
Abstract
This study examined differences between youth who engaged in intrafamilial (ISAB) and extrafamilial sexually abusive behavior (ESAB) on various characteristics covering the sociodemographic, offense-related, psychological, and environmental domains. A total of 85 Dutch male youth participated in this study. Information was obtained through self-report questionnaires and systematic screening of the case files. Youth who engaged in ISAB, compared with ESAB, came from larger families, were enrolled in higher levels of secondary education and started sexual offending at a younger age. Youth who engaged in ESAB were more frequently diagnosed with attention-deficit hyperactivity disorder (ADHD) and intellectual disabilities (ID) and primarily received longer treatment in the context of residential care. The findings are discussed in connection to the literature on (adult) sexual offending. The risk factors and criminogenic needs that distinguish youth who engaged in ISAB and ESAB appear different from those found in adult populations.
Keywords
Sexual abuse victimization is a global problem (Barth et al., 2013; Stoltenborgh et al., 2011) which poses a substantial burden on victims’ health and social participation (Edwards et al., 2003; Van Vugt et al., 2014; Van Vugt et al., 2017). Therefore, research on sexual offending is vital to inform public and mental health policies to prevent sexual offenses and treat perpetrators of sexual abuse in an attempt to reduce recidivism (Andrews & Bonta, 2006). Despite tremendous research efforts carried out to better understand factors that contribute to the onset and persistence of sexually abusive behavior (Van den Berg et al., 2017), heterogeneity within the sex offender population continues to complicate the assessment of risk factors and criminogenic needs, in turn hindering the development of effective treatments (Andrews & Bonta, 2006; Becker, 1998; Hendriks, 2006; Knight & Prentky, 1993; Zimring, 2009).
Generally, sexually abusive behavior committed by youth accounts for only a small proportion of all sexual offenses (Warner & Bartels, 2015). For instance, in 2018, the Netherlands counted 320 suspects of sexually abusive behavior under the age of 18. This number comprises approximately one eight of the total number of sexual offense charges that year. In contrast, 40% of the suspects involved adults between the ages of 25 and 45 (Central Bureau of Statistics, 2018). This may explain why the clinical practice, while intervening with juveniles, has continued to rely on assessment and treatment models based on the knowledge and experience gained from working with adult sex offenders (Eastman, 2004; Veneziano & Veneziano, 2002; Zimring, 2009). Nevertheless, this may overlook the fact that sexually abusive behavior among juveniles has different correlates and predictors than sex offending behavior among adults (Lussier et al., 2015). Thus, conducting research focused specifically on youth is imperative to broaden the evidence base available to devise treatments that are appropriate to youth instead of blindly applying interventions based on knowledge gained in adult samples.
In addition to this debate, a number of scholars have stated that there is much heterogeneity among youth who engage in sexually abusive behavior (Hendriks, 2006) and that more research is needed to gain insight into the characteristics of specific subgroups, as is also done among adult sexual offenders (Seto et al., 2015). Paralleling the tradition of studies on adult sexual offenders, the two most widely used categorizations among youth who engage in sexually abusive behavior are based on (a) the victim’s age, distinguishing between child and peer abusers and (b) the relationship with the victim (Joyal et al., 2016), distinguishing between offenders with intrafamilial and extrafamilial victims.
Studies that have used the victim’s age as a categorization found little differences between the groups (Fanniff & Kolko, 2012; Van Vugt et al., 2011; Zeng et al., 2015). This suggests that this categorization may not have sufficient clinical relevance and be unnecessarily less parsimonious than considering youth who engaged in sexually abusive behavior as one group, regardless of their victims’ age. Comparatively, a few studies have examined whether a different type of categorization, such as the one on the relationship with the victim, may provide a more nuanced view of different subgroups of youth who engage in sexually abusive behavior (Joyal et al., 2016). Arguably, this distinction may have relevant implications for risk assessment and practice. First, because these two subgroups of youth are likely to pose risk in different environmental contexts (i.e., family vs the broader community). Second, because it is possible that engaging in sexually abusive behavior against close others as opposed to people that are not related to the perpetrator may be due to different underlying psychological mechanisms (e.g., more substantial empathy deficits may be needed to abuse people who are close to us).
Despite a wealth of research comparing adults who engage in intrafamilial (ISAB) and extrafamilial sexually abusive behavior (ESAB) (e.g., Seto et al., 2015), fewer studies examined these differences in youth. Furthermore, the results of these studies are often difficult to interpret for a number of reasons. First, some studies only describe the characteristics of one subgroup, mainly youth who engaged in ISAB, without including a comparison group (Grant et al., 2009; Thornton et al., 2008). Other studies used a narrower definition of ISAB including only sibling abusers and excluded other familial sexual abuse such as victimization of cousins (Latzman et al., 2011; Worling, 1995). A number of studies have shown that sibling offenders, in comparison with nonsibling offenders, experience more family dysfunction among which sexual and physical abuse, family violence, and exposure to pornography. In addition, families of sibling offenders generally tended to be larger and had more children who were placed in out-of-home care (Latzman et al., 2011; Tidefors et al., 2010; Worling, 1995). The question arises whether these differences remain when including youth with extended family victims, as they represent a less selective group, and one that is more often found in naturalistic settings (e.g., treatment institutions).
