
Abstract
The purpose of this study was to systematically review the scientific literature concerning the effect of playing background music on anxiety and physiological parameters in patients undergoing dental treatment. MEDLINE-PubMed, Cochrane-CENTRAL, and EMBASE were searched for papers up to September 2020. Inclusion criteria were randomized clinical trials (RCTs) or controlled clinical trails (CCTs) among adolescents and adults that assessed anxiety (AX), systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), or respiratory rate (RR). Data before and after treatment were extracted and the potential risk of bias was estimated. Descriptive analysis and meta-analysis were performed. Thirteen eligible studies (12 RCTs, 1 CCT) were retrieved, with an estimated low to high risk of bias. Descriptive analysis showed an effect on AX in favor of music intervention, while no effect on SBP and DBP was found. The effect on HR and RR was inconsistent among studies. Meta-analysis showed a significant difference of means (DiffM) for the end scores of AX (State-Trait Anxiety Inventory and Corah’s Dental Anxiety Scale (CDAS)) and incremental scores (CDAS) in favor of music intervention. Dental care professionals may consider playing background music while treating adolescent and adult patients. There is a moderate certainty that this can provide a small reduction in dental anxiety. With very low to moderate certainty, no effect on physiologic parameters can be expected.
Dental anxiety is defined as an aberrant fear or dread of visiting the dental care practice and unwarranted anxiety for dental procedures (Laplante, 2012). It is a common problem and is considered a hindrance for dental care professionals. It is shown that one out of six adults experience some form of dental anxiety (Hmud & Walsh, 2009) and that dental fear and anxiety decrease with age, which reflects normal psychological development. The dental care professional and patient relationship, overshadowed by severe anxiety, has the possibility to lead to misdiagnosis and incorrect treatments (Eli, 1993). It may result in a hindrance of cooperation of patients during dental treatment, which in turn is associated with an unwarranted prolonged dental treatment. Dental anxiety is also heavily associated with patients’ oral health deterioration (Armfield, Stewart, & Spencer, 2007; Lahmann et al., 2008; Mehrstedt, Tonnies, & Eisentraut, 2004).
Fear of pain is one of the primary factors causing anxiety and forms an impediment to seeking dental care (Arntz, van Eck, & Heijmans, 1990). There are several studies that have shown a relation between peri-operative anxiety levels and peri-operative perceptions of pain in surgical patients. It is also known that more anesthesia is required during the treatment when there are high levels of pre-operative anxiety (Katz et al., 2005; Maranets & Kain, 1999; Ozalp, Sarioglu, Tuncel, Aslan, & Kadiogullari, 2003; Vaughn, Wichowski, & Bosworth, 2007). Other stimulants that can trigger anxiety in patients undergoing a dental treatment are dental injections, the sight and sounds of instruments and odors related to the dental clinic, with dental injections being the most provoking stimulant (Burghardt, Koranyi, Magnucki, Strauss, & Rosendahl, 2018). Time spent in the waiting room prior to the dental treatment has also been referred to as a frequent cause of dental anxiety (Moola, Pearson, & Hagger, 2011).
A patient with dental anxiety is best helped by providing trust, realistic information and control, and applying a high level of predictability (De Jongh, Adair, & Meijeringk-Anderson, 2005). Other treatment strategies are pharmacological support or teaching coping strategies. Pharmacological interventions are, for instance, pre-medication policy (benzodiazepine) or inhalation sedation (nitrous oxide sedation). Coping is a strategy for stress management and emotional control. Three of such strategies are relaxation (e.g., relaxation of muscle groups or imaginal visualization), hypnosis (a specialized method of relaxation combined with a deep form of concentration) and distraction. Distraction refers to the idea that these behaviors or thoughts are incompatible with the experience of feelings of anxiety (De Jongh et al., 2005). Examples of distraction are instruction to concentrate on abdominal breathing, watching visual information (e.g., a poster, fish tank, video), solving mental problems or puzzles, or listening to music.
Studies on mood regulation have identified music listening as an effective regulatory strategy (Saarikallio, 2008). The use of background music is, for instance, widely recognized to influence consumer behavior. As a key ambient factor in retail environment, music engages, entertains, energizes, refreshes, involves, and creates a pleasurable memorable experience (Jain & Bagdare, 2011). Listening to music can also contribute to changing a bad mood, raising energy, and reducing tension (Thayer, Newman, and McClain, 1994). When a study population in Londen was asked, “What is the thing to do when you are feeling depressed?” one of the most frequently mentioned strategies was listening to music (Rippere, 1977). Background music has a positive impact on emotional reactions among adult listeners (Kämpfe, Sedlmeier, & Renkewitz, 2010). The so called “musical mood induction procedure” relies on music to produce changes in experienced affective processes. The procedure has shown to be able to induce positive, negative, and neutral moods (Västfjäll, 2001). Many studies on musical emotions have been performed without regard to how they were evoked and have neglected evaluation of the underlying mechanisms (Juslin & Västfjäll, 2008). It seems unlikely that it only a direct, non-cognitive response (Västfjäll, 2001). A framework that has been proposed to explain the emotional reaction to music that people experience includes eight mechanisms (Juslin, 2013). It is presumed that these mechanisms may be activated by different types of information in a “musical event” (Juslin, Harmat, & Eerola, 2013).
A recent systematic review and meta-analysis on 104 studies assessed the strength of the effect of music intervention on both physiological (e.g., heart rate, blood pressure, and hormonal levels) and psychological (e.g., anxiety, restlessness and nervousness) stress-related outcomes in different kinds of settings such as mental health care, polyclinic medical settings, during medical surgery and in daily life situations. The outcome shows a significant effect in favor of music intervention (De Witte, Spruit, van Hooren, Moonen, & Stams, 2020). However, this review categorizes dental procedures among medical procedures. The specific effect for the circumstances in a dental office are not revealed. The most recent systematic review of the effectiveness of music interventions on dental anxiety in pediatric and adult patients dates from 2011 (Moola et al., 2011). Seven studies were found of which five studies had adult participants and two studies pediatric participants. The authors concluded that there was enough evidence to suggest that adult patients may benefit from music listening. However, the evidence for reducing dental anxiety in children was inconclusive.
