
Abstract
Since the Good Lives Model’s (GLM) inception, researchers and practitioners have faced questions about its implementation. Programs claiming to use the GLM vary substantially in the extent to which the GLM informs treatment, and no tools exist to monitor therapist fidelity to the GLM. The aim of the current paper is to offer a concrete tool to monitor therapist fidelity to the GLM. The GLM Fidelity Monitoring Tool offers the beginnings of a method for how therapists and supervisors can address the central question of “How well are we implementing the Good Lives Model?” The tool consists of three sections: (i) Fundamental Considerations and Processes, which focus on therapeutic process variables consistent with the GLM but not specific to the GLM, and are rated numerically for fidelity, (ii) GLM-Specific Considerations and Processes, also rated numerically for fidelity, and (iii) Client-Focused GLM Considerations, which are a set of questions exploring the therapist’s progress developing a GLM grounded case formulation and therapy plan for individual clients. The tool is designed to help guide supervision discussions and promote therapist fidelity to the GLM. Future research implications are discussed.
Keywords
Despite many years of focus by researchers and practitioners on developing evidence-based practices, many challenges remain (Ward et al., in press). Although recent decades have seen a proliferation of evidence-based treatment protocols, arguably less attention has been paid to evidence-based therapeutic relationships (Prescott et al., 2017). Just as concerning is that programs seeking to put evidence-based practices into effect are often unaware of the research into best practices for implementing these approaches (Fixsen et al., 2005). Ultimately, attending trainings, reading journal articles, and even diligent practice cannot guarantee adherence to a practice or fidelity to a model. In the authors’ experience providing training to agencies in the practical application of the GLM around the world, most practitioners strongly desire to implement the GLM with integrity. Many have asked for guidance in ensuring the most effective possible implementation. In some cases, practitioners have openly altered their practices into something that they call the GLM when in fact, it isn’t. Unfortunately, misguided implementation risks compromising the integrity of otherwise evidence-based treatment programs, which in turn may result in higher rates of re-offense. The overall aim of the current paper is to provide a concrete tool to monitor therapist fidelity to the GLM.
Schoenwald et al. (2011) describe three components of treatment fidelity. These include therapist adherence to a treatment model (including using prescribed methods and avoiding proscribed activities), therapist competence (including the level of skill in implementing the treatment), and treatment differentiation (which involves ensuring that the treatment delivered is true to the developer’s intentions, with overlap into other approaches only as intended). Schoenwald et al. (2011) further describe a number of ways in which fidelity can be measured. They make the case that there can be several approaches and methods to ensuring fidelity, from asking therapists to assess themselves (or having their clients rate them) to having supervisors monitor sessions either in person or through a review of recordings made of sessions. Depending on the nature of the implementation, these reviews might occur once or across multiple sessions depending on the treatment and its implementation. Further, the construction of rating scales can differ depending on the treatment and its implementation. In examining items, scales may include the presence or absence of a technique or attribute or assign a rating of the quality of work from poorly done to excellently accomplished. There is no indication that there is one particular means by which to develop ratings for items; ultimately, the construction of fidelity measures depends on the desired outcomes of treatment and its implementation.
Implementing the Good Lives Model
The Good Lives Model (GLM) is a strengths-based theory of rehabilitation developed and elaborated on by Tony Ward and colleagues from the early 2000s (Ward, 2002; Ward & Maruna, 2007; Ward & Stewart, 2003). The GLM was developed to address identified shortcomings of treatment that focuses almost exclusively on risk reduction, including the inherent difficulty motivating and engaging clients in treatment when treatment program aims may not necessarily align with the client’s values and priorities. The GLM adopts the dual aims of risk reduction alongside supporting clients to develop and implement a prosocial good life plan underpinned by the client’s core values, priorities, and strengths. The GLM accommodates the RNR principles and criminogenic needs are conceptualized as signaling problems with capacity to achieve primary human goods (e.g., relationships, mastery, inner peace, and autonomy) in prosocial ways. Criminogenic needs are thus addressed in the broader pursuit of strengthening a client’s capacity to achieve valued goods (vs. addressing criminogenic needs with the sole aim of reducing risk) by way of the acquisition of internal (e.g., skills and knowledge) and external resources (e.g., social supports and vocational training). The GLM has been embraced by treatment providers in a wide range of settings and in countries all over the world (e.g., The USA and Canada, McGrath et al., 2010); however, early observations of programs advocating a GLM approach showed variation in the extent to which the GLM was implemented in practice (Willis et al., 2014).
Willis et al.’s (2014) multi-site study exploring the application of the GLM in 13 North American sexual offending treatment programs found that operationalization of the GLM included reframing of program components using approach versus avoidant goals, adopting individualized rather than one-size-fits all treatment/intervention plans, expanding a program’s focus and content beyond criminogenic needs (often through the addition of a GLM inspired assignment or module), and treating clients with dignity and respect. All of these strategies are consistent with a GLM approach; however, on their own they fall short of what might be considered a GLM derived intervention. The GLM was largely absent from assessment practices and protocols and individualized intervention plans often amounted to extra space for client goal/s to be added to generic treatment goals. The majority of programs were considered to show some responsiveness to the GLM; however, integration was largely additive to an overarching focus on risk management and relapse prevention. Only 2 of the 13 programs formally integrated GLM concepts into program content. These findings were not surprising given that at the time data were collected, few resources were available to support clinicians implement the GLM. The number of GLM resources for clinicians working across settings and client groups have since multiplied (e.g., Barnao, 2013; Barnao et al., 2016; Prescott, 2018; Prescott & Dent, 2018; Purvis et al., 2013; Willis et al., 2013; Yates & Prescott, 2011). Yet resources do not guarantee therapist and treatment fidelity to the GLM.
Individually and collectively, the authors have provided training to various agencies seeking to implement the GLM in offending treatment programs. Lessons learned from international implementation projects are described in (Prescott & Willis, 2021). Briefly, a recurring challenge observed by the authors is upholding the GLM as an overarching practice framework (see Ward & Durrant, 2021), whereby treatment is informed by the client’s good life plan and the obstacles they have faced in their pursuit of primary human goods. Necessarily, such a focus includes addressing hypothesized causal processes underlying offending. Problematically, and inconsistent with the GLM, such processes are often reduced to a list of dynamic risk factors, with treatment plans centring on reducing dynamic risk factors (see Heffernan et al., 2019). The authors have observed a disconnect between addressing risk factors and supporting clients work toward attaining prioritised primary human goods in personally meaningful, adaptive ways. To illustrate, sexual interest in children, emotional congruence with children, and offense-supportive cognitions are empirically supported risk factors for sexual reoffending (Mann et al., 2010). For some clients, such risk factors may originate in childhood bullying and perceived rejection by adults and peers. The individual may perceive children as less threatening and more accepting, and gravitate toward children to meet relational needs (primary human good = relationships and friendships). Utilizing the GLM, treatment goals would focus on strengthening the client’s capacity for experiencing meaningful adult relationships and friendships, which would necessarily involve addressing obstacles (including maladaptive schemas and associated risk factors, and/or the residual effects of traumatic experiences, e.g., by impeding the development of internal capacities to attain primary human goods more effectively) that previously precluded the individual from experiencing relationships and friendships in adaptive, nonharmful ways. By contrast, focusing treatment goals specifically on dynamic risk factors without reference to primary human goods is inconsistent with the GLM. Thus, according to the GLM, dynamic risk factors are seen as summary labels for clusters of causal, contextual, and mental state factors that need to be disentangled in order to (a) adequately explain the reasons why someone offended and (b) to develop an effective good lives plan (see Ward, 2016).
