
Abstract
Occasionally brain-dead organ donors go into cardiac arrest before reaching the operating theater. In such cases, the needed resuscitation of the potential donor stimulates a range of concerns among the responsible staff. If the intensive care unit staff are going to carry out the organ retrieval, they must rush in with demanding treatment measures such as defibrillation shock and cardiac massage that may break breast bones and make the donor vomit. Such treatment measures conflict with widespread ideals of tranquility in donor care and yet they are currently under consideration in Danish intensive care units. Why is this type of ‘aggressive organ harvesting’, as it is sometimes called, considered a likely development, even to the extent that the interviewed health professionals request a policy prescribing procurement measures they morally deplore? We suggest that to understand this change of treatment norms, we must move close to everyday work practices and appreciate the importance of material–technical treatment options as well as the interplay of professional ethics and identity. The cardiac treatment of brain-dead donors may thereby illuminate how treatment norms develop on the ground and thus can theoretically develop our understanding of the mechanisms associated with increasingly ‘aggressive organ harvesting’.
I had never even considered the thought that you’d jump onto a brain-dead patient having a heart attack. Really, I hadn’t imagined that it was something anybody should or would do, or could see themselves doing! I would just think, well, yes, it just wasn’t meant to be. So it has really got me thinking, ‘cause for me it’s unnatural – it’s not unnatural to walk up to a brain dead and seize the organs – but it’s really provocative for me to have to jump onto a patient who’s then suddenly also suffering from cardiac death because then the game is kind of over, eh?
This article explores how postmortem organ donation and its associated techniques of dying affect and are affected by professional work ethics. We investigate the dilemmas faced by Danish health professionals in intensive care units (ICUs) when brain-dead donors go into cardiac arrest and need physically demanding treatment to conserve the organs. We outline how the professionals make sense of and deal with the situation, and we seek to understand why they, in a paradoxical manner, appear to welcome a policy suggesting a more ‘aggressive’ mode of organ procurement despite their personal dislike of the anticipated policy outcome. We argue that an explanation of the paradox can be found in the professional work ethics, understood as a sociomaterial modus operandi, and that these work ethics have implications for ICU work in general and for organ procurement from brain-dead donors in particular. By studying the relatively few instances of treatment of cardiac arrest, we thereby explore a set of more general mechanisms potentially at play when medical treatment norms gradually develop. Our point is to direct attention to how changes in norms take place on the ground and to the importance of organizational practices in this process.
Since the establishment of criteria for brain death in the late 1960s, which made it possible to harvest organs from bodies in which the heart continued beating (Beecher, 1968), brain death has been debated around the globe. It is considered highly controversial in, for example, Japan (Lock, 2002b) and was for years also controversial in Denmark where the brain death criterion was embedded in law as late as 1990 as one of the last countries in Europe. Despite continuing interest in the ambiguities of death (Zamperetti et al., 2003; Zeiler, 2008), the international literature indicates a very limited interest in instances where the two criteria of death collide, so to speak, as when brain-dead donors go into cardiac arrest (Cummings et al., 2009). Nevertheless, these instances raise issues of great concern for the people who care for the dying body. By exploring their concerns in light of their everyday work ethics, we learn about a lot more than a local moral dilemma; we suggest that it allows us to understand better the central mechanisms involved in increasingly aggressive organ procurement regimes and that it develops our analytical approaches to the sociology of work and work ethics.
The dead body, organ donation and professional ethics
Roger Cooter (2000) suggests that during the 20th century, the dead body underwent even greater changes than the living: it moved out of the home and into institutions; the average person stopped seeing and touching the dead; and with autopsies and organ and tissue procurement, the dead body became a resource for the living rather than merely laying claim to their resources with demands for funerals and sacrifices. As a consequence of its institutionalization, for the most part, death today is controlled and shaped by hospital staff, and as such, it has become subject to a professional ethics embedded in the norms and techniques of everyday work (Kaufman, 2005).
Postmortem organ donation constitutes a prime arena for negotiation of norms in the professions that work with death and dying. Health professionals have to orchestrate a bearable death for the bereaved relatives, while simultaneously ensuring organs for patients on the waiting list (Jensen, 2011). Stefan Timmermans (2006) observed how organ procurement has become increasingly insistent to the extent that one may talk about a ‘normalization of deviance’. Often social scientists have pointed to the tendency in the medical establishment to support an increasingly ‘aggressive organ harvesting’ regime, leading to exploitation of donor populations (Becker, 1999; Cohen, 2005; Fox and Swazey, 1992; Kaufman et al., 2009; Lock, 2002a; Lundin, 2010; Scheper-Hughes, 2001; Sharp, 2000). It is important, however, to avoid seeing health professionals as somehow automatically complicit in a societal appetite for organs because we would thereby bypass the opportunity to understand the mechanisms through which donor procurement evolves and instead assume a given set of motivations. In fact, we wish to suggest that enhanced organ supply has surprisingly little influence on the choices of health professionals when they face dilemmas relating to organ procurement from brain-dead donors with cardiac arrest. Also, we suggest that such dilemmas are handled not so much as conscious choices but, rather, are dealt with through a practical work ethics.
As Durkheim (1957) once argued, professional ethics and professional identity are coproduced. The social study of the mechanisms through which moral norms arise in medical work was pioneered by Charles Bosk (1979) in his seminal book Forgive and Remember: Managing Medical Failure. Bosk showed how norms and hierarchy are dependent on each other and how dealing with extraordinary life and death decisions necessitates developing equally extraordinary social mechanisms through which failures may become sources of learning rather than moral despair. Following Bosk, several studies have explored the emotional and moral demands imposed on health professionals. Such studies have illustrated the futility of attempts to separate fact and value: norms are embedded in medical technologies and vice versa (Anspach, 1993; Cambliss, 1996; Jennings, 1991). Sharon Kaufman (1997) has argued that health professionals learn to make decisions as part of a community engaged in a ‘lived practice’, not as autonomous individuals. In a study of work practices in ICUs, Robert Zussman (1992) nonetheless argued that norms manifest themselves in a ‘culture of the ward’ and suggested a contrast between this ‘culture’ and external bioethical discourses of individual rights. In fact, many sociologists and anthropologists have made sharp distinctions between lived medical morality, or local moral worlds, on the one hand, and universalistic bioethics, on the other (Fox and Swazey, 1984; Kleinman, 1999). Paul Brodwin (2008), conversely, has argued that the distinction between ethics and local norms has become somewhat overplayed. Professional ethics is socially produced (as is bioethics), and bioethical arguments and reasoning are part of the social pattern. Everyday hospital practices continually produce new and unproven situations in which no common ground has been found and where practitioners must act as ‘moral pioneers’ (Rapp, 1988). The materiality of these situations is rarely acknowledged, but ICU work does involve machines in a material environment that clearly goes beyond words. To address the local work ethics in such situations, we therefore need to appreciate this hyper-technical work environment as well as the physicality of donor management, in order to explore how it interacts with multiple forms of sense-making.
