
Abstract
Organists who start as skilled pianists may later maladapt their keyboard technique to play the organ. This randomized controlled study investigated the feasibility of using an audio cognitive intervention to correct organists’ playing technique. Forty participants played a music excerpt with two dynamics (soft/loud) on two musical instruments (organ/piano) at baseline, while their corresponding forearm muscle activities were measured by surface electromyography (sEMG). They also rated their playing force. Participants were then randomized to receive either a 5-min audio cognitive intervention (learning to use self-talk phrases “organists—stops/ expression pedals—minimal force” to reduce their tension in playing the organ; n = 21) or a control audio recording (instructing them to rest for 5 min; n = 19). All participants then repeated the two dynamics on the two musical instruments. The intervention group displayed significantly lower forearm sEMG muscle activity during organ playing, whereas the controls’ playing was unchanged. Our study shows that organists use unnecessary muscle tension to produce dynamics and that our intervention was effective and could improve motor control in playing the organ. Self-talk is therefore a viable way for music educators to help learners correct habitual but maladaptive techniques arising from prior learning.
The majority of pipe organists learn the piano, a similar instrument, before they start playing the organ; therefore, it is likely that learning on one is transferred to the other. According to Thorndike and Woodworth’s (1901) theory of identical elements, the extent of transfer depends on the similarities between two conditions (in this case, musical instruments). Notably, the more identical they are, the more transfer there will be. Therefore, one possibility is that organists transfer techniques they acquired while playing the piano to their organ playing. In many instances, such transfer is positive because previous learning in one condition facilitates the learning in another. For example, a pianist who has developed bimanual coordination to play the manual keyboard would need to master additionally only the techniques of using feet to play organ pedals, whereas learning to play the organ with hands and feet would be a completely new skillset for a non-keyboardist such as a violinist. In this study, we focus on potential negative transfer whereby previous experience in piano playing hinders organ playing technique. In particular, it has been suggested that organists may have acquired a piano technique in which they vary their muscle tension to produce different dynamics (loudness in music; as cited in Dillard, 1998, p. 452), which is unnecessary for playing the organ.
Pianists change the music’s loudness by varying the amount of energy used to strike keys (and therefore the energy with which a hammer hits the piano strings; Kinoshita et al., 2007). However, the mechanism by which an organ produces loudness is independent of the force with which the keys are struck: the loudness of the organ is altered using stops and expression pedals, which control the number and type of pipes through which pressurized air flows (Gleason, 1937). Therefore, attempting to produce dynamics on the organ by varying muscle tension is redundant and potentially maladaptive, because playing forcefully (in loud music) elicits increased muscle loading and risk of strain injuries (Furuya et al., 2011).
The development of techniques for playing dynamics on keyboard instruments (in our case, piano and then organ) can be illustrated using Fitts and Posner’s (1967) skill acquisition model, which has been used to explain the process of developing expertise in musicians (Hallam & Bautista, 2012). The model suggests a three-phase learning process in humans, namely the cognitive, associative, and autonomous phases. In the cognitive phase, learning is conscious. Pianists (who later become organists) learn the meaning of dynamics symbols explicitly and understand that the loudness of notes produced on a piano is positively related to their keystroke tension. During the associative phase, pianists start to “proceduralize” (make associations) between visual stimuli (dynamics symbols), knowledge (meaning of symbols), and response (playing tension). Over time and repeated practice, the skill is acquired and can be performed spontaneously (autonomous phase) such that the visual-motor response does not require conscious thought (Ashby & Crossley, 2012). According to this model, when a pianist (organist) reads a dynamics symbol on the score (e.g., ff-fortissimo; meaning: very loud), that stimulus automatically triggers an associated muscle tension to play the keys (e.g., a greater tension), bypassing the process of linking meaning (“very loud”) to the symbol at a cognitive level. It is likely that organists who previously trained as pianists may intrinsically develop this automatic response and transfer it to their organ playing.
Playing-related musculoskeletal disorders (PRMDs) are symptoms that interfere with musicians’ ability to play an instrument, including but not limited to pain, weakness, numbness, and tingling (Zaza & Farewell, 1997). Although no study has specifically examined the prevalence of PMRDs in organists, systematic reviews revealed that PMRDs ranged between 39% and 87% in adult musicians (Zaza, 1998) and 26% and 93% in pianists (Bragge et al., 2006). Organists share common risk factors for PRMDs with pianists, such as prolonged practice (> 4 hr per day), playing forcefully, and anxiety traits (Furuya et al., 2006). Furthermore, the physical disparities in layout and design from one organ to another may create additional risks amongst organists, for example, organists may need to reach keyboards placed at different heights (Loman, 2004). The virtuosity of making music with four limbs means that organists can be likened to “musical athletes,” but with an aesthetic character comparable with dance and gymnastics (Yearsley, 2012). Accordingly, it can be inferred that organists are at risk of PRMDs just as are pianists and other musicians.
The general population may be conditioned to think “louder” means having to use “greater muscle force,” because in everyday interactions greater force is usually required to create greater excitation of physical objects and therefore increased loudness. We acknowledge that organists who did not start to play piano before organ may also associate different muscle force with the production of different levels of music loudness. Nevertheless, one motivation for us to understand the transfer of techniques for playing dynamics from piano to organ is that this may place organists at an increased risk of musculoskeletal injury. If organists can be made aware that they are using extra muscle force when playing loudly, and if this redundant playing force can be reduced, then so too will the risk of injury.
Given the above, we carried out a study to determine: (a) whether the potential (negative) transfer of technique in playing dynamics existed among organists as measured by comparison of forearm muscle activity and self-reported playing force when playing piano and organ; and (b) the feasibility of a researcher-developed cognitive intervention to reduce organists’ unnecessary playing tension (if any).
