
Abstract
This study aimed to elucidate factors related to suicidality in a high-stress population—music industry touring professionals. It also examined whether trait mindfulness plays a moderating role in relations among these factors and suicidality. Touring professionals (N = 1,154) responded to an online questionnaire that included the Center for Epidemiological Studies Depression Scale–Revised (CES-D), Perceived Stress Scale (PSS), Suicide Behavior Questionnaire–Revised (SBQ-R), and the Mindful Attention Awareness Scale (MAAS). Mediation and moderated-mediation analyses were conducted on data from completed instruments (n = 550) with PSS as the antecedent, CES-D as the mediator, MAAS as the moderator, and SBQ-R as the outcome. The indirect effect of stress through depressive symptoms on suicidality was significant. The moderation of this indirect effect by mindfulness also reached significance, with greater mindfulness scores associated with an attenuation of the impact of stress on suicidality through depressive symptoms. Mindfulness was a moderator of stress on depressive symptoms and suicidality. Mindfulness-based interventions for populations under high stress, such as touring professionals, may be an important topic for future research.
The World Health Organization classified suicide as a “leading cause of death worldwide” in 2019 and the fourth leading cause of death among people aged 15 to 29 years (World Health Organization, 2021). Suicide is the 10th leading cause of death in the United States and the second highest cause of death in Americans aged 10 to 34 years (Adams & van Dahlen, 2021). Although the formal study of suicide began in earnest more than a century ago (Durkheim, 1897), the growing number of individuals who take their own lives in the United States and around the world (Alicandro et al., 2019) indicates that more effective clinical interventions are needed to counter this alarming trend. One high-risk population consists of musicians and crew members (such as audio, lighting, and instrument technicians, along with a myriad of other production roles) in music touring, an industry with elevated levels of suicidality (D. T. Kenny & Asher, 2016; Ludwig, 1992; Preti et al., 2001; Van den Eynde et al., 2016) and depression (Barbar et al., 2014; Kapsetaki & Easmon, 2019; D. Kenny et al., 2014). Stressors known to affect individuals in this profession include arduous travel schedules, long workdays, erratic sleep patterns, challenging interpersonal dynamics, and availability of substances of abuse (Raeburn, 1987). A descriptive study on an international sample from this population (508 touring musicians/crew members), published recently, found 50% to be at high-risk for depression, 39.4% exhibiting high scores for suicidality, and stress levels that put them at high-risk for health issues (Newman et al., 2022). The results of this study also indicated that trait mindfulness might be protective against risk factors such as stress and depressive symptoms. The current study aimed to investigate the relationships between stress, depressive symptoms, trait mindfulness, and suicidality in this population. The goal was to identify potential interventions for individuals in high-stress environments.
Suicidal behavior and its underpinnings have been investigated since Émile Durkheim (1987) proposed his seminal theory in 1897. Later work introduced concepts such as hopelessness, emotion dysregulation, and diathesis-stress models (Beck et al., 2006; Joiner, 2005; Klonsky & May, 2015; Kovacs & Garrison, 1985; M. M. Linehan, 2018; O’Connor, 2011). Although theories of suicidal behavior continue to evolve, there is a strong line of evidence showing a positive relationship between stress, depressive symptoms, and suicidal behavior (Arria et al., 2009; Beck et al., 2006; Branley-Bell et al., 2019; G. K. Brown et al., 2000; Chu et al., 2017; Dean & Range, 1999; Joiner, 2005; Kendler et al., 1999; Kliem et al., 2010; Klonsky & May, 2015; Yurgil et al., 2021). As stated above, elevated levels of all these factors have been reported for touring musicians and their crew members (Newman et al., 2022). Thus, finding ways to intervene and mitigate these relations is especially important in this community.
Mindfulness-based interventions (MBIs) are recent additions to psychotherapy’s toolbox and have already been shown to be effective in treating a variety of psychological problems, such as anxiety, stress, and depression (Khoury et al., 2013). Mindfulness is the practice of paying attention to one’s experiences in the moment with an attitude of curiosity, openness, and acceptance (Kabat-Zinn, 2009). MBIs such as mindfulness-based stress reduction (Kabat-Zinn & Hanh, 2009), mindfulness-based cognitive therapy (Teasdale et al., 2000), and mindfulness-based relapse prevention (Bowen et al., 2014) incorporate techniques such as guided meditations, yoga, body scanning, and breathing exercises into psychotherapeutic treatments to foster increased mindfulness in patients. Kabat-Zinn (2009) notes that mindfulness is a tool individuals can use to “ride the waves of stress,” which is less detrimental to one’s psychological well-being than actively fighting against distressing experiences, cognitions, and emotions. Mindfulness, in other words, cannot stop individuals from experiencing stress, but can help dampen its effect.
Recent research suggests that these approaches could be efficacious in treating many of the contributors to suicidal behavior, including difficulties with emotion dysregulation, stress regulation, depressive symptoms like hopelessness, and symptoms associated with cognitive deconstruction (Arria et al., 2009; Chesin et al., 2016; Forkmann et al., 2014; Goldin & Gross, 2010; Hill & Updegraff, 2012; Hofmann et al., 2010). A meta-analysis of 13 studies (n = 627) provided preliminary evidence for MBIs as an effective treatment for suicidal ideation and replicated previous research that demonstrated their efficacy in treating depression (Schmelefske et al., 2020). Moreover, studies have found that higher levels of trait mindfulness have been associated with lower levels of cortisol awakening response (Daubenmier et al., 2014), are protective against depression in high stress periods (Bränström et al., 2011), and have a dampening effect on the positive relationship between perceived discrimination and depressive symptoms (Brown-Iannuzzi et al., 2014). High trait mindfulness and improved mindfulness in general may attenuate the complex interactions between stress and mood symptoms described in diathesis stress models of depression (Hammen, 2005; Monroe & Simons, 1991).
Finally, scatterplot data from the previously mentioned study (Newman et al., 2022) clearly showed two distinct groups among touring professionals: one with high levels of suicidality, low levels of mindfulness, and higher levels of depressive symptoms, and another with low suicidality, high mindfulness, and lower depressive symptoms scores. This trend, along with participants’ mean mindfulness score of 3.69 (Barajas & Garra, 2014)—similar to that of clinical populations diagnosed with depression and/or anxiety disorders—indicates that this population may benefit from MBIs. Furthermore, an intervention study with a pre–post design using MBIs found significant increases in mindfulness in a sample of 25 music students (Czajkowski et al., 2022), which suggests mindfulness may be amenable to change in a related population.
Study hypotheses
Based on recent studies and the body of work discussed above, it was hypothesized that there would be positive relationships between stress and depressive symptoms, as well as between depressive symptoms and suicidal behavior. In addition, it was hypothesized that there would be an indirect (mediation) effect of stress through depressive symptoms on suicidal behavior. Finally, it was predicted that trait mindfulness would moderate the indirect effect of stress through depressive symptoms on suicidal behavior by attenuating the positive relationship between stress and depressive symptoms (conditional indirect effect, moderated mediation).
