
Abstract
Recent estimates indicate that attention deficit hyperactivity disorder (ADHD) is prevalent in about 2.5% of adults and 5.9% of young people. Negative impacts of ADHD are often reported in academic performance, emotional and cognitive functioning, and peer relationships, but little is known about ADHD and music. Using a detailed case study approach, structured observations in contrasting settings over a period of several school terms were made of one Primary and one Secondary school-aged boy, each with a formal assessment of ADHD. Analyses of video-based observations every 30 s (n = 5,961 in total) were related to (1) the particular core ADHD symptoms attributed to inattention, hyperactivity and impulsivity, together with their observed severity; and (2) tutors’ and pupils’ actions during their focus music sessions. These quantitative data enriched the qualitative analyses. The research findings indicate that, notwithstanding their ADHD-related symptoms, the affected individuals could engage successfully in music and acquire musical skills. ADHD was not a static condition, but variable according to pedagogical and musical context. Habitual ADHD symptoms were either reduced or entirely absent when participants were engaged in playing and performing music. Analyses suggest that an effective, context-sensitive and inclusive pedagogy can integrate pupils into successful individual and collective music making.
There is considerable research evidence to suggest that sustained and successful engagement in active music making can be a characteristic of neurotypical development and can also be of potential benefit to individual health and well-being (cf. Fancourt & Finn, 2019; Hallam, 2015; Jaschke et al., 2018; Knox et al., 2011; MacDonald, 2013; Welch et al., 2014, 2020; Williams et al., 2015). However, there is generally less research literature about the nature of musical behavior and the development of musically relevant skills in individuals with special educational needs and disabilities (SEND)—presumably because engagement in music for such individuals is still commonly associated with music therapy (see Ockelford, 2000, 2012).
Within the available SEND and music literature, there is evidence that people with SEND can have a successful engagement in music and, in many cases, exhibit and develop musical skills (cf. Jellison, 2012, 2015; Ockelford, 2015; Welch et al., 2009; Wilde et al., 2016). These include adults with learning disabilities (MacDonald & O’Donnell, 1994; Wilson & MacDonald, 2019), blind and partially sighted children and adults (Baker & Green, 2018; Ockelford et al., 2006), children who are deaf and hearing impaired (Petersen et al., 2012; Welch et al., 2015), and children and young people with autism (Hillier et al., 2012; Hogle, 2021; Lindblom, 2017; Stamou et al., 2019). In addition, a small number of recent studies have suggested that effective music workshop provision for young adults with learning difficulties and/or other disabilities can bring wider social and emotional benefits, such as related to self-expression, confidence, and social skills (Diaz Abrahan et al., 2019; MacGlone et al., 2020; Wilson & MacDonald, 2019).
Another important area of SEND is attention deficit hyperactivity disorder (ADHD). Following a thesis that, as a species, we are musical by design (Blacking, 1974; Gardner, 2017; Savage et al., 2020; Sternberg, 2021), it may be hypothesized that individuals diagnosed with ADHD can also successfully develop in music—as well as through music (in a therapeutic sense)—despite the characteristically challenging behavior that is commonly associated with ADHD (see below). However, within the existing literature on music with children and young people with SEND, there is very little research evidence to offer an understanding of the various aspects of ADHD in the context of musical behavior, development, and education.
Consequently, the exploratory study reported in this article aimed to offer insights into the nature of musical engagement and behavior of children and young people diagnosed with ADHD in various music education contexts, using a case study approach. In the light of growing interest in ADHD (e.g., https://adhd-institute.com), and—in particular—on the multifaceted challenges that it may bring for the affected individuals in many domains, it may seem surprising this condition has been neglected within research in the fields of music education and music psychology. This study focuses on the real-life music making of two young individuals, each with an official diagnosis of ADHD. The musical behavior of each case participant is illustrated in two separate settings, providing four contexts in total. Throughout the article, the term “behaviors” refers to observed actions of the participants, whereas “ADHD-like behaviors” and “symptoms” refers to behaviors which appear to match the reported characteristics of ADHD. Observed behaviors were interpreted in the light of the literature and subsequently assigned to a symptom (i.e., possible ADHD symptom as to the common classification systems).
An introduction into the complex nature of ADHD
In recent years, ADHD has been a subject of growing investigation in many fields, such as medicine, psychology, neuroscience, and education. It is found to be listed among neurodevelopmental disorders, psychological disorders, and mental health problems, and most often addressed in the context of children’s disorders (cf. American Psychiatric Association, 2013; Mental Health Foundation, 2015; National Institute for Health and Care Excellence, 2018; Thapar & Cooper, 2015). This multifaceted condition is commonly associated with particular “developmentally inappropriate” (American Psychiatric Association, 1980, p. 43) behavior patterns and characterized by three core attributes—inattention, hyperactivity and impulsivity—and an underlying cluster of (sub)symptoms. These include an inability to pay sustained attention, or failing to finish assigned tasks, fidgeting and moving about, talking excessively, and interrupting other people (American Psychiatric Association, 2013; World Health Organization, n.d. 1 ). Symptoms and diagnostic criteria appear to conform with each other across all definitions and countries, such as with both commonly used classification systems: the “Diagnostic and Statistical Manual of Mental Disorders (DSM)” (American Psychiatric Association, 2013) and the “International Statistical Classification of Diseases and Related Health Problems (ICD)” (World Health Organization, n.d. https://www.who.int/standards/classifications/classification-of-diseases). The latest worldwide synthesis of all major research studies reports that the prevalence of ADHD 2 is estimated as 5.9% in youth and 2.5% of adults (Faraone et al., 2021).
Although available data regarding ADHD prevalence must be regarded as indicative—as ages, numbers, population and means for obtaining prevalence estimates can vary across studies—the impact of ADHD on both individuals and society is likely to be immense and not to be underestimated. For example, due to the characteristically challenging behavior, individuals diagnosed with ADHD are at risk for school failure, mental health, and social difficulties (American Psychiatric Association, 2013; DuPaul et al., 2011; Tarver et al., 2014; Thapar & Cooper, 2015), as well as elevated risk of drug and alcohol abuse, accidental injury and premature death (Faraone et al., 2021).
Against this backdrop, it may be assumed that children and young people with a formal diagnosis of ADHD may also display difficulties in developing musical skills due to their condition. However, individuals diagnosed with ADHD are under-represented in literature concerning music education and music psychology. Despite widespread research evidence to indicate the likely benefits of music therapy on individual well-being, there has been little to no research into music and ADHD, nor whether ADHD is evident in the moment of making music.
Aims of the current research
Rooted in a general lack of research literature, the overall aim of this study was to investigate the extent to which ADHD behavior—with its three core attributes (inattention, hyperactivity, impulsivity)—manifests itself, both in the moment of musical activity, as well as when the activity stops. Based on literature that suggests symptoms related to ADHD might be mitigated by an appropriate teaching environment and effective practice (e.g., Purves et al., 2011; Wiebe, 2007), another focus was also on the context and provision of active music making.
Consequently, this study formulated three research questions: (1) Can children and young people diagnosed with ADHD engage successfully in music education? (2) Do presentations of ADHD change in the moment of engagement in music and, if so, how? and (3) Does the educational context and type of pedagogy shape the musical experience and attainment of participants with ADHD?
Framework and methods
The research adopted an exploratory case study approach (cf. Creswell, 2007; Stake, 1995; Verschuren, 2003; Yin, 2014). Case study research allows the researcher to pay attention to rich contextual detail in observing and interpreting social processes, and to focus on actions, behaviors, and events in real-life situations (Mills et al., 2010). Flyvbjerg (2006) challenges the conception that you cannot generalize from a single case study, arguing that you need context-dependent knowledge in order to begin to build a theoretical understanding of the particular area of research focus. In this case, we have very little previous research evidence of musical behaviors in the context of ADHD and, additionally, children and young people with SEND often have somewhat unique profiles and individual needs (e.g. Castro & Palikara, 2016; Lendrum et al., 2015). Previous studies related to ADHD and music (cf. McFerran, 2009; Mullins, 2017; Swope, 2018) were not designed from a music education perspective in that (1) there are no data on the nature of musical behaviors and ADHD symptoms in the moment of the music intervention, (2) data are vague regarding any contextual elements that might impact on ADHD behavior within lessons, (3) their focus lay on therapeutic effects through music rather than put music education in the foreground, and (4) some findings were generated through surveys rather than real-time observation. Consequently, exploratory case study offered the most suitable approach in terms of research methodology.