The aim of this systematic review was to comprehensively search the scientific literature, as to identify, critically appraise, analyze, and synthesize studies concerning the effects of playing background music on physiological parameters and dental anxiety in adolescent and adult patients undergoing a dental treatment.
Material and methods
This systematic review was prepared and described in accordance with the Cochrane handbook for systematic reviews of interventions (Higgins & Green, 2011), and the guidelines of Transparent Reporting of Systematic Reviews and Meta-analyses (Moher, Liberati, Tetzlaff, & Altman, 2009; PRISMA Statement, 2009). The protocol that details the review method was developed a priori following an initial discussion among the members of the research team.
Focused question (PICO)
The focused question to be answered is: What is the effect of playing background music as compared to no music on dental anxiety and physiological parameters in adolescent and adult patients undergoing a dental treatment?
Eligibility criteria
The following criteria were imposed for inclusion in the systematic review:
Randomized clinical trials (RCTs) or controlled clinical trails (CCTs)
Carried out in humans: Adults and adolescents (≥13 years)
Undergoing dental treatment
Intervention: Playing background music (via loudspeakers or headphones)
Comparison: No music
Outcome parameters measured before and after dental treatment: Anxiety (AX; scale or questionnaire), systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and respiratory rate (RR).
Search strategy
To retrieve all the scientific papers concerning the effect of music on dental anxiety of adult patients during their dental treatment, a structured search method was used (Figure 1). To find appropriate papers that would address the main question the search strategy was modified appropriately regarding differences in controlled vocabulary and syntax rules for each database. The MEDLINE-PubMed, EMBASE, and Cochrane-CENTRAL database were searched for applicable papers from inception until September 2020 (F.N.W., D.E.S.). The reference lists of the included studies were hand-searched to identify additional potentially relevant studies.
Search Terms Used for PubMed-MEDLINE, Cochrane-CENTRAL and EMBASE. The Search Strategy Was Customized According to the Database Being Searched.
Screening and selection
Titles and abstracts of the studies obtained from the searches were screened independently by two reviewers (F.N.W., D.E.S.) and were categorized as definitely eligible, definitely not eligible, or questionable. No language restrictions were imposed. No attempt was made to blind the reviewers to the names of authors, institutions, or journals while making the assessment. If eligible aspects were present in the title, the paper was selected for further reading. If none of the eligible aspects were mentioned in the title, the abstract was read in detail to screen for suitability. Papers that could potentially meet the inclusion criteria were obtained and read in detail by the two reviewers (F.N.W., D.E.S.). Disagreements in the screening and selection process concerning eligibility were resolved by consensus. The papers that fulfilled all of the inclusion criteria were processed for data extraction.
Risk of bias assessment
The potential risk of bias of the included papers was scored by two independent reviewers (F.N.W., D.E.S.). If there was a disagreement between the two reviewers, a consensus was achieved through discussion. A checklist for RCTs was used as proposed by Van der Weijden et al. (2009) (Online Appendix S1). In brief, when defined inclusion/exclusion criteria, random allocation, blinding to examiner and patient, balanced experimental groups, reporting to follow-up and identical treatment between groups were present, an article was classified as having a “low risk of bias.” If the article missed one of these criteria, it was considered to have a “moderate risk of bias.” If two or more of these criteria were missing, the article was considered having a “high risk of bias.”
Data extraction
From all eligible and included studies, the characteristics of the population, intervention, comparison, and outcomes were extracted by two independent reviewers (F.N.W., D.E.S.). A specially designed data extraction form was used. If there was a disagreement between the two reviewers, a consensus was achieved through discussion. Not all the papers provided sufficient data to be included in the analysis. For these papers, the first or the corresponding authors were approached via mail to request the missing data.
Data analysis
As a summary, a descriptive data presentation was used for all studies. Studies were categorized relative to the style of music and dental procedure. Subsequently, where feasible, a meta-analysis was performed to explore the efficacy of playing background music versus no music on the various parameters (Review Manager, version 5.3 for Windows, The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark). A meta-analysis was only performed if more than one study could be included irrespective of the number of comparisons. The difference of means between test and control was calculated using a random effects model. The goal was to estimate the mean effect in a range of studies where the overall estimate is not overly influenced by any one of them (Borenstein, Hedges, Higgins, & Rothstein, 2010). If possible, formal testing for publication bias was used as proposed by Egger, Smith, Schneider, and Minder (1997).
Assessment of heterogeneity
Several factors were used to evaluate the clinical and methodological heterogeneity across the included studies: Study design, dental procedure, style of music and method of dental anxiety assessment. As part of the meta-analysis, heterogeneity was statistically tested by the chi-square test and the I2 statistic. A chi-square test resulting in a p < .1 was considered an indication of significant statistical heterogeneity. As an approximate guide to assessing the possible magnitude of inconsistency across studies the I2 statistic was interpreted as follows: 0%–40% indicates unimportant levels of heterogeneity, 30%–60% may represents moderate heterogeneity, 50%–90% represents substantial heterogeneity, and an I2 statistic of greater than 75% indicates considerable heterogeneity (Ryan, 2016).
Rating the certainty and quality of the evidence
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was used, as proposed by the GRADE working group (2000), to appraise the evidence emerging from this review. Two reviewers (F.N.W., D.E.S.) rated the quality of the evidence, and the strength and direction of the recommendations (Guyatt et al., 2008) according to the following aspects: risk of bias, consistency of results, directness of evidence, precision and publication bias, and magnitude of the effect. Any disagreement between the two reviewers was resolved after additional discussion.