Method
This study was conducted in accordance with the principles of the Declaration of Helsinki and the protocol was approved by the institutional review board at the Biomedical Research Alliance of New York (Brany; Lake Success, NY). Online informed consent was obtained from all participants.
Study sample
The study consisted of self-identified individuals from the touring music industry, including performers and crew members. Inclusion criteria for the study included: experience as a touring professional, age 18 years and over, full comprehension of the English language, and access to a computer with an internet connection. Recruiting took place via emails, which were distributed by organizations within the music industry, as well as snowball sampling on social media (Facebook, Instagram, etc.). Participants reviewed eligibility criteria on the survey website, provided online informed consent, and then were directed to begin the survey battery. Data collection took place between February 2 and March 15, 2020, and informed consent was provided by 1,154 individuals. Of these individuals, 550 completed the psychosocial instruments used in this study (47.6% completion). Two-way χ2 analyses were conducted with each variable listed in Table 1, including whether the participant worked as an artist or a member of the touring crew, to investigate significant differences between those who completed the survey and those who did not. As expected, there were many more crew members than artists, given the large support staff required to maintain a sizable music tour. Region of origin (collapsed into four regions: the United States, Canada, the United Kingdom, and Other) was the only significant result. Individuals in predominantly English-speaking countries (the United States, Canada, the United Kingdom) were more likely to finish the survey than participants in the Other category, N = 1,154, χ2(3) = 139.97, p < .001. This difference might have occurred because English is likely not the first language for many of the participants in the Other category.
Demographic Characteristics of Artists and Crew (N = 550).
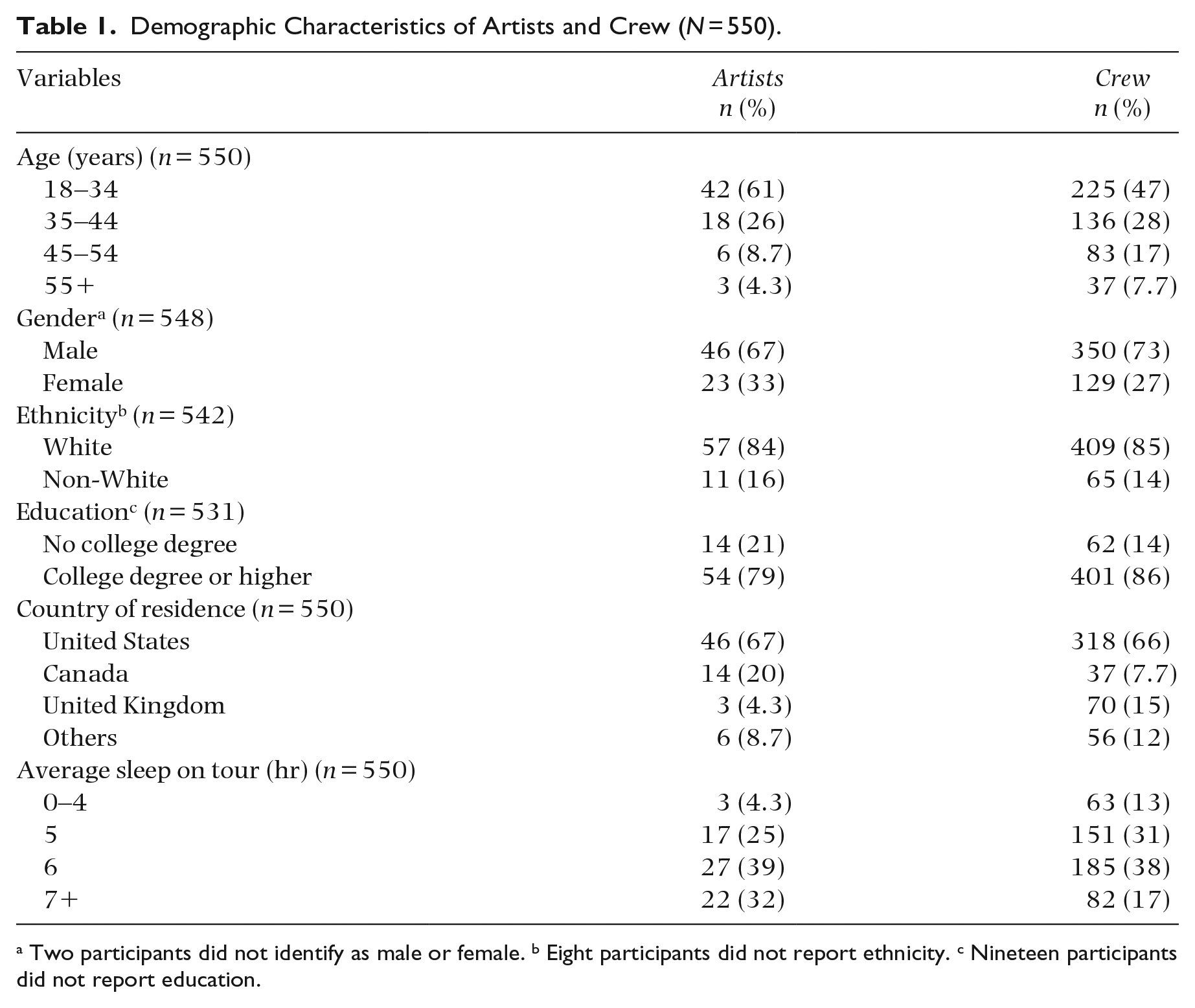
Two participants did not identify as male or female. b Eight participants did not report ethnicity. c Nineteen participants did not report education.
Measures
This study employed a survey design to collect demographic and psychosocial information about music industry touring professionals. Participants completed a battery consisting of 239 items, including questions about sociodemographic background (i.e., gender, ethnic identity, income, age), health behavior (i.e., sleep, fitness, nutrition, screen time), workplace stressors, home life, experiences of loss, and spiritual behaviors (Newman et al., 2022). Seven validated psychosocial instruments were included in the survey, four of which were included in the current study.
Perceived stress was measured using the Perceived Stress Scale (PSS), a widely used 10-item self-report scale designed for use in community surveys (Cohen et al., 1983). The mean score for this instrument in a 2,837 community sample was 13.02 (SD = 6.35), with a Cronbach’s α of .78 (Cohen, 1988). Subsequent studies have validated the PSS for use in a variety of settings and cultures (Andreou et al., 2011; Lee & Jeong, 2019; Leung et al., 2010; Sun et al., 2019).
The Mindful Attention Awareness Scale (MAAS; K. W. Brown & Ryan, 2003) was used to assess participants’ trait mindfulness, that is, one’s awareness and attention to what is taking place from moment to moment. The MAAS is a 15-item self-report measure, with each response measured on a 5-point Likert-type scale. Higher average scores indicate greater mindfulness. The mean mindfulness score for undergraduates in the original 2003 study was 3.85, while Zen meditators’ mean score was 4.38. Cronbach’s α estimates of internal consistency for a variety of samples ranged from .80 to .87.