To our knowledge, only a few studies examined youth who engaged in ISAB (with a sibling or extended family victim) by contrasting them with youth who engaged in ESAB. These studies have alternatively focused on differences in individual characteristics, sociodemographic factors, environmental factors, offense-related characteristics, or a combination of these. To date, no significant differences between groups were found with regard to the age of the offender (Fischer & McDonald, 1998), ethnicity, and criminal history of the caregivers (Perez, 2017). However, youth who engaged in ISAB did often experience more child sexual abuse and had higher cognitive capacities than youth who engaged in ESAB. Furthermore, youth who engaged in ESAB, in contrast to ISAB, tended to have a larger criminal history (Perez, 2017). These results are partly in line with studies on adult offenders with intrafamilial or extrafamilial victims. For instance, a recent meta-analysis by Seto et al. (2015) found that adults who engaged in ISAB, in contrast to ESAB, had experienced more child sexual abuse and other forms of child maltreatment, and were more poorly attached to their parents. Subsequently, this meta-analysis showed that adult offenders engaging in ISAB displayed lower levels of cognitive distortions and fewer interpersonal problems. Overall, it appears that there are more differences between adults than juveniles who engaged in ISAB or ESAB. However, research on youth who engaged in sexually abusive behavior that has compared these two groups is still too sparse to draw conclusions. In contrast, the relatively richer literature on adults who engage in either ISAB or ESAB constitutes only indirect evidence for research on youth, given the little overlap between the two populations they are drawn from. That said, it is unlikely that a sample of adults who engaged in ISAB or ESAB is representative of youth samples with the only differences being due to aging and changing social roles.
This study aimed at replicating and extending previous knowledge in this area, comparing youth engaging in ISAB and ESAB on a wider array of risk and needs factors. In an attempt to spur more research in this area, and due to the paucity of studies in this area, we elected to include a wide range of characteristics across different domains and investigated them in a largely exploratory fashion. Specifically, based on the literature reviewed above and on clinical wisdom, we identified potentially relevant factors in the following domains: (a) individual sociodemographic characteristics (i.e., level of education, ethnicity); (b) individual psychological characteristics (i.e., empathy, implicit theories), including psychopathology and other noncriminogenic needs (i.e., internalizing and externalizing symptoms, intellectual disabilities [ID] autism spectrum disorder [ASD] and attention-deficit and hyperactivity disorder [ADHD]); (c) offense-related characteristics (i.e., non-sexual delinquency, age at first offense, age of youngest victim, gender of victim, treatment type and duration); and (d) environmental factors (i.e., family factors, maltreatment experiences, peer relationships).
Based on previous studies, we expected that youth who engaged in ISAB would report more child maltreatment than those who engaged in ESAB (Latzman et al., 2011; Perez, 2017; Worling, 1995). In addition, we expected youth who engaged in ISAB to belong to larger families and report greater family dysfunction (Latzman et al., 2011; Tidefors et al., 2010; Worling, 1995). In contrast, we expected youth who engaged in ESAB to have greater cognitive impairments and cognitive distortions (i.e., implicit theories) (Perez, 2017; Seto et al., 2015). Due to the paucity of previous studies and theories on youth who engaged in either ISAB or ESAB, our hypotheses concerning the other factors were largely exploratory.
Method
Participants
A total of N = 85 Dutch males from three juvenile correctional facilities and six offices of a forensic outpatient treatment center participated in this study. The male adolescents had a mean age of M = 17.54 (SD = 2.22) ranging between 13 and 23 years of age at the time of assessment. A number of questionnaires were completed by the youth in individual sessions under the supervision of a trained assistant. Subsequently, the case files of the youth, which contained psychological and psychiatric evaluations, judicial information, and treatment reports, were systematically reviewed by a group of trained assistants following an extensive coding schema (see for an explanation of the coding schema: Hendriks, 2006). The inter-rater reliability of the coding is not available. However, the assistants worked in pairs at the same location and coded approximately five case files simultaneously. Afterward, the coding of the files was compared and differences in coding were resolved through discussion until agreement was obtained. All case files had information about the index sexual offense for which treatment was demanded. Apart from the index offense, information was coded for up to three most recent sexual offenses. No information was available in case more sexual offenses had been committed.
Based on the case files, it was established that n = 26 (30.6%) youth committed uniquely intrafamilial sexual abuse, indicating they abused a member of the core or extended family. Thirty-nine juveniles (45.9%) committed uniquely extrafamilial sexual abuse, referring to abuse outside the family context, for example, at school and/or in the neighborhood. Twelve juveniles (14.1%) committed both intrafamilial and extrafamilial offenses and were therefore excluded from the analyses. Information about the nature of the offense was missing for eight juveniles (9.4%). These cases were also excluded from all analyses.
Procedure
All respondents signed a consent form to declare that they voluntarily participated in this study and allowed researchers to analyze their psychological and criminal records. In case the youth had not yet reached the age of 16 years, a caregiver or guardian was asked to co-sign the consent form. From age 16 and on, youth are allowed to give their independent consent in the Netherlands. It was explained to the respondents that withdrawal from the study did not have any consequences for their treatment (evaluation) or detention situation. All information was anonymized and stored safely in line with procedures of the local university Ethics Review Board. Participants received a small reward of €5 for their collaboration.
