
Abstract

ABOVE: An pneumonia porch at the US Army Camp Hospital in Aix-les-Bains, France, during the flu epidemic of 1918-19
Credit: Everett Collection Historical/Alamy
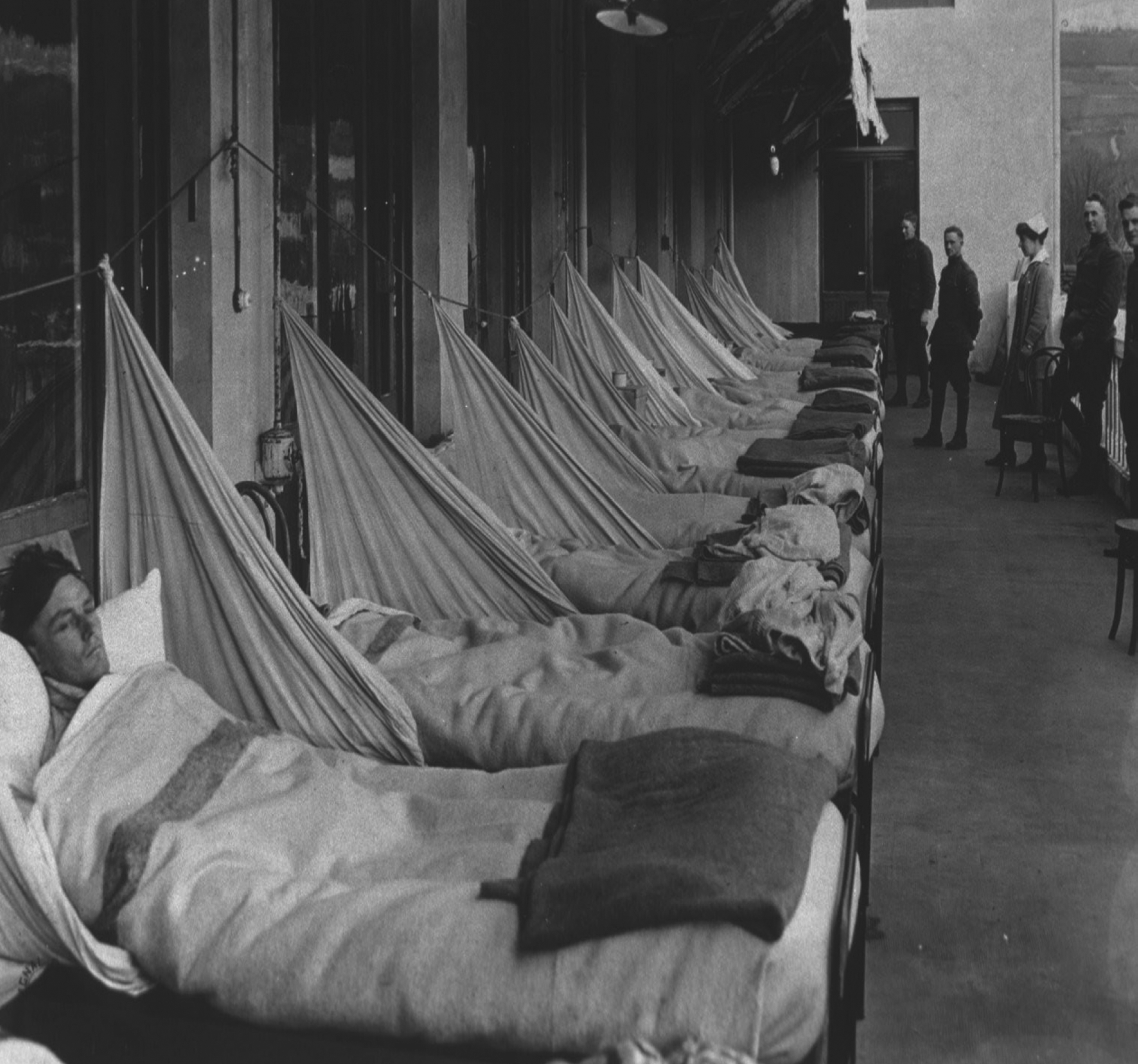
The great influenza pandemic of 1918, at the end of World War I, killed at least 50 million people across the globe, despite huge efforts to contain and control it. But the first reaction of the Allied governments was to shroud it in a cloak of secrecy for fear of sapping morale and hindering troop movements just as the war was reaching a climax.