Results
Search and selection results
From the search actions on MEDLINE-PubMed, EMBASE and Cochrane-CENTRAL, 150 unique papers emerged (see Figure 2). Eighteen papers were selected for full-text reading upon screening of the titles and abstracts. After a detailed reading of these selected papers, five papers were excluded. One of these concerned just a study protocol and three were congress abstracts (Hernandez, Baeza, & Espinoza, 2013; Salvador-Hernandez Rodrigues, 1999; Žugaj, Vranic, & Katusic, 2017). Two of the five excluded papers (Keilani et al., 2017; Mejia-Rubalcava, Alanis-Tavira, Mendieta-Zeron, & Sanchez-Perez, 2015) played music solely pre-operatively. No other publications were revealed while manually searching the reference lists of the selected papers. Finally, 13 eligible papers were included in this review (Apostolova et al., 2017; Aravena, Almonacid, & Mancilla, 2020; Corah, Gale, Pace, & Seyrek, 1981; Di Nasso et al., 2016; Gulnahar & Kupeli, 2020; Kim et al., 2011; Kupeli & Gulnahar, 2020; Lahmann et al., 2008; Lai et al., 2008; Maulina, Djustiana, & Shahib, 2017; Packyanathan, Lakshmanan, & Jayashri, 2019; Santana et al., 2017; Yamashita, Kibe, Ohno, Kohjitani, & Sugimura, 2019) which provided 23 comparisons. One study (Di Nasso et al., 2016) provided four comparisons based on different preoperative anxiety levels, two studies (Gulnahar & Kupeli, 2020; Kupeli & Gulnahar, 2020) provided three comparisons based on different types of music, and three studies (Aravena et al., 2020; Corah et al., 1981; Maulina et al., 2017) provided two comparisons also based on different types of music.
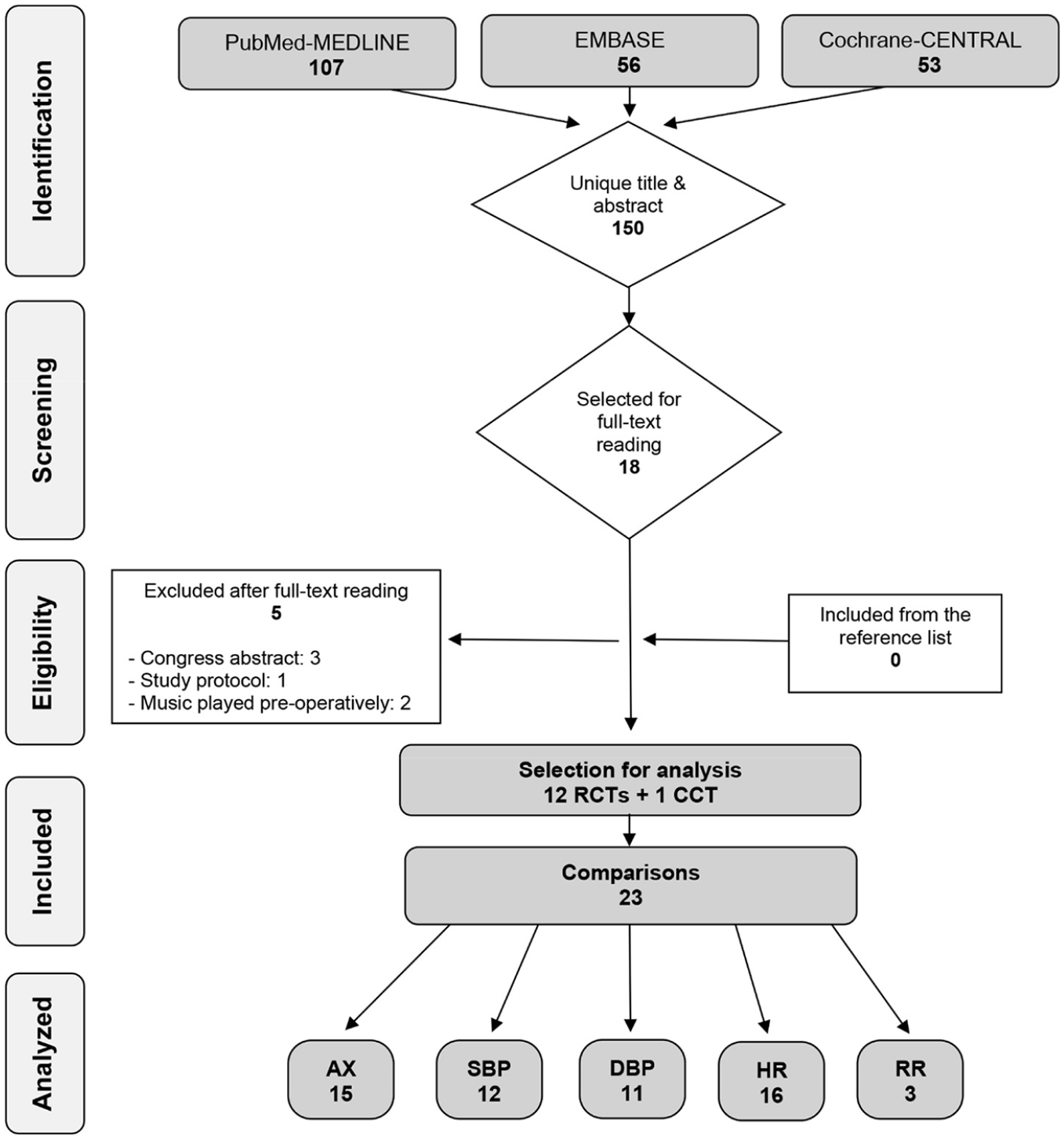
Flow Chart of Search Actions.
Study characteristics
The study characteristics of the included papers are listed in Table 1. Twelve studies were RCTs, one study was a CCT. Sample sizes ranged from 35 to 232 participants. Different types of dental treatments were performed: extraction (6 studies), endodontic treatment (3 studies), caries treatment (2 studies), implant surgery (1 study), and “oral surgery” (1 study). Also different types of music were used as intervention: classical music (6 studies), non-classical relaxing music (3 studies), Islamic/Turkish music (3 studies), soft rock (2 studies), and various music styles (2 studies). Five studies used multiple intervention groups with different types of music. The background music was played via headphones (9 studies) or loudspeakers (2 studies). Two studies lacked information on how the music was played.