Depressive symptoms were measured using the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). The CES-D is a 20-item self-report questionnaire that was designed to measure depression risk at the population level and for use in nonclinical samples, which reported a high Cronbach’s α of .90 (Skorikov & Vandervoort, 2003). A clinical cutoff score of 20 was used to classify participants’ risk of depression, as a recent meta-analysis found that this score afforded the instrument a better trade-off between sensitivity and specificity than the traditional score of 16 (Vilagut et al., 2016).
Participants’ suicidality was measured with the Suicide Behavior Questionnaire–Revised (SBQ-R; Osman et al., 2001), which is a modified version of the Suicide Behavior Questionnaire (M. Linehan & Addis, 1983) that has utility in population-based research due to its small number of items and adequate psychometric properties (Batterham et al., 2015). A four-question self-report measure, the SBQ-R assesses history of suicidal ideation and attempts, the prevalence of suicidal thoughts over the past year, current risk for a suicide attempt, and the probability of suicidal behavior in the future. Following a transformation, scores range from 3 to 18, with higher scores indicating higher suicidality. In non-clinical samples, internal consistency was found to range from .76 to .87. The recommended cutoff score for high suicidality in the general population is ⩾7, (Lew et al., 2020; Osman et al., 2001), and is used to form a dichotomized measure in the current study.
Statistical analyses
Statistical analyses were conducted using computer programming software R and SPSS version 27 (IBM Corp., 2020; R Core Team, 2021). Descriptive statistics included means, count data (%), and standard deviations. Bivariate correlation coefficients were calculated for all psychosocial instruments using the Holm adjustment for multiple comparisons. Multiple regression analyses were conducted, one for depressive symptoms (linear) and another for suicidality (logistic) as an outcome measure with and without the covariates listed in Table 1. The χ2 tests of independence were run for the categorical variables listed in Table 1 to compare participants who completed the survey versus those who did not. Multivariate analysis of variance (MANOVA) was conducted to assess differences between artists and crew members on the psychosocial measures described above. MANOVA was followed up by performing discriminant analysis to investigate further the relations between the psychosocial measures and group membership (artists vs. crew members). A single χ2 test of independence was run for the SBQ-R to compare artists versus crew members.
Hayes’ Process macro for R was used to test the hypotheses (Hayes, 2022). Mediation between perceived stress (antecedent), depressive symptoms (mediator), and suicidality (outcome) was tested using Hayes’ Model 4 (Figure 1). Moderated mediation between perceived stress (antecedent), depressive symptoms (mediator), mindfulness (moderator), and suicidality (outcome) was tested using Hayes’ Model 8 (Figure 2). Effects were considered significant if the 95% bias-corrected and accelerated (BCa) bootstrap confidence intervals did not contain zero. The data set analyzed in the present study is available from the corresponding author on reasonable request.
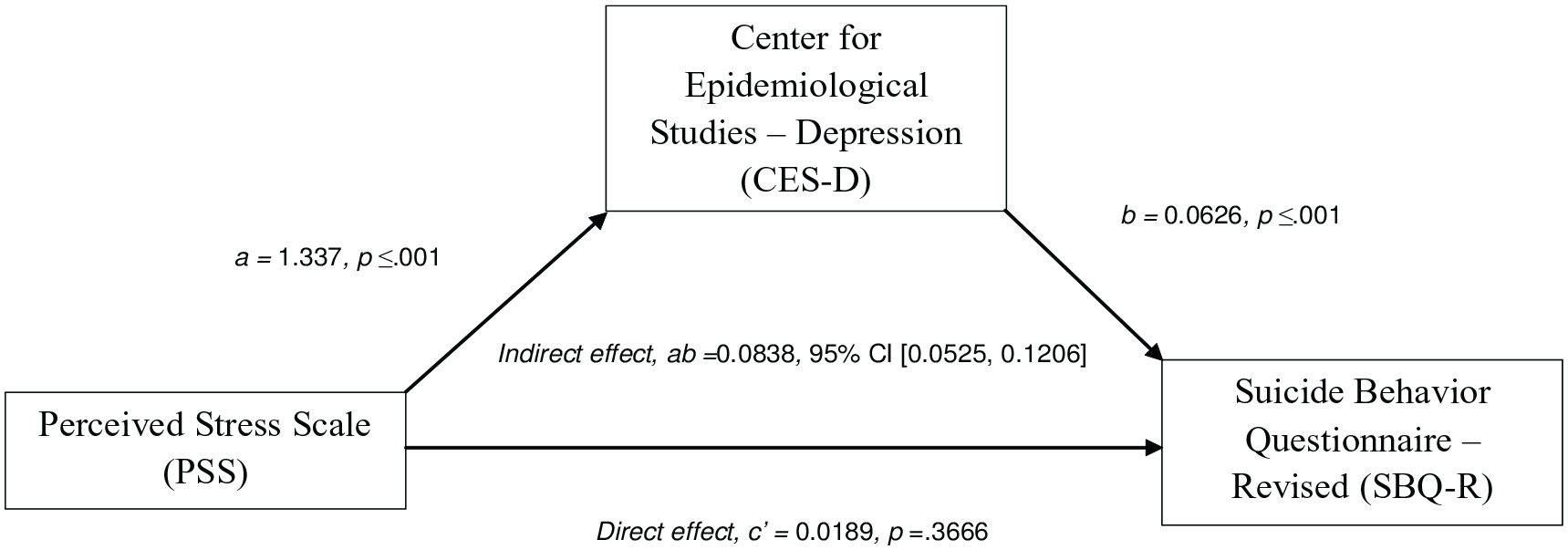
Mediation Model of the Indirect Effect of Perceived Stress on Suicidal Risk, Mediated by Depressive Symptoms. The Confidence Interval for the Indirect Effect is a BCa Bootstrapped CI based on 5,000 Samples.