Method
Research design and sample size
The study protocol was approved by and administered following the institutional ethics review board of the University of Sheffield. Forty participants were recruited for this double-blinded randomized controlled trial (RCT). The sample size was based on a prior study from which our intervention was developed (Bellomo et al., 2020).
Participant recruitment
Potential participants were recruited by convenience sampling. Individuals who learned to play piano before organ were included regardless of their level of experience in organ (and piano) to increase the generalizability of the findings; people were excluded if they had a pacemaker implantation. During a screening questionnaire, if participants indicated presence of a PRMD (as defined by Zaza and Farewell, 1997) in the upper limbs in the last 7 days, the experiment was postponed or the participant was excluded. Participants were informed of their inclusion, collection/use of data, and publication.
Pre-experiment preparation
After providing written consent, eligible participants received the same experiment music score via email 2 weeks prior to the experimental session. Participants were encouraged to practice until they felt confident in playing the piece. They were informed that they would be asked to play the piece a few times on piano and organ during the session. They were also reminded to use consistent fingering, articulation, and tempo in each rendition and to bring the annotated score.
Experimental procedure
The experiment was conducted in a music practice room that housed a grand piano (Karl Müller model G175) and a classical electronic organ (Johannus Studio 150), as illustrated in Figure 1. To eliminate any variability in sound intensity caused by the organ sound effects, participants were not allowed to change the pre-setting of the organ cathedral (“echo”) and volume knobs.
Experimental Setup—Piano (Left) and Organ (Right).
An investigator, who was a registered nurse, attached eight pairs of wireless surface electromyography (sEMG) electrodes to bilateral fingers/wrist flexors and extensors. Participants started with a 10-min warm-up to familiarize themselves with the musical instruments and apparatus they were wearing and to adjust the benches to comfortable height/positions. Subsequently, their elbow angles on the piano and organ (Great manual) keyboards were measured with a goniometer by holding a D minor triad (notes D4, F4, and A4) with the right hand (first, third, and fifth fingers). As participants needed to change seats to play two instruments, their elbow position was reconfirmed to the respective measured angle before each experimental trial so as to eliminate potential confounder of wrist/forearm positioning on sEMG signals (Oikawa et al., 2011).
Experimental trials and manipulation
All participants played an identical music excerpt in four trials repeated twice: four at pre-test and four at post-test. Participants received a written instruction before each trial that indicated which dynamics to play and on which instrument, including (a) pp-pianissimo (meaning very softly) on organ, (b) ff-fortissimo (meaning very loudly) on organ, (c) pp-pianissimo on piano, and (d) ff-fortissimo on piano. The order of playing was randomly assigned without repeating among participants.
Following the four pre-test trials, participants drew one of two tokens (marked “1” and “2”) to be randomly assigned to either an intervention group or a control group. After the investigator exited the music room, the participant clicked the respective number on an iPod to play an audio recording. Participants listened to a 5-min cognitive intervention audio (n = 21) or a control audio (n = 19) that instructed them to take a 5-min break. The investigator was blinded to the group assignment, while participants were blinded to the other audio recording. The experimental trials and manipulation are shown in Figure 2.
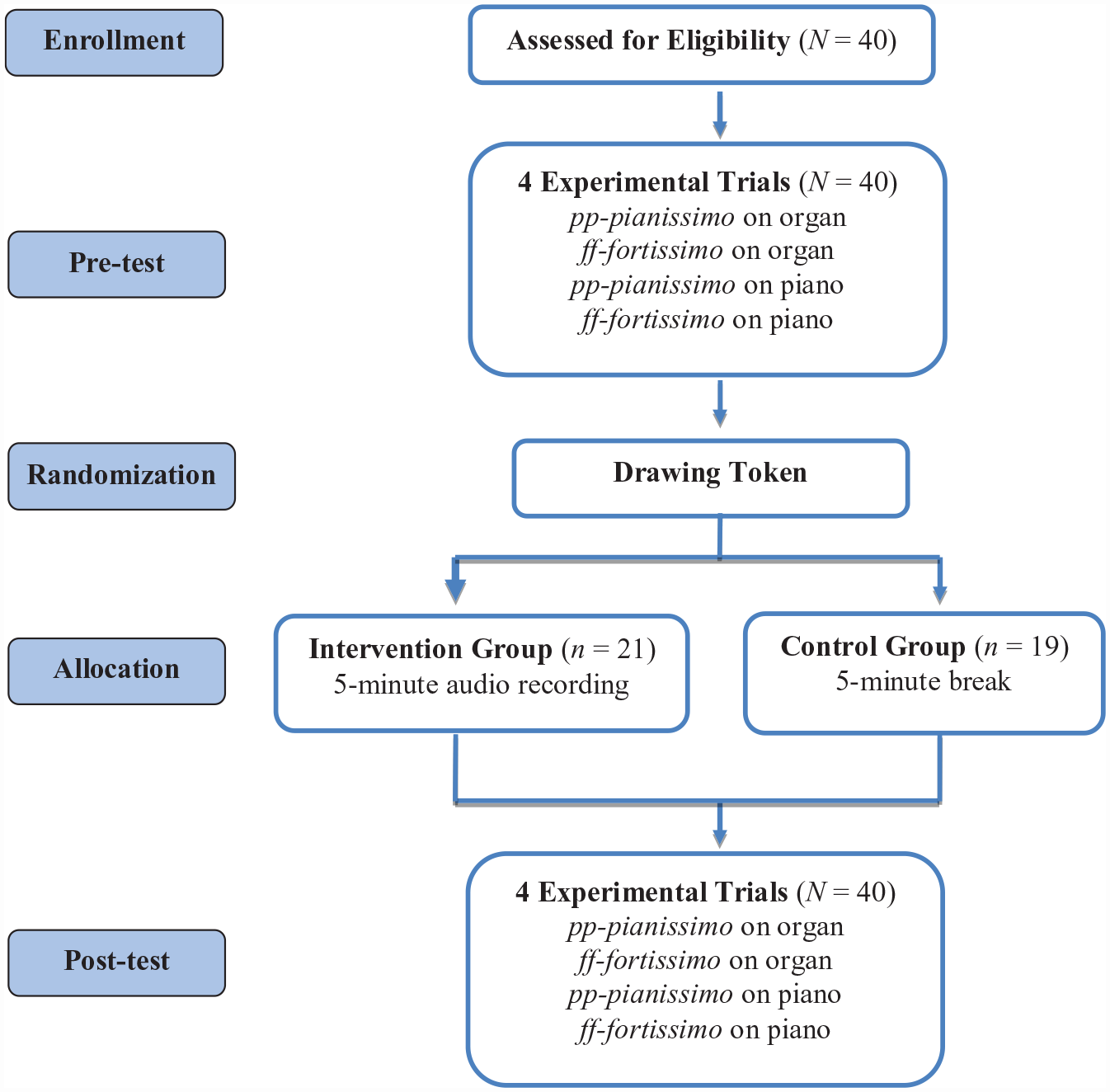
Flow Diagram of the Randomized Controlled Trial.