Instruments
Cognitive and affective empathy
The basic empathy scale (BES) was used to examine cognitive and affective empathy, respectively—the cognitive ability to recognize someone else’s emotional state and the affective ability to sympathize with and share the other person’s emotional state (Cohen & Strayer, 1996; Jolliffe & Farrington, 2004). The BES contains 11 affective empathy items and nine cognitive empathy items. All items had to be responded to on a 5-point Likert-type scale, ranging from (1) strongly disagree to (5) strongly agree. The items of the BES are based on four basic universal emotions, respectively: fear, sadness, anger, and happiness. An example of an affective and cognitive empathy item is, “I get caught up in other people’s feelings easily” and “I can often understand how people are feeling even before they tell me.” The BES was translated into Dutch and validated for use in The Netherlands in a study by Van Langen et al. (2009), who replicated the positive validation results of the original validation study by Jolliffe and Farrington (2006). In this study, we found internal consistency reliability coefficients of α = .68 for affective empathy and α = .67 for cognitive empathy.
Implicit theories
Implicit theories were measured with the Sex With CHildren (SWCH) scale, an instrument that is used in both prison and community settings in the United Kingdom. Mann et al. (2007) acknowledge that offenders who identify themselves with the beliefs that are measured with the SWCH are more likely to generate distorted statements about their own abuse victim(s). The SWCH was translated into Dutch and adapted for the use among youth. The SWCH consists of 18 items, which are responded to on a 5-point Likert-type scale ranging from (1) strongly disagree to (5) strongly agree. For the purpose of this study, the total scale score was used. An example of an item is, “Having sex with a child is not really all that bad because it doesn’t really harm the child.” Higher scores on the SWCH indicate stronger beliefs that justify sexual contact with children. Cronbach’s alpha for our sample proved to be excellent (α = .91).
Psychopathology
The Strengths and Difficulties Questionnaire (SDQ) was used to measure psychopathology. The SDQ was originally developed by Goodman (1997) but in this study the Dutch version of Goedhart et al. (2003) was used. This screening questionnaire aims to measure psychological problems in the past 6 months in adolescents. The SDQ consists of the following scales: attention deficit and hyperactivity, emotional problems, problems with peers, behavioral problems, and prosocial behavior. However, research has shown that it is more appropriate to use the internalizing and externalizing problem scales of the SDQ (Goodman et al., 2010). The emotional and peer problem scale constitute the internalizing problem scale (10 items), whereas the attention deficit and hyperactivity scale and the behavioral problem scale form the externalizing problem scale (10 items) (Goodman et al., 2010).
The scores are based on a 3-point Likert-type scale, with the answer options varying from (1) not true to (3) certainly true. An example item of the externalizing problem scale is, “I am constantly wobbling or fidgeting,” whereas an example of an item of the internalizing problem scale is, “I am often unhappy, or sad.” Higher mean scores indicate higher levels of psychopathology. After analyzing the interitem correlation matrices and deleting three items of the internalizing problem scale, the internal reliabilities of the internalizing and externalizing problem scales were, respectively, α = .60 and α = .75.
Nonsexual delinquency
Self-reported nonsexual delinquency was measured with the youth delinquency survey of the Dutch Research and Documentation Centre (WODC). The questionnaire consists of 35 items with descriptions of (nonsexual) delinquent acts which had to be answered with yes or no if they were committed during the past 12 months. The nonsexual delinquency items covered the following areas: internet, public order, violation, theft, violence, white-collar crime, drugs, and possession of weapons (Van der Laan & Blom, 2005). An example of a theft item is, “Have you ever stolen a bike or scooter?” All the “yes” answers on the items were summed and higher scores indicated higher levels of nonsexual delinquency. The internal reliability of the scale proved to be excellent α = .90.
Case files
A number of individual and familial characteristics were based on the information reported in the case files. The characteristics treated in a continuous fashion were as follows: duration of treatment (in 6-month periods), family size, age of the offender at the time of the index offense, and age of the youngest victim (based on all sexual offenses committed). Other characteristics had to be recoded into binomial (yes/no) categories, respectively: level of education, child maltreatment, family violence, parental divorce, school and peer problems, official diagnoses such as intellectual disability (ID), ADHD or ASD, gender of the victim, and type of treatment (outpatient or residential). See the table notes for further explanation of the categories.
Analytic Strategy
Statistical analyses were conducted using SPSS statistics version 20. A number of independent t tests were performed to examine differences between youth who engaged in ISAB and ESAB for the continuous variables. All the categorical variables were analyzed by means of chi-square tests. To facilitate the interpretation of the magnitude of the differences, effect sizes (Cohen’s d) were calculated and presented in the tables, with d = .20 considered a small, d = .50 a medium, and d = .80 a large effect (Cohen, 1988).
Results
With regard to the individual sociodemographic characteristics (see Table 1), no significant differences were found between youth who engaged in ISAB and ESAB in ethnicity, differentiating between native and non-native Dutch. However, significant differences were found for level of education. Youth who engaged in ISAB were enrolled in higher levels of secondary education than those who engaged in ESAB.
Comparisons Between Youth Who Engaged in Intrafamilial and Extrafamilial Sexually Abusive Behavior on Sociodemographic Characteristics.