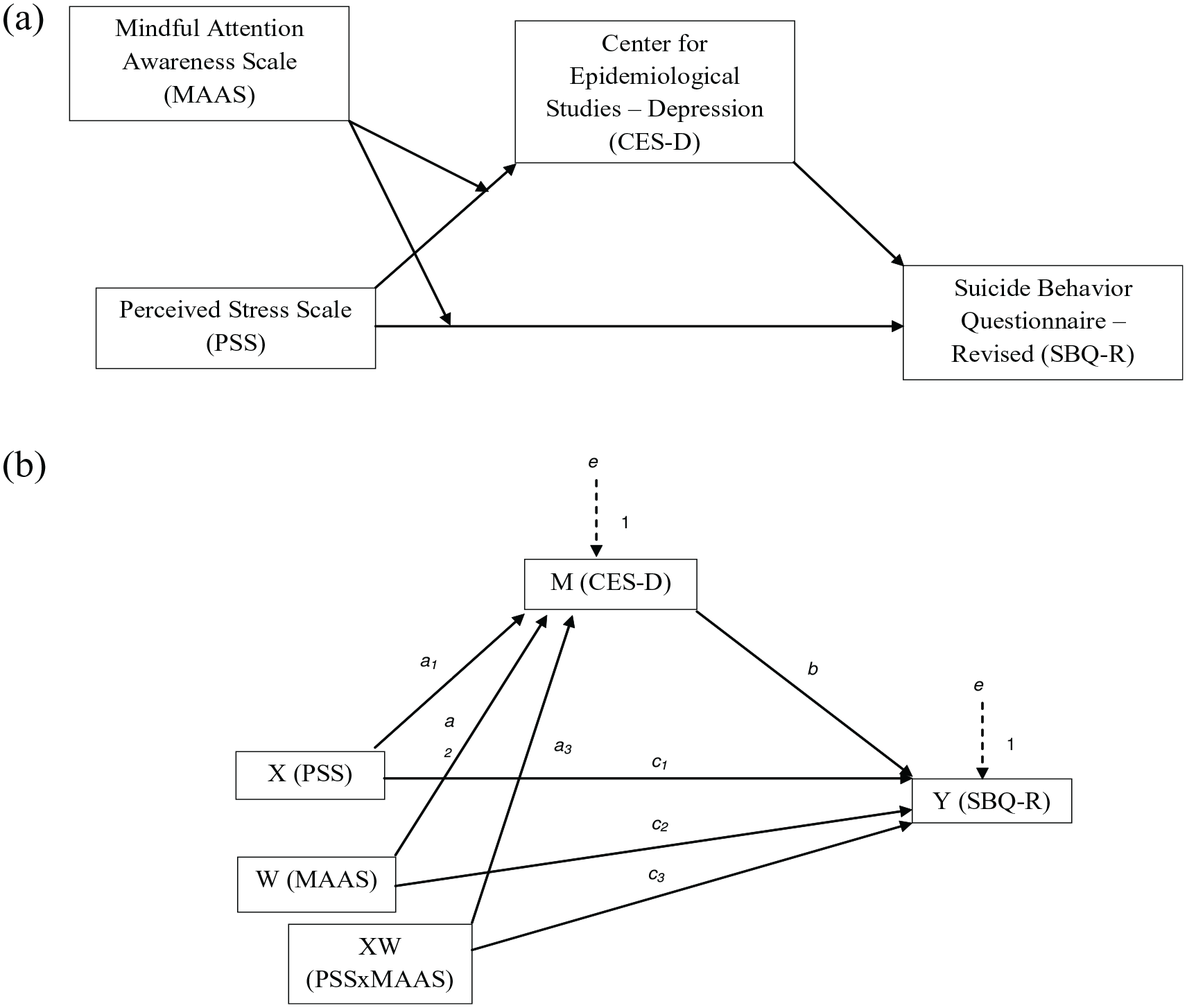
Moderated-Mediation Model of Perceived Stress as a Predictor of Suicidality, Mediated by Depressive Symptoms with Mindfulness as a Moderating Factor for the Relationships Between Perceived Stress and Depressive Symptoms and Perceived Stress and Suicidality: (a) Conceptual Diagram of the Moderated-Mediation Model and (b) Statistical Diagram of the Moderated-Mediation Model.
Results
Table 2 gives means and standard deviations of each psychosocial measure stratified by artist/crew. The mean CES-D score for the total sample exceeded the criterion cutoff score of ⩾ 20 for depression risk. Moreover, of the 550 participants in the sample who completed the relevant instruments, 218 (39.6%) had a score of 7 or above on the SBQ-R, categorizing them as high risk for suicidality. The mean PSS score for the sample was 18.4, which falls within the moderate range. The mean MAAS score was 3.7, which is below scores found in the general population and well below Zen meditators (K. W. Brown & Ryan, 2003). The previous study on touring professionals indicated that high trait mindfulness might be a protective factor against suicidality (Newman et al., 2022). Figure 3 illustrates histograms and density plots split by level of suicidality. Each panel represents a different range of MAAS by level of PSS, with CES-D scores along the x-axis. As we inspect higher levels of MAAS for each level of stress, there are fewer individuals that reach the cutoff score for the SBQ-R, and the peak depressive symptoms values concurrently shift to the left. This mirrors the correlation matrix results in Table 3, which showed significant negative correlations between MAAS and CES-D, SBQ-R, and PSS.
Psychological Instruments (n = 550).
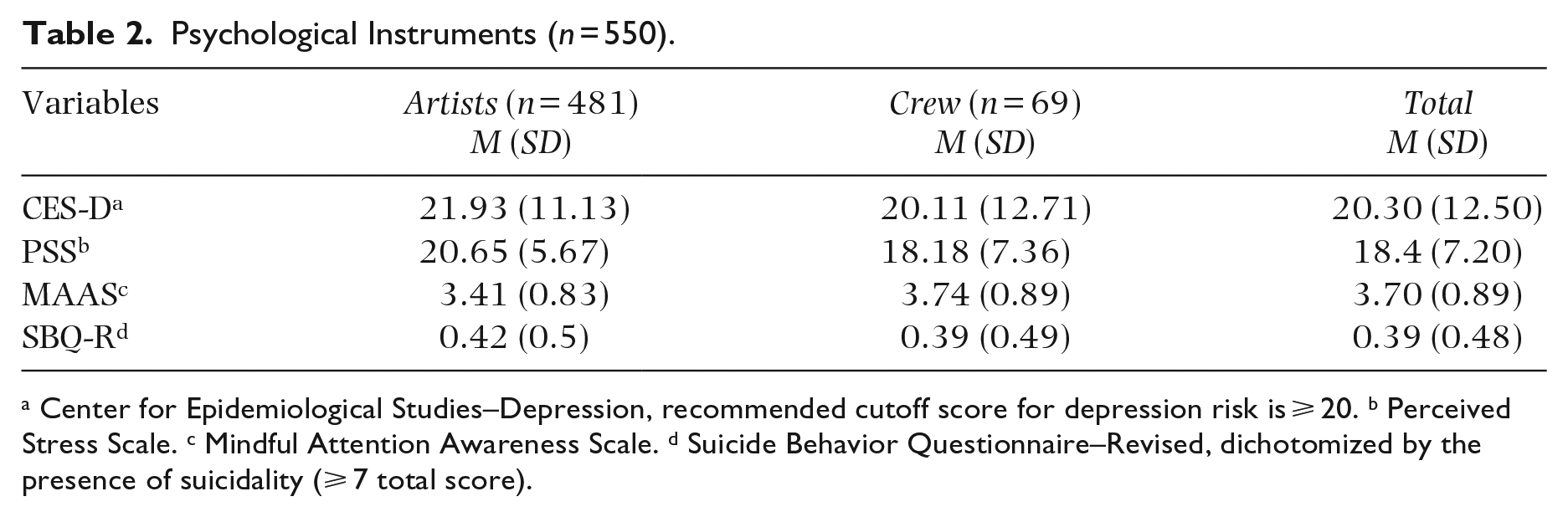
Center for Epidemiological Studies–Depression, recommended cutoff score for depression risk is ⩾ 20. b Perceived Stress Scale. c Mindful Attention Awareness Scale. d Suicide Behavior Questionnaire–Revised, dichotomized by the presence of suicidality (⩾ 7 total score).