Data collection
The participant’s forearm muscle activities during the eight experimental trials were recorded by the sEMG, while the respective sound intensity was measured by a sound level meter. In addition, participants put on one wireless earphone on the preferred side for a “click” track (92 clicks/min for the set tempo of the music). Corrections to playing errors were not essential as accuracy was not the focus of the current study, however, the trial could be rerecorded upon participants’ request. Seven participants requested to replay a trial and nine trials (out of 320 trials) were remeasured. All participants took a 3-min break between playing each experimental trial. They completed a self-reported questionnaire after playing the eight trials.
Music (experiment score)
The music excerpt “Vieux Noel” in D minor was taken from César Franck’s L’Organiste: Fifty-Nine Pieces (Kalmus edition). It was chosen because it is a piece of standard repertoire written for organ, and has an estimated level of difficulty which would make it moderately easy to play by a competent organist (comparable with Associated Board of the Royal Schools of Music [ABRSM] Grade 5). A few minor amendments were made to the score to satisfy the research purpose. Notably, to ensure consistency between participants, all registration and division markings, and expression markings (e.g., tempo, dynamics, and articulation markings) were deleted and replaced with the division label “Manual” (meaning: play with hands) and a single tempo marking “♪ = 92.” In addition, the dotted quavers in the bass clef on the second beat of bars 3, 7, and 25 were changed to double dotted quavers based on our organ experts’ opinion that the original rhythm was likely to be a publication error.
Cognitive intervention
The cognitive intervention aimed to mitigate the muscle tension of organists when they played the music with different dynamics. It was derived from a cross-disciplinary approach, integrating the insights from cognitive psychology and sports psychology. It took the form of an audio instruction, pre-recorded by an occupational therapist. This intervention was designed based on an assumption that organists were influenced by prior piano learning experience such that they unwittingly used a playing technique which associated different musculoskeletal tensions with the production of different dynamics. The intervention comprised two components: (a) an educational script to increase organists’ awareness of a piano playing technique which is maladaptive to the requirements of organ playing and (b) self-talk to facilitate change of the maladaptive technique. Participants were instructed to say the phrase “organist—stops/expression pedals—minimal force” silently before playing on the organ. This self-talk phrase was formulated following a similar approach described by Bellomo et al. (2020). The theoretical background and conceptualized framework for developing the intervention and the audio script are included in the Supplementary Material.
Subjective and objective measurements
Self-reported questionnaires
An 11-point numeric rating scale was used to assess participants’ self-perceived degree of force in playing each trial, where a score of 0 = minimal force and 10 = maximal force. Participants gave ratings after completing the eight experimental trials to reduce pre-test sensitization and experimenter-expectancy effects. In addition, participants rated the perceived level of easiness of the music and the level of confidence in their playing on two 5-point scales, ranging from 0 = not very easy to 5 = very easy and 0 = not very confident to 5 = very confident, respectively. They were also asked how much time they spent rehearsing the music and on which instrument(s).
Sound level
To ensure the participants’ compliance with instructions and production of dynamics, a digital sound level meter Benetech GM1353B (sound range: 30–130 dB; accuracy: ± 1.5 dB) was used to measure real-time sound intensity at 200 ms intervals. The meter was vertically hung on a tripod stand between the piano and the organ, and Bluetooth-connected to a data-logging application. The sound level data for each trial were retrieved and a mean value was calculated.
sEMG muscle activity
A sEMG system (Ultium EMG, Noraxon, USA) recorded signals at a sampling rate of 2000 Hz wirelessly from four bilateral forearm muscles that are responsible for the fingers and the wrist movements, including the left (Lt) and right (Rt) extensor digitorum communis (EDC), extensor carpi radialis (ECR), flexor digitorum superficialis (FDS), and flexor carpi radialis (FCR). Although sEMG is not a direct measure of force (Hof, 1997), a higher amplitude of the sEMG signal indicates higher muscle activity (Oikawa et al., 2011).
After skin preparation by scrubbing with 70% isopropyl alcohol, bipolar Ag/AgCl electrodes with 2-cm inter-electrode distance were placed in a direction parallel to the muscle fibers for signal optimization (Maxwell, 2015); sEMG sensors were fixated on the skin using surgical tapes to minimize movement noise (Roy et al., 2007). Then, the signal quality was checked with the sEMG system’s built-in monitor. The above procedure was repeated if the red indicator flagged up (i.e., impedance > 100 kΩ, or root-mean-square value > 5 uV and the median frequency = 50 or 60 ± 3 Hz).