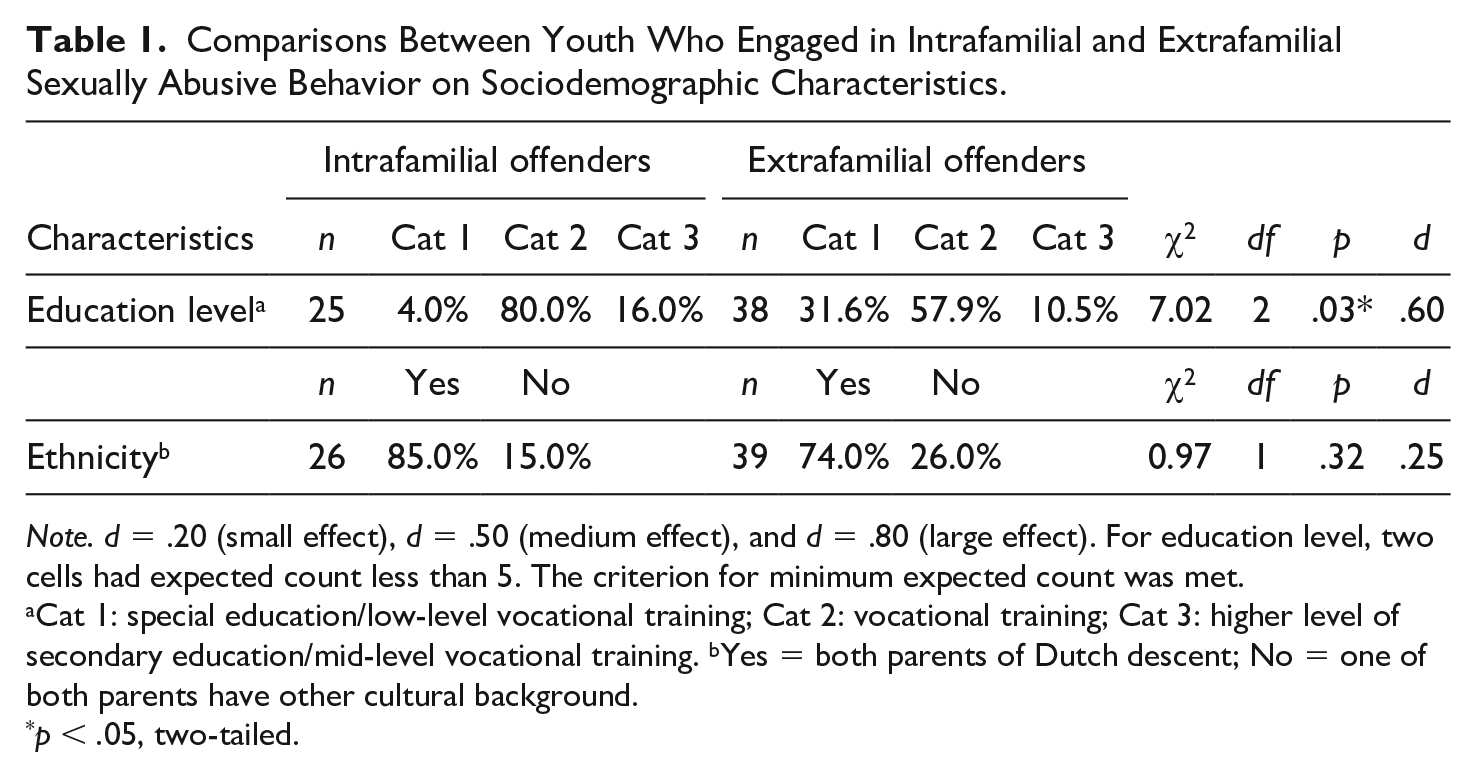
Note. d = .20 (small effect), d = .50 (medium effect), and d = .80 (large effect). For education level, two cells had expected count less than 5. The criterion for minimum expected count was met.
Cat 1: special education/low-level vocational training; Cat 2: vocational training; Cat 3: higher level of secondary education/mid-level vocational training. bYes = both parents of Dutch descent; No = one of both parents have other cultural background.
p < .05, two-tailed.
Regarding the offense-related characteristics (Table 2), age at first offense rendered a significant difference. Youth who engaged in ISAB, compared with youth who engaged in ESAB, were younger at the time of their first offense. The age of the youngest victim did not differ between youth who engaged in ISAB and ESAB. Notably, both groups had abused mostly prepubertal children. In addition, there were no differences between groups in the proportion of youth with female, male, or mixed-gender victims. Furthermore, both groups committed equal numbers of nonsexual delinquency, with an average of six offenses committed by each group. Finally, it was found that youth who committed ESAB received longer treatment than those who committed ISAB. In line with this result, we also found a significant effect for type of treatment. Youth who engaged in ESAB frequently received (judicial) residential treatment, whereas youth who engaged in ISAB were more often referred to outpatient treatment clinics.
Comparisons Between Youth Who Engaged in Intrafamilial and Extrafamilial Sexually Abusive Behavior on Offense-Related Characteristics.
