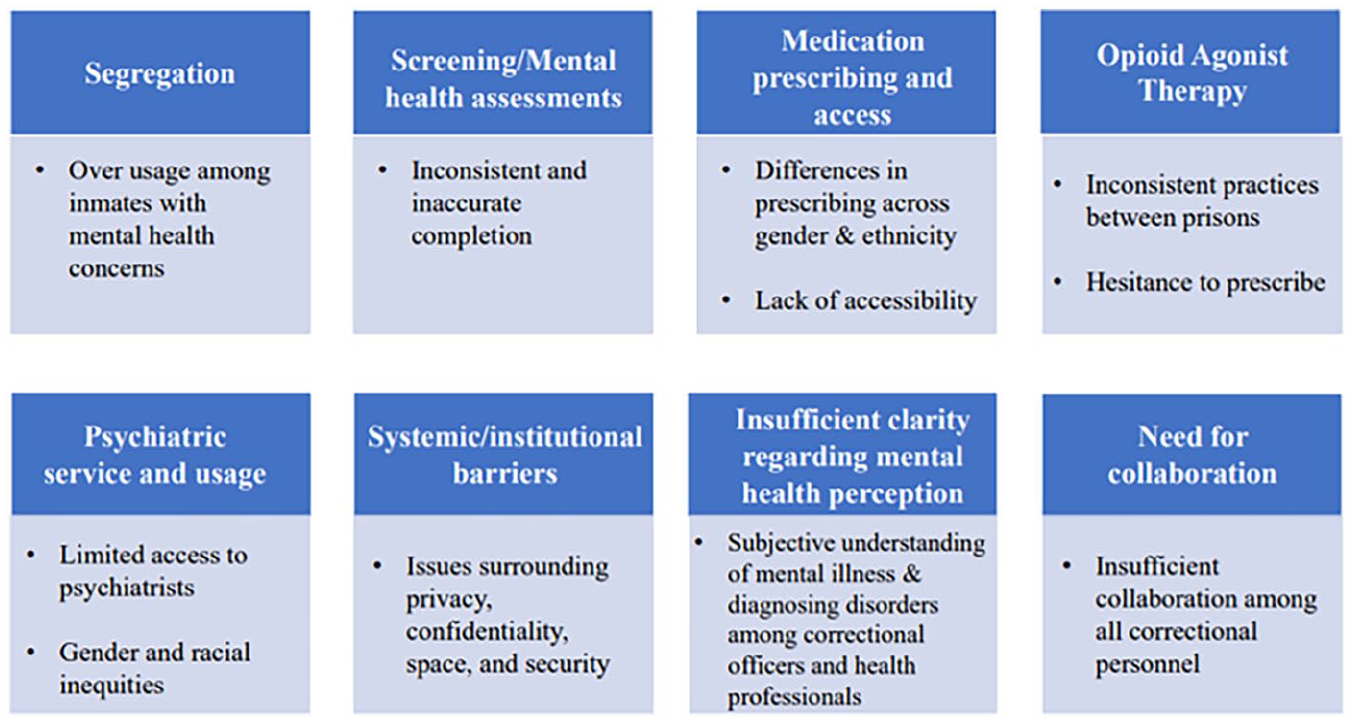
Themes and subthemes identified in relation to mental health care provision in Ontario prisons.
Segregation
The use of segregation as a mental health management tool was a common theme in the literature. Segregation refers to an individual’s confinement to a cell in isolation for 22 hours or more a day, often for prolonged periods (John Howard Society of Ontario, 2017). The practice of segregation inflicts mental health harm (Webster, 2019), and concerns have been voiced regarding the overuse of segregation among individuals with mental health issues (Ontario Human Rights Commission, 2019; John Howard Society of Ontario, 2017; Sapers et al., 2017; Iftene, 2019). No race- or gender-based differences regarding the use of segregation were reported in the studies.
Insufficient institutional resources may contribute to using segregation for mental illness management (Sapers et al., 2017). This was the case at the Toronto South Detention Centre, whereby insufficient healthcare staff resulted in the closure of medical units, and patients needing care were managed by placing them in segregation (John Howard Society of Ontario, 2016). Communication gaps and a lack of mutual understanding between correctional staff and external health providers also contribute to the segregation of individuals suffering from mental illness (Sapers et al., 2017).