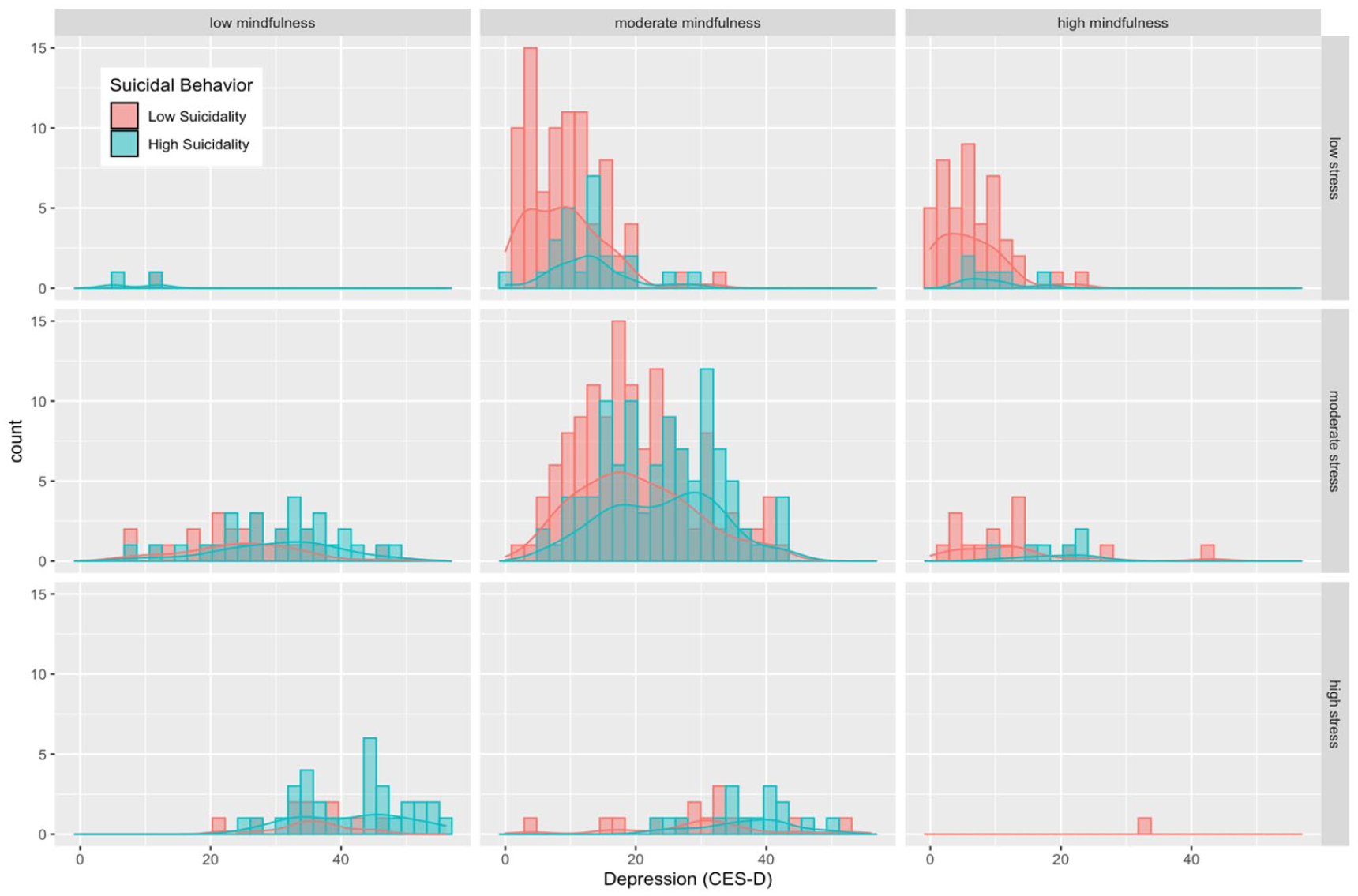
Relationship between Stress, Depressive Symptoms, and Mindfulness by Risk for Suicidal Behavior. Low, Moderate, and High Mindfulness Labels are Equivalent to MAAS Scores Ranging from 0 to 2.8, 2.8 to 4.67, and 4.67 to 6, Respectively. Low, Moderate, and High Stress Labels are Equivalent to PSS Scores Ranging from 0 to 13, 14 to 26, and 27 to 40, Respectively.
Correlation Matrix for Study Variables (n = 550).
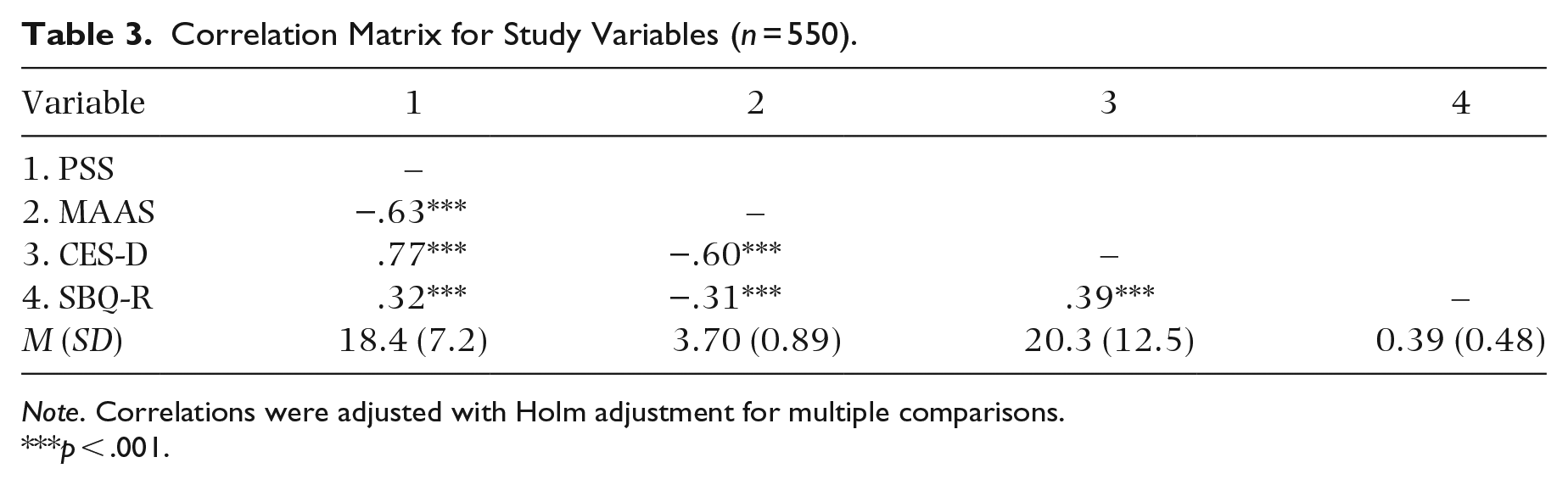
Note. Correlations were adjusted with Holm adjustment for multiple comparisons.
p < .001.