Prior to the data collection, all participants underwent maximum voluntary contraction (MVC) tests to obtain peak activation of each muscle for the normalization purpose. For each MVC test, participants maximally contracted the target muscles against manual resistance for 3 s thrice. A 30-s rest was given between exertions to avoid fatigue (Chi et al., 2021). All tests were demonstrated. Verbal encouragement was given during the tests to optimize the maximum activation (see Supplementary Material for the function, electrode placement, and MVC test method for each muscle).
sEMG data processing
The raw sEMG signals were pre-processed using the Noraxon MyoResearch software (version 3.16). Signals were bandpass filtered between 20 and 500 Hz, full-wave rectified, and smoothed with a 30 ms window (Chong et al., 2015; Oikawa et al., 2011; Wristen et al., 2006). The peak amplitude obtained from each muscle in the MVC tests was identified moving a 1,000 ms window and set as 100%MVC. To allow within- and between-participant comparisons (Halaki & Gi, 2012), the sEMG signals collected in the eight experimental trials were normalized to the respective muscle amplitude, averaged, and expressed as the percentage of MVC (%MVC). Therefore, 64 sEMG data (8 muscles × 8 trials) were computed for each participant. Of those 2,560 sEMG data (64 × 40 participants), three contaminated data were not included in the analysis.
Statistical analysis
The data were analyzed using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA). For inferential statistical tests, the significance level was set at .05. Between-group baseline characteristics were compared using independent t-tests (for continuous data) or χ2 (for nominal data).
The variables, self-perceived force, eight sEMG signals, and sound level, were analyzed separately. To answer the first question, whether a difference in playing force exists between dynamics on the organ and whether this is the same as used in producing dynamics on the piano, dependent t-tests were performed on pre-test data to examine the differences between dynamics (pp-pianissimo/ff-fortissimo) for each instrument (organ/piano). To test the effectiveness of the intervention (second aim), a three-way repeated-measures analysis of variance (ANOVA) was performed on the data from the organ trials with inclusion of the factors dynamics (pp-pianissimo/ff-fortissimo), time (pre-test/post-test), and group (intervention/control). When significant dynamics × time × group interaction were identified, a two-way repeated-measures ANOVA was conducted separately for each group. If a significant dynamics × time interaction occurred, post-hoc dependent t-tests were performed to understand the effect of time by dynamics. To reduce type I error in multiple pairwise comparisons, Bonferroni correction was used to adjust the significance level.
Transparency and openness
The data and research materials supporting this publication can be freely downloaded from the University of Sheffield Research Data Repository at https://doi.org/10.15131/shef.data.19188161.v2, under the terms of the Creative Commons Attribution (CC BY) license. This study’s design and its analysis were not pre-registered.
Results
Characteristics of participants
Forty organists (27 females and 13 males) with a mean age of 30.9 years (SD = 7.9 years) participated in this experiment. The majority of participants, 92.5% (n = 37) were Chinese (Hong Kong) and 85.0% (n = 34) received a bachelor’s degree or higher in any field. Participants played the piano for an average of 23.7 years (SD = 7.3) and organ for 6.0 years (SD = 5.6). They started learning to play the organ approximately 17.5 years (SD = 6.7) after the piano. Over the last 12 months, these participants on average spent around 2 hr per week playing the piano and organ, respectively. In addition to piano and organ, participants on average played 1.3 instruments (SD = 1.1).
Table 1 presents the participants’ baseline characteristics. The intervention and control groups showed no significant difference in participants’ characteristics, the time they spent practicing the experiment music, or perceptions about the music (ps > .05).
Characteristics of Participants (N = 40) in the Intervention and Control Groups.
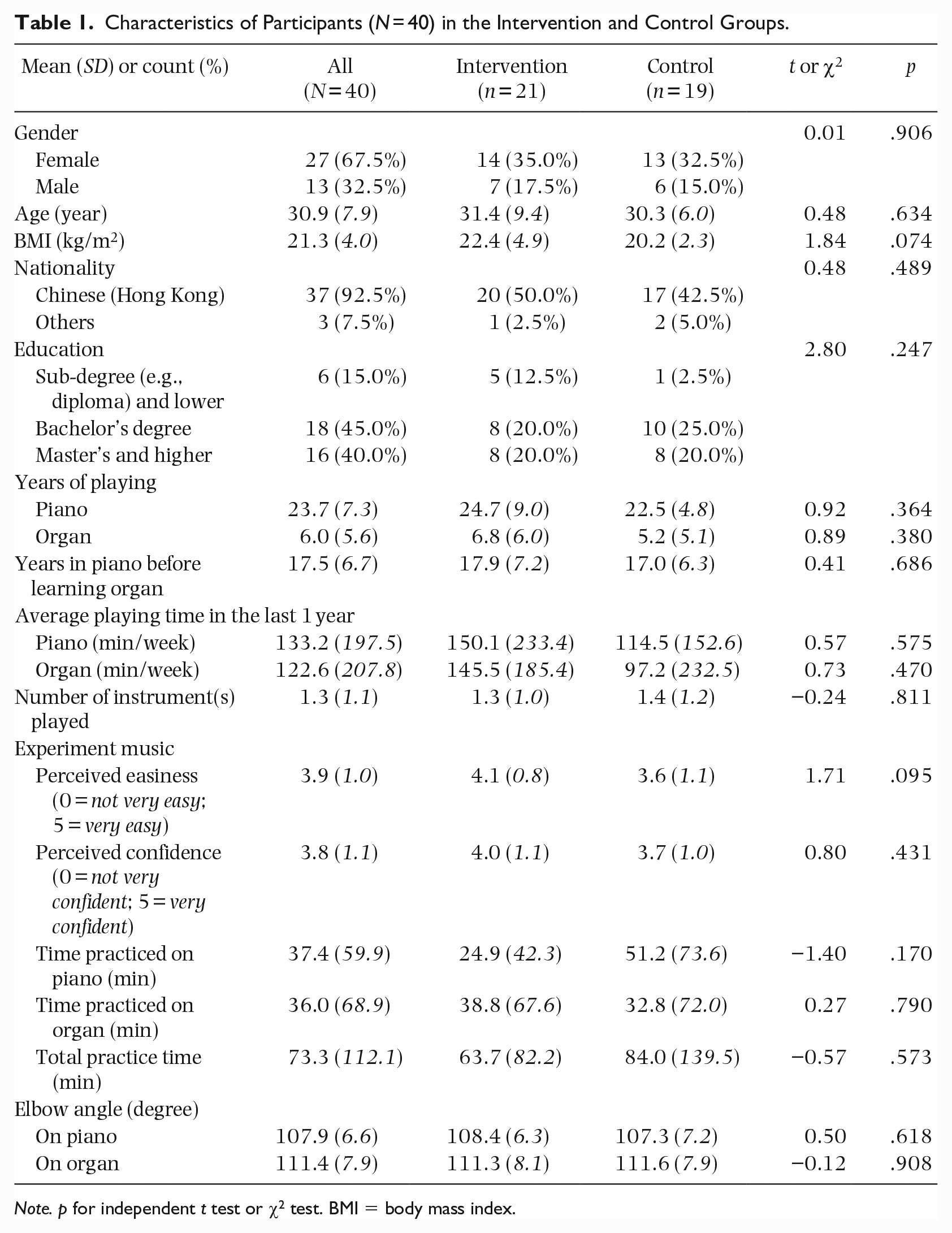
Note. p for independent t test or χ2 test. BMI = body mass index.