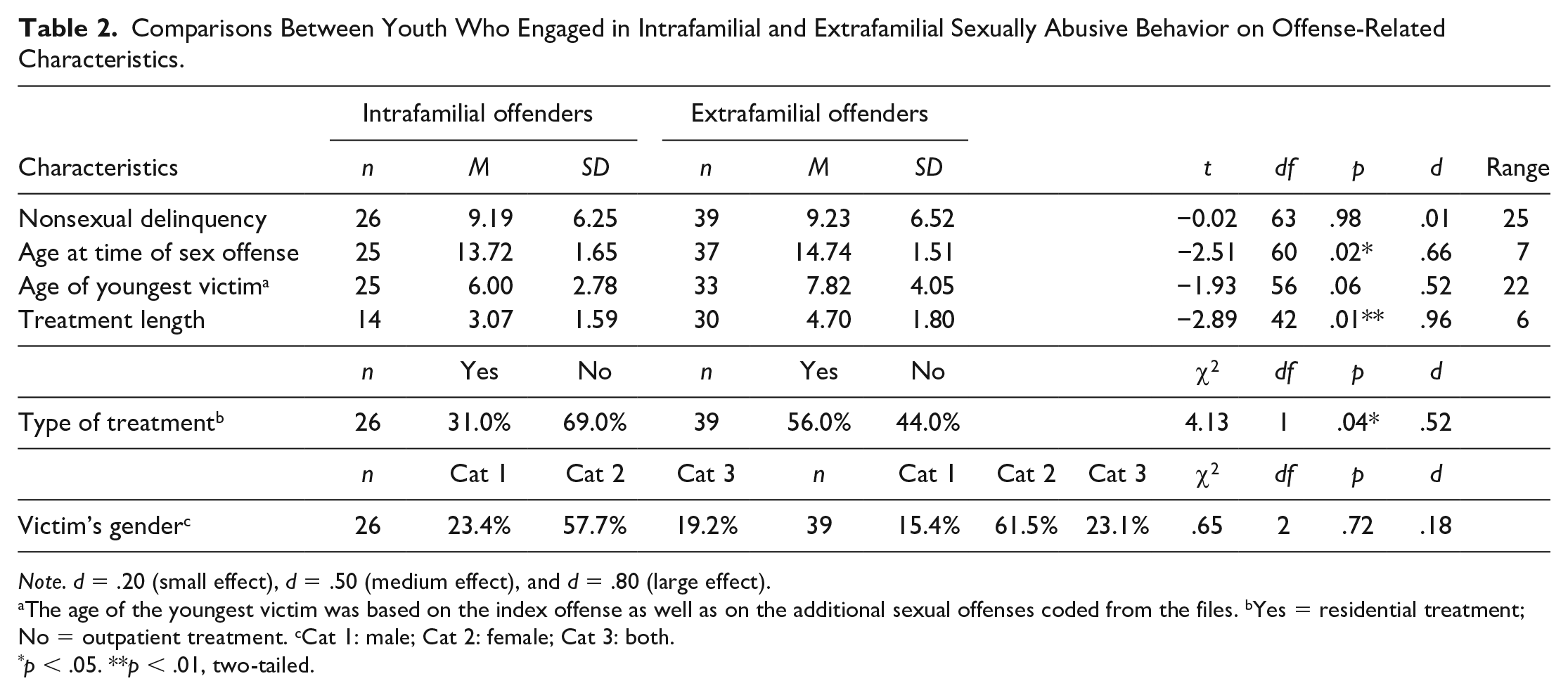
Note. d = .20 (small effect), d = .50 (medium effect), and d = .80 (large effect).
The age of the youngest victim was based on the index offense as well as on the additional sexual offenses coded from the files. bYes = residential treatment; No = outpatient treatment. cCat 1: male; Cat 2: female; Cat 3: both.
p < .05. **p < .01, two-tailed.
With regard to the individual psychological characteristics (Table 3), youth who committed either ISAB or ESAB reported similar levels of cognitive and affective empathy as well as cognitive distortions (implicit theories). In addition, in terms of psychopathology and noncriminogenic needs, similar levels of internalizing and externalizing problems were reported between the groups. Furthermore, ASD was equally present among the youth. The only significant differences in this domain were found for (borderline) ID and ADHD. Youth who engaged in ESAB, compared with ISAB, were more frequently diagnosed with (borderline) ID and ADHD.
Comparisons Between Youth Who Engaged in Intrafamilial and Extrafamilial Sexually Abusive Behavior on Individual Psychological Characteristics.