Overview of the studies processed for data extraction.
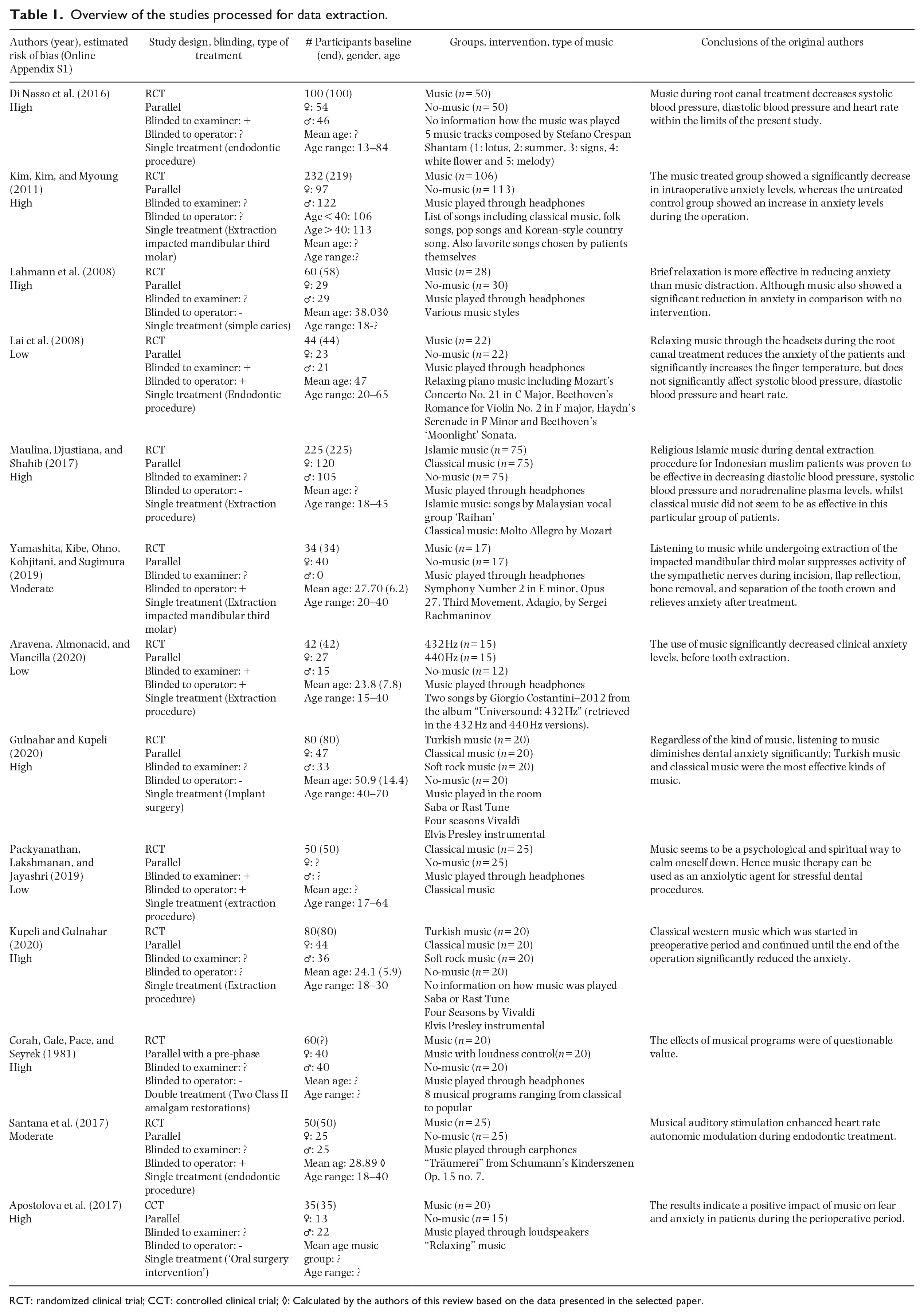
RCT: randomized clinical trial; CCT: controlled clinical trial; ◊: Calculated by the authors of this review based on the data presented in the selected paper.
Nine included studies examined AX as an outcome measure. Four types of anxiety scales were used (Online Appendix S2). The State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, & Lushene, 1983) was used by three studies (Lahmann et al., 2008; Lai et al., 2008; Yamashita et al., 2019), Corah’s Dental Anxiety Scale (CDAS; Corah, 1969) by four studies (Corah et al., 1981; Gulnahar & Kupeli, 2020; Kim et al., 2011; Kupeli & Gulnahar, 2020) and Corah’s Modifed Dental Anxiety Scale (Humphris, Morrison, & Lindsay, 1995; Coolidge et al., 2010) by three studies (Aravena et al., 2020; Packyanathan et al., 2019; Yamashita et al., 2019).
Of these nine studies, five had participants with high anxiety at baseline (Aravena et al., 2020; Kim et al., 2011; Lahmann et al., 2008; Lai et al., 2008; Yamashita et al., 2019), two studies had participants with mild anxiety at baseline (Gulnahar & Kupeli, 2020; Kupeli & Gulnahar, 2020). The other two studies lacked information on baseline anxiety (Corah et al., 1981; Packyanathan et al., 2019). Di Nasso and colleagues (2016) did not examine anxiety as outcome measure. However, they used CDAS to create four groups based on different preoperative anxiety levels (see Online Appendix S3-5). Also Maulina and colleagues (2017) did not examine anxiety as outcome measure, but used the Modifed Dental Anxiety Scale as a filtering tool for screening anxious participants.