The use of segregation affects the quality of mental health care provided in correctional facilities, such that fear of being placed in segregation can deter individuals from seeking mental health care or being honest during mental health assessments, which will impact the amount and type of care they receive (Hunter, 2020). Expressions of intent to self-harm or suicidal ideation are precursors to being sent to segregation (Fayter & Payne, 2017; Iftene, 2019; Hunter, 2020). Placement of individuals with mental health concerns in segregation can not only further exacerbate their mental health issues, but also limit their ability to access mental health care during their time in segregation. In some institutions, the baseline physician assessments and 5-day check-ups that are required to be provided to individuals with mental health needs in segregation are not being performed, and primary care physicians and psychiatrists do not visit individuals in segregation unless a specific medical issue arises (Sapers et al., 2017). This may be due to systemic barriers including insufficient space and security measures that limit access to inmates in this setting (Metzner, 2015), as well as a lack of current resources, with one healthcare manager noting that insufficient resources made the health assessment requirements unachievable (Sapers et al., 2017).
In November 2019, the use of administrative and disciplinary segregation in federal correctional institutions was eliminated, and Structured Intervention Units (SIUs) were established to facilitate rehabilitation (Corrections and Conditional Release Act, 2019). Inmates in an SIU are provided with an opportunity to engage in interventions to help them get out of segregation and can spend a minimum of four hours a day outside their cell, with two hours of meaningful human contact (Correctional Service Canada, 2022). However, SIUs may not be operating in a manner consistent with expectations. There have been reports that inmates are staying in SIUs for long periods, not getting their promised time out of their cells or for meaningful human contact and that there are regional/institutional variations in practices (Sprott & Doob, 2021). Thus, additional research on SIU practices and their impact on mental health is needed.
Screening/Mental health assessments
Mental health assessments are the primary method by which the prison assesses mental health, and they also influence where inmates are housed at intake (Hunter, 2020). The Corrections and Conditional Release Act mandates in-person mental health assessments to be performed as soon as practicable and within 30 days of admission to Correctional Service Canada (CSC) (Cameron et al., 2020). For offenders placed in the Structured Intervention Unit (SIU), a referral for a mental health assessment should be provided within 24 hours of admission, and the assessment performed within 28 days (Cameron et al., 2020). These mandates are insufficiently performed or not performed at all. There is no consistent review of mental health status and post-intake assessments occur only after a visit to a general practitioner or after a correctional officer observed behavioral concerns (Hunter, 2020).
Sapers and colleagues (2017) found that mental health screening is often delayed and there is significant variation in the timelines for completing screening. For inmates admitted in June 2016, the average time to complete the Brief Jail Mental Health Screen (BJMHS) was 1 day, with average monthly completion times ranging from 24 hours to 2.5 days. Overall, the majority (96%) of the institutions completed preliminary screening within the two-day timeline. However, administration of the Jail Screening Assessment Tool (JSAT) was much more delayed; for individuals admitted in June 2016 and identified as needing a JSAT, an average of 11 days passed between the two assessment stages (Sapers et al., 2017). The completion of the BJMHS and JSAT is required for a referral to a psychiatrist, thus delays and inconsistencies in screening completion are concerning as individuals with significant mental health needs may have had to wait over a month to receive medical attention (Sapers et al., 2017).
Staff shortages compromise the accuracy of mental health assessments, as it leads to correctional officers completing assessments rather than qualified mental health nurses (Hunter, 2020). Correctional officers lack sufficient knowledge to ensure the accuracy of their assessments as they do not receive feedback or relevant information due to privacy concerns regarding sharing health information (Hunter, 2020). They rely on subjective assessment of the situation and individual when assessing mental health status, such as appearance and basic hygiene, the individual’s paperwork, or prior experience with the person (Hunter, 2020). Accurate and comprehensive mental health assessments are critical to identify mental health concerns and inmate needs (MacKenzie & Amirault, 2021). Subjective or incompletion of assessments may result in missed cases of mental health needs. This oversight impacts inmates’ access to mental health care as those who have not screened positive for possible mental health concerns are not referred to a psychiatrist and are not often reassessed for mental health issues at regular intervals (Government of Ontario, 2022).