Even today, with the cloak of secrecy long since lifted, no one knows exactly how or where it started. The great flu pandemic of 1918 was a global holocaust that seems to have arisen spontaneously among the shifting swathes of desperate, debilitated and chronically overcrowded humanity caught up in the maelstrom of World War I.
What we know for sure is that, in the summer and autumn of 1918 and the following spring, the pandemic swept without mercy through the fighting forces of the Western Front, the transit camps and supply routes, and the ports, towns and cities of neighbouring countries. Within a month or two it had reached almost every corner of the globe. We also know that it was the deadliest affliction ever visited upon humanity, killing at least 50 million people worldwide, probably nearer 100 million, several times more than 15-20 million killed by the war itself – and more in a single year than the Black Death killed in a century.
The pandemic came in three waves that merged into one another, differing greatly in severity. The preliminary phase was a scattered series of outbreaks of a prostrating respiratory illness variously called “three-day fever”, “la grippe”, epidemic bronchitis or “lung block”. These outbreaks occurred in military camps as early as December 1916 at Étaples in France and Aldershot in England, culminating in a much more widespread contagion in spring 1918 among the rapidly massing US Army troops in dozens of huge training camps across the eastern United States.
One of the few countries where the press were free to publish news of the flu was Spain, so it was dubbed the “Spanish flu”
As the American war machine built up its two-million-strong force, with many thousands of soldiers crossing the Atlantic every month, pouring into the ports, camps, billets and trenches of France and Flanders, the deadly disease came with them, spreading like wildfire. By early summer 1918 it was already hitting combatants and non-combatants alike in their hundreds of thousands throughout Europe, the US and beyond. India was particularly hard-hit, with as many as 17 million people dying, 5 per cent of the entire population.
Then, in early autumn 1918, just as the worst seemed to be over, a second, far more devastating, wave of influenza was unleashed on a world still reeling from the first onslaught. Somehow, no one knew why, the illness had become even more deadly than it had been in the summer. Case fatality rates had doubled or, in some communities, trebled – so that altogether about one person in every five of those infected perished.
The worst cases triggered bacterial pneumonia, which before the advent of antibiotics was almost invariably fatal. With a raging temperature and gasping for breath, patients appeared to be drowned by a massive accumulation of pus, fluid and blood in their lungs. Their fingers and lips turned blue and their complexion a pallid grey.
Everyone knew someone who had caught the deadly fever, but no one knew exactly what was causing it. Could it be influenza, which had been a regular visitor for centuries? Or was it a novel form of plague? Or perhaps some new typhus? Typical influenza was known to be especially dangerous for frail elderly people, infants and young children, and anyone with a serious medical condition. But this new disease was also devastating for previously healthy young adults who would normally shrug off ordinary influenza after a few days of misery. And unlike influenza, which typically struck in the winter months, this disease was happening in the summer and autumn. What could it be? Why didn’t anyone say? Nobody in authority was even acknowledging its existence.
Most of Europe was subject to wartime censorship, as were belligerent allies overseas such as Australia, New Zealand, South Africa, Canada and the US, with stringent restrictions on what could be reported in newspapers and magazines or published in pamphlets, monographs and books. Blanket rules were applied to suppress key information for fear of providing the enemy with useful intelligence on the state of military readiness and capability, the resilience of the supply chain and morale on the home front. This meant that information on the real severity of the epidemic and details of the numbers and location of cases were not permitted.
One of the few countries where the press was free to publish news of the epidemic was neutral Spain. The unfettered Spanish papers had no hesitation in documenting the horrors and mounting death toll from the respiratory fever they loosely dubbed “influenza”, relishing in particular the near-fatal illness of King Alfonso XIII. It didn’t take long for word to spread that the ghastly new disease felling whole communities across the world must be the infamous “Spanish flu”.