MANOVA conducted with CES-D, PSS, and MAAS as outcome measures revealed an overall significant difference between the two groups, artists and crew (Pillai’s trace = .023), F(3, 546) = 4.401, p = .004. Post hoc one-way analyses of variance (ANOVAs) revealed significant group differences for PSS, F(1, 548) = 7.175, p = .007, and MAAS, F(1, 548) = 8.556, p = .003. No significant group difference was found for CES-D, F(1, 548) = 1.275, p = .259.
To further investigate how CES-D, PSS, and MAAS in combination distinguish between artists and crew, a linear discriminant analysis was run (Table 2). The overall discriminant function was found to be significant (Wilk’s Λ = .976), χ2(3) = 13.060, p = .005, with post hoc analyses mirroring the results from the one-way ANOVAs mentioned above (CES-D was not significant). Although the linear discriminant model was found to be significant, the function’s weak squared canonical correlation coefficient (R2 = .023) indicates that PSS and MAAS are not meaningful predictors of group membership (Barcikowski & Stevens, 1975; Sherry & Henson, 2005; Tabachnick & Fidell, 1996). Finally, no significant difference was found between artists and crew on a χ2 test of independence comparing SBQ-R cutoff scores, χ2(1) = 0.091, p = .762. Based on these statistical tests, a combined data set (n = 550) of artists and crew members was used for the main analyses. Moreover, the demographic variables listed in Table 1 did not have a significant impact as covariates, and were therefore excluded in the final mediation and moderated-mediation analyses.
Mediation and moderated-mediation models
Figure 1 illustrates the mediation model and reports the results. PSS was a significant predictor of CES-D (a = 1.337, p ⩽ .001). CES-D significantly predicted the presence of SBQ-R (b = 0.062, p ⩽ .001), and the direct effect of PSS on SBQ-R was not significant (c′ = 0.018, p = .366). The indirect effect (product of path coefficients for the mediating pathway) was significant with CES-D as the mediator (ab = .083, 95% BCa CI [0.052, 0.120]).
Table 4 provides results from the moderated-mediation analysis. Similar to results from the mediation analysis, CES-D was a significant predictor of suicidality (b) and the direct effect of PSS (c′1) was not. Perceived stress remained a significant predictor of depressive symptoms (a1). The conditional direct effect at values of the moderator (c′1 + c′3 W), MAAS, did not significantly predict SBQ-R. However, the conditional indirect effect ((a1 + a3 W)b) of MAAS on SBQ-R did reach significance (index of moderated mediation, a3b = −.007, 95% BCa CI [−0.013, −0.002]). Figures 4 and 5 illustrate the effects of stress mediated through depressive symptoms on suicidality ((a1 + a3 W)b) and perceived stress on depressive symptoms (a3) attenuated by the moderator (trait mindfulness). The significant conditional indirect effect of trait mindfulness on suicidality is also reported in the bottom section of Table 4, which shows the indirect effect of PSS through CES-D decreasing as the value of MAAS increases in units of standard deviation.
Conditional Process (Moderated-Mediation) Analysis (n = 550).
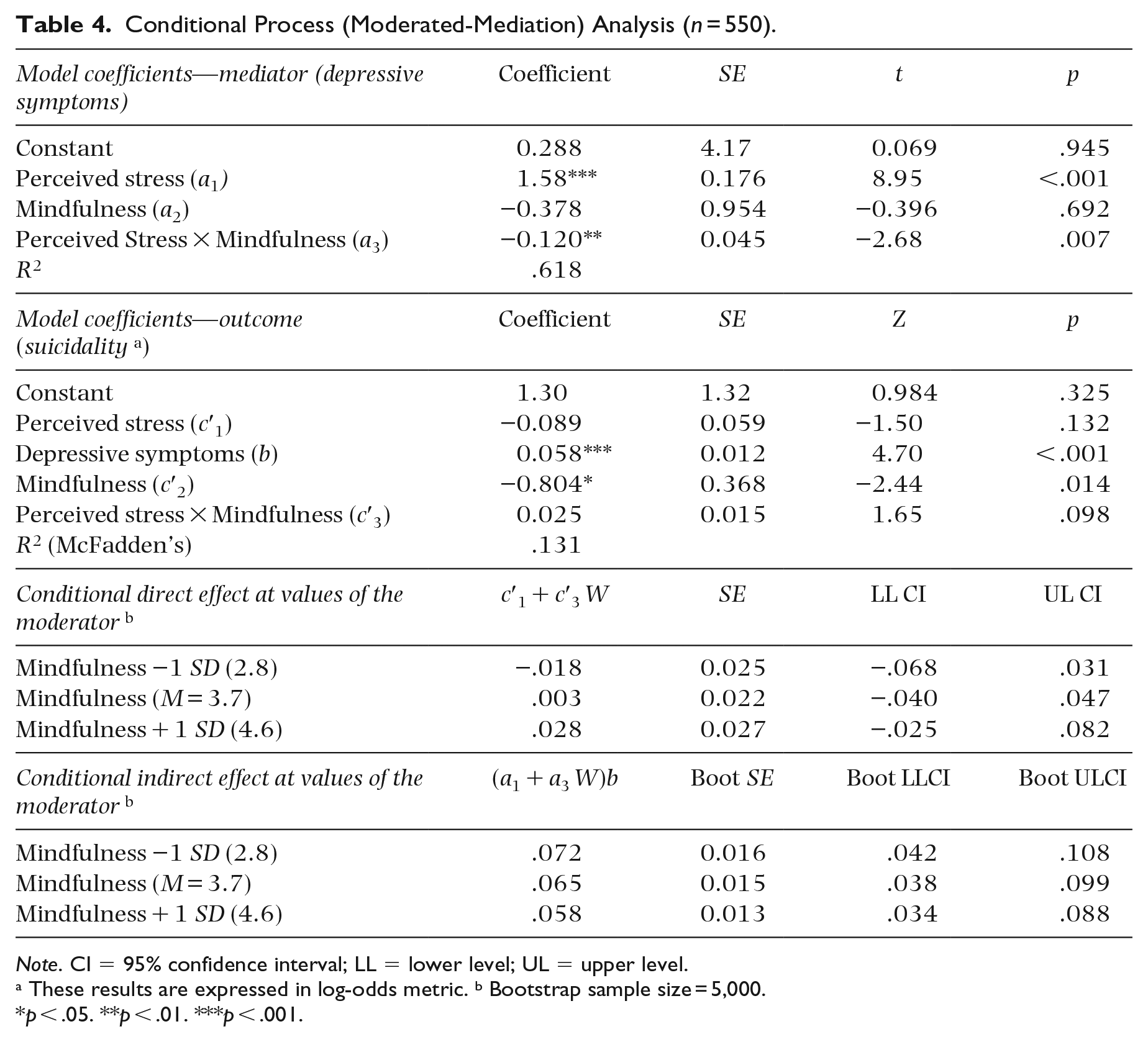
Note. CI = 95% confidence interval; LL = lower level; UL = upper level.
These results are expressed in log-odds metric. b Bootstrap sample size = 5,000.
p < .05. **p < .01. ***p < .001.