By placing ourselves among the health professionals in an investigation of colliding criteria for determining death, we build on the tradition for studying medical norms as socially engrained while paying attention to the materiality of work practices. Specifically, we seek to understand the acceptance of controversial treatment options in organ procurement to get behind the phenomenon identified by Timmermans (2006) as ‘normalization of deviance’ – and to do so we take the perspective of the people acting as moral pioneers: the people who in the course of their daily practices make the previously deviant into something normal.
Methods
This article is based on individual interviews and focus groups with health professionals who work with organ procurement in Denmark. It is a piece of ethnography-by-invitation in the sense that the authors were invited by the Danish Center for Organ Donation (DCO) to investigate the ethical dilemmas experienced by health professionals when treating cardiac arrest in brain-dead donors. DCO had received enquiries from health professionals finding this aspect of organ procurement troubling, and it is part of their organizational mandate to develop educational material to meet ethical challenges. To locate the right response, they wanted a better empirical understanding of the problem. We were asked to design an interview study, and an ethicist was asked to do an ethical analysis. The reason for contacting us was our previous experience with qualitative research in this field. For 4 years, one of us (A.M.B.J.) has studied organ procurement in Denmark (see Jensen, 2011), where she regularly came across the topic when observing organ donation cases and in interviews with health professionals. Since 2007, the other coauthor (K.L.H.) has studied bone donation in Denmark (see Hoeyer, 2010a, 2010b) and now serves as member of an ethics committee under the DCO in which ethical challenges faced by health professionals in organ procurement are discussed.
When designing the study, we began with the interview material from Jensen’s previous work and conducted a search for the topic of cardiac arrest, which turned out to be mentioned in 17 of her interviews with health professionals. Based on a preliminary analysis of this material, we developed a set of questions and selection criteria for relevant informants. In Denmark, brain death is established by neurosurgeons, who are also responsible for ensuring informed consent to organ donation from the donor relatives. ICU nurses attend to donor patients when they occasionally go into cardiac arrest, and anesthesiologists are medically responsible for treatment plans for potential organ donors. In conjunction with the DCO, we then identified representatives of these three occupational groups. We wanted to ensure that we included people of different ages, sexes and levels of experience, from different parts of the country, and we wanted to let these individuals express personal concerns. We also wanted to hear how the topic was discussed among nurses, among all ICU staff groups when brought together, and among neurosurgeons. We therefore set up the individual interviews and focus groups listed in Table 1. All interviews lasted for around an hour. The numbers in the left column are used as references for quotes. A total of 59 health professionals were included in the study.
List and number of respondents.
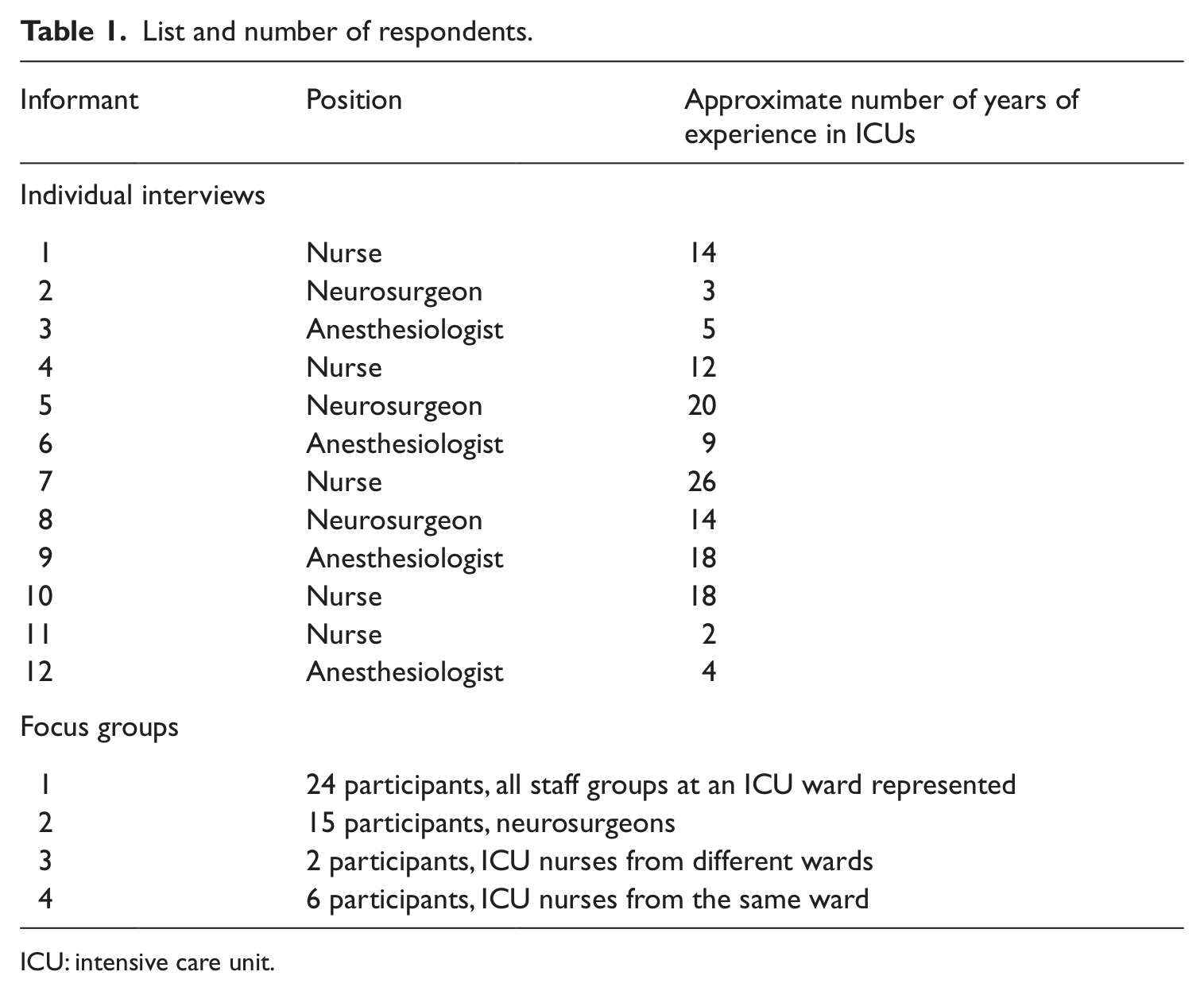
ICU: intensive care unit.