The transfer of learning: pp-pianissimo versus ff-fortissimo in organ/piano
The self-perceived force, sEMG signal of all eight muscles, and the sound level differed significantly between the two dynamics in both instruments (ps < .001; Table 2). This means that no matter which instrument participants played, they exerted more tension to play the music ff-fortissimo than pp-pianissimo.
Mean (SD) Self-Perceived Force and Surface Electromyography (sEMG) for pp-pianissimo and ff-fortissimo in Organ and Piano (N = 40).
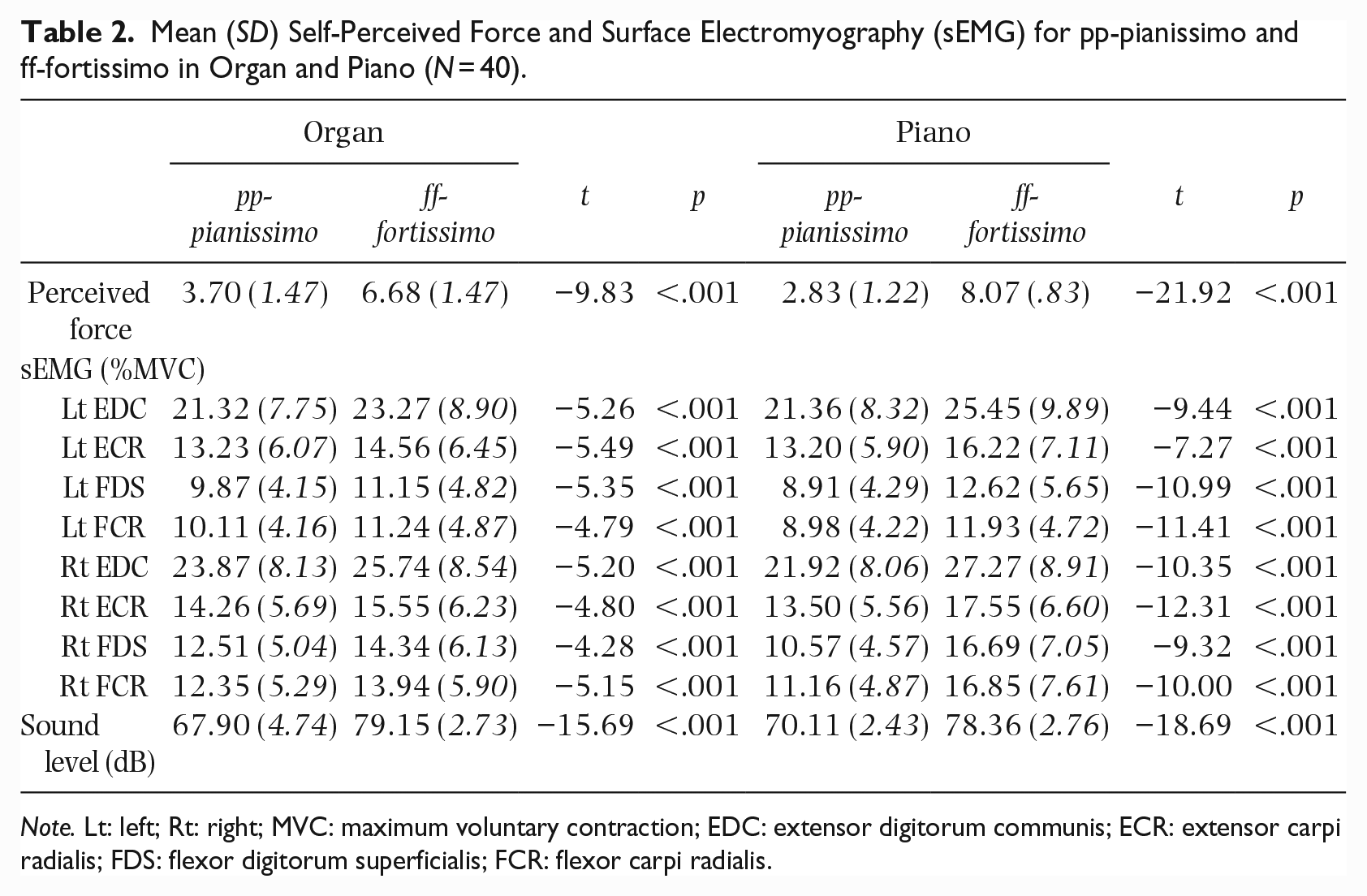
Note. Lt: left; Rt: right; MVC: maximum voluntary contraction; EDC: extensor digitorum communis; ECR: extensor carpi radialis; FDS: flexor digitorum superficialis; FCR: flexor carpi radialis.