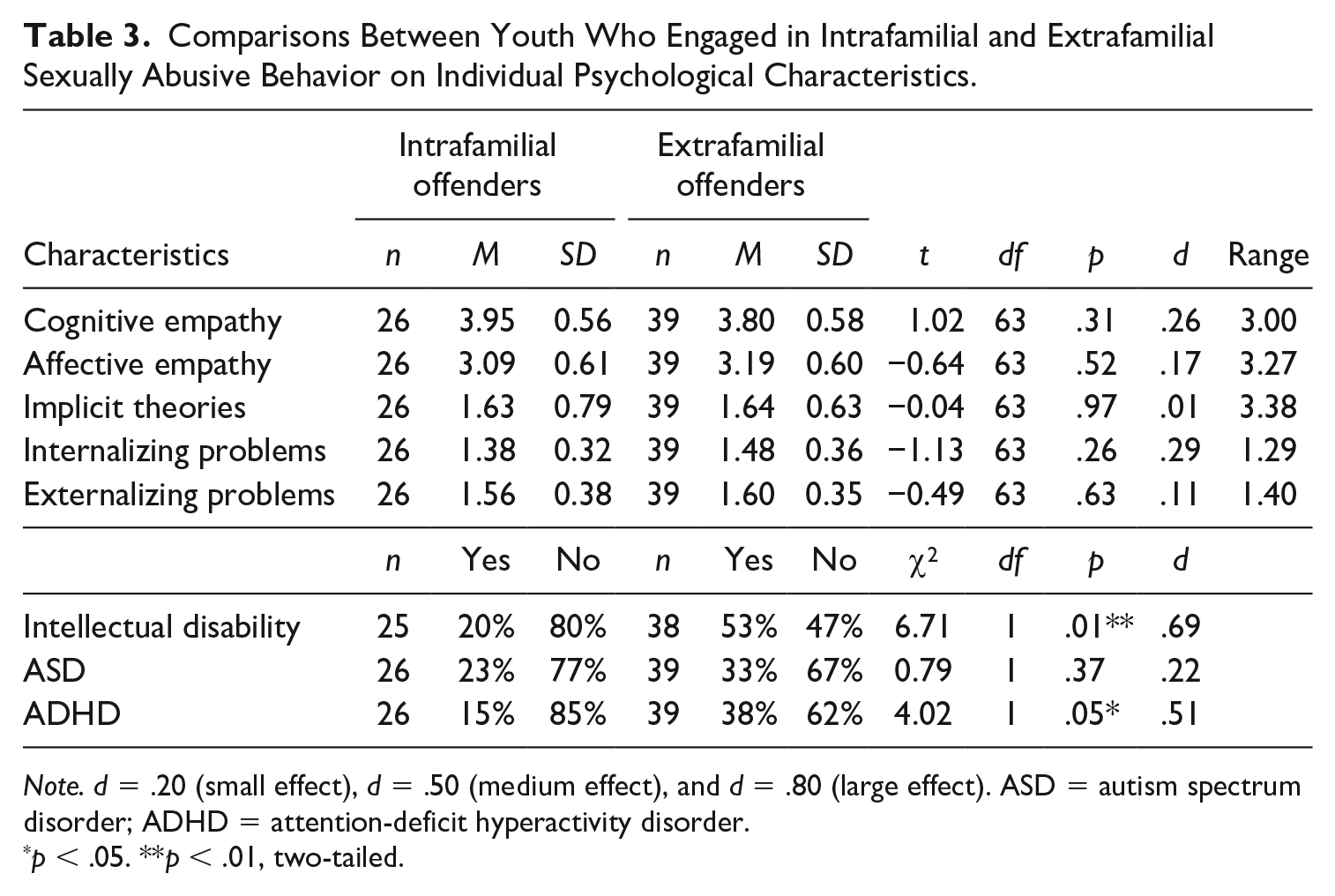
Note. d = .20 (small effect), d = .50 (medium effect), and d = .80 (large effect). ASD = autism spectrum disorder; ADHD = attention-deficit hyperactivity disorder.
p < .05. **p < .01, two-tailed.
Regarding the environmental characteristics (Table 4), there were no significant differences between the groups for physical and emotional abuse, physical and emotional neglect, and sexual abuse victimization. In addition, similar percentages of parental divorce and family violence were reported among the youth. Furthermore, there were no differences between groups regarding the quality of peer contact and being bullied at school. More specifically, the majority of the youth in the ISAB and ESAB group were bullied at school and had poor peer contacts. The only significant difference within the environmental domain was family size. Youth with intrafamilial victims came from larger families than those with extrafamilial victims.
Comparisons Between Youth Who Engaged in Intrafamilial and Extrafamilial Sexually Abusive Behavior on Environmental Characteristics.
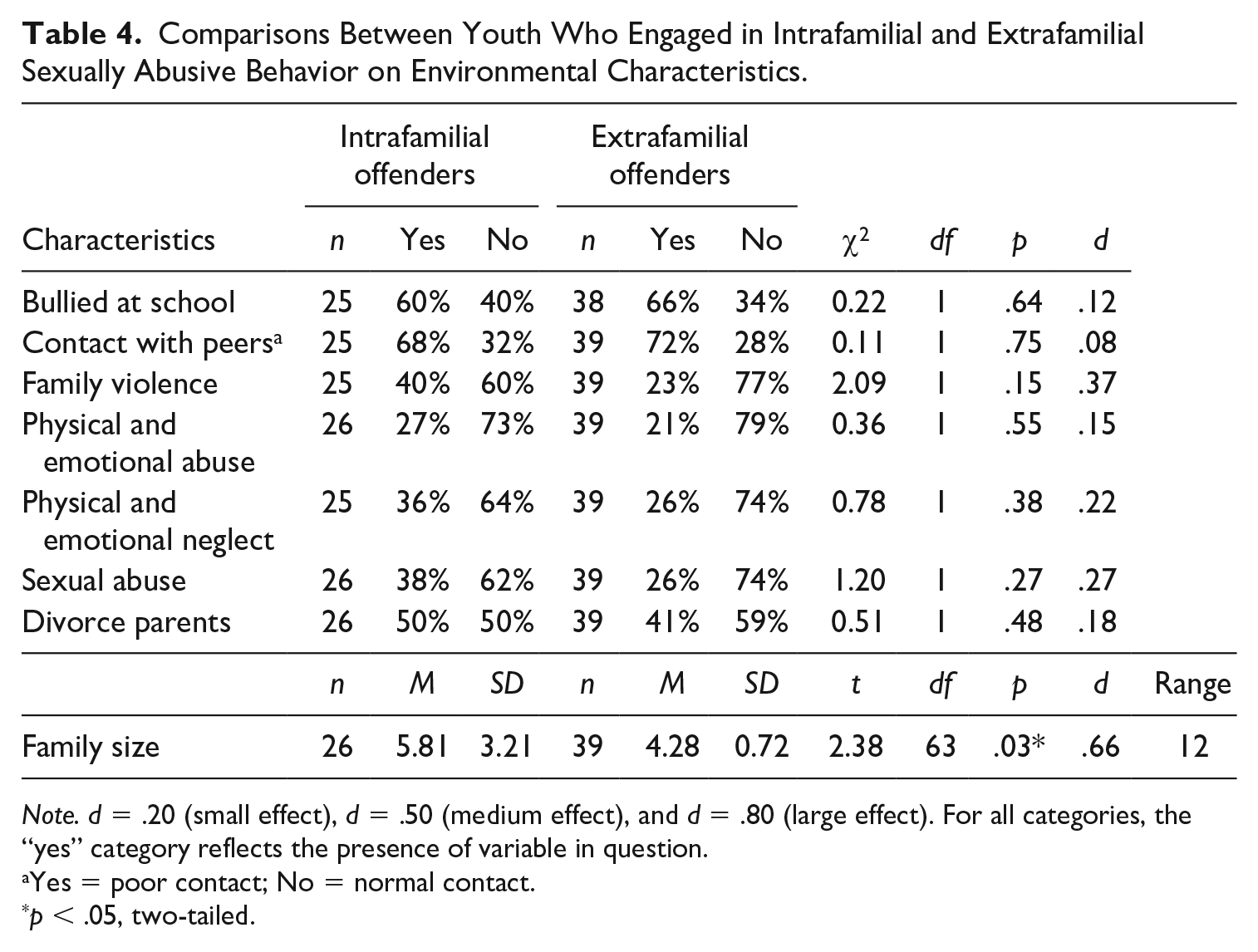
Note. d = .20 (small effect), d = .50 (medium effect), and d = .80 (large effect). For all categories, the “yes” category reflects the presence of variable in question.
Yes = poor contact; No = normal contact.
p < .05, two-tailed.
Discussion
This study examined differences between youth who engaged in ISAB or ESAB by focusing on a number of characteristics covering sociodemographic, offense-related, psychological, and environmental factors. By and large, our findings suggest that there are more similarities than differences between these two groups. Yet, some notable differences occurred and were associated with moderated effect sizes. It was found that youth who engaged in ISAB, compared with ESAB, came from larger families, were enrolled in higher levels of secondary education, and had a younger age at the time of their first offense. In contrast, youth who engaged in ESAB were more likely to be diagnosed with ADHD and ID. Last, youth who engaged in ESAB were more often referred to residential treatment and tended to receive longer treatment. No significant differences between groups were found for a number of psychological and psychiatric problems among which for internalizing and externalizing problems, cognitive distortions, cognitive and affective empathy, and ASD. Furthermore, no significant differences were found for nonsexual delinquency and characteristics in the environmental domain including family violence, parental divorce, child maltreatment, peer contact, and being a victim of bullying at school.
Although the results need to be interpreted with caution, this study seems to suggest that youth with intrafamilial and extrafamilial abuse victims might show more similarities than differences where it concerns psychological and environmental characteristics as well as nonsexual delinquency. Similarly, in line with previous findings (e.g., Wolfe, 2007), there were no significant differences between the two groups in having male, female, or mixed-gender victims. Thus, it appears that whether youth who engage in sexually abusive behavior choose male or female victims is not related to their tendency to engage in either ISAB or ESAB.