Risk of bias assessment
The potential risk of bias was estimated based on the methodological quality aspects of the included studies as presented in the Online Appendix S1. All studies had balanced experimental groups. Blinding to operator was realized in 5 of the 13 studies, by letting both groups wear headphones. In the control group, the headphones were turned off (Santana et al., 2017; Yamashita et al., 2019), in noise cancelation mode (Aravena et al., 2020; Packyanathan et al., 2019), or a CD of silence was played (Lai et al., 2008). In seven studies, the treatment was identical except for the intervention, because both groups wore headphones (Aravena et al., 2020; Lai et al., 2008; Packyanathan et al., 2019; Santana et al., 2017; Yamashita et al., 2019), or because the music was played via loudspeakers (Apostolova et al., 2017; Gulnahar & Kupeli, 2020). Based on a summary of the proposed criteria, the potential risk of bias was estimated to be low for three studies (Aravena et al., 2020; Lai et al., 2008; Packyanathan et al., 2019), moderate for two (Santana et al., 2017; Yamashita et al., 2019) and high for the other eight studies (Apostolova et al., 2017; Corah et al., 1981; Di Nasso et al., 2016; Gulnahar & Kupeli, 2020; Kim et al., 2011; Kupeli & Gulnahar, 2020; Lahmann et al., 2008; Maulina et al., 2017).
Descriptive analysis
Table 2 summarizes the descriptive analysis for the statistical differences between the music and no music groups regarding AX, SBP, DBP, HR, and RR. When reported, the statistical differences were obtained from the full text articles. When not reported, the statistical differences were adapted from the meta-analysis. When a meta-analysis for the incremental scores was available, this was used. When not available, the meta-analysis for the end scores was used.
A descriptive summary of statistical significance with music compared to no music during dental treatment.
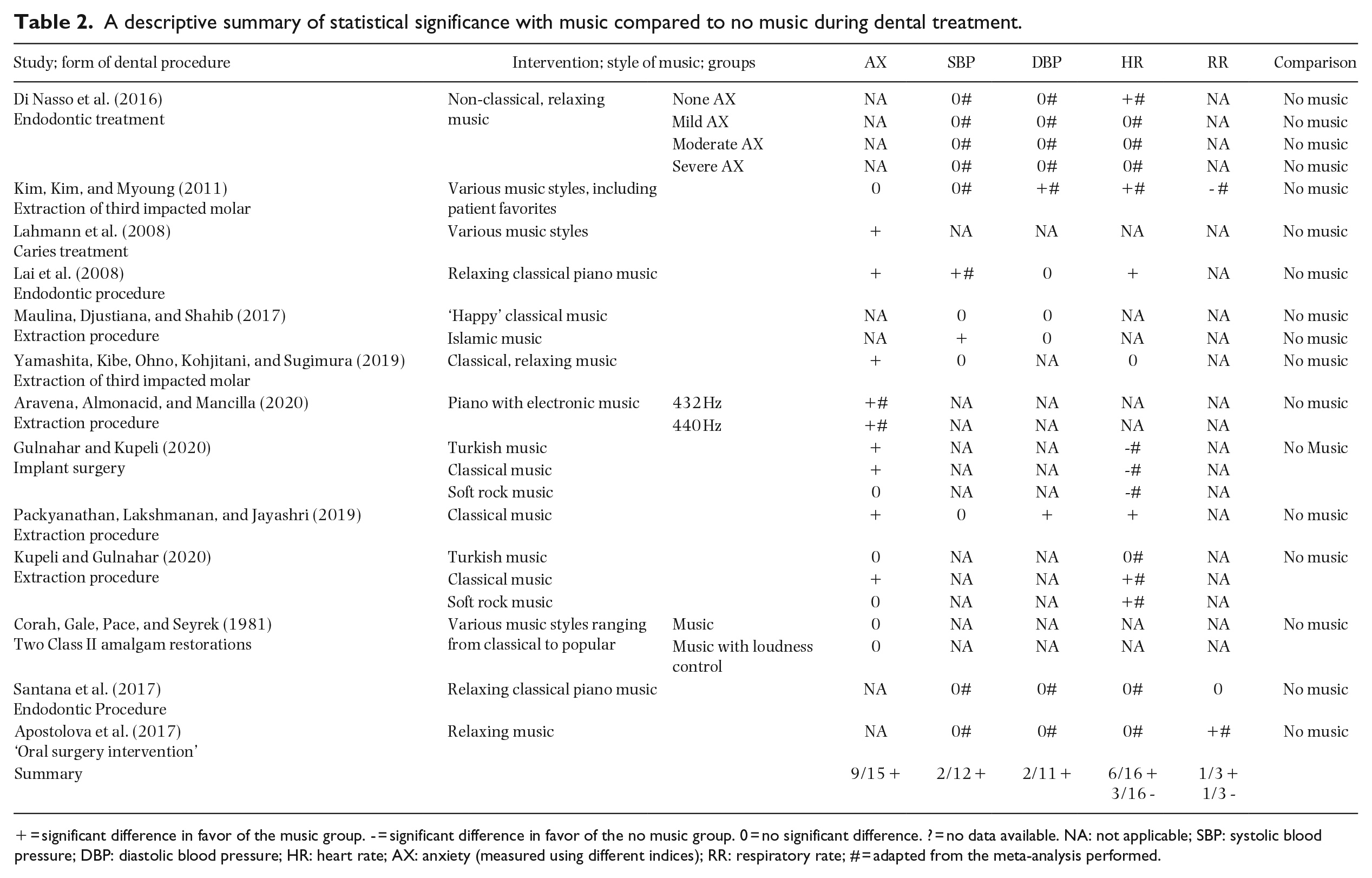
= significant difference in favor of the music group. - = significant difference in favor of the no music group. 0 = no significant difference. ? = no data available. NA: not applicable; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; AX: anxiety (measured using different indices); RR: respiratory rate; # = adapted from the meta-analysis performed.
For the outcome parameter AX, 9 out of 15 studies showed a significant difference in favor of the music group. For the physiological parameters, the outcomes were less consistent. For SBP and DBP, 2 out of respectively 12 and 11 studies showed a significant difference in favor of the music group. For HR, 6 out of 16 studies showed a significant difference in favor of the music group, while 3 out of 16 studies showed a significant difference in favor of the control group. For RR, 2 out of 3 studies showed a significant difference, one in favor of the music group and the other in favor of the control group.