The effects of the cognitive intervention
Three-way repeated-measures ANOVA showed that there was significant Dynamics × Time × Group interaction in self-perceived force and sEMG data of seven muscles (Lt EDC, Lt ECR, Lt FDS, Rt EDC, Rt ECR, Rt FDS, and Rt FCR; ps < .05), but not for Lt FCR (p = .081; Table 3). A subsequent two-way ANOVA test on self-perceived force and the seven named muscles revealed that there was a significant Dynamics × Time interaction in the intervention group (ps < .025), while these measures remained non-significant in control participants (ps > .025; Table 3).
Summary Table for Three-Way and Two-Way ANOVA Tests.
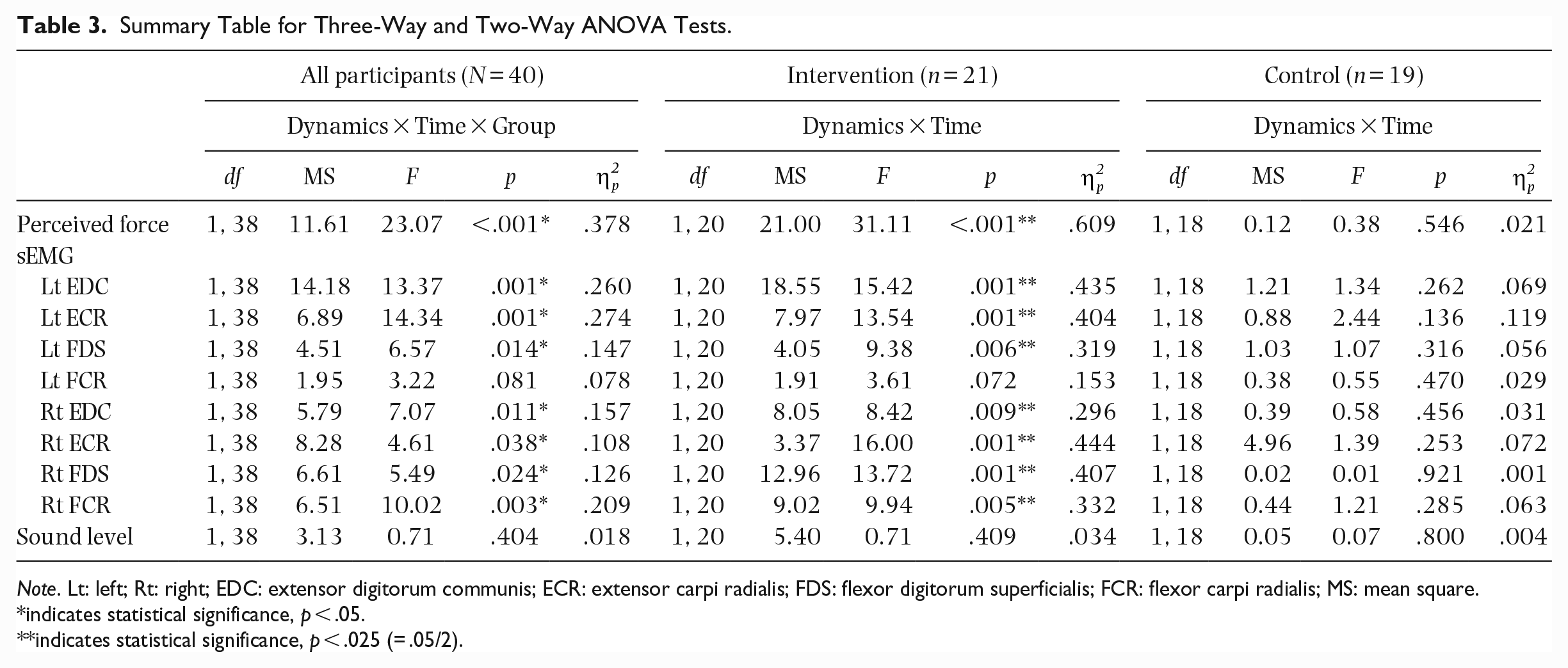
Note. Lt: left; Rt: right; EDC: extensor digitorum communis; ECR: extensor carpi radialis; FDS: flexor digitorum superficialis; FCR: flexor carpi radialis; MS: mean square.
indicates statistical significance, p < .05.
indicates statistical significance, p < .025 (= .05/2).
Post hoc dependent t tests were performed for the intervention group, separately for each dynamic (Table 4). The results indicate that when the dynamics were pp-pianissimo, there was a significant decrease in sEMG activities of six muscles (Lt EDC, Lt ECR, Lt FDS, Rt EDC, Rt ECR, and Rt FCR) after the participants learned the cognitive intervention (p < .017), although there was no significant difference in the self-perceived force (p = .629). When the dynamics were ff-fortissimo, the intervention group displayed significantly lower self-perceived playing force (p < .017) and sEMG muscle activity (seven muscles; p < .017) at post-test than at pre-test.
Mean (SD) Self-Perceived Force and Surface Electromyography (sEMG) Between Pre-Test and Post-Test Organ Trials by Dynamics in the Intervention Group (N = 21).