Analyzing the material, we first read through the material and established themes and analytical questions and then coded the interviews. Based on this, we selected material, made a preliminary analysis and checked that we found nothing in the previous 17 interviews contradicting what we found, and then decided to include only material from this study. The material was then organized in relation to three analytical questions on which the structure of this article is based (several quotes illustrate more than one point, but each quote is presented only once): What makes treatment of cardiac arrest problematic; how do health professionals deal with the sense of predicament; and how are transgressions perceived in relation to ICU work in general? We thereby seek to illustrate how ICU norms change on the ground.
Understanding the predicament: the sense of concern
The sense of concern experienced by health professionals who contemplated treating cardiac arrest in brain-dead donors is related to a set of linguistic and practical features, as well as to a concrete dilemma relating to the goals in organ-donor care and to the accentuation of more general tensions in the course of organ procurement. This section outlines these features. We then address the strategies used for dealing with the resulting sense of predicament.
Intervening actively in death and dying: confusion and concern
Current concerns about cardiac arrest in brain-dead donors relate to more general concerns about the proper definition of death. In Denmark, the introduction of brain death was relatively controversial and came into effect after 20 years of debate, in which widespread popular and political skepticism was expressed (Det Etiske Råd, 2008). In 1988, a majority of members of the newly established Danish Council of Ethics recommended preserving the existing cardiac death criterion when procuring kidneys. They based their decision on the assumptions that the relatives would not understand that a person with a beating heart could be declared dead. 1 Up until 1990, when brain death was introduced in law, doctors would wait for the heart to stop, declare death and then restart circulation and remove the kidneys (what is known as non-heart-beating donation). This practice has not been reintroduced in Denmark, and today, it is often referred to as more disconcerting than donations from brain-dead patients. Cardiac arrest in brain-dead donors nevertheless brings back the controversy about definitions of death because the two criteria of death collide in one and the same body. Ironically, it does not sustain confidence in the status of the person as dead.
The native terminology typically used in relation to treatment of cardiac arrest accentuates these problems. The Danish word for cardiac resuscitation is genoplivning, which is not just associated with medically restoring the function of the heart; it literally means ‘bringing-back-to-life’. During interviews and discussions, informants constantly corrected themselves and contemplated the need for a different vocabulary, not least when they communicate with donor relatives. One very experienced nurse, for example, explained: I think that if we use the word resuscitation [genoplivning] when talking to families where we’ve been discussing brain death, I think one will get very, very confused, because if one talks about death we can’t resurrect, really, and we’ve just been saying exactly that – that you can’t wake up when declared brain death. So I think you need to guard your words carefully! (10)
One anesthesiologist began using the English term ‘resuscitate’ with Danish pronunciation to avoid the Danish word, but most interviewees preferred to use ‘treatment of cardiac arrest’ (hjertestopbehandling). That we would also adopt the latter term almost seemed to be a condition for conducting interviews in this setting.
However, if we were to focus only on language, we would miss an important phenomenological dimension of the issue. Dealing with death and dying is a very material practice, and the health professionals experience bodies, and the responsibility they acquire for them, in a very concrete way. The nurse whom we quoted above, who otherwise was focusing on communicating with the relatives, later in the interview conferred a feeling of personal worry about cardiac treatment when explaining: Well, the person is dead, really, I think it would be … because it is a dead patient, on whom you must do something active, and that would perhaps be difficult … because it is so tangible – it’s very different from going in there and administer[ing] some medicine. (10)
The physical engagement that treating cardiac arrest involves thus provides a sense of the donor management being more active, which can be important not only in relation to the relatives, but it also tends to make cardiac arrest morally demanding for the medical personnel performing the act. Besides ‘active’, words such as ‘corporal’, ‘violent’ and ‘physical’ were used to describe what makes cardiac treatment special. In an uncanny way, treatment of cardiac arrest is an act of violence with benign intent. The almost violent physicality of resuscitation is usually justified as being the only possible way to rescue the patient’s life (Timmermans, 1996). In this case, however, it is too late to rescue the life of the donor. Cardiac treatment serves to conserve organs only. One nurse, who otherwise described herself as a great supporter of organ donation, explained why she felt that treatment of cardiac arrest implied a sense of (double) transgression: It relates to this thing that we somehow are playing God, really, it is going to the limit of what you can, really, the patient is sort of dead once and now he’s not allowed to die the second time he wants to do so. Really, what are we up to? Can you allow that? What do the relatives think and what do my colleagues think who stand right beside me? So I think you kind of step over a frontier [grænse] which is already transgressed once … perhaps. (4)
Throughout the interviews and focus groups, participants repeatedly referred to the visible and material spectacle in which the relatives see the treatment, which is unlike pharmaceutical donor management that can be performed very quietly and that ‘feels more natural’ (7) even if there ‘ought to be no difference’ (1). One neurosurgeon even thought of ‘active treatment’ as a ‘quantum leap’ compared to pharmaceutical treatment (8).