Martin and colleagues (2018) reported disparities in screening among subpopulations, reporting that nonwhite inmates were more likely to not complete screening due to inmate refusal and/or not attending the screening.
Medication prescribing and access
Differences in prescription medication provision and usage were noted across gender and ethnicity. Female inmates take more psychotropic medications than their male counterparts in terms of frequency and number (Fayter & Payne, 2017; Johnson et al., 2021). Johnson and colleagues (2021) also note that psychotropic medication use was increased among Caucasian and Aboriginal groups compared to other ethnic groups.
Difficulty with accessing medications promptly is a challenge. If the community pharmacy is closed, medication may not be provided for up to 92 hours, which is concerning given the importance of medications such as antipsychotics (Hunter, 2020). Inmates may also be unable to access their prescribed medication for a prolonged period while waiting for a physician’s assessment, which can exacerbate or destabilize symptoms (Murphy & Sapers, 2020; John Howard Society of Ontario, 2016).
Opioid agonist therapy (OAT)
Opioid agonist therapy is a treatment for opioid use disorder and works to manage withdrawal symptoms and reduce cravings for opioids. OAT can be used to increase stability and daily functioning and reduce harm related to drug use (Centre for Addiction and Mental Health, 2016). Several of the included studies identified limitations of OAT provision in correctional facilities (Bodkin et al., 2021; Russell et al., 2022; Kouyoumdijian et al., 2018; Murphy & Sapers, 2020; Marmel & Bozinoff, 2020).
One concern was the inconsistency in OAT practice. Bodkin et al. (2021) found a statistically significant difference in prescribing prevalence between prisons. Participants reported that OAT processes were inconsistent, non-standardized, and seemed to be based on individual institutional policies and medical staff preferences/abilities (Russell et al., 2022). Physicians’ specifications on allowable dosages and periods for increasing or decreasing medications differed across institutions. Physicians in the institutions would not match OAT doses participants received in the community, and many participants reported that the dose they received was insufficient to address their cravings, pain, and withdrawal symptoms (Russell et al., 2022). Russell and colleagues (2022) also noted a difference between institutions and individual OAT physician practices relating to the process of switching OAT formulations. Most physicians required individuals to undergo a 3-day detoxification period from methadone before they could induce buprenorphine-naloxone, while other physicians allowed individuals to slowly wean off methadone through micro-dosing while gradually being introduced to small doses of buprenorphine-naloxone (Russell et al., 2022). The former process is undesirable as it would result in withdrawal symptoms. Institutional discrepancies in OAT administration were also found (Russell et al., 2022). Some institutions administered OAT one-on-one with patients where they would go to the healthcare unit or delivery would occur at the individual’s cell/range, while other institutions used a mass-dosing process where all individuals on OAT would receive it in a common room. Based on the findings of Russell and colleagues (2022), timely access of mental health/addiction treatment as well as the quality of treatment- such as providing doses to address inmates’ symptoms, switching formulations in a way that minimizes undesired side effects (i.e. withdrawal) and considering the treatment setting- are influenced by the specific institution and the preferences of the provider responsible for OAT administration.
Furthermore, there were differences in accessibility to OAT upon incarceration, whereby individuals who obtained OAT immediately pre-incarceration described an easy and relatively smooth transition from community- to institutional-based OAT, while those who were not on community-based OAT immediately before incarceration or who experienced treatment disruptions at the provincial correctional point of entry to the criminal justice system experienced significant challenges (Russell et al., 2022). The former group may have still experienced treatment interruptions and adverse side effects, including withdrawal since the presentation of proof of their last dose could take 1 day up to 2 weeks. However, those not on community-based OAT experienced even longer wait times, amounting to multiple months (Russell et al., 2022).