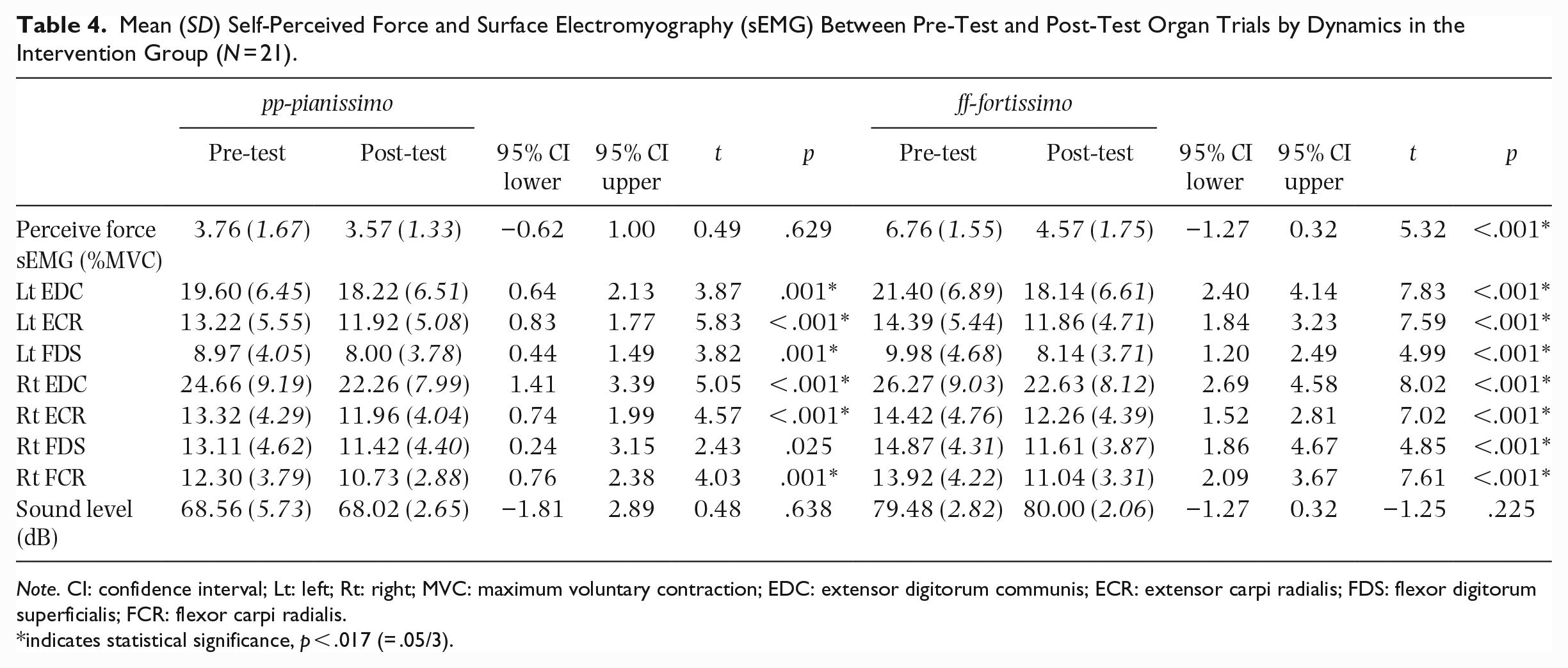
Note. CI: confidence interval; Lt: left; Rt: right; MVC: maximum voluntary contraction; EDC: extensor digitorum communis; ECR: extensor carpi radialis; FDS: flexor digitorum superficialis; FCR: flexor carpi radialis.
indicates statistical significance, p < .017 (= .05/3).
Discussion
In this study, subjective (self-reported) and objective (sEMG) measurements of playing force on piano and organ substantiated that this element of organists’ technique for playing dynamics was the same as that used in their piano playing, despite the redundancy of this technique for organ playing. Also, both the self-reported and sEMG results evidence the feasibility and effectiveness of our newly developed cognitive intervention in reducing the muscle tension of organists when playing organ music.
This was the first study to investigate the transfer of learning of dynamics across instruments (from piano to organ), rather than the transfer of skills on a single instrument (piano) across changes in musical features (tempo and melodic/sequential change; Duke & Pierce, 1991; Palmer & Meyer, 2000). Our findings suggest the existence of a learning transfer process: participants used a similar method to play dynamics on the organ and piano, that is, using higher muscle tension to play the music loudly (evidenced by higher self-rated force and higher muscle activities) than to play it softly. Given that the majority of keyboardists started with the piano, they are susceptible to this transfer of learning. However, there are additional explanations for the observed phenomenon. First, the instruments differ in regard to popularity and accessibility: there are generally fewer organs available than pianos, and traditional pipe organs are only located in places of worship. Therefore, as well as starting by playing the piano, organists are likely to rehearse organ music on a piano. Second, the type of organs on which organists usually rehearsed on is likely to influence playing technique. We mentioned that the loudness of the organ is determined by stops and expression pedal; a general principle is that the music will be louder when more stops are added. In the case of a tracker-action pipe organ, adding stops (increasing loudness) increases the initial force required to move the keys, that is, keys are heavier (Asutay et al., 2012). Therefore, it is possible that organists acquire the technique of using altered keystroke force from playing the tracker-action organ and transfer it to play the electronic organ in our experiment. Third, the mechanism of many musical instruments and even our interactions with objects in daily life correlate loudness with force. For example, violinists use a bow on the strings with different muscle tension to alter the music’s loudness; and we use more abdominal energy to shout than to whisper. We may unintentionally associate higher muscle tension with louder sound volume.