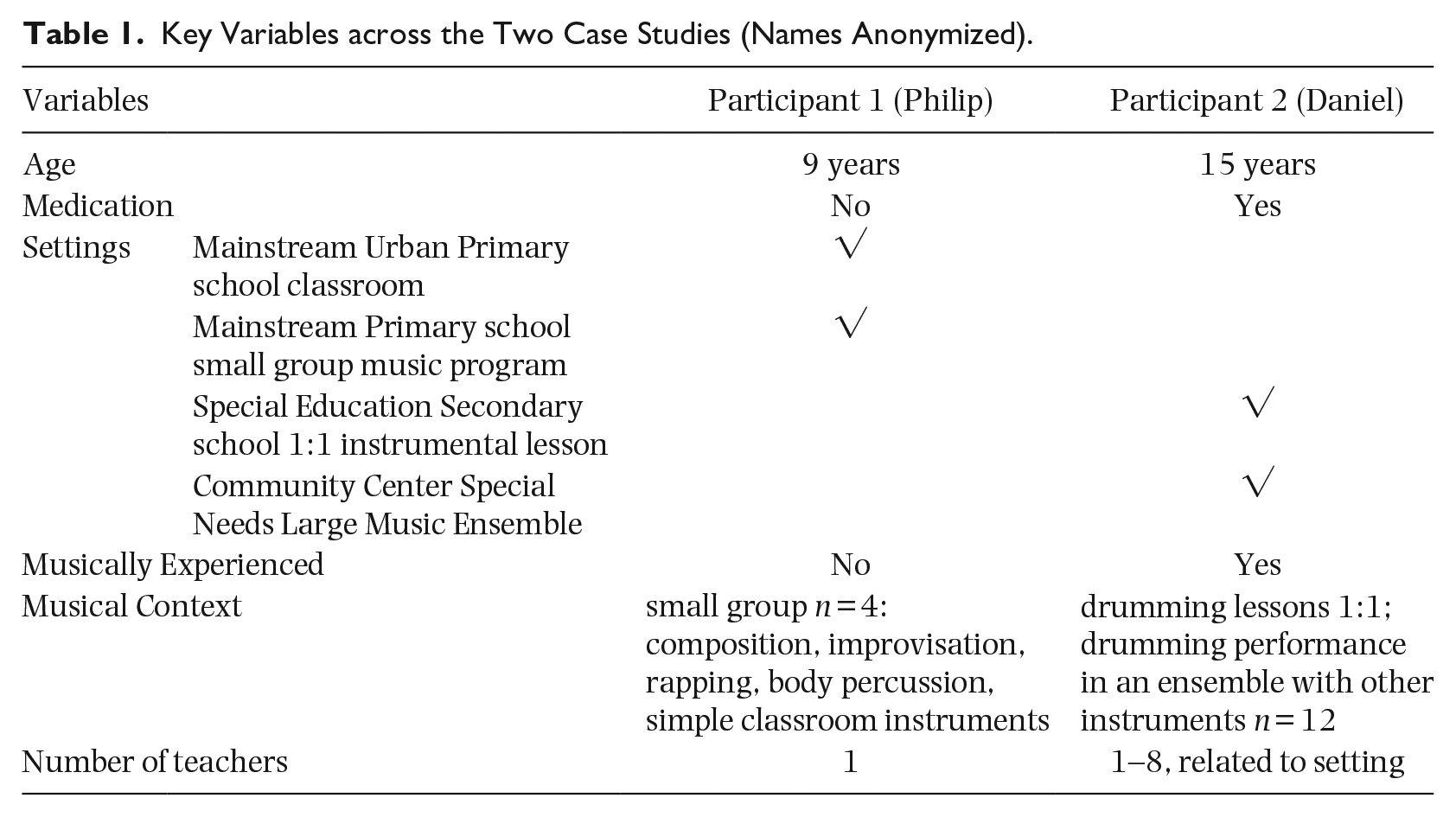
The intention was for individuals to be observed in their natural (real-life) contexts, addressing a wide range of corresponding factors and variables and considering multiple sites. Thus, the resultant evidence can be regarded as being more robust (Yin, 2014). Accordingly, two young individuals with an official diagnosis of ADHD were chosen to be observed in their real-life music making and learning contexts. Both individuals were boys, aged 9 years and 15 years, respectively, with varying ADHD and medical profiles (i.e., one receiving ADHD-related medication, versus one non-medicated), as well as being at different levels of musical competence related to age and experience.
Also, in order to understand the possible impact of context, structured classroom-based observations of these two boys were conducted in a total of four contrasting educational settings (two for each case) in the South-East of England over a period of several school terms. The four locations were, first, a mainstream Primary school, where the 9-year-old individual with ADHD was observed, both (1) in his normal classroom setting and (2) in a researcher-designed, small group musical program in the school’s music room; and second, the 15-year-old in his (3) special education Secondary school one-to-one instrumental lessons, and (4) in a large SEND music ensemble at a local community arts center (see Table 1). The small group music program and setting were established by the researchers as both, the 9-year-old boy’s class did not participate in any (curricular) musical learning program at the time, and the classroom was occupied at the time the program happened. The 15-year-old individual could not observed in his normal classroom setting because of both the school’s preference for the researcher not to sit in these general lessons, but rather to focus on the instrumental music learning.
Key Variables across the Two Case Studies (Names Anonymized).
In order to ensure methodological data triangulation, several forms of qualitative data were collected. Related to the participants’ ADHD diagnoses, the first author was granted access to the two main case study individuals’ official medical records as well as their school reports. Multiple observations of each participant and their musical and other-than-musical behaviors were made as the respective sessions unfolded, and documented in the form of field-based notes. Furthermore, to ensure a holistic approach and to provide the best possible validity and reliability of gathered data, both audio and video recordings were also employed alongside the classroom observation field notes. Where possible, the researcher also met with parents/carers to explain the purposes of the research. However, in both cases, participants and their parents/carers were informed in writing about the research and they provided written permission for their child’s participation; appropriate ethical permissions were obtained in line with university requirements and British Educational Research Association guidance (2011, since updated 2018—see https://www.bera.ac.uk/resources/all-publications/resources-for-researchers).
Data analyses were conducted by assessing field notes and related audio-visual data (observational data) and creating micro-analysis-transcripts of the audio-visual data. Video data which were thought to be representative of each music program session were analyzed, such that regular observations were entered every 30 s on a specially designed Excel-based observation grid. A total of 5,961 entries were recorded across both cases from a total of just over 24 hours of video data. Entries were related to (1) tutors’ and pupils’ actions and (2) the occurrence of particular behaviors that could be attributed to the reported ADHD symptoms of inattention, hyperactivity, and impulsivity, respectively, as well as their observed severity on an ordinal scale from 0 to 3, where “0” = absence of any ADHD-like symptoms, “1” = a mild presentation of symptoms, “2” = moderate presentations, and “3” = severe presentations. This was based on the design of common (ADHD) rating scales 3 , where “0” is an observed absence of symptoms. It is important to note that, overall, there seems to be a lack of a universal definition for assessing the severity of ADHD symptoms. Therefore, an understanding of ADHD severity derived from both the existing, albeit limited, literature, and the particular (re-occurring) presentations of characteristic behaviors of an ADHD diagnosis that were exhibited by the case individuals throughout this study.