Kouyoumdjian et al. (2018) surveyed physicians providing services in Ontario provincial prisons and identified common reasons for not providing OAT, including lack of exemption from Health Canada, others being responsible for the service; no interest in adding OAT to their clinical work, and having inadequate knowledge about the treatment. Common barriers to OAT provision included concerns about medication diversion, appropriateness of treatment initiation for people not currently using opioids, lack of linkage with community-based OAT providers at the time of release, and concerns about adherence to OAT on release (Kouyoumdjian et al., 2018). Other barriers included insufficient nursing and institutional support, lack of resources required for program delivery, insufficient time, insufficient financial compensation, costs to patients on release, and patients who needed treatment were not brought to the physician’s attention (Kouyoumdjian et al., 2018). Russell et al. (2022) also noted barriers related to institutional policies that involved delaying treatment initiation until individuals were transferred to their main institution and maximum patient capacity. The identified barriers to OAT access in Ontario correctional facilities hinder the implementation of an evidence-based treatment for inmates living with addiction (Kouyoumdjian et al., 2018). Addressing these barriers offers potential to improve access and quality of mental health care for this population.
Marmel & Bozinoff (2020) presented a case study of a client who was forced to experience a prolonged period of opioid withdrawal upon incarceration as they waited over 48 hours to be restarted on their OAT. The client was forced to taper off their OAT over six days as a disciplinary measure for suspected diversion despite the client reporting no involvement, leading to a relapse on illicit fentanyl to combat withdrawal symptoms. This case study highlights the negative consequences that can emerge when opioid agonist treatment is discontinued as a disciplinary measure or is not accessible promptly. While incarcerated, discontinuing OAT puts individuals at increased risk of relapse and overdose as illicit drugs are often readily accessible in prison (Marmel & Bozinoff, 2020).
Psychiatric service access & usage
Several studies noted limited access to psychiatrists in prisons (Fayter & Payne, 2017; Iftene, 2019; Russell et al., 2022; Zinger, 2020; CAMH, 2020). Fayter & Payne’s (2017) study noted that the psychology department only allowed 12 sessions to incarcerated individuals. Hunter (2020) noted that psychiatrists are difficult to find and may not be available for extended periods if contracts are not renewed. Participants in Iftene’s (2019) book commented that the psychiatrist was available for five minutes every second year, and their primary role was to assess suicide risk. At Warkworth Institution, everyone was permitted three counseling sessions for the duration of their time at the institution (Iftene, 2019). Limited time with psychiatrists was also noted by Hunter (2020), whereby the time available for psychiatric assessment was shorter and less in-depth than those provided in the community. Correctional physicians do not get to know their patients the way they would in the community, limiting their role to managing symptoms rather than making complete diagnoses (Hunter, 2020). In the study by Russell and colleagues (2022), participants stated that physician visits were unreliable and infrequent; visits were often only once a month and, in some cases, not for several months, with waiting periods varying across institutions. The correctional investigator’s annual 2019-2020 report noted that planned staffing for correctional facilities did not match actual staffing at any site, resulting in high inmate-to-mental health staff ratios and limited access to mental health services (Zinger, 2020). For specialized services, which include psychologists and psychiatrists, the situation is exacerbated as all sites reported shortages or unreasonable long waits, ranging from 6-12 months (Zinger, 2020).
Gender-based differences in mental health care were highlighted in one study, revealing that women offenders may be overtreated (Martin et al., 2018). The study found that approximately 20% of inmates who self-reported a history, self-harm risk, or distress received more treatment than expected based on screening results. Moreover, research has found that women inmates are prone to being over-medicated with psychiatric drugs (Fayter & Payne, 2017), and have a higher frequency and proportion of psychotropic medication usage compared to their male counterparts (Johnson, 2021). Mental healthcare services have also been described as inequitable due to a lack of services that address the unique challenges experienced by women offenders, such as motherhood, and a history of sexual and physical abuse (Centre for Addiction and Mental Health, 2020). These findings suggest poor quality of mental health care among women, with inaccessible programs tailored to address gender-specific challenges.
Racial differences in mental health care access and provision were also found. The Centre for Addiction and Mental Health (2020) noted that Indigenous offenders have extremely limited access to culturally appropriate services and are less likely than other offenders to receive mental health care while incarcerated. Similarly, disparities related to responding to the needs of Black and other minority inmates were revealed. Black inmates who reported a previous mental health history had treatment rates slightly higher than expected based on screening results, but those who reported self-harm risk or distress were 1.41x more likely to be untreated (Martin et al., 2018). This pattern also existed for other minority inmates, who were 1.15x more likely to be untreated if they self-reported self-harm risk or distress (Martin et al., 2018). Similar proportions of white and Indigenous inmates received treatment, while black and other minority inmates had treatment rates that were approximately half those of white inmates (Martin et al., 2018).