Some historians have asserted that, in Britain, the War Office was so anxious to conceal the true nature and extent of the disease that they deliberately leaned on the government to avoid giving practical information to the public on how best to protect themselves. Other commentators cite evidence to suggest that the real reason for the delay was rather more prosaic: during the first wave of the epidemic in early summer 1918 the Army Medical Services were still at a loss as to exactly what disease they were up against. Pathologists and epidemiologists in all the Allied nations were working round the clock to identify the causative agent and develop a vaccine, but there was no consensus as to which of several candidate bacteria it was. The possibility of a virus being to blame was hardly even considered, so little was known about viruses at the time.
As far as public information was concerned, Sir Arthur Newsholme, chief medical officer to Britain’s public health body, the Local Government Board, refrained from issuing a notice to the civil authorities for the same reason: no one was certain of the diagnosis or what could be done about it.
Meanwhile, in the US, the authorities made similar attempts to hush things up and keep people in the dark regarding the true seriousness of the situation. No national official publicly acknowledged the real risks of the by-then-rampant epidemic. Instead an anxiety-provoking mix of truth, half-truth, distortion and downright lies was promulgated. As California senator Hiram Johnson remarked at the time: “The first casualty when war comes is truth.” The US government’s clumsy efforts to prop up national morale simply had the counter-effect of fostering fear.
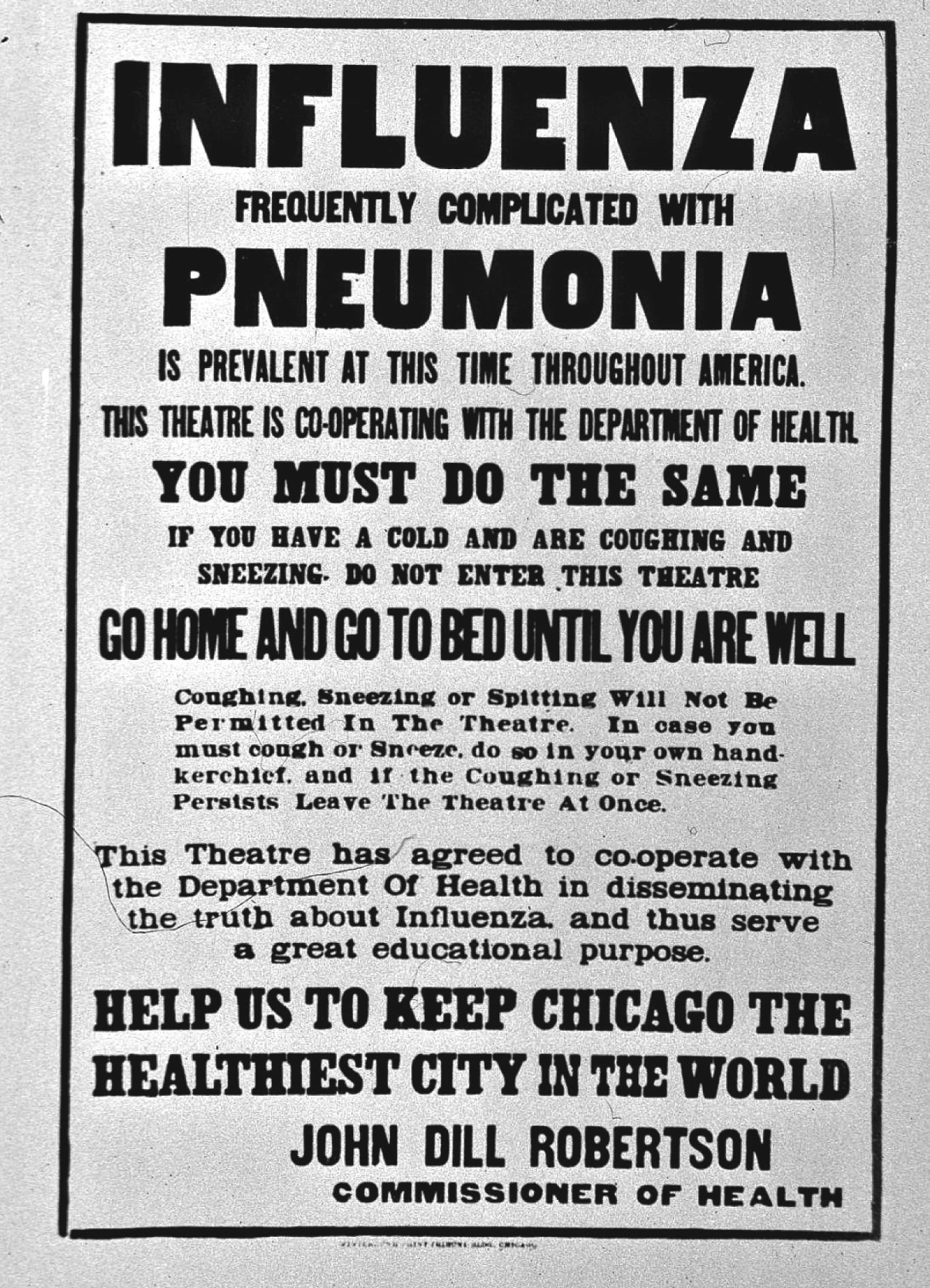
ABOVE: Poster relating to the Spanish Flu epidemic in Chicago in late 1918 when censorship was being relaxed in some states
Credit: Everett Collection/REX
The press echoed this misguided approach by making light of mortality figures and putting a positive spin on the horrendous struggle to save lives. According to historian John M Barry, day after day in hundreds of newspapers the reassurance rang out: “There is no cause for alarm if precautions are observed.”