With regard to individual psychological characteristics, no significant differences between the groups were found for the level of empathy and cognitive distortions. Furthermore, in the psychopathology domain, no differences were found between the two groups for internalizing and externalizing problems. Breuk et al. (2007) showed that youth tend to underreport psychopathology when compared with reports from others, such as parents or clinicians. Therefore, this study also included official psychiatric diagnoses as an additional source of information to determine the youth’s mental health.
First, the percentage of juveniles who were diagnosed with ASD was similar among both groups of offenders. More specifically, a quarter of the youth who committed ISAB and one third of the youth who committed ESAB were diagnosed with ASD. ‘t Hart-Kerkhoffs et al. (2009) showed in their study on sexually abusive behavior among juveniles an overrepresentation of ASD symptoms when compared with a healthy control group. As one of the core symptoms of ASD is problems in social interaction, this may also explain the nonsignificant findings between the groups where it concerned the quality of their peer interactions. Based on official reports from treatment files, more than 60% of the youth had poor peer contacts and bullying experiences.
Second, a higher prevalence of official diagnoses of ID and ADHD was found among youth who committed ESAB compared with youth who committed ISAB. It should be emphasized that high comorbidity between ADHD and ID has been documented (Mayes et al., 2000). For instance, Simonoff et al. (2007) showed that ADHD symptoms are increased in adolescents with mild ID. Similar results were found for a group of adult offenders with intellectual disabilities, for which ADHD was found to be the most prevalent psychiatric disorder (Lindsay et al., 2013). Taken together, given the psychiatric profile of the youth with extrafamilial victims in our sample, characterized by poorer cognitive abilities and higher levels of attention deficits, hyperactivity, and impulsivity, this may explain why this group generally received longer treatment and were more often institutionalized. However, these aspects do not necessarily represent specific risk factors for sexually abusive behavior and may in part be construed as responsivity characteristics. Accordingly, Lindsay et al. (2010, 2013) found that those with ADHD were more likely to be in secure settings compared with those without ADHD. This possibility is not only due to the links between ADHD, ID, and offending or recidivism. Rather, it may also due to the fact that—at least in the Dutch context where the study was conducted—youth whose risk profile may warrant more intensive treatment (including those with ADHD and ID) are generally referred to residential treatment as these institutions have more means to deliver a range of different interventions. In addition, youth who are placed in residential settings often have less protective factors in their familial context.