The ability to clearly operationalize fidelity to rehabilitation theories or frameworks helps facilitate research examining the effectiveness of different therapeutic elements and approaches. Indeed, the principles of effective correctional interventions and in particular the highly influential risk, need, and responsivity principles (Bonta & Andrews, 2017) have been defined concretely and operationalized into various fidelity assessment protocols, with greater fidelity associated with improved treatment effectiveness (see Duriez et al., 2018). Thus, fidelity monitoring helps promote evidence-based practice. Despite its popularity, no tools exist to monitor fidelity to the GLM. Willis et al. (2013) outlined how to integrate the GLM into a program’s aims/orientation, assessment and intervention planning, treatment content and delivery—guidelines which provided the basis for exploring overall program fidelity to the GLM in Willis et al. (2014).
Briefly, treatment programs that are GLM-consistent focus on the dual aims of risk reduction and the enhancement of wellbeing. The underlying ethos, program guidelines and therapy plans use approach-oriented (as opposed to avoidance-based) language (for further discussion, see Mann et al., 2004; Willis et al., 2013; Yates et al., 2010). A prerequisite to GLM application is that each client has received a comprehensive individualized assessment to inform a working formulation of the client’s offending and its associated problems, which includes use of validated measures to identify empirically supported risk factors alongside key GLM considerations such as identifying primary goods implicated in offending and those prioritized in the client’s life currently. The aim of the current paper is to supplement the Willis et al. (2013) program guidelines with a concrete tool to monitor therapist fidelity to the GLM. In the sections that follow, we briefly introduce the GLM Fidelity Monitoring Tool, before reviewing each section in depth. The current paper concludes with a discussion of the tool’s current utility, and implications for future research.
Introducing the GLM Fidelity Monitoring Tool
To reiterate, the GLM is an overarching rehabilitation model and practice framework intended to be used in an individualized manner and in accordance with the principles of effective correctional treatment (see Bonta & Andrews, 2017) as well as factors such as those that make up the therapeutic alliance (Bordin, 1979; Prescott et al., 2017). Therefore, fidelity can be examined through observing therapy sessions, and through reviewing case conceptualizations and intervention plans for individual clients. The GLM fidelity monitoring tool is designed to support GLM implementation when working with adult clients across forensic/correctional treatment settings. The tool is intended for use by supervisory staff who are reviewing sessions (either in person or through recordings) and relevant written documentation (e.g., assessment reports). It can also be used as a self-reflection measure by clinicians who want to strengthen their understanding of the GLM and their adherence to key principles. However, its use solely as a self-reflection measure will be limited without any external feedback and clinical discussion. Ultimately, this tool is intended as a supervisory tool used in the spirit of team-driven continuous quality improvement. In designing the current tool, the authors examined approaches that have proven themselves to be effective in fidelity monitoring in similar circumstances, such as the Motivational Interviewing Treatment Integrity measure (Moyers et al., 2014). Alongside rating the extent to which various GLM consistent features are observed, professionals using this tool can consider what kinds of activities and processes are entering treatment that do not reflect the items described, and the extent to which they are compatible with a GLM approach to treatment as outlined in Willis et al. (2013).
The GLM fidelity monitoring tool comprises three sections, summarized in Table 1. Section 1 examines fundamental considerations and processes, Section 2 focuses on GLM specific content, and Section 3 offers practitioners and supervisors a set of questions to help guide self-reflection and supervision discussions as they relate to individual clients. Sections 1 and 2 include numeric ratings based predominantly on session observations (and written documentation, when relevant); items are rated on a 3-point scale, with 0 indicating poor (or absent) fidelity, 1 indicating partial fidelity, and 2 indicating fidelity. We recommend that supervisors and supervisees rate items prior to or during clinical supervision sessions and use ratings to help guide supervision discussions.
GLM Fidelity Monitoring Tool Overview.
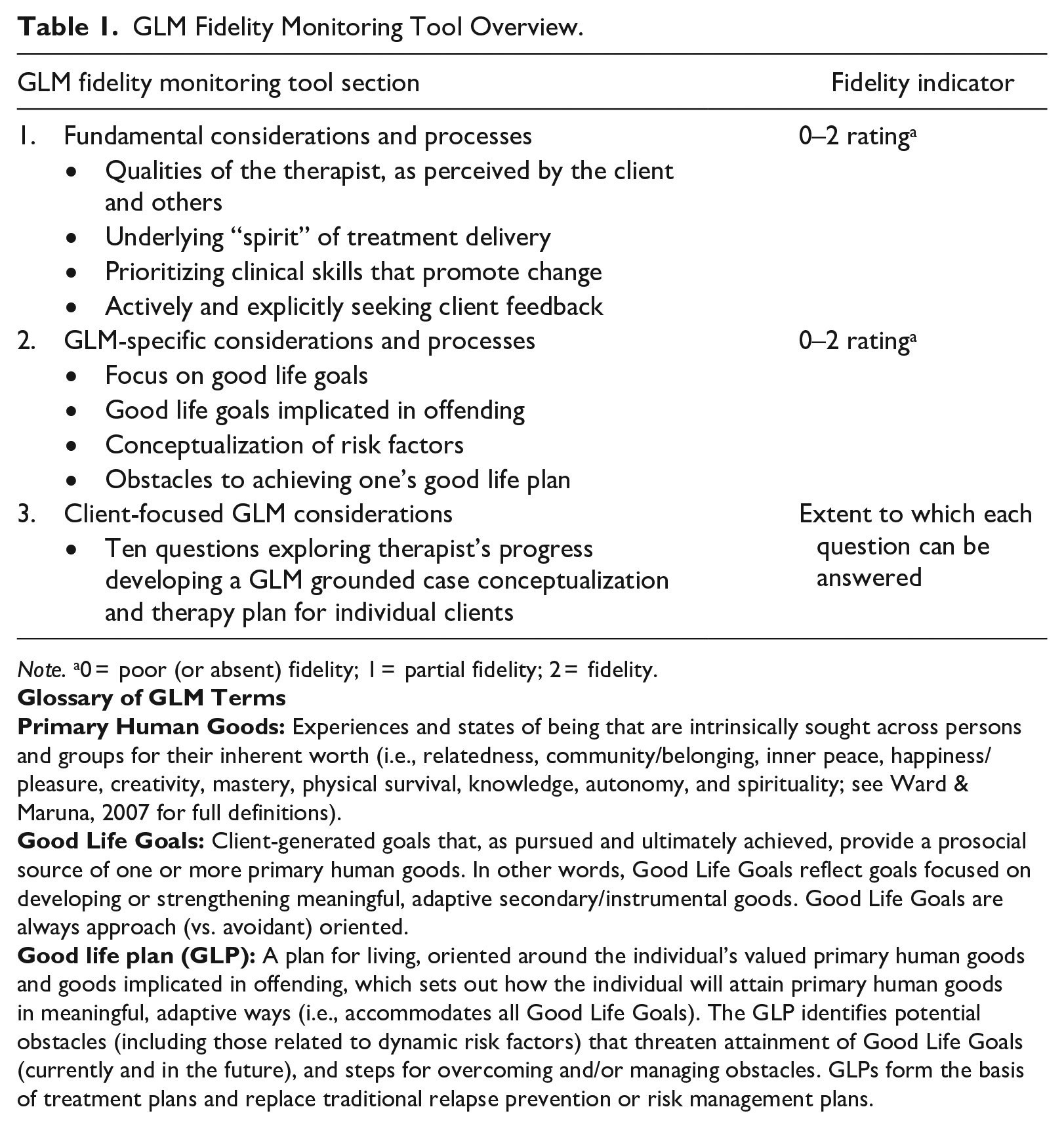
Note. a0 = poor (or absent) fidelity; 1 = partial fidelity; 2 = fidelity.