Subsequent statistical data analyses resulted in an overview for the two focus case studies that enriched the accompanying qualitative data. Data for intensity over the duration of the lesson/session were mapped against each other to illustrate pictorially individual ADHD profiles (see examples in Figures 1, 2(b), and 3) of both case individuals. First, the sum of the exhibited symptoms/perceived behaviors attributed to ADHD symptoms in each of the three categories—(1) inattention, (2) hyperactivity, and (3) impulsivity—was converted to a percental statement of ADHD occurrence during a music lesson/session. Second, the average intensity of the indicator variables—being (sub)symptoms belonging to the three main ADHD categories to indicate the presence of ADHD—were measured on an ordinal scale ranging from 0 to 3 for the observed points in time—and covering the entire lesson time in 30-s intervals. This resulted in a representation of ADHD behaviors and their intensity in the specific moments that these occurred during the session for the given case individual. Although some symptoms were rated as 3 on the ordinal scale, the mean value for each category never exceeded the value of 1.6 (see, Figures 2(a), 2b, and 4). It is acknowledged that taking the average of ordinal variables is an oversimplification. However, this was regarded to be representative and a sufficient means to illustrate the particular ADHD profiles of the case individuals.
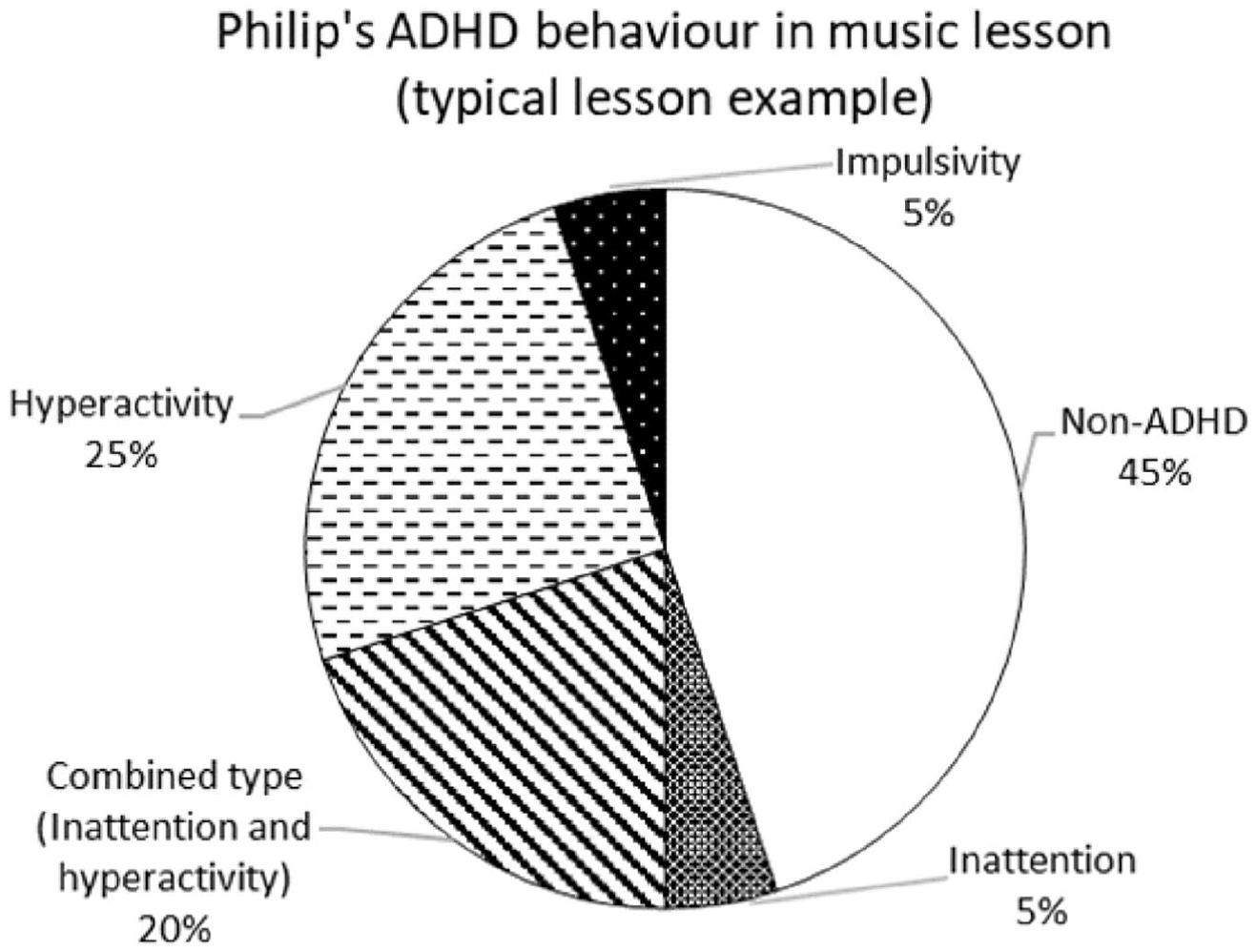
Philip’s ADHD and Non-ADHD Behaviors as a % in Relation to Each Other (Typical Lesson Example).
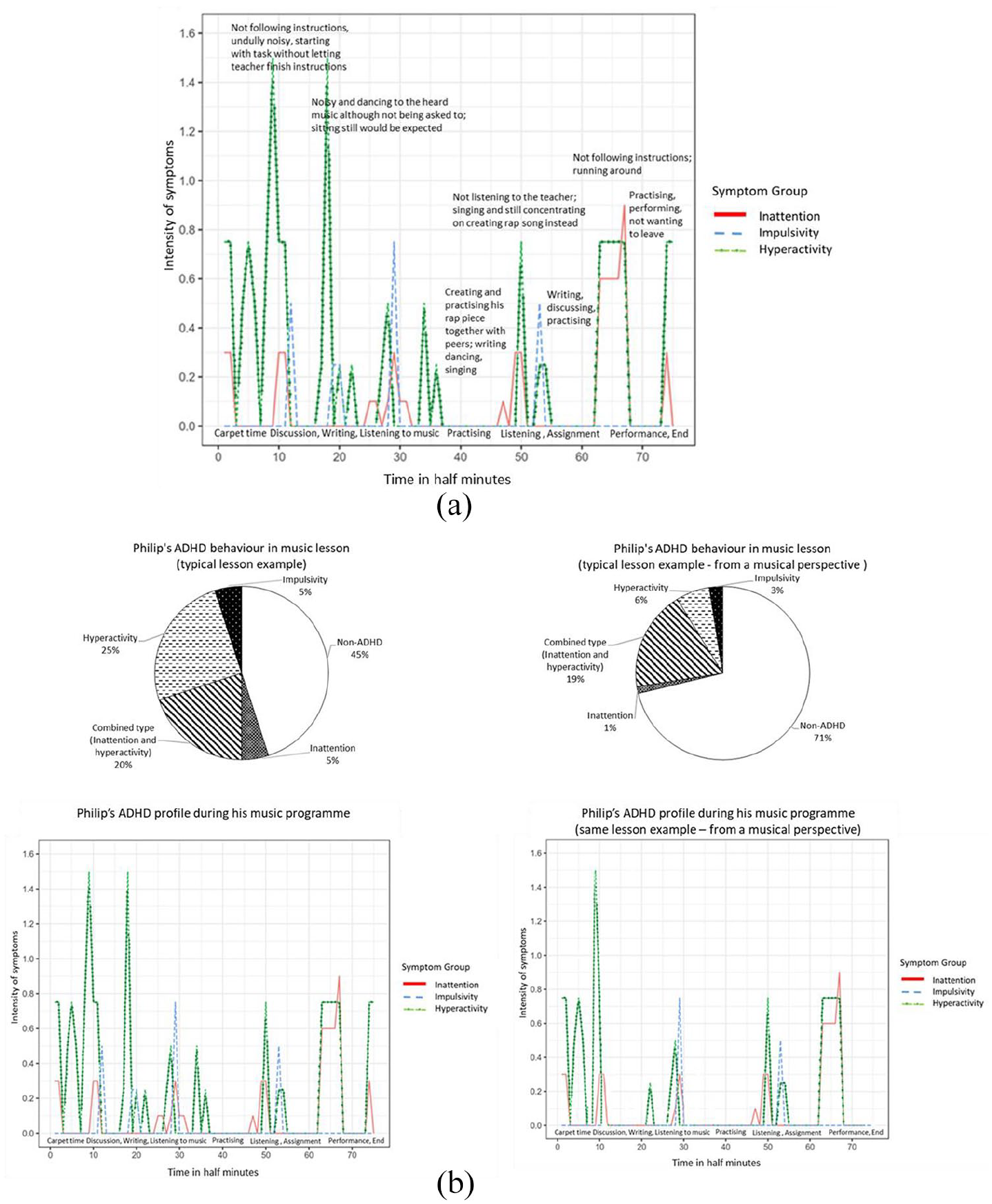
(a) Philip’s ADHD Profile During His Music Program (the Same Example Lesson as in Figure 1). Time in half-minute intervals = 38 min in total. Intensity of symptoms = mean value of all sub-symptoms (note that 1.6 is the highest evidenced mean intensity overall, using a scale of 0–3, where 3 is the absolute possible maximum of all ADHD sub-elements). (b) Philip’s ADHD profile during his music program (Figures 1 and 2a), in juxtaposition to an equivalent profile if the behaviors are translated as “musical.”