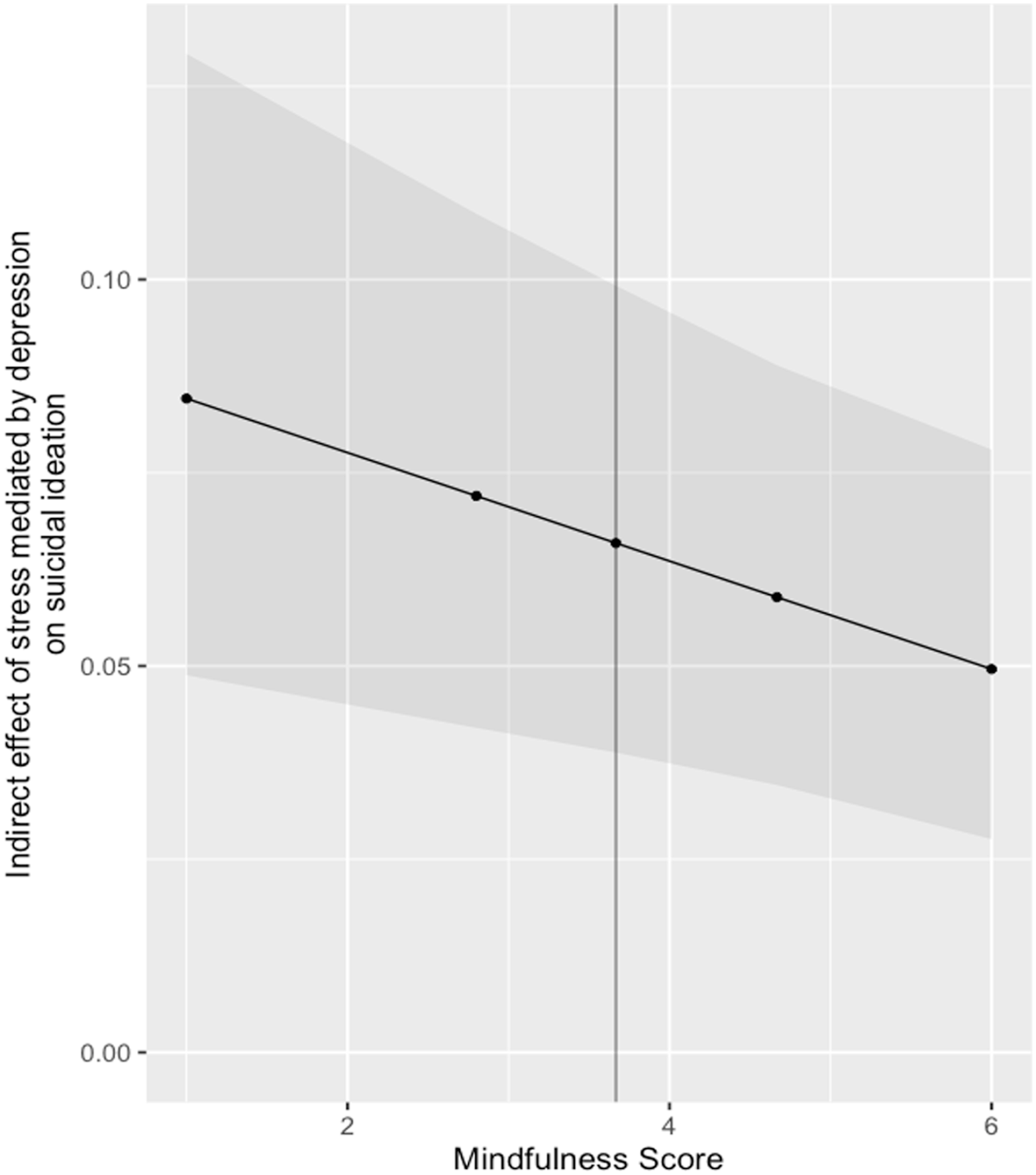
The Indirect Effect of Stress on Suicidal Ideation Mediated Through Depressive Symptoms, Moderated by Levels of Mindfulness. Dark Vertical Line Represents the Mean Mindfulness Score of 3.7. Dark Gray Region Represents the Upper and Lower Limits of the BCa 95% Confidence Interval, Which Was Obtained with a Bootstrap Sample Size of 5,000.
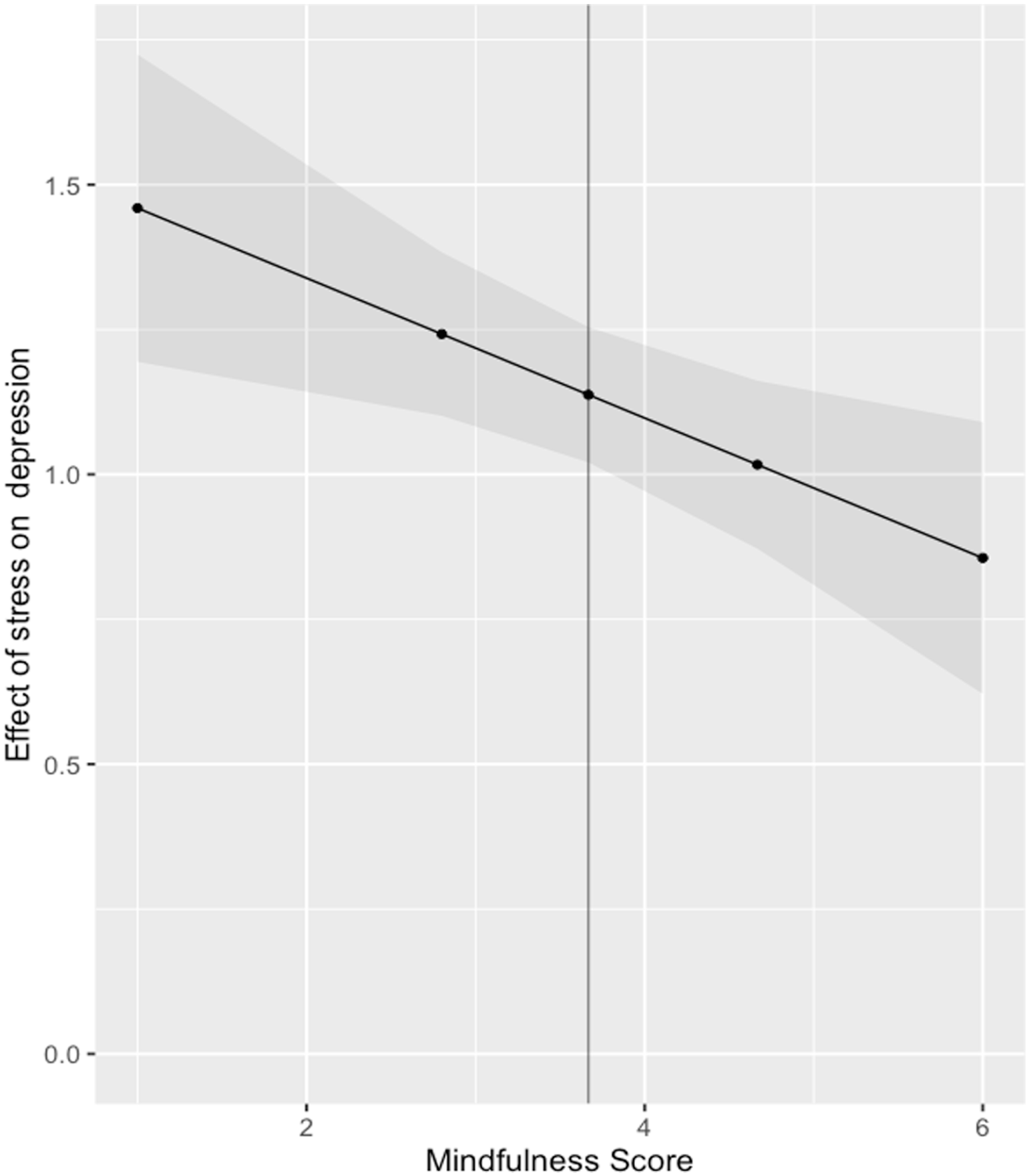
The Effect of Perceived Stress on Depressive Symptoms at Values of Mindfulness. Dark Line Represents the Mean Mindfulness Score of 3.7. Dark Gray Region Represents the Upper and Lower Limits of the BCa 95% Confidence Interval, Which Was Obtained with a Bootstrap Sample Size of 5,000.