At Camp Pike, near Little Rock, Arkansas, where 8,000 cases lined the corridors of the hospital over a peak four days and deaths were too many to list, the Arkansas Gazette blithely informed its readers: “Spanish influenza is plain la grippe – same old fever and chills.”
Similarly, whilst hundreds of young conscripts were dying at Camp Dodge just outside Des Moines, Iowa, the city attorney was warning editors and journalists: “I would recommend that if anything is printed in regard to the disease it be confined to simple preventive measures – something constructive rather than destructive.”
In Bronxville, New York, the local paper condemned “alarmism” and intoned that “fear kills more than the disease and the weak and timid often succumb first”. The Chicago Commissioner for Public Health, John Dill Robertson, proudly reported that nothing was done to interfere with the morale of the community: “It is our duty to keep the people from fear. Worry kills more people than the epidemic.” All over the US, newspapers pushed out the same messages: “Don’t Get Scared”, “Don’t Panic”, “Don’t Let Flu Frighten You to Death”.
By early summer 1918 it was already hitting combatants and non-combatants alike in their hundreds of thousands
But not surprisingly the effect of all this reassurance was that people felt they were being kept in the dark. They could see their brothers and sisters, friends and neighbours succumbing to a mysterious and frightening disease, and they not only felt let down by their civic leaders but also all the more terrified of the unknown. The constant “Don’t Get Scared” mantra was fomenting the very panic it was trying to subdue, and causing even more distress and disruption. It also hampered a coordinated civil response, which could have saved many lives.
By the time the armistice came in November 1918, the pandemic was at full spate and utterly unstoppable. Only then and in the months to follow, as censorship was relaxed, was the full horror of what had happened revealed to a world already stunned by four years of total war. And even then, demobilisation, with millions of troops returning home to their towns and villages, together with extreme shortages of food, shelter and medicines across war-torn Europe, meant the lethal pestilence persisted into the new year, with another, smaller, wave of misery and death in the spring of 1919.
Could anything like the great flu pandemic of 1918 happen again? And if so, could people again find themselves left largely in the dark?
There have been a number of viral pandemics since then. In the late 1950s we had “Asian flu”, which came out of China and spread rapidly, hastened by air travel. Altogether it killed about two million people, particularly the frail elderly whose resistance was weak. Just over 10 years later a milder variant dubbed “Hong Kong flu”, spread similarly across the globe.
In the early 1980s the world became aware of a mysterious auto-immune deficiency syndrome (AIDS) which had a predilection initially for gay men and intravenous drug users. The causative virus, HIV, was eventually isolated and its origins traced back via Haiti to west-central Africa. This pandemic is with us still.
In 2003 we saw the alarming outbreak of SARS (severe acute respiratory syndrome), a highly contagious and deadly form of viral pneumonia – again starting in Asia and quickly threatening to engulf the world via air travel. Only rapid action by the World Health Organization (WHO) and national public health authorities managed to contain its spread and prevent a global catastrophe.