A real dilemma
From an outsider’s perspective, it can be tempting to compare increasingly aggressive organ procurement strategies with vultures watching over the dead and the dying. From the perspective of the health professionals who deal with the relatives, as well as with dying patients, however, this analogy is too simple. They are deeply engaged in orchestrating a meaningful course of events and often find that organ donation can be of great help to the donor’s relatives for whom the prospect of helping others and securing a legacy for the deceased can provide a ray of comfort in the midst of their grief (Jensen, 2011). One very experienced nurse explained that it was ‘one thing to ask for organs’ in the first place but ‘a hundred times harder’ to have to go back to the families and explain that the donation had failed (7), and in a focus group of nurses, a less experienced nurse had also seen the disappointment brought about by a failed donation, and she told her colleagues: You actually hold out the prospect for them of it not being all in vain that, for example, their mother dies. But then suddenly she suffers from cardiac death too, and if we don’t do anything they’re lost and that seems to me to be ethically problematic. (FG4)
Conversely, the interviewed health professionals typically emphasized several aspects of a dignified death, particularly a sense of tranquility that is incompatible with cardiac treatment. In one focus group including different professional groups, there was wide agreement that even if death was sure to be ‘messy’ when a patient was first admitted to an ICU, the ideal would be to keep the procedure silent, gentle, without pain and with a minimum of machines (FG1). Successful orchestration of a donor’s death implies a particular material aesthetics (Jensen, 2011). According to the participants in the focus group, organ donation is especially problematic when the patient’s relatives see it as prolonging the farewell unnecessarily or when the doctors find it necessary to quickly introduce choices for which the relatives are not prepared. The physical action of treating a cardiac arrest interferes with such aspects of a smooth orchestration of a quiet and dignified transition from patient to donor. The staff therefore faces a real dilemma: if they choose to treat the donor, the transition risks becoming undignified, but if they do not conduct the treatment, the effort to donate fails, and the donor’s relatives incur a second loss of control and meaning. One nurse explained the dilemma as follows: It is this thing with the farewell, that the farewell becomes different and the tranquility you ought to have and this consideration of the relatives … But then again, if the relatives have a very great desire that this must make sense, and they want to donate the organs, then it could become meaningful [for them]. (4)
In the course of one of the focus group discussions, one of the nurses said that treatment of cardiac arrest was the exact opposite of the ideal for donor care: Really, it is an extremely undignified situation, to be totally stripped and having, I don’t know how many people, throwing themselves on top of you, administering a lot of medicine and everything getting into a frenzy! It is very, very much in contrast to the other situation [donor care] where we gently and quietly administer Dopamine and attend to the small things, walk softly, and treat the patient with dignity. (FG1)
Some of her colleagues responded saying that treating heart failure ‘ought not’ be different from other forms of donor treatment, but the nurse was supported by the chief anesthesiologist, who said: I just believe it’s deeply rooted in us that you need to exit life in a proper manner and you should be paid respect on your way to your grave, one way or another. And it is not compatible, we believe, I think, with this thing – vomit floating all over the body, cardiac massage, and breaking the chest [bones]. (FG1)
An anesthesiologist from a different ward also was concerned about the prospect of treating cardiac arrest and said that a good death involved an element of letting go. She rhetorically asked, ‘Are they not allowed to die?’ (3). Letting go or ensuring the donation – there is no safe choice for the health professional who faces a brain-dead donor’s cardiac arrest.
From end to means: accentuating a shift from patient to donor
Treatment of cardiac arrest is also problematic simply because it accentuates a number of general dilemmas related to organ and tissue procurement. The shift from having been person and a patient to becoming a donor and a resource for the treatment of others is always difficult to handle and is a theme that runs throughout the interviews. Because treatment of cardiac arrest is so visible, it can be an unwanted mode of communicating this shift to the relatives, who must be informed about how the treatment plan has changed, perhaps even before they have accepted death as the only possible outcome. The chief anesthesiologist discussed above provided an example during a focus group: If we haven’t decided [whether a dying patient should become a donor], and a heart attack occurs in a patient who will inevitably die, then we need to decide not only on treatment of the heart, we also need to decide if we’re beginning donor care … at this late hour, when we’re all exhausted and we might be overcrowded. (FG1)
This shift is of great significance, not only for the relatives but also for the staff. One of his colleagues in the focus group had just stated that ‘the moment the brain stops working, it’s no longer a person – then it’s a stock of spare parts [reservedelslager]’ (FG1), and for some participants, such objectifications were deeply troubling. In one of the focus group discussions with nurses, one of the women who saw herself as a somewhat reluctant supporter of organ donation felt that treatment of cardiac arrest was clearly beyond her limits: ‘I know that this person is dead, but I also think it can become too much like dealing with stocks of spare parts’ (FG4). Similarly, a neurosurgeon saw in treatment of cardiac arrest a further objectification of the brain dead, this thing that you partout keep, how should we put it, alive, or alive is not the right word, but keep their organs alive even if they’re doing everything they can to depart or to ‘get off’. I find it wrong, I think it is additional objectification [tingsliggørelse] of the brain dead. (8)
It is even worse when the person is not even declared brain dead yet, the neurosurgeon explained, while deploring the prospect of having to ‘resuscitate just to let them incarcerate’, that is, to become brain dead and thus a potential source of organs (8). Some participants in this study said that this conflict was especially pertinent when donor treatment was prolonged (‘then you end up a bit like spare parts and reduced to just that instead of a human being’, 3). Aside from the instances involving resuscitation, the very transition from patient to donor can be problematic for attending staff, as for a nurse who, during a focus group, reflected that the transition from patient to organ donor does something to me, that I have to shift from thinking ‘a living human being’ to ‘an organ laboratory’, really it does something and I can’t say that I think it’s fucking great to become organ carer [organpasser] rather than patient carer [patientpasser]. (FG1)
Such sentiments were shared by a number of other nurses and came across in statements, such as ‘Here I’m getting into these things, that you keep alive, or create life, or resurrect [genopliver] to this factory, this organ factory … all of a sudden the donor has become the organs, I can’t stand that’ (FG3).