Section 1: Fundamental Considerations and Processes
Many items included in this section are derived from the general literature on effective therapeutic approaches with people who have abused and/or committed other crimes, as well as the general psychotherapy literature. They are included in this tool because of their explicit overlap with the intended atmosphere in which the GLM is applied.
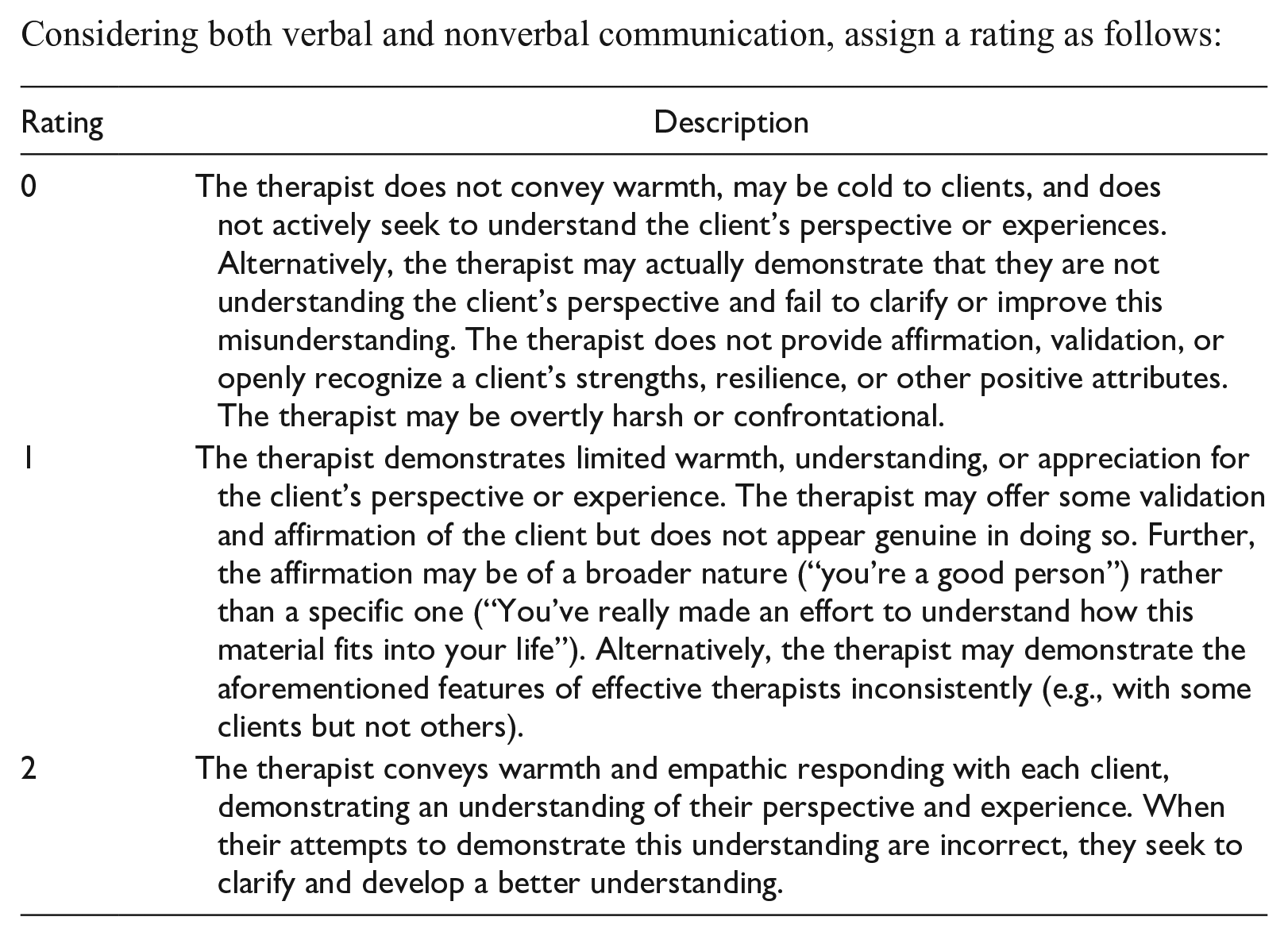
Qualities of the therapist, as perceived by the client and others
As highlighted by Bill Marshall and colleagues (e.g., Marshall, 2005; Marshall et al., 2003), effective therapists are:
Warm
Empathic
Rewarding
Directive (in other words, keeping the flow of treatment moving/not becoming stuck)
Unlikely to engage in harsh or confrontational behavior
Considering both verbal and nonverbal communication, assign a rating as follows:
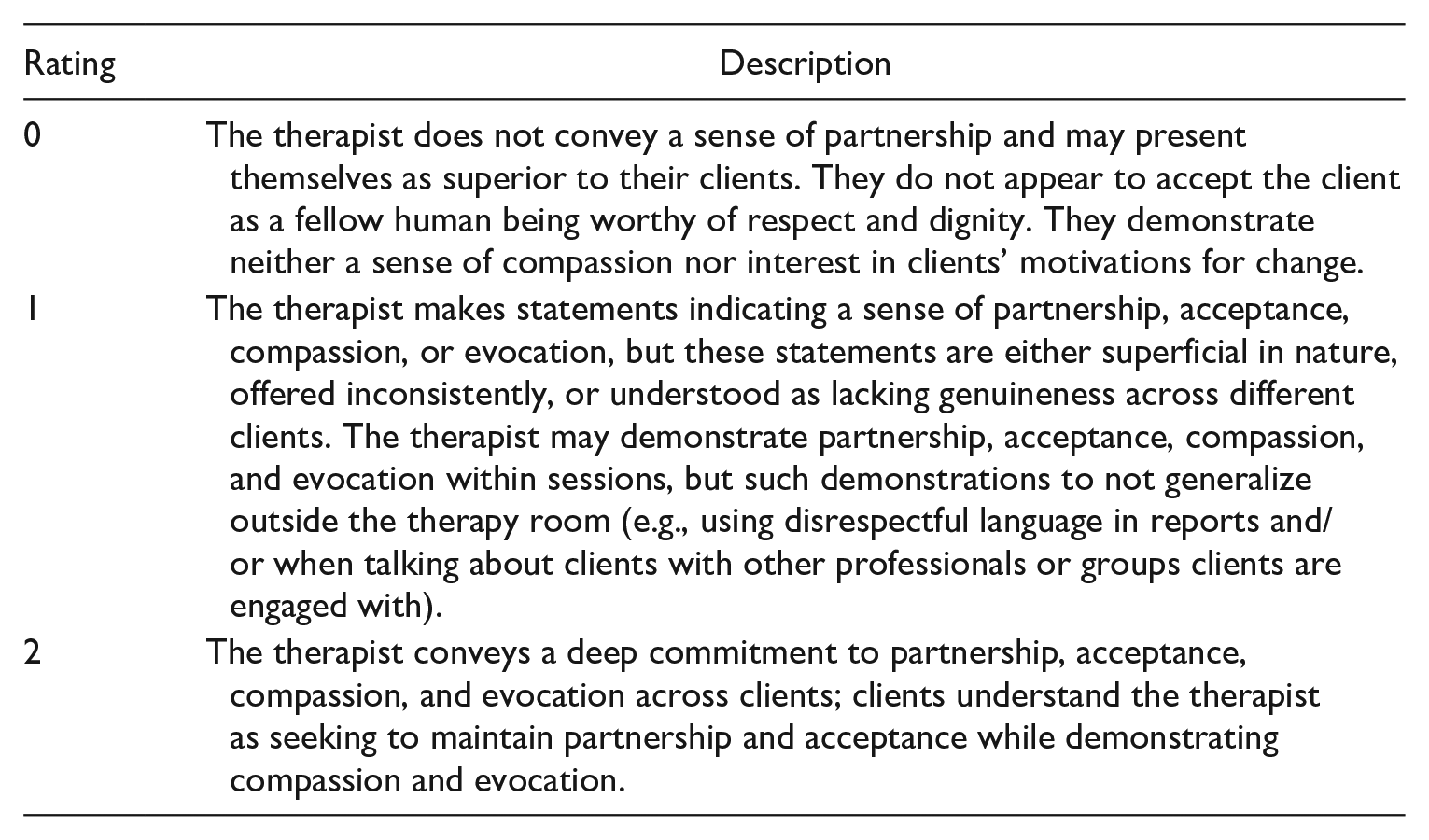
Underlying “spirit” of treatment delivery
The following attributes are taken from the Motivational Interviewing literature, where they have received considerable empirical support (e.g., Hettema et al., 2005; Miller & Rollnick, 2013; Moyers et al., 2014).
Partnership: the therapist views the client as a fellow human being and displays no moral judgment about them as a person. Moreover, when talking with and about clients, they use respectful language, avoiding stigmatizing and potentially harmful labels (see Willis, 2018)