Medical practitioners highlighted that severe mental illness, such as psychosis, is easier to treat pharmaceutically than less severe forms of mental illness, such as personality disorders (Hunter, 2020). Those without severe mental illness, and particularly those with personality disorder, are challenging diagnoses to manage and would benefit from care not currently offered in Ontario provincial prisons (Hunter, 2020). This population is then managed as a security problem (Hunter, 2020) which may include placement in segregation. For individuals without easily pharmacologically treatable mental health concerns, appropriate mental health care is insufficient and inaccessible (Hunter, 2020).
Systemic/Institutional Barriers
Barriers to mental health care delivery in prisons include a lack of privacy (Hunter, 2020). Correctional officers are often present during psychiatric consultations and assessments may sometimes need to be performed in the cell block, through the food slots, which limits non-verbal means of assessment and can impact assessment accuracy (Hunter, 2020). Correctional officers and the whole cell block can hear the interaction between doctor and patient, increasing the risk of individuals withholding information essential for appropriate treatment plan development. Doctors perceive little to no privacy or confidentiality in prison (Hunter, 2020).
Confidentiality issues may also arise when healthcare providers are employed by CSC staff, making inmates uncomfortable sharing information based on the concern that it will be recorded in their paperwork (Fayter & Payne, 2017). This challenge may be exacerbated in provincial prisons since many individuals in provincial custody are waiting for trial, so they may withhold information to prevent it from affecting their legal case (Hunter, 2020). Deprivation of liberty can also contribute to discomfort in sharing information as inmates cannot choose their care providers (Hunter, 2020). Lack of privacy and confidentiality impacts the accuracy of mental health assessment as well as the patient-doctor relationship, which can contribute to poor quality of mental health care and inability to access appropriate health services.
Insufficient space was a common challenge in prisons, with limited medical treatment rooms often used by multiple practitioners (Hunter, 2020; Zinger, 2020; Ghelani, 2020). Since prisons are not built with consideration of service delivery, even newer facilities may not have available room for physicians to see patients, resulting in competition for space (Zinger, 2020). Overcrowding, a current challenge in Ontario prisons, worsens this issue and some institutions have resorted to using cages to facilitate care where a physician and nurse sit outside the cage during a medical visit (Zinger, 2020). This may be traumatic for patients and can impede efforts to improve mental health as patients are hesitant to disclose information in such settings (Zinger, 2020).
Security issues impact mental health care access and delivery (Ghelani, 2020; Hunter, 2020; Zinger, 2020). Ghelani (2020) described the challenges of delivering group programs in a maximum-security detention facility in Toronto. Due to limited space, the program takes place outside client cells in the open area of a supportive care unit. Security or staffing issues and incidents in other areas (institutional searches or physical altercations) can affect staff availability to monitor programs (Ghelani, 2020). Zinger (2020) also reported security issues as a barrier to mental health programming in maximum-security institutions as many populations cannot mix. Hunter (2020) highlighted that even when treatment rooms are available, they may not be used due to security issues related to moving someone. Based on these findings, it is evident that both space and security issues can directly impact access to mental healthcare services.
Insufficient clarity regarding mental health perception
Correctional officers are central gatekeepers to medical care as they can bring mental health concerns about inmates to a nurse, who can then assess and refer them to a psychiatrist (Hunter, 2020). However, correctional officers’ understanding of mental illness is insufficient to efficiently fulfill this role. They have a subjective understanding of mental illness and obtain their knowledge through on-the-job experience (Hunter, 2020). As a result, medical professionals have limited access to those who need care, with many people not receiving any treatment (Hunter, 2020). Lack of clarity and understanding about mental illness and diagnosing disorders are also evident among professionals, as they are subject to professional interpretation and power dynamics (Hunter, 2020). Some medical professionals felt the need for further clarification, some felt that the Diagnostic and Statistical Manual of Mental Disorders (DSM) provides sufficient information, and others felt ambiguity about mental illness (Hunter, 2020). The lack of understanding and clarity regarding what mental illness is and how disorders are diagnosed leads to the question of who is recognized as having mental health concerns, and what kind of care they receive if they receive any (Hunter, 2020). This impacts the accessibility to mental health care, given that obtaining a diagnosis is needed to access treatment. Furthermore, insufficient clarity about mental illness & diagnosing disorders may lead to misdiagnosis or delayed diagnosis and as a result, inappropriate or delayed treatment. To provide high-quality mental health care, healthcare providers must have a thorough understanding of mental illness and how it is diagnosed. This is essential to facilitate accurate and timely diagnoses, as well as appropriate treatment.