Cardiac arrest in brain-dead donors thus accentuates a number of more general concerns relating to organ donation procedures. It also introduces some additional concerns performing to the way the need for an aggressive treatment to fulfill the plan of organ donation disrupts the ideal of a dignified treatment of the dying person surrounded by tranquility. So what do the health professionals do? How do they deal with their predicament?
Learning to deal with it
As indicated above, renaming is a prevalent strategy to deal with the predicament. Not only do the health professionals seek to avoid the term ‘genoplivning’, but they also try to avoid terms associated with death in general, as if proper naming could erase the phenomenological sense of transgression and ethical quandary. Besides renaming, other strategies appear to be common: appeal to authority, appeal to rationality and medical fact, appeal to destiny or fate, call for debate, and giving in to practical obstacles. These strategies can be characterized as mechanisms for transfer of decision-making power and responsibility, and these mechanisms find particular expression in a desire for ‘policies’, as we explain below.
Strategies for transferring responsibility
Appeal to authority is a strategy commonly used among nurses who state that irrespective of their personal perception of treatment measures, they are not in a position to decide what is right or wrong: ‘it is always the doctor who decides’ (11). One quite experienced nurse maintained strong support for ‘aggressive donor care’, despite the opposition to such treatment expressed by other nurses. However, he would immediately stop the procedure if the doctor on call said to do so (1). Similarly, another nurse stated, ‘if you’re on duty with a doctor who says “we’re not doing that”, then that’s it, we don’t do it’ (4). Hence, medical authority translates into moral authority, and it works to enhance as well as to decrease the level of aggressiveness in donor care. Arguably, these nurses do not transfer responsibilities, since doctors already possess the formal medical authority. But, as Zygmunt Bauman (2000 [1989]) pointed out, such structures of authority do serve to relieve agents of their sense of personal moral responsibility for their acts, and as such, they circumvent or transfer their capacity to act as moral agents.
Interestingly, some medical doctors also appeal to authority, only in a slightly different way. One neurosurgeon was opposed to treatment of cardiac arrest, but said: I’m employed to carry out a piece of work and as far as I know it is only gynecologists and obstetricians who are entitled to decline performing abortions if against their conviction. I’m not sure I’m allowed to say no to this. (8)
Through appeal to authority, nurses and doctors appear to displace the responsibility for choosing to act, and this appears to ‘close the case’ – to present the decision as settled.
On the face of it, appeal to rationality is the exact opposite, and yet, on closer inspection, it is not all that different. Throughout the interviews and focus groups, participants pointed to a conflict between emotional and intellectual understanding and viewed the latter as superior. One neurosurgeon, when interviewed in his office, had just discussed the need to enlighten both the attending staff and the donor’s relatives about how the treatment of the heart in organ donation is no different from the treatment of other organs. He then commented on the need for rationality: ‘I believe it is important to try to consider what it is that makes you reach the decisions that you do … Is it rational or irrational …’. When we asked, ‘When is a decision irrational?’ he responded: Well, I think it is irrational if you don’t have any medical [faglig] reason for reaching it, but base it on something emotional that has no solid grounding in the reality that you face – because it’s your own boundaries you need to cross, and I guess you can say it’s no fun having to transgress one’s own boundaries, but then you have to put them aside. (5)
The Danish term ‘faglig’ has no proper English translation but signifies that it relates to the epistemic grounding of the speaker’s profession or discipline. Appeal to rationality therefore mirrors appeal to medical authority. An anesthesiologist also argued that treatment was ethically correct when ‘medically necessary’ and suggested that opposition to treatment of cardiac arrest was related to inadequate understanding of the physiological mechanisms of the heart (12).
Interestingly, she did not want to pursue prolonged cardiac massage beyond ‘a few [defibrillation] shocks’, explaining that ‘I’ve got limits too’ (12). Another anesthesiologist was opposed to prolonged treatment and explained her opposition by trying to move beyond the discourse of medical necessity when stating that the team had to see itself as treating not only organs but also attending to the wishes of the donor’s relatives (3). One neurosurgeon who was also opposed to treatment of cardiac arrest specifically stated that figuring out how far you would go ‘is more like an ethical issue than a medical issue’ (8). Note, however, that this is the same neurosurgeon who appealed to the law in an earlier quotation. In effect, this appeal defers the authority to the legal system, while the first neurosurgeon deferred to medical necessity and the anesthesiologist deferred to the relatives.
A slightly different way to frame decisions as being beyond medical settlement is to make a call for internal debate at the ward. This strategy also appeals to an agency beyond the individual. Though very common in ethical debates, in general, it is not common in our interviews. One young neurosurgeon (2), who said that debate would be the way to establish what to do, had never talked with anybody about this issue. She also admitted that she did not know anything about her colleagues’ general attitudes toward organ donation. This indicated that she did not use ‘debate’ to find out how to position herself. Rather her call for debate seemed to reflect a trainee’s tendency, when in doubt, to consult more experienced colleagues. One anesthesiologist asserted that discussions rarely affected anybody’s position; on the contrary, when somebody said that something was in need of ethical debate, it usually served to close a discussion: ‘this is not ethical, and then they don’t say anymore’ (9).
A different way of displacing the decision was to present the outcome as a result of destiny or fate, beyond personal control. In the focus groups, some informants saw a cardiac arrest as ‘a broad hint [vink med en vognstang]’ that donations were not supposed to be completed or ‘if the heart keeps stopping and we continue resurrecting, it’s just not supposed to be’ (FG3). One anesthesiologist said that in case of cardiac arrest, she would ‘… go and tell the relatives “I’m sorry, but it was others than us deciding”, and I’m pretty sure they’d understand’ (6). When we asked her who these ‘others’ were, she responded, ‘Well, then I’d say it was some kind of divine authority [højere magter], or the body itself saying stop. I’m not that afraid of saying such things’. She also made clear that ‘you should do everything possible to avoid getting into that situation and that’s what we do with pharmaceutical treatment’ (6). According to her account, pharmaceutical treatment does not interfere with such divine authority but physical massage and defibrillation do. Pharmaceuticals thereby represent an attempt to establish a technical solution to an ethical quandary.