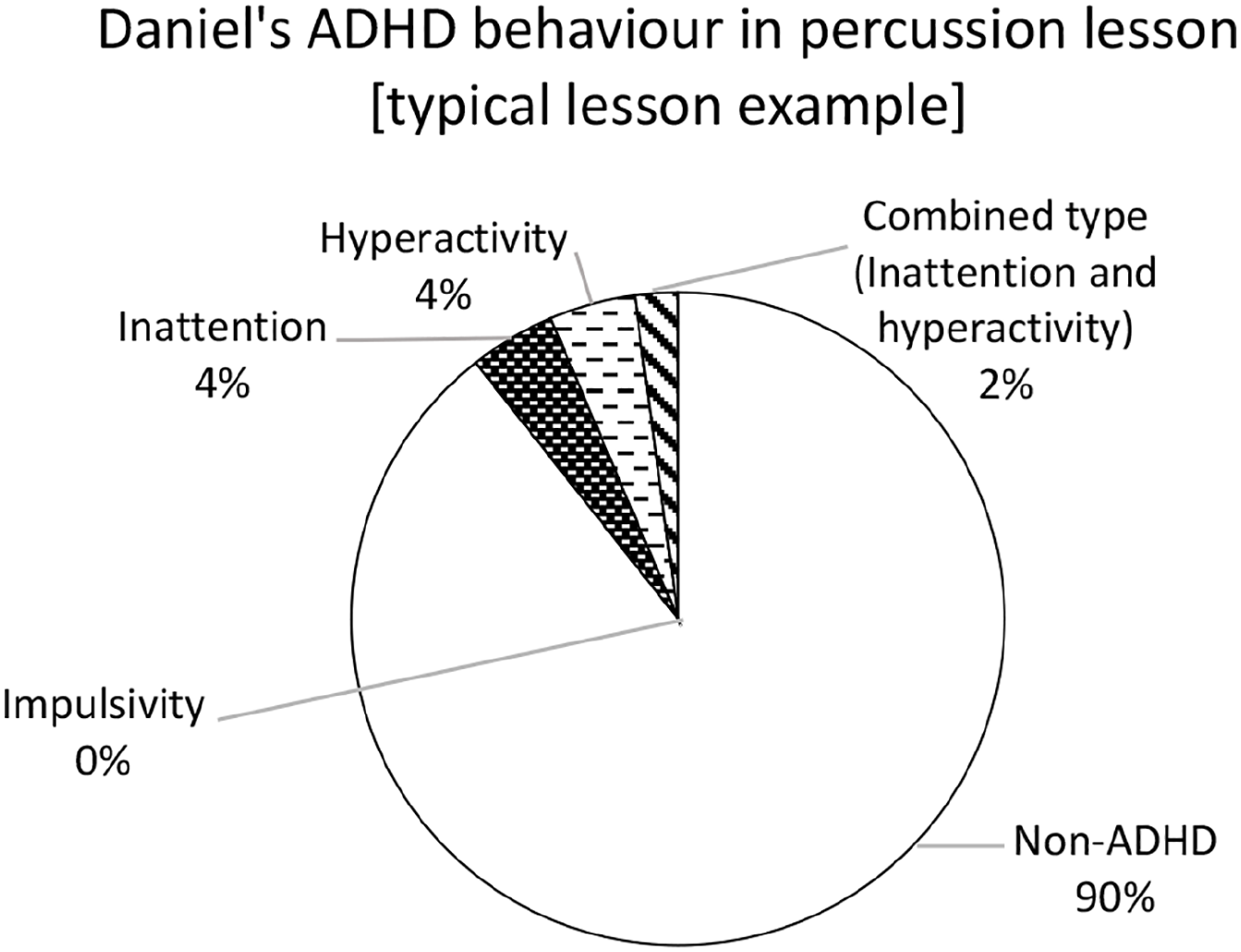
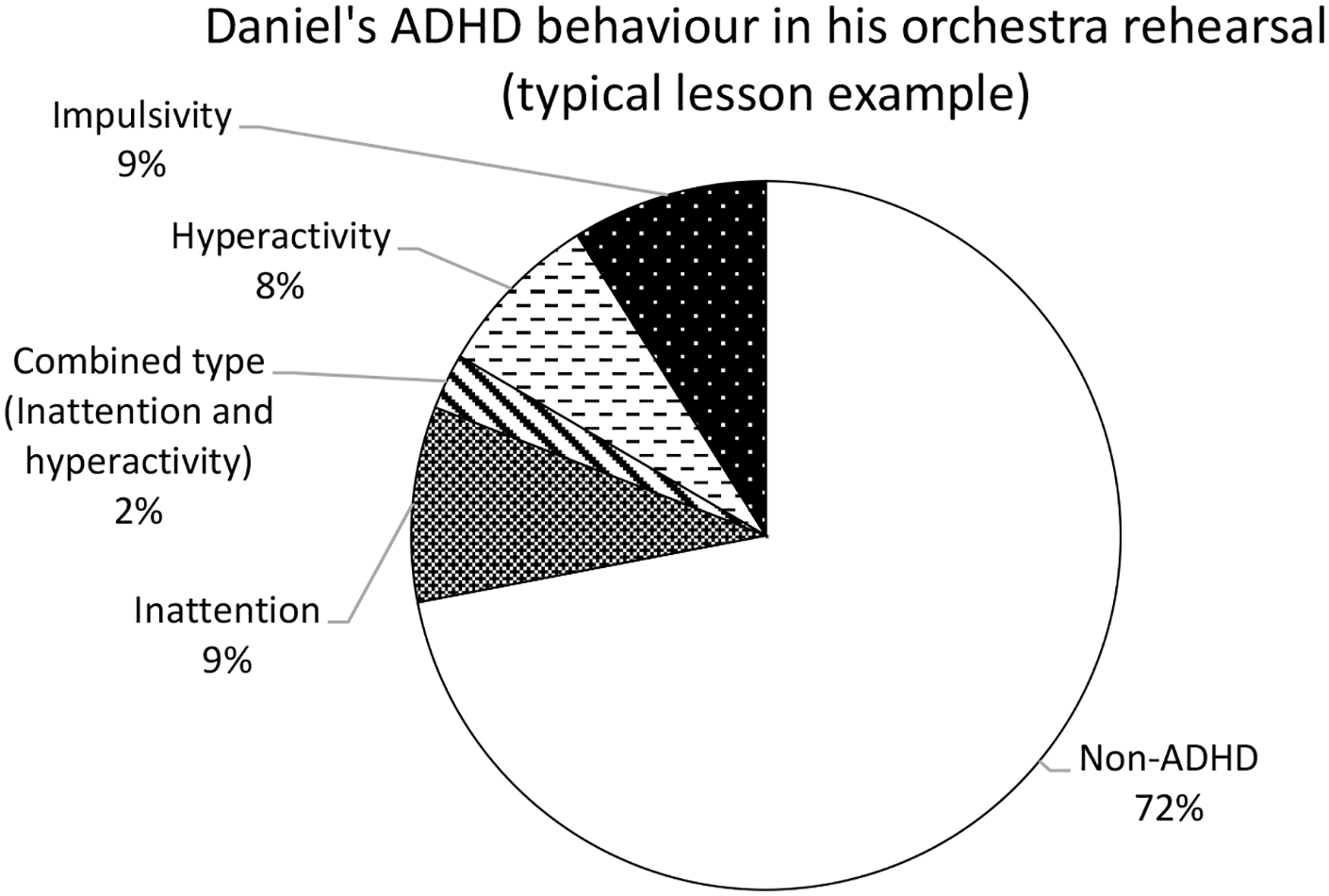
Daniel’s ADHD and Non-ADHD Behaviors as a % in a Typical 1:1 Lesson.