Studies were categorized relative to the style of music and dental procedure (Table 3). Classical music and non-classical relaxing music showed the most marked effect on AX. For the other music styles the effect was inconclusive. The effect of the music intervention on the physiological parameters was indecisive.
A descriptive subgroup analysis relative to the style of music intervention and dental procedure.
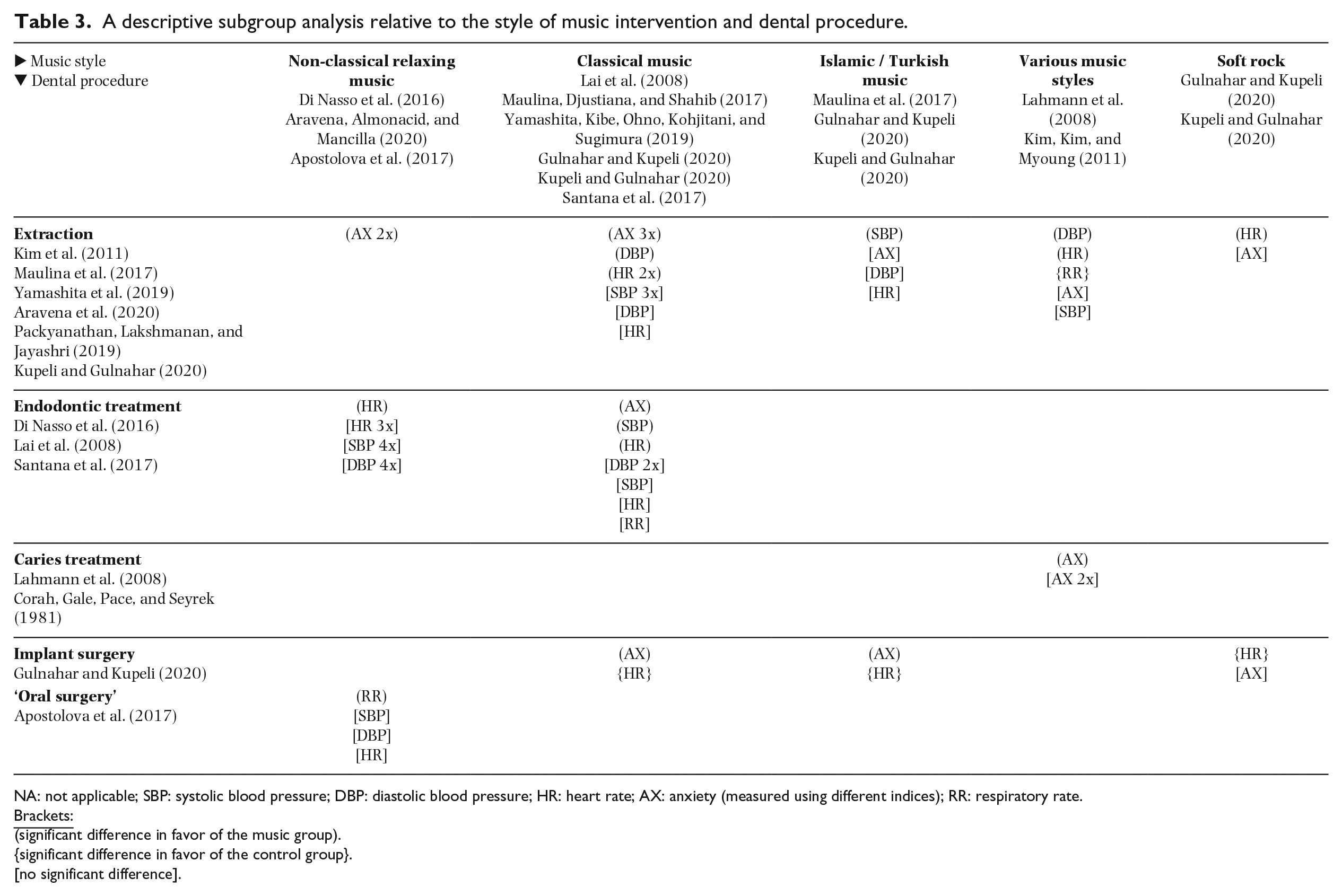
NA: not applicable; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; AX: anxiety (measured using different indices); RR: respiratory rate.
(significant difference in favor of the music group).
{significant difference in favor of the control group}.
[no significant difference].
Meta-analysis
Online Appendix S2-6 presents the results of the data extraction from the selected studies for the various clinical indices. When available, the baseline, end and incremental scores are presented. A meta-analysis was feasible for all parameters.
Online Appendix S7-23 present forest plots of the meta-analysis. The green squares indicate the mean difference, while the horizontal lines connected to the squares show the 95% confidence interval. Intersection of the horizontal lines with the zero axis indicates an insignificant difference, whereas the difference of means (DiffM) size will increase the further the horizontal lines are from zero. The summary evaluation as overall DiffM at the bottom row is depicted by a black diamond symbol. The center is the point estimate and the width represents the 95% confidence interval. Significance is interpreted based on whether or not zero is incorporated in the interval.
Table 4 summarizes the detailed outcomes of the performed meta-analysis. Significant differences were found for AX and SBP. The meta-analysis on STAI-S (AX) showed a significant difference in favor of the music group for the end scores, DiffM: -6.35, p < .00001, 95% CI = [-8.61; -4.09]; I2 = 0%, p = .53 (based on three studies). No significant difference was found for the incremental scores, for which only two studies provided data for the meta-analysis. The meta-analysis on CDAS (AX) showed a significant difference in favor of the music group for the end scores, DiffM: -1.57, p = .02, 95% CI = [-2.93; -0.22]; I2 = 79%, p < .0001 (based on four studies/nine comparisons) and incremental scores, DiffM: -2.33, p = .0002, 95% CI = [-3.55; -1.11]; I2 93%, p < .00001 (based on three studies/eight comparisons), however with high heterogeneity. The meta-analysis on SBP showed a significant difference in favor of the music group for the incremental scores, DiffM: -5.34, p = .02, 95% CI = [-9.66; 1.03]; I2 = 0%, p = .92 (based on two studies/five comparisons). No significant difference was found for the end scores, for which five studies (eight comparisons) provided data for the meta-analysis.