The technical fix is not always enough, however, and in cases when it fails, many of the medical practitioners do talk about fate. The most common expression of this type is to talk about a decision reached by the brain-dead body. In one of the focus groups, a nurse was trying to articulate her own hesitancy about the treatment of cardiac arrest, when she looked down at the table in front of her while explaining, ‘It might also be that it’s the body’s way of, or how can I put this, somehow to say “Stop!”, eh, that “I don’t want this anymore”’ (FG4).
This way of imagining a dead body’s agency may contribute to the sense of an uncanny predicament. Accordingly, it may be more than a way to deal with the predicament. One neurosurgeon, who supported the treatment of cardiac arrest (but also said that it was unlikely that he would ever have to perform the physical operation himself), knew about such talk of the body ‘saying no’, but he felt it was just an expression used to avoid having to transgress personal norms (5). Some of our informants also recounted how donor relatives also would occasionally appeal to fate. For example, the wife of a brain-dead man initially had agreed to the donation of his organs, but when he went into cardiac arrest she was relieved to hear ‘the husband’s own voice’ opting out: he had shown her what he wanted (10). Again there is the feeling of relief that somebody else made the choice and acquired the moral responsibility.
Although appealing to fate holds some legitimacy for the health professionals, there are times when treatment plans can also be decided upon simply by adapting to practical obstacles – what we have elsewhere called an ‘ethics of muddling through’ (Hoeyer and Jensen, 2011). Again, the outcome is presented as being beyond personal control, or at least beyond planning, but this sort of explanation was seen by most informants as absolutely illegitimate. Nevertheless, an overwhelming workload can be given as the actual reason for declining to treat cardiac arrest (FG1). Often decisions must be made quickly and the available resources make it necessary to prioritize. The effect is to transfer decision-making capacity to something outside the individual. This transfer mechanism also seems pertinent to a strategy discussed in all interviews and focus groups – namely, a call for policy – which combines elements of all the above strategies.
A call for policy to close the case
One of the anesthesiologists had prepared herself for the interview by going through all the guidelines and policies of the ICU, and in the interview, she remarked how practically all aspects of donor care seem to be described in detail, except for cardiac arrest (6). Cardiac arrest is indeed an exception to regulations for donor care, and a clear majority of practitioners we interviewed mentioned that they would like to have clearer guidance. They apparently assumed that an explicit policy would prescribe treatment of cardiac arrest, though the current (unarticulated) policy on most wards seems to be not to treat cardiac arrest. The well-prepared anesthesiologist said that a written policy ‘would make treatment acceptable’ (6). One of the nurses explained that she would really need an official policy to begin treatment: ‘I would demand a guideline’ (10). Another nurse, who otherwise strongly supported cardiac treatment, felt that an official policy was needed to make the act legitimate: Really, if now a mother is lying in bed next to a child or a young person, caressing, about to say their farewells, and then suddenly there’s a cardiac arrest. Then you really need clear guidelines, also about talking to the relatives, about telling that the heart stops working so now I need to do something, because then it’s out of bed with mum and a whole bunch of other things you need to do. (7)
These medical practitioners advocated a policy as a solution to the ethical quandary, and interestingly, they believed that a policy would prescribe cardiac treatment as an element of standard organ donor care. They also appeared to hope that such a policy would deliver an appropriate vocabulary to alleviate the problem associated with the currently used term [genoplivning], which, as mentioned above, quite literally means ‘bringing-back-to-life’. Only four of those we interviewed did not support the development of policies or guidelines in this area. All four were reluctant to embrace resuscitation, and they argued for a need to accommodate ‘exceptions’ in which resuscitation would not be performed.
How policies can serve to clarify controversial and morally demanding treatment decisions and relieve the individual from the sense of personal responsibility is further illustrated with a quote from one of the nurses, who explains what participation in a training course earlier the same day had done for her. The course had outlined general procedures for organ procurement: It really straightened out some things for me, well, that it really absolutely doesn’t matter … every patient is a potential donor. It is really an important point, right?! Then you don’t need any qualms of consciousness, [when thinking] is this patient also …? And are these organs also suitable? I don’t need to decide any of that, I just need to optimize. That’s what I learned today. (FG3)
Previously, the nurse experienced the dilemma related to the transition from patient to donor as involving personal responsibility for asking only the relevant families to consider organ donation, but she viewed the course as having relieved her of this responsibility. Policy making thus seems to support a number of the strategies for dealing with the ethical predicament outlined above. The practitioners we interviewed envisioned a type of policy document that would provide a means of renaming the procedure in a way that would help redefine the ethical quandary as a medical necessity. Consequently, it could relieve the attending medical staff of the burden of personal responsibility by relegating it to institutional authority. If ethics is about open questions with no clear answers, a policy serves to bring clarity and close the case. Strikingly, most of the professionals who did not personally support cardiac treatment of brain-dead donors wanted a policy although they expected it to prescribe this anxiety-provoking treatment. Even if it is understandable that they felt a need to act in accordance with rules deemed medically and morally right, it is still not clear why they seemed to assume that a policy would necessarily prescribe aggressive donor care. Why did they not perceive termination of treatment of cardiac arrest in brain-dead or near-brain-dead donors as a policy option? Why would an option that contravenes the moral feeling of most of our informants be seen as the obvious choice when designing a policy?
Transgression as a vocation
To understand the paradoxical longing for a policy prescribing actions deemed immoral, we need to understand the mechanisms at play in the prevailing professional ethics in the workplace. We wish to suggest that the work ethics are saturated with transgression. To understand what we mean by this, it is necessary to go into the concrete experiences that provoke change as well as the wider context of professional ethics.