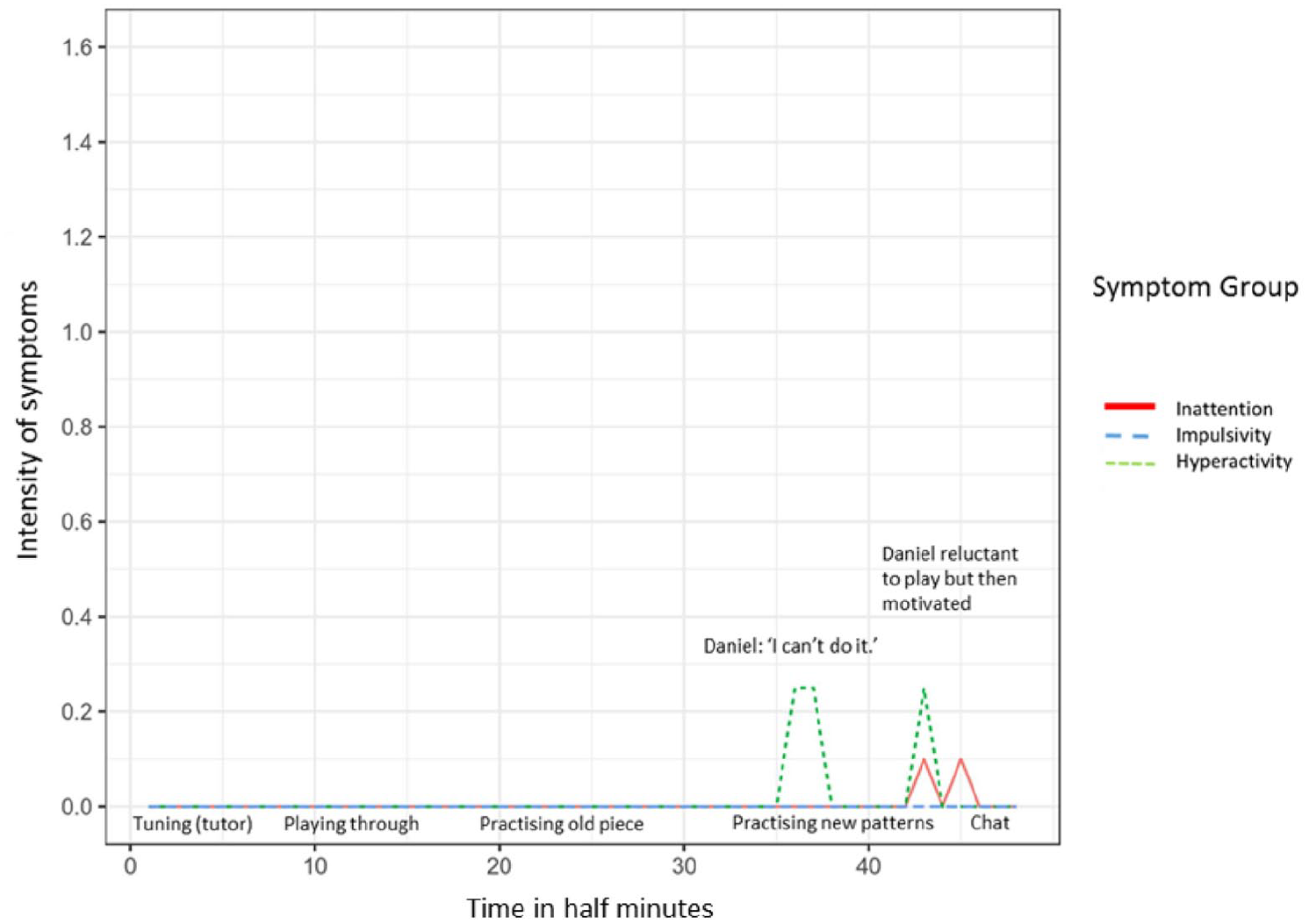
Daniel’s ADHD Profile During His Percussion Lesson (the Same Example Lesson as in Figure 3). Time in half-minute intervals = 23 min in total. Intensity of symptoms = mean value of all sub-symptoms (1.6 being the highest evidenced aggregate symptom intensity overall).
Findings
Case Study 1: Setting 1 Mainstream Primary school—a small group music program
Case 1 Setting 1 illustrates the musical experiences of a 9-year-old boy (Philip) with a formal assessment of ADHD and not on medication for his condition. Philip was selected along with three of his school class peers to form a small music group and receive regular music lessons that were designed and enacted by the first author (an experienced musician and music teacher).
When matched against current standard criteria for the classification of ADHD, all the small group participants (Philip, as well as his non-ADHD peers) occasionally showed characteristic behavior of an ADHD diagnosis, although Philip (the participant officially diagnosed with ADHD) showed these behaviors to a greater extent and more frequently when compared with his peers. Figure 1 illustrates Philip’s ADHD-like behavior as percentages of total time during one typical lesson. It can be seen that non-ADHD behavior is displayed almost to the same extent, albeit slightly less than ADHD-like behavior.
The most frequent ADHD-like behaviors that were observed were attributed to the hyperactive type (25%) and combined type (20%, i.e., inattention and hyperactivity together) of ADHD symptoms. Impulsivity and solely inattention were observed the least (5%). The particular behaviors attributed to ADHD were evident in moments before, after, and between the active engagement in music making and learning, such as before the lesson started, when setting up instruments, between tasks during the lesson, and when pupils had an argument prior to or after the music lesson (e.g., see Figure 2(a)). Conversely, ADHD symptoms were absent or least noticeable when making music.
In this lesson, Philip illustrated his creative use of verbal expressions together with singing and dancing in a hip-hop style. In such instances of creative music making and creating, he could act on his feelings and needs in a musical way—such as by simultaneously trying out and practicing his ideas.
Overall, Philip was able to be attentive, to stay on task, engage in learning about music and take part in all the musical activities despite his diagnosis. In this context, perhaps the most remarkable finding was that, in all moments of active music making (creation and performance) and spontaneous musical expression, no ADHD symptoms were evident in his behavior. Furthermore, from a pedagogical perspective, often Philip’s need for movement and to talk could be integrated and combined with the set task, such as to invent and perform a rap song, or enact rhythms with his body using body percussion. Overall, his musical outputs were at least of the same quality as those of his peers’. In those instances when the small group were asked to sit at their table and complete an assigned task while listening to music, very often Philip spontaneously stood up and moved to the music—indicated as ADHD-like behavior if seen from a non-musical perspective; see Figure 2(a), time intervals 18–20. Nevertheless, he listened to the heard music attentively, hummed along, and his movements and interpretation matched the music’s character. Whereas standing up and moving without being asked might be seen as misbehavior in other school subjects, this particular behavior could be interpreted as positive in the context of engagement with music. Furthermore, it did not disturb the other participants in completing their assignment, nor did it lessen the quality of his finished task. Consequently, in this case, ADHD behavior was not seen as an impediment to taking part successfully in musical activities, but could be—intentionally and spontaneously—integrated. Consequently, it could be suggested that, if the pedagogy was responding in the moment to the individual’s needs and the observed behavior was uniformly regarded as being musical rather than ADHD-like, the ADHD profile would look different. Figure 2(b) provides an example of how the pedagogical “lens” can make a difference if the observed behaviors are seen as “musical” rather than “ADHD-like.”
Philip was free to act on his feelings and needs in a musical way, as the context provided him with a sense of agency in terms of creating a scaffolding for the musical activity. Consequently, what might normally be regarded as ADHD behavior in another context could be accepted and observed to be as either “non-existent” or “less” in the context of active music education. In particular, behaviors translated as “hyperactive” through an ADHD “lens” become “musical.”