Acceptance: the therapist fully accepts the client as a fellow human being who is therefore always worthy of respect and dignity, while condemning their offending behavior. In other words, clinicians accept the person, but not the offending behavior.
Compassion: the therapist seeks to understand the client’s experiences (i.e., thoughts and feelings) and prioritizes their best interests in the development of an intervention plan.
Evocation: the therapist demonstrates an interest in the client’s personal motivation to make positive changes in their life and listens closely to identify their values, goals, strengths, and other positive attributes.
Considering both verbal and nonverbal communication, assign a rating as follows:
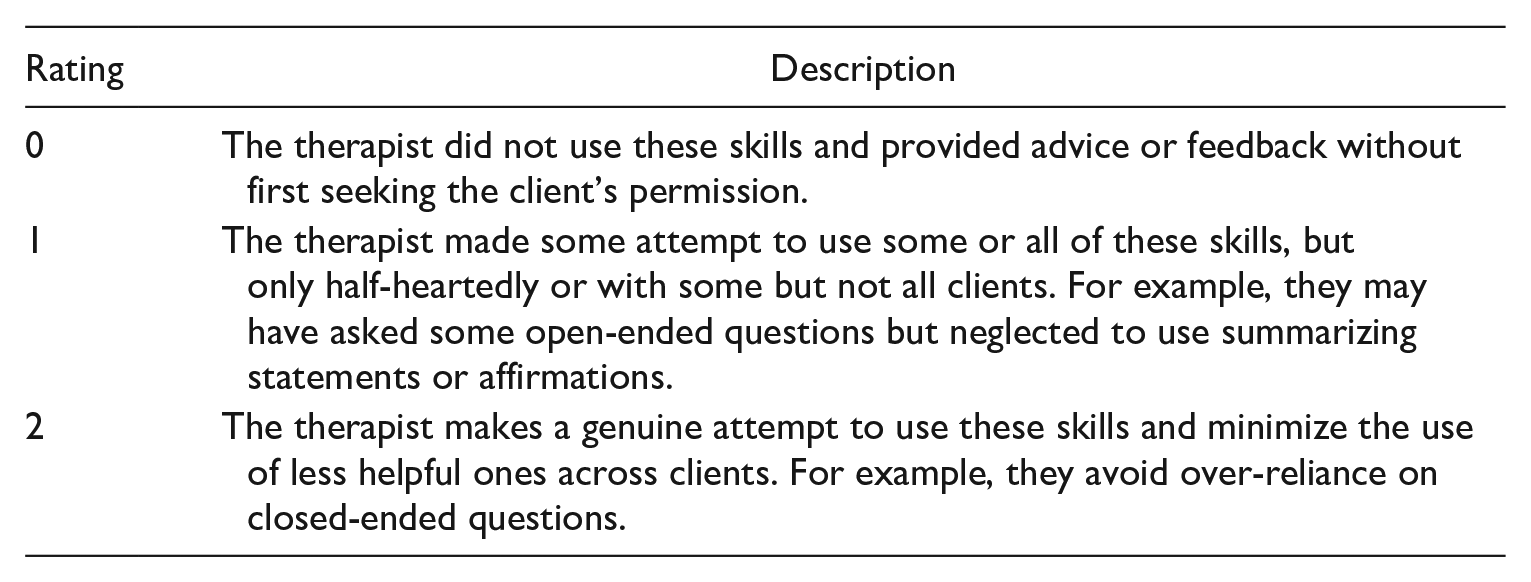
Prioritizing clinical skills that promote change
The following skills are also taken from the Motivational Interviewing literature, where they have considerable research support (e.g., Hettema et al., 2005 Miller & Rollnick, 2013; Moyers et al., 2014). These skills have been chosen because of their direct link to client autonomy and the fact that they help to elicit the client’s internal motivation to change, which in turn helps them to envision goals that they can achieve rather than avoid.