And in 2009 the world braced itself for a pandemic of “swine flu”, caused by influenza type A (H1N1), a near-copy of the 1918 virus similarly dangerous to previously healthy young adults. This flu originated in Mexico and rapidly spread to the US, Spain and elsewhere. This time, with early warning of the threat, the authorities were reasonably well prepared. They soon knew what organism they were up against and had some idea of how it might behave – although, as in 1918, no one really knew how severe it would be. Fortunately, the virus was nothing like as deadly as in 1918, and its fatalities were counted in the tens of thousands rather than tens of millions.
Over the past few decades the WHO and national public health services have set up a remarkably effective global surveillance and monitoring system, which can identify and track the progress of infectious diseases as they sweep across the globe. This system is authorised and supported by binding international agreements, with rapid reporting via the internet to health authorities and the mass media throughout the world. Within hours of a suspected human-to-human transmission being reported, its progress can be followed by anyone, anywhere.
This system relies on openness and transparency. Communicable diseases know no borders, and what happens on the other side of the world can all too rapidly overwhelm any nation’s capacity to function. A shared responsibility for global health and wellbeing is recognised as essential. But the system has its vulnerabilities.
The first is at the very start of the alert chain – the response of the local health worker faced with a suspected case. Crucial decisions have to be made. Is there anything unusual or particularly worrying about this case? Should I report it to my superior? What samples do I need to take? How can I prevent it spreading to family, friends and neighbours? How quickly do I need to act? Will I get into trouble if I make a fuss? These first few hours are by far the weakest link in the chain, and the risks can only be minimised by proper training and back-up. All countries need robust public health teams, especially in remote rural areas, with well-honed protocols and reliable lines of communication.
The next weak link is where disclosure of a virulent and dangerous disease by the authorities might have negative commercial or political consequences. In these circumstances there is obvious potential for coercion or corruption. It’s a worrying prospect, and it would be comforting to think it wouldn’t happen, but there have been many past instances when deception and delay in reporting outbreaks have cost lives.
A third vulnerability is similar to the cloak of secrecy that characterised the early weeks of the 1918 pandemic. How much should governments tell the people? How to strike the right balance between giving people the full facts and scaring the life out of them? One of the biggest worries the UK government had about the 2009 pandemic was that, in the worst-case scenario, people would be too frightened to leave their homes, essential services would break down and the economy would grind to a standstill. Detailed plans had been made for clearing hospitals and nursing homes to care for the sickest victims. Hundreds of refrigerated containers would have been commandeered to store the thousands of bodies awaiting burial. Volunteer forces were earmarked not only to keep essential services running but also to control panicky crowds and defend stockpiles of antivirals and antibiotics. This was scary stuff. How much did the public need to know?
In the event, there were almost daily bulletins and a balance was struck in terms of what was pushed out to the public and what was left unsaid. Fuller details were available on the net for those who wanted to know. There was no censorship, except where things touched on national security, but there was a selective approach to public communication: explicit about the risks and clear about the actions, but no more detail than was thought necessary. Subsequently, when the swine flu turned out to be much milder than feared, many people complained about too much hype causing too much anxiety.
The internet and social media have changed everything. For governments and individuals alike, secrets are much harder to keep. Even highly “secure” databases can be hacked and internal emails leaked. Not only are we now more aware of how much information governments are gathering about each of us, but also how much they are withholding from us. Increasingly, attempts at concealment fail. The political price of keeping the facts from the people is becoming ever more prohibitive.
So what can we expect with the next flu pandemic? We know it’s not a question of if, but when. Pandemic flu remains a top priority for governments throughout the world. In June 2013 the World Health Organization issued revised pandemic influenza guidance, again emphasising that openness and transparency are key.
So too, however, is the “precautionary principle” of erring on the side of caution. Does that caution mean telling people more than they need to know, or withholding potentially “counterproductive” information from them? In the routine medical world the prevailing practice is to share everything with patients – all the risks, all the benefits – and help them decide a course of action. With a highly infectious pandemic the authorities have to exert much more command and control, particularly if things get so bad that a state of emergency is declared.
So will this mean a return to the cloak of secrecy when the next pandemic strikes? It will be interesting to see how closely history repeats itself.