In addition, an overall ongoing positive wider impact of the musical intervention could be observed intermittently—a kind of halo effect—when re-joining his classroom lessons, as he was more socially included and neither hyperactive nor inattentive; this is despite often being reported to be agitated, difficult, and not able to attend properly to his classroom lessons prior the music sessions.
Case Study 1: Setting 2 Mainstream Primary school—the same pupil in the general classroom
In addition to observations in the specially designed music program, Philip was also observed in his normal classroom environment (Setting 2), both before and after the music sessions. This was to gain some insights into his behavior outside music. Philip was observed to be a very talkative person when compared with his peers, often speaking without being asked (and also mumbling to himself). He usually used every opportunity to talk to his peers. However, his behavior did not seem to disturb his peers to a great extent. The class teacher reported that the other children intentionally and demonstratively tried to ignore Philip’s (mis)behavior and his attempts to engage them in conversations.
Although this may seem like a paradox, in most instances Philip’s ADHD behavior—or the presence thereof—was not always observed in the classroom situations, but it rather was implied by his regular absence from the classroom during the children’s normal school program. When he was regarded as being unable to participate in his lessons because of his unstable emotional state, he was removed—together with his special educational needs support assistant—and engaged in non-lesson-related activities with the school’s Special Educational Needs Coordinator (SENCO). This was justified officially by the intention of giving him a separate space for his emotional outbreaks, to calm down, and to offer a means for acting out his urge for movement (hyperactivity). Whenever this happened, Philip missed out on the education being provided for his peers in the classroom. Observational data analyses suggest that the boy seemed to enjoy this kind of “time out” and hardly showed any signs of emotional discomfort during that time.
Case Study 2: Setting 1 Secondary Special School—one-to-one instrumental lessons
In the second case study, the musical experiences of a 15-year-old boy (Daniel) with an official diagnosis of ADHD (being treated with medication) is described during his weekly one-to-one drumming lessons in his Secondary Special school.
Daniel presented as a very enthusiastic and engaged musician, who was always keen to attend his instrumental lessons. Despite his ADHD diagnosis, in these one-to-one lessons he was observed rarely to show behavior that could be associated with ADHD. The following illustration (Figure 3) shows the proportions of Daniel’s ADHD behaviors in relation to non-ADHD behavior in percentage term for one typically observed lesson.
Figure 3 shows that Daniel behaved “neurotypically” or ADHD-less for much of the lesson time (90%). ADHD-like behavior accounted for only 10% of the total lesson. For the largest part of the lesson, he was neither inattentive, nor hyperactive, nor impulsive. In this regard, analyses of the observational data revealed that most of the lesson time was filled with music, such as music performance, practicing, and improvising. Tutor instructions and explanations were kept very short. At some points, mostly toward the end of a lesson, Daniel seemed to be self-conscious and anxious in that he was observed suddenly to fidget around, being shy, and communicating that he “can’t do that” as well as resist to do the assigned task and rather not try something new; a characteristic that was consistent with his school and medical reports. Also, it was in these instances in which he appeared to show signs of ADHD-related behavior. Figure 4 represents how a typical lesson (the same lesson example as in Figure 3) evolved over time, showing when and in which lesson context the above illustrated ADHD symptoms occurred or were absent.
As can be seen in Figure 4, ADHD-like behavior (attributed to inattention and hyperactivity) was only evidenced at the end of Daniel’s 23-min-long lesson. All these behaviors could be attributed to ADHD symptoms as sub-elements: (1) avoiding tasks that required mental effort/inattention and (2) fidgeting/hyperactivity. However, as he was reported generally to be prone to anxiety, these behaviors might also be an inherent anxiety trait rather than being linked to ADHD. At the beginning and middle part of the percussion lesson, no ADHD-typical behaviors were observed. Also, no signs of behaviors that could be attributed to ADHD were evident in the moments of playing his instrument.
Daniel was able to (re)create music as well as improvise at an advanced level of musicianship. Overall, he showed a wide range of musical behaviors. In particular, he liked to envisage himself as a member of a rock group. He saw himself as the imaginary band’s member whose task it was to coordinate the group, as well as count everyone in before starting to play the gig on an imaginary stage. The tutor allowed him to act on his feelings and let him speak to his imaginary group and count in each time. While playing, he gave the impression of being totally immersed in the music. Occasionally, he would be starting to sing along to the music, too.
The tutor was very thoughtful, engaging, and intuitive in both his pedagogical and interpersonal approaches, reacting in the moment to Daniel’s needs. He was able to motivate Daniel to resume playing and try the new things if he appeared reluctant to engage with new techniques. He saw Daniel as a musician and had high expectations, reporting his belief that Daniel had great musical potential. The amount of observed musical engagement during the lessons was high and both pupil and teacher often played together as a duo—percussion and electric guitar, or percussion and piano. In no instances were negative words noted; conversely, Daniel was praised for his good progress.
Case Study 2: Setting 2—special needs orchestral rehearsals in a local community center
As well as his one-to-one drumming lessons in the Special school (Setting 1), Daniel voluntarily played the piano in a community-based ensemble for young people with SEND (Setting 2).
In contrast to his one-to-one tuition, Daniel had the opportunity to interact musically with other young people and engage in large group music making. In a similar manner to his percussion lessons, Daniel was observed to be an enthusiastic musician in this instrumental music program. He was perceived to enjoy the orchestra rehearsals and to be part of an ensemble. As in his one-to-one setting, Daniel displayed advanced musical abilities. Apart from (re)creating and playing the orchestral piece on the piano, he had the opportunity to engage in creative music making and guided improvisation.
Nevertheless, apart from occasions when he was encouraged to conduct the ensemble as part of a game, it seemed that Daniel could not act on his immediate feelings to the same extent as in his school-based music making. For example, when engaging in smaller, sub-group activities, Daniel was observed to lead his peers and instruct them according to his musical ideas. In other instances, he liked to count the whole ensemble in, as was his custom in his one-to-one percussion lessons. However, these particular contributions were (1) either not noticed, or (2) regarded by the tutors as disruptive. In addition, there were musical improvisation games between selected musicians and the tutors. Yet, Daniel was rarely picked to engage in these games and instead had to wait. In these moments, he seemed bored and impatient. Consequently, it can be said that he had to adapt and hold himself back personally as well as musically in such instances.
In contrast to his school-based program (Setting 1), and despite being on medication in both contexts, Daniel exhibited more instances of ADHD-like behavior (relative to his school-based program) and across a wider range of ADHD-like symptoms during the ensemble rehearsals (see Figure 5).
Daniel’s ADHD-Like Behaviors as a Percentage in an Example Ensemble Session.
It can be seen that for much of the rehearsal time (72%), Daniel was observed to display no behavior that could be attributed to ADHD (see Figure 5). However, if compared to his one-on-one percussion lessons at school (Setting 1), overall Daniel displayed more ADHD-like behaviors in his orchestra rehearsals. It may be that one factor which increased the likelihood of ADHD behavior could be the time factor as the ensemble sessions were longer than his one-to-one lessons. However, in this ensemble music-making context, ADHD behavior could be observed at the beginning of the session, including instances of ADHD behavior in mid-rehearsal and toward the end of the rehearsal. Figure 6 illustrates Daniel’s behavioral profile during one ensemble session over time as the session evolved (the same lesson as summarized in Figure 5).