Open-ended questions
Affirmation
Reflective statements
Summarizing what the client is saying
Giving advice or feedback only with permission of the client
Although these clinical skills can be measured concretely using behavior counts and parsing speech, the intent for this tool is simply to monitor the therapist’s overall use of these skills. Assign a rating as follows:
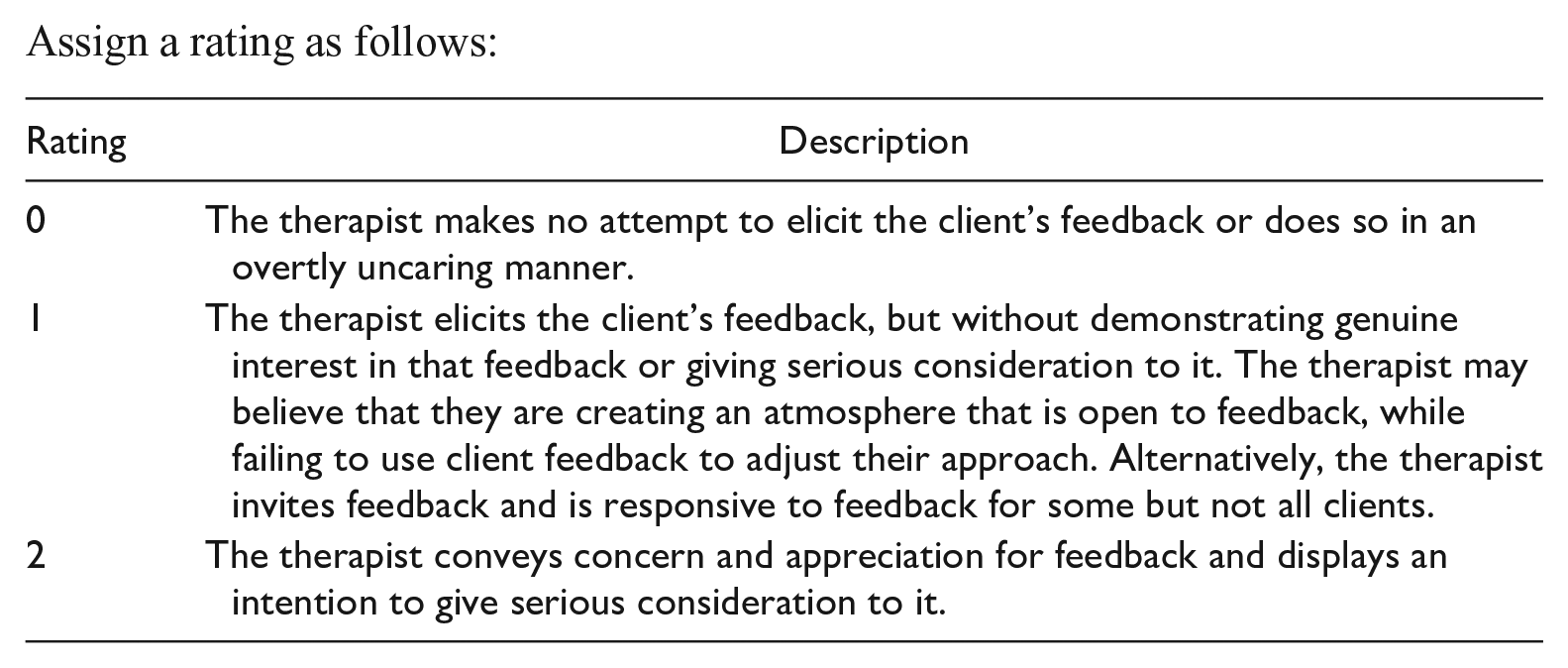
Actively and explicitly seeking client feedback
This item is based on empirical research on the nature of the therapeutic alliance and how best to establish and maintain it (see Prescott et al., 2017 for a review). In order to ensure a strong therapeutic alliance, the therapist actively seeks out feedback to ensure that treatment activities are personally meaningful and relevant and that:
The client feels heard, understood, and respected.
The client experiences treatment goals as meaningful, relevant, and important.
The client believes that the therapist’s approach is a good fit for them.
The client believes that the therapist is taking into account their culture and other deeply held personal values.
Client feedback concerning the therapeutic relationship takes place in an atmosphere where the client is confident that the therapist will actively consider it, and the s/he does not fear negative consequences of this feedback.
Assign a rating as follows:
Section 2: GLM-Specific Considerations and Processes
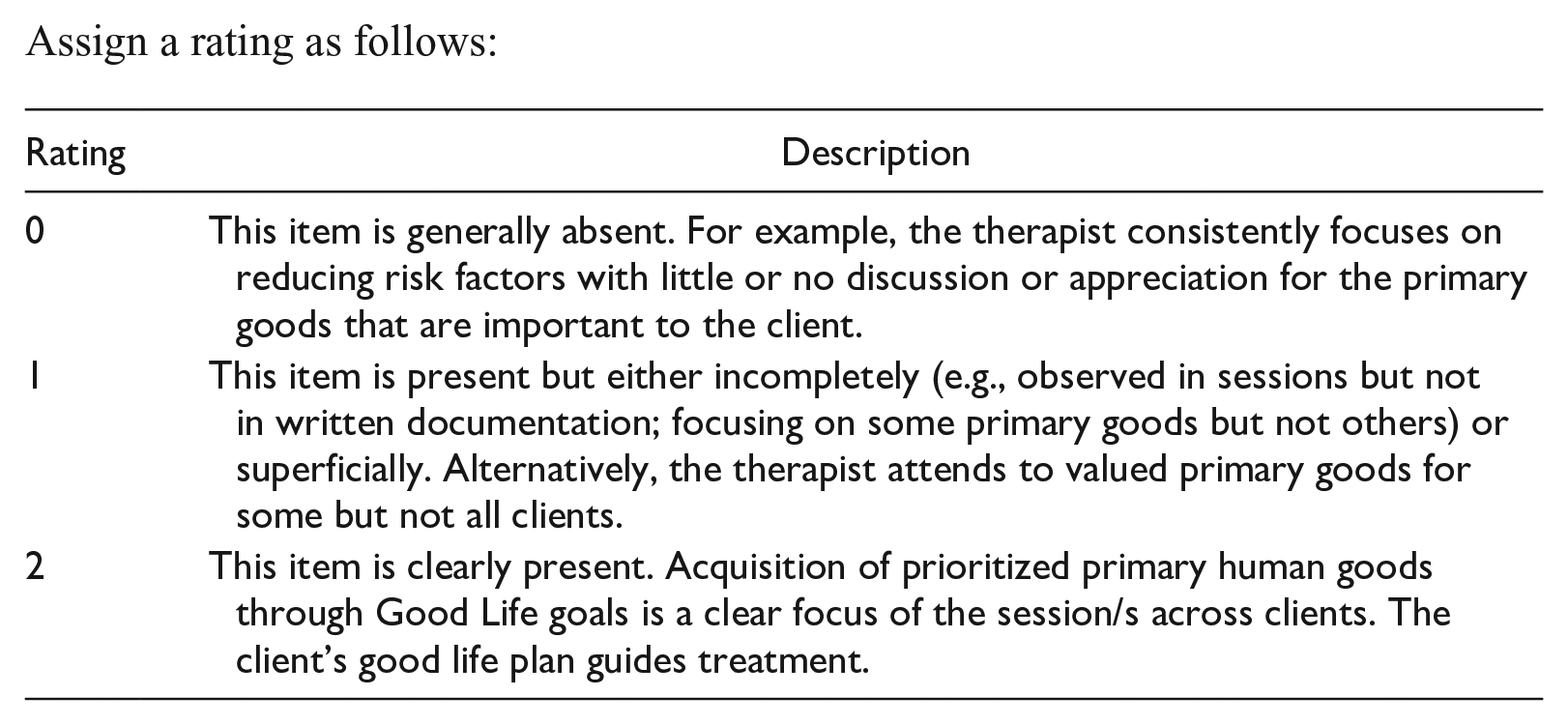
Focus on good life goals
The guiding consideration here is that case formulations and treatment sessions focus on acquiring valued primary goods through Good Life goals as well as managing risk factors.