Treatment of mental illness in the prison context classifies individuals as sick vs. not sick, but medical professionals emphasize that mental illness is more fluid than what the system allows for (Hunter, 2020). With the current system, individuals who are not sick enough to be considered to have a severe mental illness or in need of immediate attention get missed (Hunter, 2020). Thus, individuals who had their mental health managed in the community are disadvantaged when accessing mental health care in prison if they appear to be doing well as they may not get triaged until they present severe symptoms (Hunter, 2020).
Need for collaboration
Correctional officers can place a mental health ‘alert’ on an individual in the Offender Tracking Information System (OTIS) which can then be acted on by a nurse. However, these alerts carry little weight in an individual’s care path. Whether a nurse sees value in a correctional officer’s assessment influences the information general practitioners and psychiatrists receive, which may help with diagnosis or treatment (Hunter, 2020). Medical professionals noted they do not receive alerts; thus, these alerts do not accelerate care. This may be due to the subjective nature of alerts as correctional officers are not trained on when or how to use them (Hunter, 2020). However, correctional officers have more interactions with inmates compared with healthcare providers so their observations may be valuable in creating appropriate treatment plans. Not only is there insufficient collaboration and information sharing between healthcare providers and correctional officers, but also among practitioners, security and health professionals, and between levels of healthcare staff within an individual prison (Hunter, 2020; Sapers et al., 2017). A lack of reliable information-sharing between correctional officers and healthcare providers compromises access to care as inmates potentially requiring mental health care may not be followed up with by a nurse to determine whether treatment is necessary (Sapers et al., 2017). Correctional officers, healthcare providers, & security personnel may have useful information and insight regarding inmates’ mental health concerns, and everyone working in isolation from each other can lead to gaps in knowledge about the patient/inmate which can impact the quality of mental healthcare provided (Hunter, 2020).
Discussion
This scoping review synthesizes published research to present an overview of mental healthcare among adults incarcerated in Ontario. A scoping review approach was valuable to identify common themes relating to the quality and accessibility of mental health care in federal and provincial prisons in Ontario and to identify literature gaps. Limited research has been conducted on mental healthcare delivery inside Ontario correctional facilities and its outcomes. More research is warranted on the unique barriers to the provision of mental health care in Ontario prisons.
The sixteen studies included in this review identified barriers to providing quality and accessible mental health care services for adults who are incarcerated in Ontario. The data suggest that mental health care in both provincial and federal facilities in Ontario is not meeting standards set out by the Canada Health Act and Corrections and Conditional Release Act. Rather, the quality of health care provided to the incarcerated population is below standard with many of the health care requirements not being performed appropriately, in a timely manner, or completed at all. Poor accessibility to mental health care was influenced by a multitude of factors including insufficient institutional resources, staff shortages, institutional policies, lack of information sharing between correctional personnel, as well as staff preferences and availability. This is particularly true for the completion of screening assessments which determine treatment plans for offenders and influence if an inmate is placed in segregation. The performance of assessments by correctional officers rather than qualified nurses due to staff shortages increases the severity of negative consequences caused by insufficient knowledge and training in mental health held by correctional officers. In this way, not only do staff shortages impact the accessibility of mental health care directly by introducing barriers to interacting with healthcare providers and accessing medications, but also indirectly through inaccurate screening processes and mental health assessments. Further research is needed on the mental health screening and assessment processes across correctional facilities to assess whether they are appropriately performed and how they are impacting healthcare access and quality.