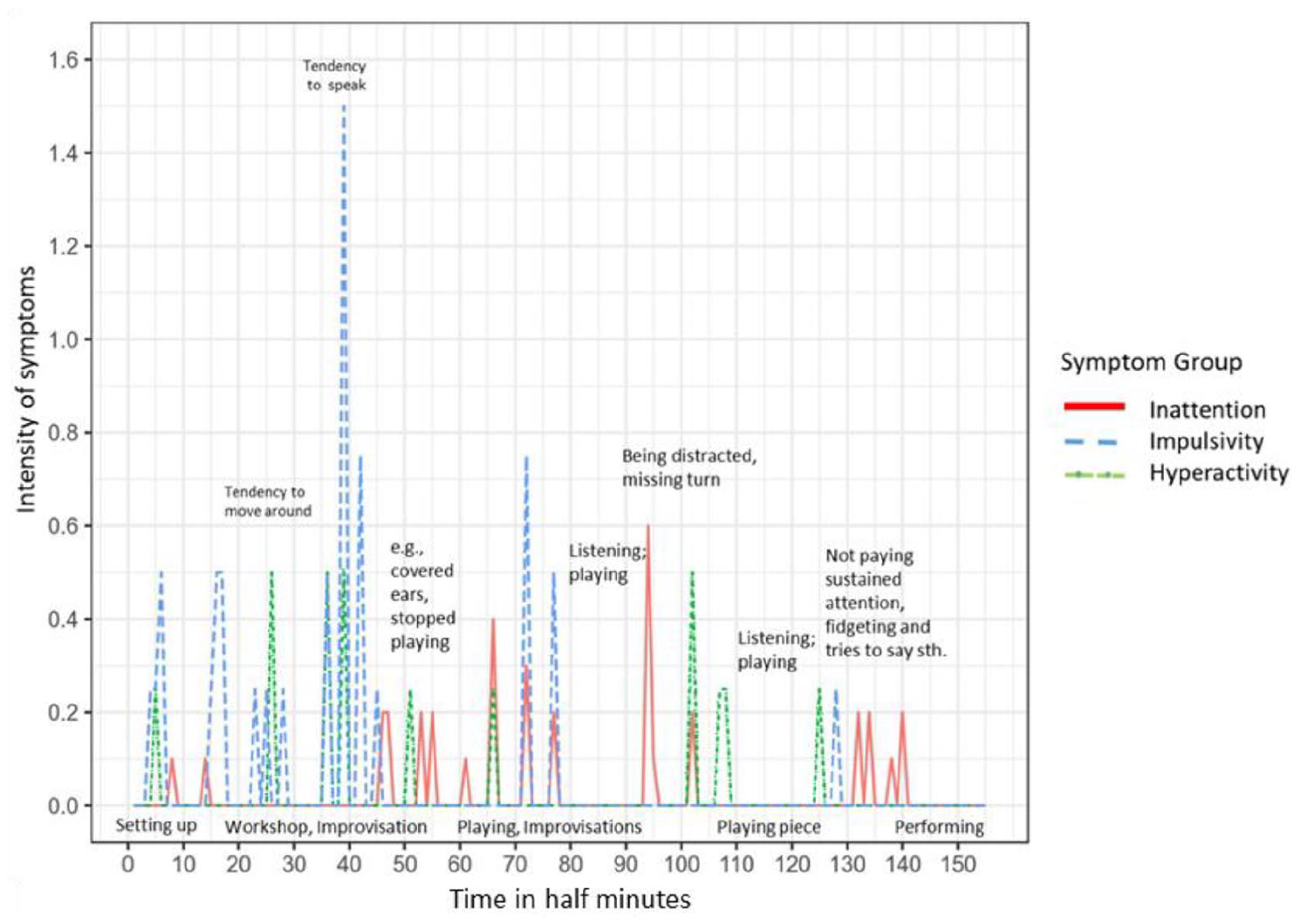
Daniel’s ADHD Profile in an Orchestra Rehearsal (Lesson Example). Time in half-minute intervals = 80 min in total; Intensity of symptoms = mean value of all sub-symptoms (1.6 being the highest evidenced intensity overall).
In particular, ADHD-like behavior was evident—or perceived as such by the reactions of his tutors—when Daniel was denied an opportunity to act spontaneously musically and in moments when he had to wait for the next opportunity for him to play, such as when tutors were giving instructions, instruments were being set up, or when it was the turn for others to play and he had to wait. In these instances, he was observed to start talking and to fidget. Nevertheless, there were other moments in which Daniel was observed to behave neurotypically. In particular, while playing the keyboard and in the actual moments of performing, behavioral symptoms related to ADHD were not observed.
Within an overall “good” rehearsal (in terms of tutors’ comments), some aspects were designated to need improvement. For example, orchestral participants were believed potentially to benefit if they were given more opportunities to express own ideas and make music in smaller groups more often. In contrast, often one third of the rehearsal time was spent in setting up or waiting, at which times Daniel started to fidget, seemed impatient, and needed to talk without being asked.
Discussion
This study examined example music learning contexts of two case study individuals with a formal diagnosis of ADHD. The investigation was framed to address three questions. The emergent data across the cases have shown that these questions, apart from being addressed individually and in their own right, are also interrelated.
Can children and young people diagnosed with ADHD engage successfully in music education?
The study’s findings suggest that, perhaps contrary to what might be expected from the customary symptoms, individuals with a formal diagnosis of ADHD were observed to be able to engage successfully in music education, and acquire musical skills, particularly (but not only) when having an opportunity to express themselves musically. This is in line with the available literature findings to suggest that individuals with ADHD can engage in (creative) music activities and both learn to the same degree as their peers and interact with them musically (Myllykoski et al., 2010; Purves et al., 2011). The case study individuals engaged in learning about music, possessed a good understanding of music and musical expressions, and were able to respond to heard music, (re)create music, and interact musically with peers in various musical ways, irrespective of their level of musical competency prior to the music program. Furthermore, in instances of engagement in musical activities that required more active and/or physical participation, and when provided with appropriate pedagogical opportunity, ADHD-like behavior could be channeled and integrated into the active music-making process as opposed to be seen as a hindrance. Observations revealed that, unexceptionally, case study individuals acted as musicians when given the opportunity by their tutor(s) to self-represent as a musician. Similar to McFerran’s (2009) study, these two individuals seemed to enjoy the music sessions and have positive experiences, in particular when being in control of their music making and when the program allowed them opportunities to act on their feelings. Different to McFerran’s context, however, was that these findings were evidenced outside a music therapy environment, that is, in formal music education contexts, both in a school and a community setting.
Overall, the presence or absence of medication did not seem to have a significant influence on both participants’ musical behaviors. In this regard, the non-medicated 9-year-old participant was able to behave neurotypically and, conversely, the medicated 15-year-old boy was observed to occasionally display behavior attributed to ADHD. Furthermore, based on these research data, neither age nor the level of musical experience seemed to be factors to determine whether an individual diagnosed with ADHD is able to engage successfully in music. These findings are, therefore, in line with other studies that report on the musical abilities of children and young people with SEND, despite any prevalent behavioral difficulties, individual physical and mental (dis)abilities, and special educational needs (cf. Ockelford, 2015; Ockelford & Matawa, 2010; Welch et al., 2015).
Do presentations of ADHD change in the moment of engagement in music and, if so, how? and Does the educational context and type of pedagogy shape the musical experience and attainment of participants with ADHD?
Data analyses revealed that, despite symptoms of the three core attributes of ADHD (inattention, hyperactivity, and impulsivity) being evidenced in the case study individuals at different moments, both within and across the music-making programs, these symptoms were not persistent, nor exhibited in ways that necessarily prevented successful musical engagement. Moreover, the perceived presence or absence of ADHD seemed to a certain extent be in the “eye of the beholder.” It became evident that the individuals’ behaviors were not perceived uniformly, as they were dealt with and rated differently across the music-making contexts and their tutors. Identical behaviors could be regarded both negatively and positively, presumably related to a tutor’s a priori expectations and understanding of ADHD.
Consequently, perhaps the most remarkable finding was that none of the case individuals (nor other participants) exhibited any behaviors that could be attributed to ADHD in the moments of active engagement in music making and creating, for example, while playing on their instruments, or performing with/to their peers. In contrast, ADHD behavior was most evident in those moments of other-than-musical engagement, such as waiting.