A focus on approaching/acquiring primary goods is clear in each session, with the focus for each client reflecting their prioritized primary human goods.
Documentation of treatment sessions and relevant assessments reference valued GLM primary goods and/or Good Life goals.
All primary goods are included in some way, even though they may be prioritized differently. In other words, no goods are left out of the treatment process entirely.
The therapist is ready, willing, and able to help the client talk about relevant and meaningful goals and develop an understanding of how the client’s own goals relate to the GLM primary goods. For example, if the client’s only goal is to be able to run a marathon, the therapist can explore underlying primary goods such as “excellence at work and play” and “living and surviving.”
Assign a rating as follows:
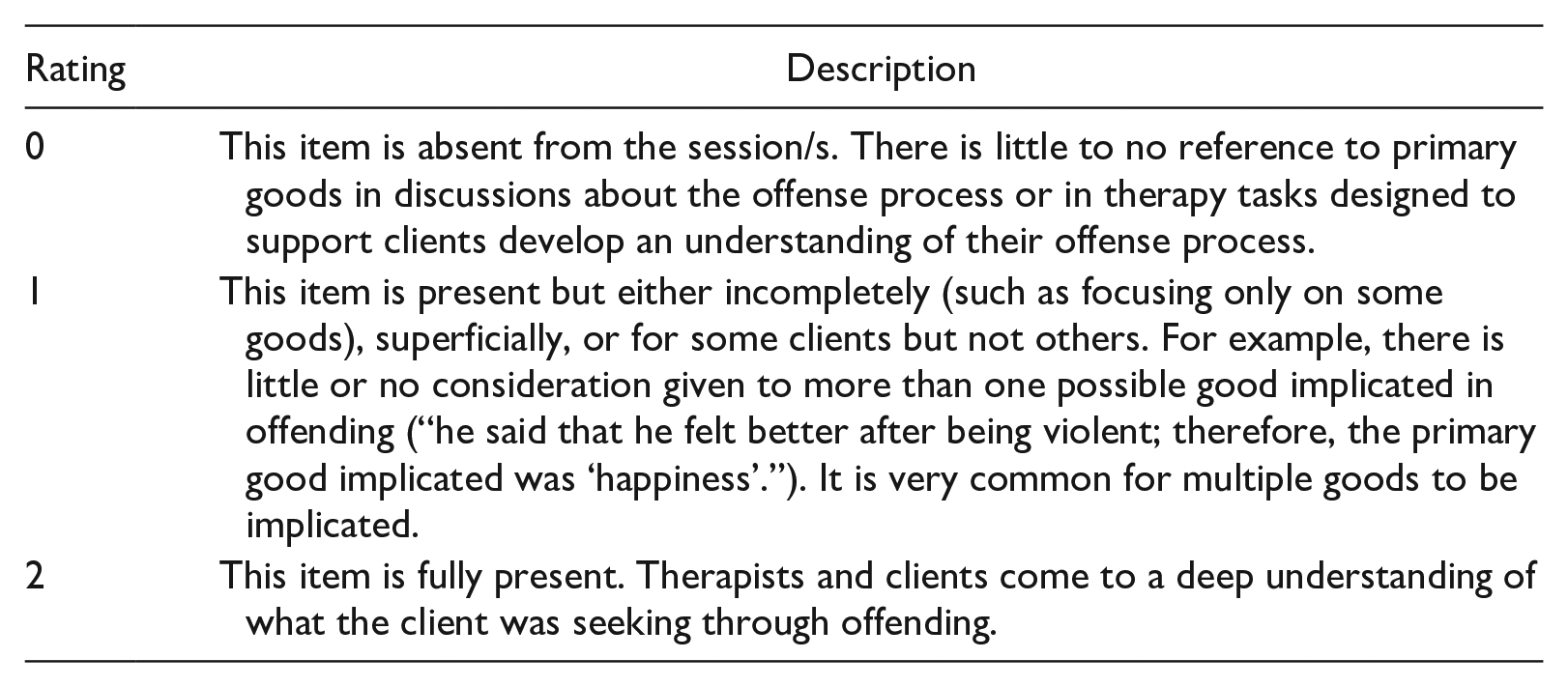
Good life goals implicated in offending
As an overarching rehabilitation theory encompassing etiological assumptions with respect to offending (see Ward & Maruna, 2007), the GLM is concerned with more than simply living a good life. It also involves understanding how the pursuit of good life goals was implicated in an individual’s offending and in their associated psychological and social problems. In other words, the GLM proposes that underlying even the most egregious behaviors are primary goods that are common to all human beings in one form or another. For example, the primary good of “relationships and friendships” is implicated in a crime where a person sexually abuses children while believing that they have a “special” relationship with them. The goal of having a relationship is central to being human. Pursuing sexual relationships with children, however, poses an unacceptable risk to the child, their loved ones, and the individual seeking the relationship.
Clinical sessions and documentation include a clear understanding of:
Which primary goods were implicated in a given offense
How primary goods were implicated (in other words, the therapist and client have arrived at a mutually agreed-upon explanation of how certain goods were implicated in an offense).