In addition to the factors mentioned above, insufficient clarity regarding mental illness and inadequate collaboration compromise the ability to provide quality mental health care for the incarcerated population. Many of the barriers to the access and quality of mental health care that were highlighted in this review are shared between both provincial and federal correctional facilities. However, a couple of challenges that were specific to provincial or federal correctional facilities were observed. For provincial facilities, barriers to accessing OAT can be exacerbated compared to federal facilities due to the shorter duration of custody in these settings. Given the limited access to psychiatrists and limited information sharing as a result of insufficient collaboration between correctional and healthcare personnel, there is insufficient time to form a therapeutic relationship or gather all relevant information needed to make a complete diagnosis and comprehensive treatment plan. This raises concerns about the quality of mental health care available to incarcerated individuals in provincial and federal settings. With the existing barriers, reliance on using pharmacotherapy to manage symptoms of severe mental illness seems to be the only choice, and those without severe mental illness are overlooked with limited management options. Those with mental health concerns that are not easily managed with pharmacological treatment are particularly disadvantaged in provincial facilities considering the shorter periods of stay. Barriers arising from healthcare providers being employed by CSC staff are also exacerbated in provincial settings due to the concern that information that inmates share will be recorded in their paperwork and will affect their legal case.
In federal correctional facilities, a specific theme that arose relating to mental health care access and quality related to gender and racial disparities in treatment, including overtreatment of women with psychiatric drugs, decreased rates of treatment among Black inmates, and lack of culturally appropriate programming for Indigenous inmates. To address these inequities, further research should investigate the factors influencing such healthcare practices. More information on institutional programming, its accessibility, usage, quality, and value for the incarcerated population would be beneficial. This knowledge would help assess the extent to which these programs are achieving their objectives and identify potential areas for improvement to better address the unique needs of subpopulations within correctional facilities. Consulting members of the incarcerated population to gather this information and identify priorities is crucial.
The findings in this review contribute a clearer understanding of the impact of staff attitudes, insufficient collaboration, and staff preferences on mental healthcare delivery in correctional facilities. This was particularly relevant for delivery of mental health care treatments in the face of space and security challenges, the value of correctional officers as gatekeepers to care, and OAT provision. Despite limitations presented by insufficient space and security, Hunter’s (2020) study participants felt that a significant contributor to mental healthcare management is the staff responding to the issue. Interviewees felt that effective treatment could occur even with spatial limitations if staff, particularly security staff, wanted it to, stressing the value of security staff supporting work done by the mental healthcare team (Hunter, 2020). Further investigation to explore whether staff attitudes play a role in the inaccessibility of mental health care programming may be valuable to determine whether addressing this can be a target to improve mental health care accessibility.
Insufficient knowledge of mental health among correctional officers plays a part when addressing insufficient collaboration within correctional institutions. Correctional officers are gatekeepers to care and have more experience with inmates than healthcare providers. Thus, they can serve as valuable resources to connect inmates who need care with appropriate resources. However, their alerts and insight carry little weight in the care path. This can be justified if they do not possess sufficient knowledge of mental illness, however, their potential to serve as resources to increase mental healthcare accessibility for incarcerated individuals highlights the need for more mental health training for correctional officers and collaboration with healthcare providers. Further review regarding the effectiveness of OTIS in fulfilling its function to signal a potential mental health concern and trigger assessment for appropriate healthcare support for inmates is also necessary. Based on the review’s findings, an interdisciplinary care approach, which emphasizes collaboration and information-sharing between correctional officers, security personnel, and correctional healthcare providers has the potential to improve the limitations that exist related to the provision, accessibility, and efficiency of mental healthcare in Ontario prisons. Everyone must be invested to address the complex mental health needs of the incarcerated population.