Discussion
Mirroring the descriptive study (Newman et al., 2022), 50% of the sample qualified as high risk for clinical depression. This percentage is higher than depression risk in a range of populations of various ages and cultural backgrounds (Cheung et al., 2007; Dozeman et al., 2011; Long Foley et al., 2002). The 39.6% rate of suicidality within this sample was higher than a 15% rate found in a sample of 10,368 U.S. adults, using a SBQ-R cutoff score of ⩾ 7 (Fitzpatrick et al., 2020). Participants’ mean perceived stress score of 18.4 classifies them as moderately stressed and at high risk for medical complications (Cohen, 1988; Epel et al., 2004; Maes et al., 1999; Malarkey et al., 1995). Moreover, the participants’ mean trait mindfulness score of 3.7 was below levels found in the general populations of the United States and Canada whose mean scores ranged from 3.97 to 4.45 (K. W. Brown & Ryan, 2003; Carlson & Brown, 2005), and closer to scores found in clinical populations diagnosed with anxiety disorders (Barajas & Garra, 2014).
The current study demonstrates the positive relationships that exist between stress and depressive symptoms, and depressive symptoms and suicidality among touring professionals, and supports longstanding research findings about the associations of these variables (Arria et al., 2009; G. K. Brown et al., 2000; Kendler et al., 1999; Yurgil et al., 2021). The mediation effect of depressive symptoms depicted in Figure 1 suggests that diathesis-stress models that posit stress as a trigger for depressive symptoms leading to suicidal behavior (Beck et al., 2006; Joiner, 2005; Klonsky & May, 2015; O’Connor, 2011) are relevant to this population, and may be an important research topic when developing effective interventions for music industry touring professionals.
The current study’s findings also demonstrate a moderating impact of trait mindfulness on the relationships between stress and depressive symptoms and between stress and suicidality. The resulting indirect effect on suicidal behavior at various levels of trait mindfulness lends credence to M. M. Linehan’s (2018) emphasis on affect regulation’s role in suicidal behavior. It also supports the attenuating effect of trait mindfulness on psychiatric symptoms (Bränström et al., 2011; Carlson & Brown, 2005; Martin et al., 2018) and supports Kabat-Zinn’s (2009) notion that mindfulness may cushion the blow of stressful environments and experiences. These findings also have specific implications for workplace interventions to treat psychiatric symptoms, especially within the touring industry and other high-stress professions, such as the healthcare industry (Lewis-Hathaway & Eubanks, 2016). Although studies have found support for MBIs in the workplace, especially their ability to reduce perceived stress (Bartlett et al., 2019; Glomb et al., 2011; Raab, 2014), none to our knowledge have investigated their efficacy in the touring industry. This type of intervention could be valuable given the moderating impact of trait mindfulness found in this study, the stressful nature of touring life, and the low levels of trait mindfulness in the touring population compared with the general population.
Strengths, limitations, and future research
This study has several strengths. Although there have been studies that assessed mental health issues in the touring music industry, few have used multiple validated psychosocial instruments. The current study included a large sample with participants from around the world. To minimize potential effects of the coronavirus disease-19 pandemic on the music industry, data collection was terminated on March 15, which is around the date in which many countries implemented restrictions on travel, work, and recreational activities. The application of conditional process analysis strengthened the findings and conclusions. This study also has several limitations. The recruitment method used for the study sample resulted in a lack of representation from music genres such as rap, country, and Latin pop. Although the touring industry is typically male (60.4%) and White (73.6%; U.S. Census Bureau, 2017), the sample’s lack of gender and ethnic diversity limit the findings’ generalizability. Participants were not asked whether they were currently working on a tour while filling out this questionnaire, which might have influenced their responses to some items in the survey. The cross-sectional design of this study limited the ability to make direct statements of causality. A prospective MBI study would be required to demonstrate the attenuating effects of mindfulness on stress, depressive symptoms, and suicidality. Furthermore, any future MBI study should consider using interventions that are empirically supported, as some mindfulness researchers have warned about potential downsides of mindfulness techniques when improperly utilized (Shapiro et al., 2018). Finally, using self-report instruments led to substantial amounts of missing data that contributed to a smaller sample size than intended.
Additional variables that focus on quality of life and general functioning should be included in future research to determine the long-term effectiveness of MBIs for this population. This would require 6-month to 2-year follow-up assessments to examine levels of remission and relapse. Moreover, more clinical instruments (Patient Health Questionnaire–9, Beck Depression Inventory, Beck Scale for Suicide Ideation, Scale for Suicide Ideation) should be employed in future investigations. Adding an additional mindfulness scale, such as the Five Facet Mindfulness Questionnaire, would add important elements of convergent validity. In addition, future work should investigate the impact of lifestyle and workplace stressors found in this population on mental health outcomes.
Conclusion
This study highlights the potential role trait mindfulness can play in better understanding suicidal behavior among touring professionals in the music industry. It also provided further support for diathesis-stress and affective dysregulation models of suicidality by identifying the positive relationships between perceived stress, depressive symptoms, and suicidal behavior. Developing and implementing MBIs in the touring industry and other high-stress professions that have elevated levels of psychopathology may be an effective way to improve mood and reduce suicidal behavior, and to help individuals “ride the waves of stress” as Kabat-Zinn has eloquently described.
Footnotes
Data availability statement
The data set analyzed in the present study is available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Chayim Newman, Vance Zemon, Ryan P. George, and Tim Beitz are principals in THRIV LLC which initiated the current study. Zachary Bergson has no conflict of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by THRIV LLC.
Ethics approval and consent to participate
This study was conducted in accordance with the principles of the Declaration of Helsinki and the protocol was approved by the institutional review board at the Biomedical Research Alliance of New York (Brany; Lake Success, NY). Online informed consent was obtained from all participants.