Assign a rating as follows:
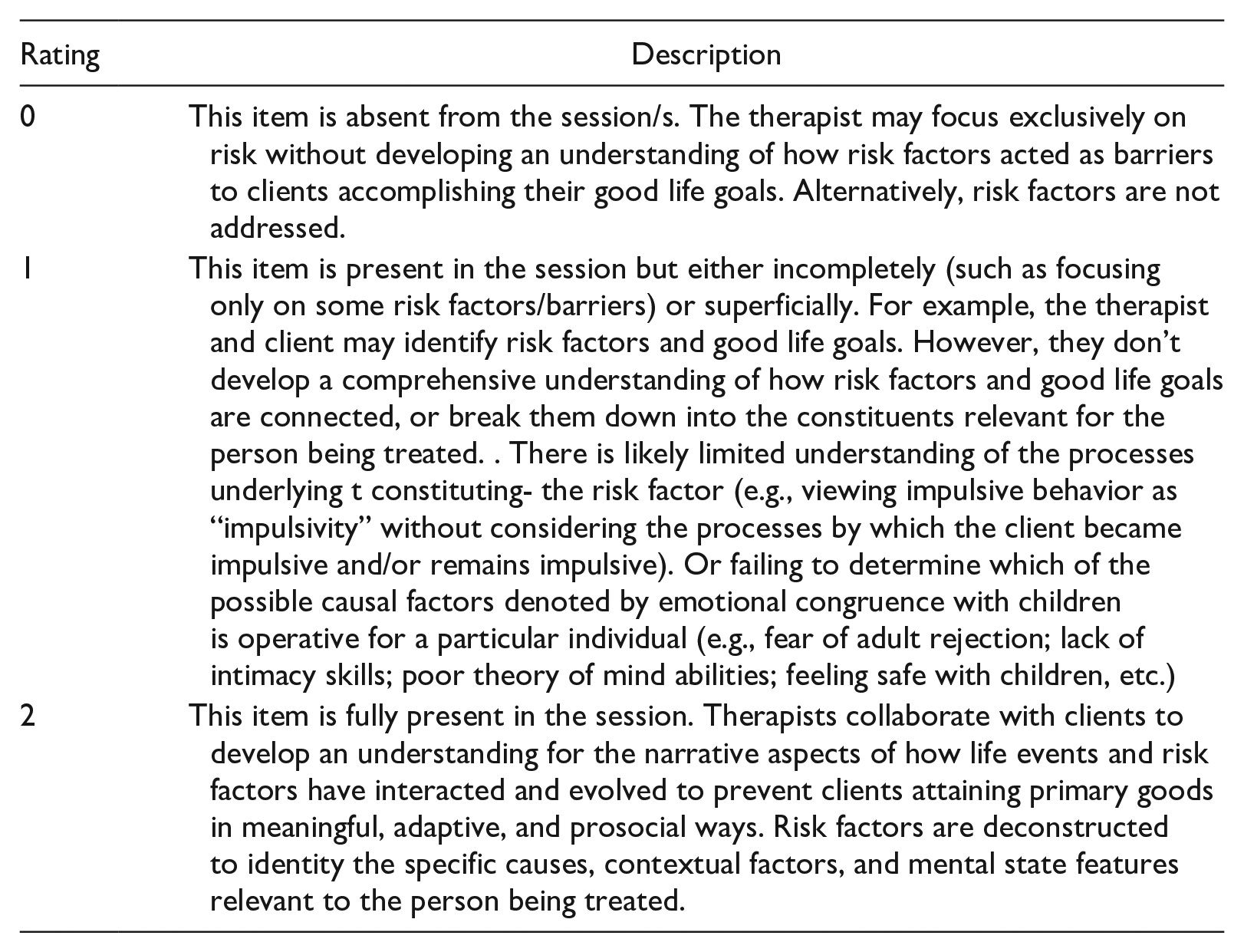
Conceptualization of risk factors
Risk factors are conceptualized as signaling barriers to implementing a good life plan and addressed accordingly. Important to note is that while the authors advocate assessing risk factors, we advise against simply taking them at face value as barriers to achieving a good life (see Heffernan et al., 2019; Ward, 2016). Risk factors are best understood as summaries for heterogenous clusters of possible causes, environmental, and mental state factors rather than depicting a specific causes; they are nonspecific, overly general, and lack theoretical coherence (Ward & Beech, 2015), The intent in this item is to consider how risk factors are conceptualized along the path to developing a narrative understanding of how earlier experiences have shaped the risk factors that have played a role as barriers or obstacles to achieving the primary goods.
Risk factors addressed in treatment are selected from empirical research and identified as relevant to the case based on a formal assessment.
Risk factors are understood as being general barriers to acquiring Good Life goals
Risk factors are understood as processes/narratives (or even “mini-stories”) which have occurred and may occur in the future if one is experiencing challenges to their good life plan.
Risk factors are broken down into the particular set of causal, contextual, and experiential (mental state) elements relevant to the individual being treated.
The clinician adequately balances a focus on risk considerations with strengths/protective factors and Good Life goals such that risk factors do not receive undue attention from one session to the next.
Assign a rating as follows:
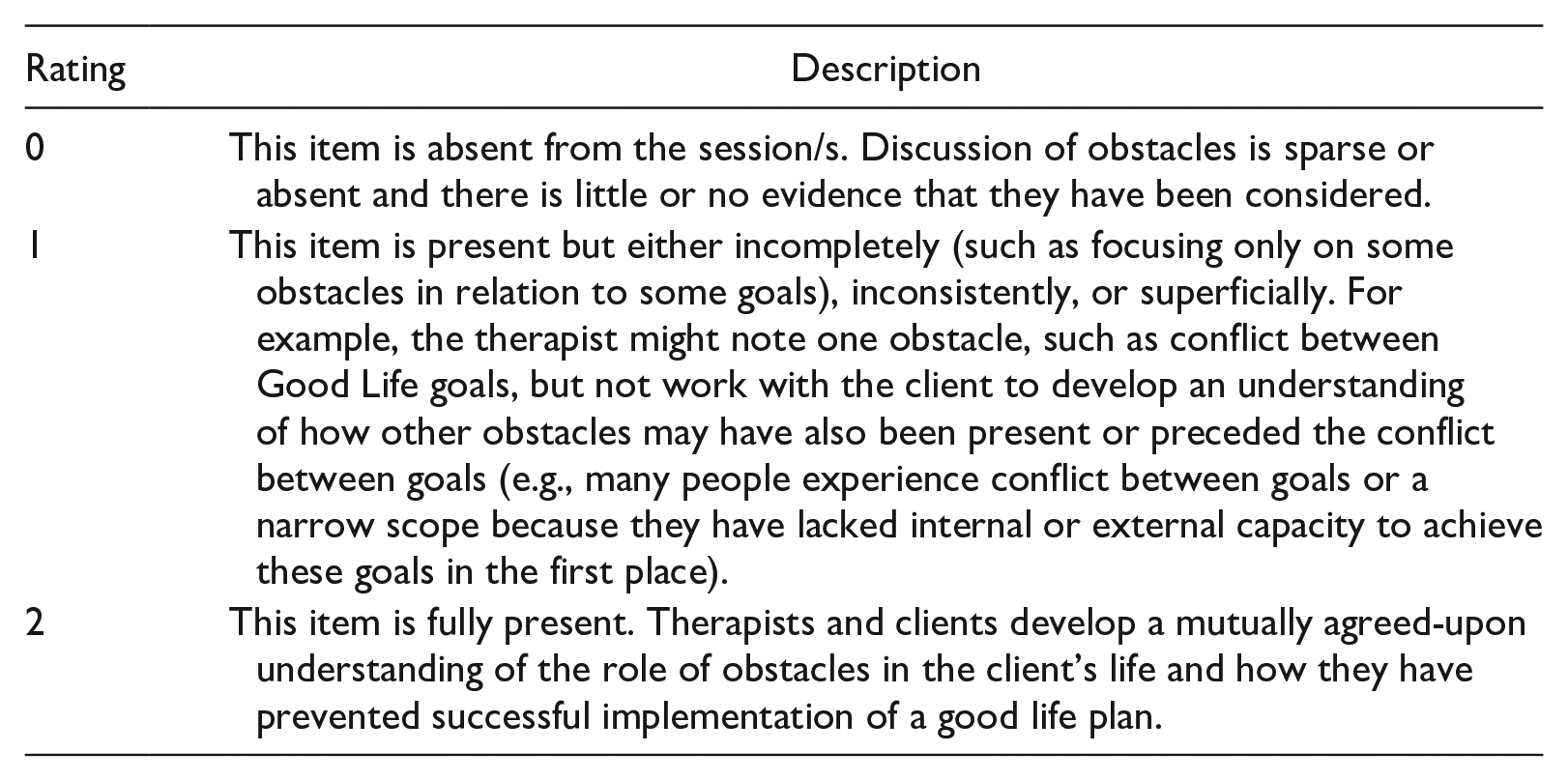
Obstacles to achieving one’s good life plan
This item is concerned with developing a shared understanding of which obstacles have obstructed prosocial attainment of primary goods. Without an understanding of the obstacles that have undermined a person’s attempt to live a fulfilling and prosocial life it is difficult for them to see the point of treatment, and also, to actively engage in the process of change. The GLM outlines the following obstacles (also referred to as good life plan flaws):
Maladaptive means to achieve primary goods.