Meta-analysis (random effect) for music compared to no music for baseline, end and incremental (difference) scores as obtained for the variables AX, SBP, DBP, HR, and RR.
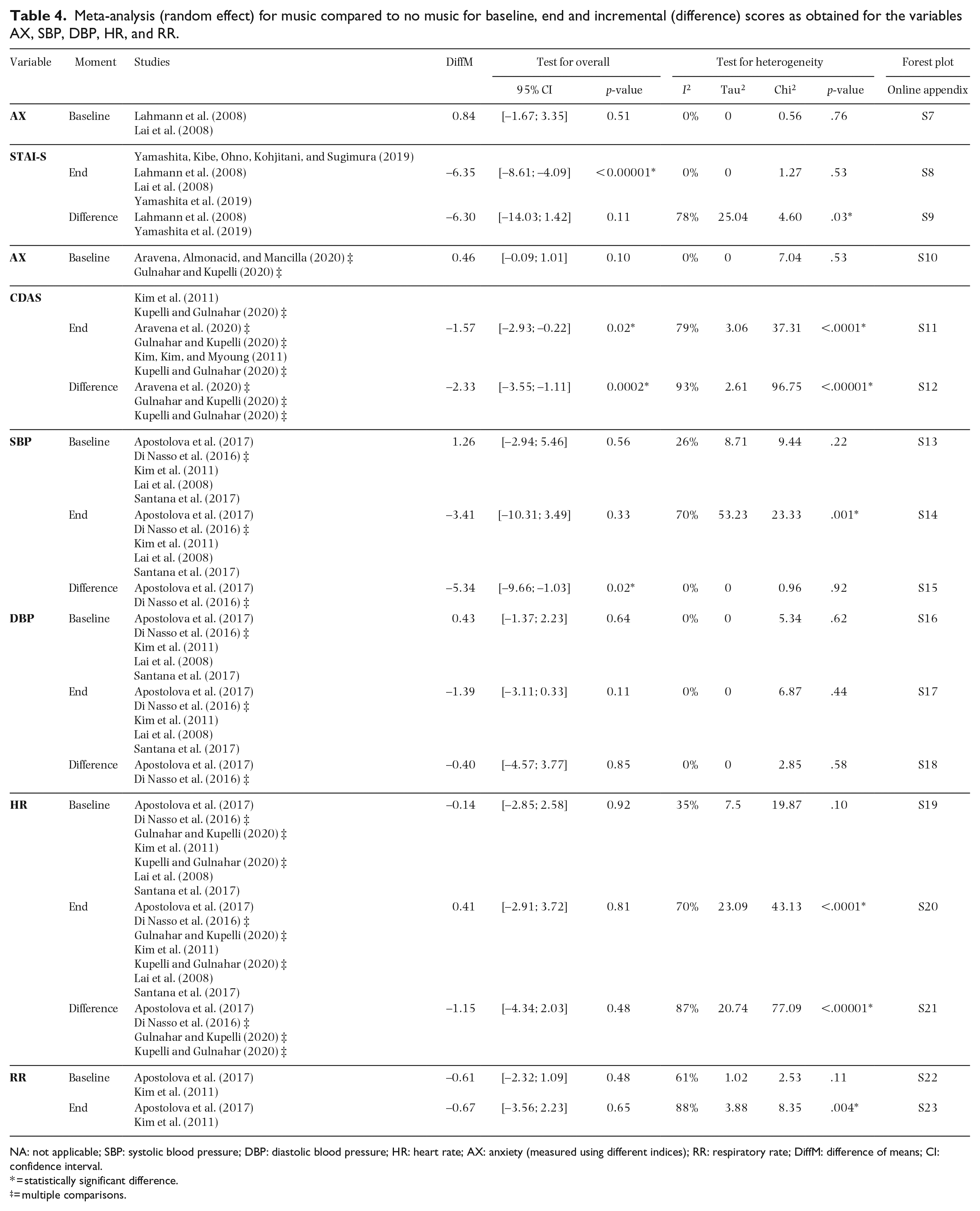
NA: not applicable; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; AX: anxiety (measured using different indices); RR: respiratory rate; DiffM: difference of means; CI: confidence interval.
= statistically significant difference.
= multiple comparisons.
Testing for publication bias could not be performed for most meta-analysis because fewer than 10 studies were included, which would result in insufficient statistical power (Egger et al., 1997; Higgins et al., 2011). Only for the meta-analysis of HR scores more than 10 comparisons were included. The funnel plots (Online Appendix S24-26) show that most outcomes are located at the top. The presence of this asymmetry in the inverted funnel is suggestive of publication bias.
Rating the certainty and quality of the evidence
Table 5 presents a summary of the various factors used to rate the strength and quality of evidence according to criteria proposed by the GRADE working group (2000) and Guyatt and colleagues (2008). The outcomes for AX were rather consistent with a small effect in favor of music intervention. The outcomes for SBP and DBP were (rather) consistent with no effect of music intervention. The outcomes for HR were inconsistent with no effect of music intervention. As a meta-analysis with 8 to 12 comparisons could be performed for AX, SBP, DBP and HR, the outcomes were precise. The outcomes for RR were inconclusive due to the very small number of included studies. The outcomes for the physiologic parameters were generalizable, while the outcomes for the AX were rather generalizable because of the use of questionnaires. Reporting bias could for most parameters not be assessed and therefore can also not be ruled out. For HR, the funnel plots indicate that outcomes could be overestimated so that the presence of reporting bias is likely. Furthermore, the potential risk of bias was estimated to be low to high. Therefore, the strength of the evidence emerging from this systematic review was estimated to be moderate for AX, SBP, DBP and HR, and very low for RR.
Summary of the estimated evidence profile (GRADE, 2000; Guyatt et al., 2008).