Furthermore, the perception of, and tolerance toward, unexpected musical behaviors, as well as the conscious integration of certain characteristics of ADHD (e.g., the need for movement/hyperactivity) emerged to be important. Not only was this allowance for individuality crucial in accommodating specific behavior in music, arguably it could also give the individuals a sense of agency, ownership, and permission to act on their feelings. It can be concluded that what might be otherwise seen as negative and ADHD-typical behavior could be channeled toward positive musical behavior, provided that this was consciously considered by the teachers. Also, ADHD symptoms may be regarded as less severe, less evident, or even absent if considered in musical contexts and through a musical lens. Moreover, physically active engagement in music may be considered to be effective in both educational and therapeutic senses (see McFerran, 2009). This is in line with existing, non-musical literature to suggest that activities that allow individuals diagnosed with ADHD to move are beneficial for their learning (cf. DuPaul et al., 2011; Kutscher, 2014).
Analyses of the music programs’ teaching contexts and learning suggest that, irrespective of the particular location and the number of tutors present, the quality of education and the effectiveness of the provision in music for children with ADHD is crucial. In this respect, and in line with music research literature (for example, see Hallam, 2015; Hargreaves et al., 2017; MacDonald et al., 2002), positive perceptions of the case study individuals’ musical potential, together with high expectations, were factors that impacted on the individuals’ behaviors and their attainments and progress in music.
Conclusion
This study’s research evidence suggests that having a formal diagnosis of ADHD should not be seen as a barrier in music-making contexts and in musical development. On the contrary, typical ADHD behavior is observed to be absent in moments of active music making and performance. Furthermore, behaviors attributed to ADHD may be regarded as less or even absent if considered through a musical lens in which musical action is required. Individuals with ADHD are identified to both be able to self-perceive and self-represent/express as musicians and act accordingly in music contexts. Moreover, individuals with a formal diagnosis of ADHD may gain from systematic education in music. It can be argued that music education, that is, the acquisition of musical knowledge and skills, can be pursued in its own right, as well as being therapeutic at the same time, such as by experiencing non-ADHD moments. Consequently, for all individuals, but particularly for children and young people with disabilities and special needs, such findings are important in reviewing opportunities for sustained engagement with music in therapeutic as well as educational senses. However, the inference is that the musical experiences of children and young people with ADHD can be influenced by contextual factors, both positively as well as negatively. Positive experiences and successful engagement in music education appear to be closely related to the quality of the music education provision and is in line with research findings on what counts as effective music education with neurotypical as well as neuro-diverse children and young people. Moreover, this study’s evidence suggests that there is an inverse relationship between the quality of musical engagement and the observable degree of ADHD behaviors, with contextual factors such as (1) the individual having a sense of agency, (2) active involvement, (3) quality of pedagogy responding in the moment to the individual’s needs, and (4) the amount of musical engagement (see Figure 7).
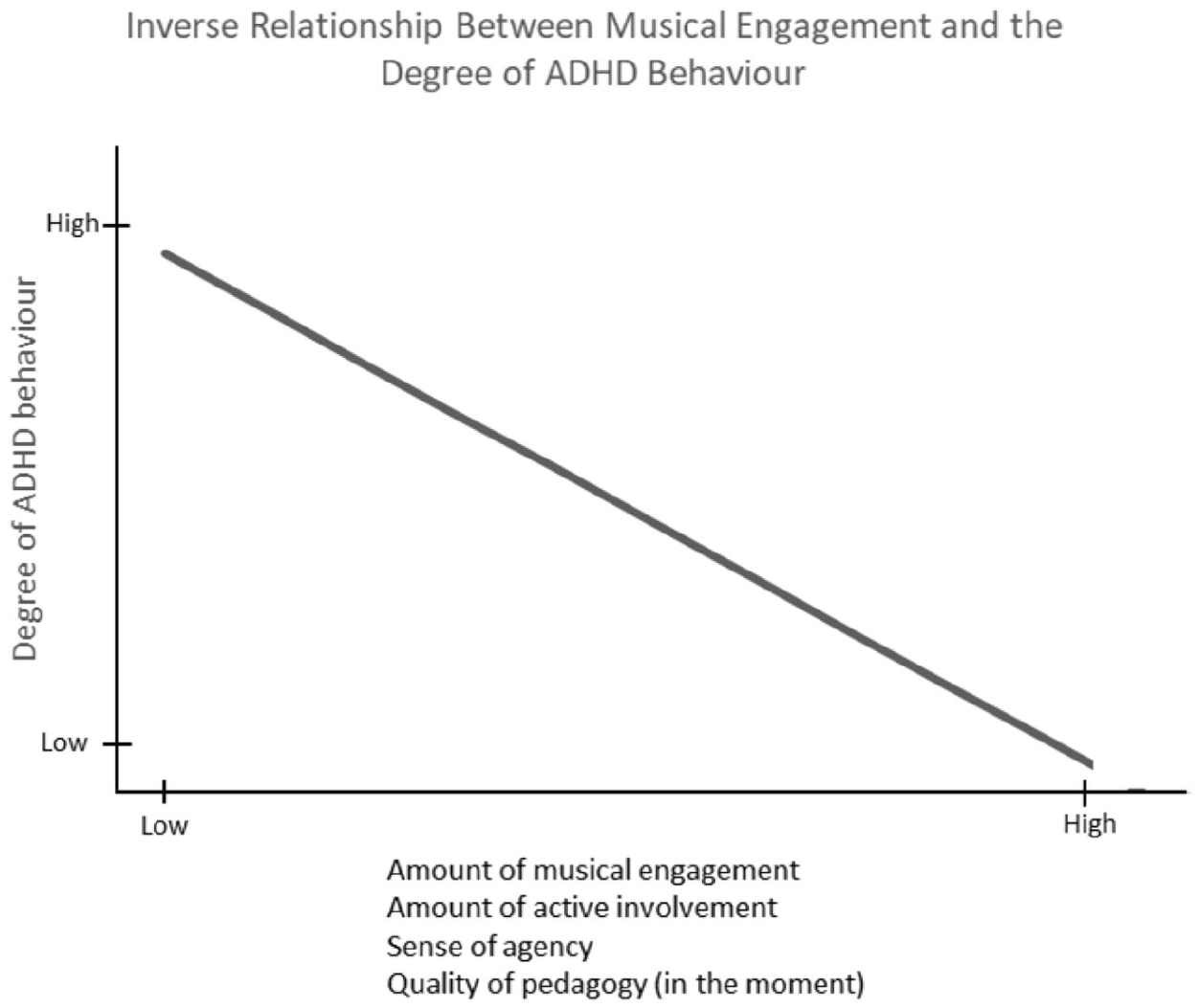
Theorized Relationship Between the Quality of Musical Experience/Engagement and Observed Degree of ADHD-Like Behaviors, That Is, an Inverse Relationship.
The adopted exploratory case study approach—which yielded a substantial amount of data that was generated in real-time and in real-life situations and circumstances through a variety of data collection methods—allowed for this rich contextual detail; consequently, to build an understanding of the particular area of research focus.
Hence, this study highlights the importance of high-quality and effective music education practice for children and young people with ADHD and, ultimately, for every individual with and without special needs. In particular, music education programs that offer opportunities to channel ADHD behavior into active music making as well as allow for personal involvement in making own decisions and expression of own (musical) feelings are believed to be beneficial for individuals with ADHD.
Consequently, professionals in the music education sector should not debate whether special needs and disabilities (SEND) are a barrier to musical behavior and development, but rather discuss what an effective, systematic, context-sensitive education in music should look like. In this respect, this implies that music educators should be appropriately trained, such that they are able to apply effective approaches in the context of pupils with ADHD and support their music learning.
In terms of limitations, it must be acknowledged that, following a case study approach with a reasonable small sample size, it cannot be excluded that more cases could have enriched this study or provided more findings although rich data could be collected. Also, the research participants were selected for pragmatic reasons, meaning that the researcher had no choice in sampling the participants as the identification and recruitment of participants with a formal diagnosis of ADHD turned out to be very difficult. In addition, it can be argued that an observation of Daniel’s behavior in his normal classroom situation as well as an observation of Philip in a non-researcher-led music program could potentially have enriched the findings and yielded more insights. Therefore, it is recommended that future studies should build on where this study concluded and investigate ADHD in music education in more depth. A replication of this study with a larger number of participants could also extend the findings of this multiple case study to a wider population.
Footnotes
Acknowledgements
We thank all the study participants, parents, teachers, tutors, and schools, without whom this study would not have been possible.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.