Lack of internal capacity (e.g., lack of social skills or knowledge as a result of early adversity, mental health conditions, learning disabilities).
Lack of external capacity (i.e., environmental circumstances that interfere with implementing a good life plan, like having a reputation as having abused someone and/or lacking opportunities for prosocial attainment of primary goods).
A narrow scope to one’s good life plan (focusing on too few areas).
Conflict between Good Life goals (when working to achieve one goal interferes with achieving another goal).
Assign a rating as follows:
Section 3: Client-Focused GLM Considerations
Questions provided in this section are included for the purpose of reflection and are not rated. They are included to help facilitate communication between observer/supervisor and the therapist to support ongoing GLM implementation. We encourage consideration of the extent to which each question can be answered, for each client:
What primary goods have been important to the client in the past? Which was the most important and how did it contribute to the sense of meaning and personal identity?
What primary goods are important to the client currently? Which was most important how did it contribute to the sense of meaning and personal identity?
How have traumatic and otherwise adverse events created obstacles to this client’s ability to achieve their good life goals more effectively?
How have traumatic and otherwise adverse events contributed to the development of risk factors (that acted as barriers to achieving their good life goals?)
What will progress in implementing a good life plan look like to the client and others?
What can the client and therapist do to make positive changes in implementing a good life plan? How does then plan align with the individual’s most highly prioritized good and subsequent sense of meaning?
What challenges might arise as the client seeks to implement their good life plan? What would living a better life look like to the person?
What warning signs might appear when things are going wrong? How would the client know when things aren’t improving? How would others know when things aren’t improving?
What can the client do when things start to go wrong? Do they go back to their good lives plan and reflect on how best to get things back on track? What can others do when things start to go wrong?
How can the client and others acknowledge progress when it happens? Does their good lives plan contain a series of gradual, achievable steps that lead to the kind of life they wish to achieve?
Discussion and Conclusion
In the authors’ experience, it is common for professionals who have little experience with the GLM to look at some of its key elements and assume that their practice is similar to the GLM. They therefore assume that they don’t need to study the model closely or adapt their practice to claim adherence to the GLM. Yet clinicians often describe their work as GLM-consistent when many elements are not (Willis et al., 2014). The intention of the current paper is to provide a tool for supervisors and therapists to monitor therapist fidelity to the GLM. Low ratings in Sections 1 and 2 and difficulties answering questions in Section 3 may highlight areas for ongoing professional development, either through clinical supervision or further training in the GLM.
The GLM Fidelity Monitoring Tool represents an initial attempt to operationalize and quantify what is meant by GLM-consistent treatment, especially Section 2. With further refinement, the tool has potential for use as a research instrument to systematically measure therapist and/or treatment fidelity to the GLM, allowing examination of whether greater fidelity improves client outcomes. Indeed, the extent to which the GLM adds value to principles of effective correctional interventions remains largely unknown. In a recent systematic review, Mallion et al. (2020) identified just five studies examining outcomes of programs meeting their criteria for a GLM consistent program. Their criteria included: (i) assessment of the client’s valued primary human goods, (ii) identification of internal and external obstacles to goods attainment through prosocial means, (iii) development of a good life plan (GLP), and (iv) use of the GLP to guide treatment. Compared to relapse prevention oriented programs, they found that GLM consistent programs were equally effective in terms of pre-post measures of psychometric change and associated with increased client motivation and engagement.
The GLM Fidelity Monitoring Tool provides a foundation from which to develop a structured measure of treatment fidelity to the GLM, which would facilitate future research examining treatment effectiveness as a function of fidelity to the GLM. In its current form, the GLM Fidelity Monitoring Tool has clinical utility, but is in the early stages of development as a fidelity measure. Although grounded in empirical research and GLM theory, and structured in accordance with other measures (e.g., Moyers et al., 2014), it is not yet known whether data produced will demonstrate interrater reliability—a necessary pre-requisite before using the tool to measure fidelity to the GLM in future research. We acknowledge that the 3-point rating scale used in Sections 1 and 2 is narrow, which was intentional given the intended (clinical) use of the tool. In addition, the tool focuses on broad considerations especially with respect to case conceptualization and the focus of treatment sessions. Additional considerations include supporting generalization of a GLP outside of therapy sessions through attending to the client’s current context (and proposed future context, if the client is in a secure setting with the possibility of release). Such considerations include engaging the client’s personal and/or professional support network (including supervising officer) in joint sessions to allow space for them to develop an understanding of the client’s GLP and discuss how they can best support a client implement their GLP. Future research implications therefore include (i) considering expanding the focus of the GLM Fidelity Monitoring Tool, (ii) considering expanding the rating scale to capture greater variance in fidelity ratings, and (iii) examining interrater reliability of a revised tool through multiple observers conducting independent ratings.
Ultimately, we hope that the GLM Fidelity Monitoring Tool inspires future research across diverse settings and cultural groups. With the proliferation of programs seeking to implement the GLM comes the need to consider many perspectives on its successful application. At a minimum, the GLM Fidelity Monitoring Tool enables users to examine their alignment with broader elements of the GLM as well as the processes within it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.