Palmer and Meyer’s (2000) study found that the degree of learning transfer differed between skilled and novice pianists; however, our study examined a group of organists with a high level of experience in piano performance that would not be able to elucidate such an observation. All but one of our participants had obtained ABRSM Grade 8 or above in piano (one had Grade 6). They had been playing the piano for an average of 23.7 years and had a mean of 17.5 years in playing piano before starting organ. Indeed, the effort involved in coordinating four limbs means that the organ can be difficult to master and this may explain why organists first learn the piano, often for many years. Their perceptual-motor process may have been strongly conditioned already, that is, they may automatically associate different degrees of tension with key strikes upon reading different dynamics symbols. Whilst the current study used sEMG to investigate forearm muscle activities and Krakauer et al. (2006) reported that the extent of transfer in motor learning depends on the prior use of the same body parts, it would be worth investigating whether the transfer occurs in organists’ lower limbs, and whether the degree of transfer differs for organists whose prior music experiences are with an instrument other than piano and/or who learned the piano after the organ.
The sEMG data consistently supported the effectiveness of the cognitive intervention when playing both loud and soft dynamics (six muscles for pp-pianissimo and seven muscles for ff-fortissimo). This indicates that the bespoke intervention was effective in reducing organists’ muscle tension when playing music, even though they perceived themselves to be still playing with the same force between pre-test and post-test pp-pianissimo trials. The playing tension of post-intervention participants was significantly reduced when playing loud music. However, it was surprising that their muscle tension could also be reduced when playing the music softly. The analysis of the secondary variable (sound level) showed that the intervention did not affect the loudness produced. Therefore, the current intervention was effective in reducing the organists’ playing tension but not the essence of making dynamics on the organ, which can be achieved by controlling stops and/or expression pedals.
Common methods used by musicians to reduce muscle tension include the Alexander technique and the Feldenkrais method. These techniques focus on increasing the awareness of bodily usage and emphasise “effortless effort” (Peterson, 2008). To our knowledge, this was the first empirical study to investigate the novel use of a cognitive intervention on organists’ maladaptive behavior. To change the maladaptive “piano technique,” instructional self-talk was embraced to reinvest consciousness when executing the technique to play dynamics on the organ. Self-talk increases a sense of control by deploying the conscious top-down process from the brain to the motor domains (Hardy, 2006). Specifically, instructional self-talk focuses on the explicit technique and sequence in executing a skill. There is extensive evidence demonstrating its benefits for information-processing and skills performance in athletes (Hardy et al., 2015; Theodorakis et al., 2000). For example, there was increased forearm muscle activity (sEMG) in golfers who used an instructional self-talk phrase “feet still—wrist locked—arms through,” manifesting better skill in the swing phase of golf putting (Bellomo et al., 2020). Given that sports skill mastering and instrumental music playing fall under the category of procedural learning, it is plausible that self-talk can benefit both athletes and musicians. For instance, cognitive interventions comprising self-talk effectively reduced musicians’ performance anxiety (Hoffman & Hanrahan, 2012) and enhanced technical aspects of music playing (Roland, 1992).
Our cognitive intervention was cheap and easy to administer. It demonstrated good effectiveness and applicability. However, our study has several limitations. First, this study included participants regardless of their experience in organ and piano, which might have affected the accuracy and consistency in performing the experimental trials. We assumed that our participants would be highly proficient in keyboards and would have allocated adequate time to prepare for the experiment by rehearsing the music, which only required playing with the hands rather than the feet. Indeed, participants rated the technical demands of the music as easy and reported feeling relatively confident in playing it (both scoring nearly 4 points out of 5). Second, as participants were educated to say the self-talk phrase silently before playing the organ, the usage of it had to rely on self-report. It was also unclear whether our participants benefited from an increased awareness of their maladaptive technique through the intervention audio and/or cueing of the self-talk phrase. However, we expect organists who have successfully adjusted to playing the instrument with minimal muscle tension regardless of dynamics may no longer need the self-talk to cue their actions, equivalent to achieving the autonomous phase of the skill acquisition model. Third, this RCT did not evaluate the long-term effect of the intervention and cannot determine whether the intervention can serve as an injury-prevention measure.
Implications for future studies
This study adds to the music pedagogical insight that the learner’s experience on one instrument (piano) may affect their learning on another (organ). From a broader educational perspective, previous learning experiences could induce positive and/or negative effects on learning. Understanding and identifying the facilitators and barriers to this may help achieve desirable teaching and learning outcomes. Self-talk that helps trigger a conscious process can improve motor controls. This may serve as a viable way for music educators to help learners correct their maladaptive habits and techniques in other contexts.
Whilst our developed cognitive intervention can mitigate immediate playing tension among organists, replication of the current protocol with longitudinal follow-ups is essential to evaluate the long-term effectiveness of the intervention and to infer whether it can lower their musculoskeletal risks.
Supplemental Material
sj-docx-1-pom-10.1177_03057356231159194 – Supplemental material for A cognitive intervention to correct a maladaptive technique in organists due to prior music learning: A randomized controlled trial
Supplemental material, sj-docx-1-pom-10.1177_03057356231159194 for A cognitive intervention to correct a maladaptive technique in organists due to prior music learning: A randomized controlled trial by Mandy MP Kan, Nicola Dibben and Arnold YL Wong in Psychology of Music
Footnotes
Acknowledgements
The authors would like to thank the following colleagues: Dr. Emma Hock suggested a range of theoretical models for conceptualizing the cognitive intervention; Dr. Anne Cheuk-Bun Lam and Dr. Simon Sheung-Chi Chan gave advice on the music selection and refined the developed intervention; Mr. Chun-Pong Siu recorded the cognitive intervention audio; Dr. Jean Russell advised on statistical analysis.
Authors’ Note
The article has not already been published elsewhere. Some of the data that appeared in this article were presented at conferences. A brief description of this research was reported by an organ magazine as a short article. Mandy MP Kan is now affiliated to School of Nursing, The Hong Kong Polytechnic University, Hong Kong, China after submitting this article.
Data and materials availability
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.