Concrete experience
Some of the health professionals who had no personal experience with treatment of cardiac arrest were shocked that anybody could even consider treating a cardiac arrest in a brain-dead donor. However, some of them who had actually tried giving full cardiac treatment said that it was similar to, or no worse than, other demanding tasks at the ICU. One nurse explained that ‘[t]he first time you have to do it … it’s a little transgressive, or how should I put it, but perhaps it’s really no worse than a lot of the other stuff you’re doing’ (1). Another nurse, working in a different part of the country, also initially experienced it as transgressive: ‘I remember that I thought, gosh, at the time, I thought it was going slightly beyond my limits that [the doctor] in that way stood there and defibrillated the brain dead to normalize the pulse again’ (7). For this nurse, the procedure made sense, however, because of her previous experiences with disappointed relatives of potential donors. After failed donations, she had asked herself, ‘Why did we stop the donor care, really?’ (7). Another nurse similarly thought after confrontation with disappointed relatives: ‘It must mean a lot for these people that the donation is accomplished and that’s why I’ve actually changed my position, so that today, well, I’m ready to provide treatment of cardiac arrest’ (10).
Moreover, she said that one would need to have concrete experiences with relatives before truly understanding this issue. She added that families reacted differently and that, for some, donation was not a desirable option. This concern for the relatives illustrates something about the type of ethics at play in this setting. It emerges through dialogues with people in desperate grief, and it originates in a very material practice. The technologies, bodies and the dramatic physical actions matter for the development of norms. Furthermore, transgressions can be transformative for the norms involved. Ethical norms in medicine are in a continual process of modulation, as was repeatedly pointed out to us, so that a transgression at one point in time need not be one at another. Just a decade ago, fewer people were prepared to consider organ donation. When the neurosurgeon would bring up the very possibility of donation, for many relatives it seemed like a violation of their moment of shock and grief after receiving the announcement of brain death. Today, relatives often raise the issue of donation before the staff do, and many already know about brain death (Jensen, 2011). Consequently, the formerly transgressive act is thus normalized, because of changes in the world in which it is performed.
The wider context: transgression as an integrated element of the work environment
Doctors and nurses alike spoke about transgressing individual boundaries as an integrated element of their professional development and daily work. The ability to sidestep initial disgust, disapproval and skepticism and just do stuff that in all other circumstances would be revolting is essential to the upkeep of ICU routines (cf. Anspach, 1993; Zussman, 1992). While transgression is often presented in the literature as action that violates ethical norms, in this case, it is more akin to an ethical norm in its own right. It facilitates treatment and it promotes equality, irrespective of personal prejudice. And as such, it is a cherished and respected moral value at the ICU, and part of the working habitus. In a focus group, one nurse looked at her colleague and reminded her: We constantly move between ethical dilemmas, we work in that space [felt], and sometimes we’re actually instructed to do stuff that I as an ICU nurse can feel I do somehow against my will, ethically speaking … but then again, then you can’t work at an ICU, if you can’t compromise. (FG3)
Later, she considered whether this willingness to embrace the transgressive act would make her sidestep her initial dislike of the treatment of cardiac arrest in brain-dead patients: ‘God only knows if one will feel differently tomorrow when you’ve slept on this … you never know’ (FG3). Change of one’s personal stance is a deeply integrated element of the work experience in the ICU, or as one anesthesiologist put it: You’ve got some limits [grænser] to what you’ll do, and you listen to them but you also have to push them and it all comes with knowledge and experience and it can also come simply from seeing satisfactory courses of events. (3)
Of course, awareness of the so-called organ shortage is an important incentive for transgressing personal norms, ‘we’ve got to get these organs’ (2), as a young neurosurgeon put it. It is striking, however, that we heard few such arguments and that most interviewees preferred not to know about organ recipients and lives saved: they focused on donor relatives.
The general experience of changing norms translates into an expectation of continual changes also in relation to the treatment of cardiac arrest. The logic seems to be that a future policy will make it obligatory, and if it is deemed the right thing to do, in general, medical staff will learn how to do it and will get used to it. It does not mean that they will cease having limits to what they are willing to do; only that these limits will change in response to the environment in which they work. It does not mean that anything goes; rather, it means that the creation of limits is a never-ending element of ICU work. Boundaries are not there waiting to be transgressed; they are sensed and enunciated through ‘transgressive’ practices. This form of transgression and moral pioneering is the order of the day.
Studying ethics as an intervention in ethics
Prior to their participation in our study, many informants had not imagined that anybody would consider treating cardiac arrest in a brain-dead donor. All the same, they expected such treatment to become standard following the interview or focus group discussion. Gradually, we realized that our study interacted with this ethics of transgression. Simply by way of introducing the theme, we were changing norms. In the focus group with neurosurgeons, one man ended the discussion by saying, ‘No doubt this unwritten code saying that we’re not beginning treatment of cardiac arrest in conjunction with organ care, I think that will change’ (FG2). A colleague responded with a call to write up a guideline, a policy. This was a consequence of the focus group!
Our study was done by invitation from the DCO. This organization specifically works to stimulate ethical debate among health professionals, by offering courses, conferences and educational material. Although we simply intended to introduce topics of concern, these topics were never neutral, as they were treated within an underlying frame of an ethics of transgression. For example, one nurse recounted, ‘We went on an ethics conference with DCO and we got to talk about it and hear opinions and then you change [opinion] bit by bit and begin to think, why was it that we used to say no?’ (4). We believe that the various strategies outlined in the previous section – call for debate, call for rationality, call for authority and call for policy – must all be understood in light of the underlying moral framework described in this section. It is within this framework every new topic is worked upon and digested.
Conclusion
When a brain-dead donor goes into cardiac arrest, a sense of confusion emerges: Can the dead donor die a second time? What can legitimately be done to a brain-dead body? The confusion imposes a responsibility on the health professionals who are on the scene. Either they must accept a failed donation, and the accompanying frustration among the relatives, or they must do something very active to the body, something which is perceived as violent. It creates a dilemma between donation and dignified dying, and it accentuates an already existing conflict associated with the shift from patient (considered an end in his or her own right) to donor (serving as a means for others). The depth of the predicament relates to the implications of having to actively execute a violent act. The physicality, the sense of brutality, is a central element of the predicament, as illustrated with the common reference among the health professionals to a more acceptable ‘pharmaceutical fix’. The feeling of performing a violent act provides the health professionals with a weightier sense of responsibility. The physicality is not problematic in its own right, indeed resuscitation is performed everyday in ICUs and elsewhere, but it seems to become problematic when performed on a person who does not stand to gain from it. In that sense, it is the changed parameters of benefit that make physical procedures into a form of violence, but the physicality seems to work on the health professional, as it were, independent of more intellectual reflections. Previous work on resuscitation highlights how the procedure strips the patient of identity and makes him or her into a medical case (Timmermans, 1996). However, when performed on a brain-dead patient, the ‘stripping’ seems to reduce the patient to organs, to ‘meat’, rather than merely a medical case, and as such, it accentuates the tensions associated with the shift from patient to donor. 2 This objectification of the body is complicated further by the contradictory movement expressed in the practitioners’ sense of the body in cardiac arrest as ‘opting out’ of the procedure and thereby ‘making a choice’. By meeting two sets, rather than one set, of criteria for defining death, the body’s status as dead is thus paradoxically destabilized.