In line with the ID diagnosis being more prevalent among youth who engaged in ESAB, these youth were also more frequently enrolled in lower levels of education. More specifically, 31% of youth who engaged in ESAB, compared with 7% of the youth who engaged in ISAB, were enrolled in special education and practical training. In line with our study, Perez (2017) showed that youth who engaged in ISAB exhibited higher IQ scores than those who engaged in ESAB.
As individuals with ID often lack the skills to adequately interact with peers, they tend to start friendships with younger children. As a consequence, this may increase the risk to experiment sexual behavior with younger children (Briggs, 2006; Danielsson et al., 2010). Day (1994) concluded that sexually abusive behavior among individuals with ID could be perceived in the light of trying to fulfill normal sexual impulses and desires in a context of poor adaptive behavior, social naiveté, and lack of social skills. In this case, ESAB could possibly be explained from a deficit model, whereas ISAB perpetration may be better understood from a deviancy perspective. Accordingly, adults who engaged in ESAB showed poorer interpersonal and social functioning compared with those who engaged in ISAB (Seto et al., 2015). Therefore, assessment and treatment of youth who engaged in sexually abusive behavior with ID should focus on enhancing interpersonal skills and sexual knowledge (Claire, 1993). Promising results have been found for the treatment of adults and youth with ID who engaged in sexually abusive behavior with regard to improving social skills, elimination of cognitive distortions, as well as enhancing sexual knowledge (Heaton & Murphy, 2013; Murphy et al., 2007, 2010; Patterson, 2018).
In terms of environmental characteristics, the finding that youth who engaged in ISAB tend to come from larger families is in line with previous findings based on sibling abuse (Latzman et al., 2011; Tidefors et al., 2010; Worling, 1995). However, this finding needs to be interpreted with caution as the result may be caused by other interacting factors such as poor parenting skills, inadequate supervision, poverty, and parental criminality (Brownfield & Sorenson, 1994; Farrington, 2010).
Apart from family size, no other differences were found in the environmental domain including family functioning. However, it should be noted that family dysfunction was highly prevalent among both groups with about a quarter of the youth who committed ESAB having experienced family violence, and/or child maltreatment including sexual abuse. These percentages were equally high for youth who engaged in ISAB with up to 40% of these juveniles having reports of sexual abuse and family violence. Similarly, O’Brien (1991) showed that family dysfunction is an important risk factor for all youth who engage in sexually abusive behavior, and not only for those with intrafamilial victims. This result is however in contrast with findings from a recent meta-analysis on adults who engaged in sexually abusive behavior, in which those with intrafamilial victims were more often exposed to sexual abuse and other forms of child abuse and neglect than those with extrafamilial victims (Seto et al., 2015). Possibly, family dysfunction is a unique general risk factor in the development of juvenile sexually abusive behavior, whereas it is a specific risk factor for sexually abusive behavior against family members in adulthood (O’Brien, 1991; Righthand & Welch, 2001; Seto et al., 2015).
Some limitations of this study should be mentioned. First, the subgroups of offenders were relatively small which may have resulted in a lack of power to detect differences with small effect sizes and allowed for type 1 errors to occur. Furthermore, it was not possible to match both offender groups on background characteristics due to the limited sample size. Nevertheless, this study was unique in its kind given that information was available on the index as well as three other recent sexual offenses. For this reason, it was possible to establish subgroups based on the youth’s profile and to include only those juveniles who uniquely offended within or outside the familial context, hence providing novel findings in this area of investigation that can inform future, highly powered, studies. Second, some of the outcomes were measured by means of self-report or official reports only. In particular, with regard to psychopathology, research has shown that juvenile offenders tend to underreport, and that information from other sources such as parents, teachers, and clinicians are needed (Breuk et al., 2007). In this study, we were able to obtain information on official psychiatric diagnoses to partially undermine this problem. Third, a valuable addition to the present investigation could have been to have information about the total number of offenses committed by the participants, information we did not have access to. Similarly, we did not have enough participants who had committed both ISAB and ESAB or participants who had committed nonsexual offenses to constitute what would be relevant comparison groups. Fourth, some of the measures had relatively low internal consistency and therefore results concerning those scales could have been underestimated.
In sum, this study provided insights into the similarities and differences between youth engaging in ISAB and ESAB. Overall, it appeared that these two offender groups may be more similar than different, in contrast to what is typically reported among adult offenders with intrafamilial and extrafamilial sexual abuse victims. This possible difference between juvenile and adult offenders who engaged in ISAB or ESAB should give us pause when considering to simply apply knowledge obtained on adult offenders to their juvenile counterparts. Nevertheless, some interesting differences emerged in our study. Youth who engage in ESAB were characterized by poorer cognitive functioning and a greater prevalence of ADHD, suggesting a crucial difference in the responsivity profiles of these two subgroups and recommended treatment. In contrast, youth who engaged in ISAB belonged to larger families and tended to offend at a younger age, suggesting that early psychosocial intervention may be vital to preventing sexual offenses perpetrated within the family.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.