As outlined in CSC’s guidance on opioid agonist treatment document, consistent and standardized OAT practices are required across all sites and regions (Correctional Service of Canada, 2021). However, the practices set out in this guide don’t seem to be adhered to. Rather, preferences amongst correctional healthcare providers were found to be relevant for medication prescribing and timely access to OAT, contributing to inconsistent practices across institutions. The guide also highlights that effective OAT incorporates physical and mental health care along with harm reduction in an integrated fashion, which may include counseling, comprehensive primary care, and psychosocial treatment (Correctional Service of Canada, 2021). The current quality of treatment provided does not meet expectations and the guidelines set out by CSC may not be feasible based on the challenges highlighted in this review, including insufficient space and staff shortages. An additional avenue for future research is Drug Treatment Courts (DTC), which offers eligible offenders with a substance use disorder the chance to complete a court-monitored drug treatment program as an alternative to incarceration (Government of Canada, 2023). The use of DTCs has been shown to reduce recidivism rates compared to traditional criminal justice interventions, decrease substance use, and improve quality of life among participants, even among those who did not graduate from the program (Centre for Addiction and Mental Health, 2020). Funding is a barrier to DTCs; however, further research is warranted to determine the effectiveness and value of DTCs, specifically whether it could help improve access to OAT treatment for offenders and how this may broadly impact barriers to mental health care provision in correctional facilities.
In their final report, Ontario’s Advisory Committee on Healthcare Transformation in Corrections called for a system-level transformation emphasizing integrated, consistent healthcare with increased transparency, coordination with the broader health system, continuity of care, and funding (John Howard Society of Ontario, 2019). To improve mental healthcare in correctional facilities, a level of continuity between community and correctional healthcare is needed. This would be valuable in the context of accessing psychiatric medications and OAT, particularly in custodial settings. This type of systems-level change could also help overcome the restrictive perception of health as sick vs. not sick, which prevents care from being provided until individuals develop acute or severe health conditions.
This review revealed challenges arising from the present configuration of correctional healthcare, where the Ministry of Justice or the Correctional Service of Canada holds the responsibility for healthcare. Other Canadian provinces including Alberta, Quebec, B.C., and Newfoundland have taken action to transfer responsibility for healthcare from the Ministry of Justice to the province’s Health Authority (John Howard Society of Ontario, 2019). The inadequate quality and accessibility of mental health care supported by the findings of this review add support to the recommendation made in the Independent Review of Ontario Corrections (Sapers et al., 2017) and by The College of Family Physicians of Canada (2016) for all provinces and territories to transfer responsibility of correctional healthcare delivery to the ministry of health and separate from CSC for federal facilities. However, further research is warranted to assess the impact of this transition on mental healthcare in correctional facilities and determine how a change in healthcare governance can best be implemented to improve healthcare for the incarcerated population in Ontario.
Limitations
There are several limitations to this review and the presented data. Although numerous databases were searched and a comprehensive search strategy was used, relevant studies may have been missed including texts published outside the search period and texts in the gray literature. In the study search, selection, and data extraction process, study quality was not assessed and only one reviewer performed the process. This may have resulted in the non-detection of relevant studies and increased risk of bias. Further, this review relied on research and grey literature to acquire an understanding of mental health care in correctional facilities in Ontario. As a result, the article may not fully capture the entire scope of the topic, as there are aspects of mental health services that are not disclosed in the literature. Moreover, the definition of mental health services included those provided inside correctional facilities and excluded other types of offender programming such as sex offender and batterer programming. Although these types of programming may not directly treat mental health issues, they address behavioral risk factors that may impact mental health and function as a form of mental health care. Thus, the information presented in this review may not be fully representative of the range of mental health care available to individuals incarcerated in Ontario. Lastly, limited research on the topic compromises the reliability and validity of data. Many studies also implemented a self-reporting methodology which can introduce the potential for misinformation and bias, and findings may not be generalizable.
Conclusion
Mental illness is a significant issue among adults incarcerated in Ontario correctional facilities, however, the delivery of mental health care in the institutions is not adequate to meet the needs of these individuals. There are significant gaps in the literature relating to mental health care access and quality among minority and Indigenous populations, women inmates, and challenges related to providing care in provincial institutions. Healthcare providers, policymakers, and researchers should investigate and assess current mental healthcare practices in Ontario prisons and use acquired data to inform the implementation of interventions to meet the mental health needs of the incarcerated population.
Supplemental Material
sj-docx-1-ijo-10.1177_0306624X241228218 – Supplemental material for The State of Mental Health Services for Incarcerated Adults in Ontario: A Scoping Review
Supplemental material, sj-docx-1-ijo-10.1177_0306624X241228218 for The State of Mental Health Services for Incarcerated Adults in Ontario: A Scoping Review by Sara Mohamed in International Journal of Offender Therapy and Comparative Criminology
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.