We have shown how the way out of the predicament involves a set of strategies, which, besides renaming the procedure, consist of appeals to authority (Bosk, 1979), to rationality and medical fact, to destiny or fate, to calls for debate or simply to the necessity of adapting to practical obstacles. All these strategies combine in a call for policy. The central mechanism that makes a strategy appealing revolves around its ability to transfer decision-making capacity and responsibility. A ‘solution’ is judged by its ability to close the case. It seems to be driven by a longing to leave a moral swamp for a safe haven of rectitude (Hoeyer, 2005). Even if this longing is understandable, the analysis produces a new question: Why is a policy expected to be in conflict with the prevalent moral intuition among the health professionals? Why is it automatically assumed that a policy will advise more aggressive treatment?
In order to understand this paradoxical call for an unwanted demand, we need to understand the professional ethics that serve as an unarticulated modus operandi, a work ethics, a lived practice (Kaufman, 1997). We find in the lived practice a moral motor for the digestion of new topics, a tacit and socially engrained set of values guiding the constant need for instant problem solving. The central element of this modus operandi is what we have called a transgressive ethics. It imposes on the staff a set of demands that are part of making ICUs into lifesaving places. It motivates care even in cases of personal aversion or prejudice against selected patients. As consistently pointed out in this article, a workplace ethics is more than a social or emotional issue; it emerges in conjunction with very material – even violent – practices. Perceptions of cardiac arrest change through concrete experience: as one nurse said, once you try it, it is no worse than a lot of other stuff, but it also changes through experiences with disappointed relatives hoping for all organs to be used. The needs of the actively responding subjects – the relatives – in this way make more pressing demands on the staff than the purely abstract principle of ensuring a dignified death for the deceased. This focus on concrete experience does not mean that philosophical bioethics is of little or no relevance to the work ethics, as social scientists sometimes hold (e.g. Kleinman, 1999; Zussman, 1992). Ethicists lead courses and appear at conferences, and the statements they make are used – sometimes in contradiction with their intentions – to bring the desired closure of the case: this is right and this is wrong. Such advice is seen as useful. But ethical principles are not driving the modus operandi, they are digested by it.
Like the messages relayed by philosophers, our study was also digested by the transgressive ethics of the clinic. The way in which we introduced the topic became a way of stimulating change. Even at the plain level of adopting a vocabulary of ‘treatment of cardiac arrest’ and cleaning out all references to resurrection (‘genoplivning’), we, somewhat inadvertently, supported a new approach to these issues. It imposed upon us a responsibility and a need to reflect on our task. We do not think there is any easy way out: treatment of cardiac arrest in brain-dead donors involves real dilemmas that cannot be erased with the armchair analysis. We do not believe that our task is to settle the matter for the health professionals or politicians. On the contrary, we see a role for social studies of medicine for facilitating reflections when people are otherwise eager to close a case. Michael Jackson (1982, 1998) has pointed out how passing a moral judgment aims at producing closure, despite inherent ambiguity. Once it is settled, whether as a ‘good’ or ‘bad’ action, one does not need to think anymore.
We believe that it is necessary to keep thinking, if only for a little longer than transgressive ethics would suggest. Why is that? Incorporation of technical options such as cardiac treatment has complex implications for the health professionals as well as for patients and relatives. They involve interplay of techniques and norms for producing necessary choices. The health professionals who are left with having to make these choices seem to want some form of societal support. It needs to be well reasoned. This longing for guidance might be a particularly Danish phenomenon, of course, and it certainly is different from the usual portrayal of medical self-confidence. All the same, there is reason to contemplate the shared social responsibility involved in asking people to perform violent acts (Arendt, 1998, 2006). Much social science commentary on ‘aggressive organ procurement’ has pointed to medical institutions as transgressors of societal norms (Becker, 1999; Fox and Swazey, 1992; Scheper-Hughes, 2001). Such framings easily convey the impression of donors and donor relatives as victims of society’s boundless appetite for body parts and portray health professionals as mere instruments for procurement. However, in this case, the health professionals who perform these transgressive acts appear to be the ones who are left with a sense of suffering. They suffer if they perform the act; they suffer if they do not do it and thus lose the donation. Who is responsible for this suffering? Who helps them out? We believe that it is important to contemplate more complex patterns of guilt and victimhood in organ procurement than a literature on ‘normalization of deviance’ would tend to do, and we believe that we need to appreciate the workings of the moral motor embedded in everyday work, rather than yielding completely to metanarratives about societal needs or personal moral deviance when explaining changing moral norms. The alleged ‘normalization’ of so-called aggressive organ procurement cannot be properly understood without appreciation of a transgressive work ethics that makes everyday dilemmas manageable.
Footnotes
Acknowledgements
We would like to thank the health professionals for taking their time to discuss their concerns with us. An earlier version was presented in an AAA session in Montreal (November 2011), organized by Linda Hogle and Lynn Morgan, and we would like to thank the organizers for the invitation and discussant Hannah Landecker as well as Morten Rod for comments at this early stage. We also thank two anonymous reviewers with this journal, Editor Michael Lynch and our colleagues in Section for Health Services Research, University of Copenhagen, for comments on earlier drafts.
Funding
This study has received support from the Danish Research Councils and Danish Centre for Organ Donation (DCO).