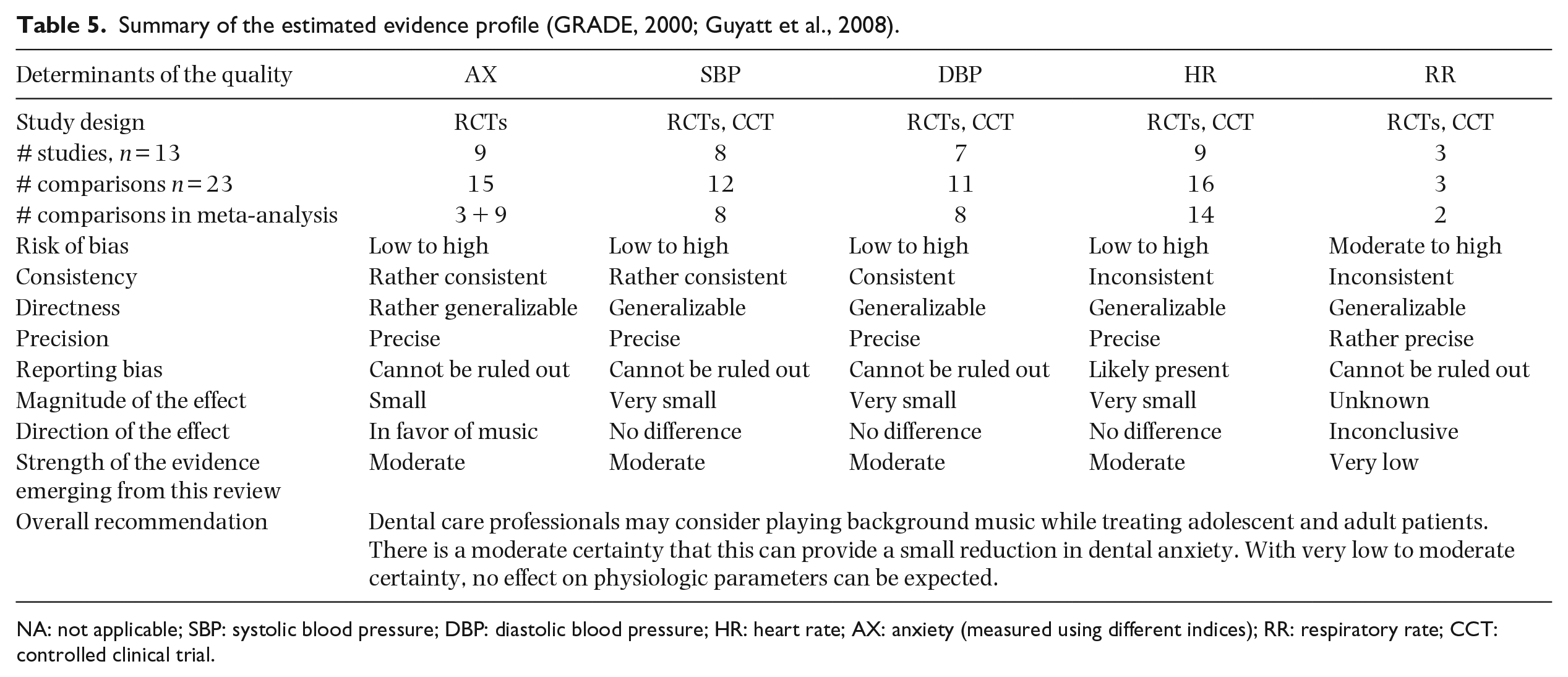
NA: not applicable; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; AX: anxiety (measured using different indices); RR: respiratory rate; CCT: controlled clinical trial.
Discussion
Answer to the focused question
This is the first systematic review that synthesizes the effects of playing background music on dental AX and physiological parameters in adolescent and adult patients undergoing a dental treatment. Based on the data emerging from the studies included in this systematic review, the descriptive and meta-analysis shows that music intervention may give a small reduction in AX. While descriptive analysis indicated no effect of background music on SBP, meta-analysis shows a significant difference in favor of the music group on the difference scores. For DBP, both descriptive and meta-analysis indicated no effect of background music. For HR, both descriptive and meta-analysis showed an inconsistent pattern, with some studies indicating an effect in favor of the music group, while other studies indicating an effect in favor of the control group. For RR, the number of studies was too small to reach a conclusion. Overall, a small psychological effect of playing background on dental anxiety can be expected, but no effect on physiological parameters.
Psychological mechanisms underlying emotion reactions to music
Juslin (2013) formulated a framework (BRECVEMA) which includes eight mechanisms of how music can influence emotions such as anxiety:
Brain stem reflex: One or more fundamental acoustic characteristics of the music are taken by the brain stem to signal a potentially important and urgent event that needs attention. In music, this could involve sounds that are sudden, loud, or dissonant, or accelerating. Brain stem reflexes may induce general arousal and feelings of surprise.
Rhythmic entrainment: A powerful, external rhythm in the music influences some internal bodily rhythm of the listener (e.g., heart rate), such that the latter rhythm adjusts toward and eventually “locks in” to a common periodicity. Rhythmic entrainment may induce general arousal and feelings of communion.
Evaluative conditioning: A regular paring of a piece of music and other positive or negative stimuli, leading to a conditioned association. For example, a particular piece of music may have occurred repeatedly together in time with a specific event that always make you happy, such as meeting you friends. Over time, through repeated pairing, the music itself will eventually arouse happiness, even in the absence of the friendly interaction. Evaluative conditioning may induce basic emotions.
Emotional contagion: The listener perceives the emotional expression of the music, and then “mimics” this expression internally. The idea is that we become aroused by voice-like features of the music because a “brain module” responds automatically to certain stimulus features as if they were coming from a human voice expressing emotions. Emotional contagion may induce basic emotions.
Visual imagery: The listener conjures up inner images (e.g., a beautiful landscape) while listening to the music. It may arouse feeling of pleasure and deep relaxation. Visual imagery may induce all possible emotions.
Episodic memory: The music evokes a personal memory of a specific event in the listeners’ life. When the memory is evoked, so is also the emotion associated with the memory. Episodic memories may induce all possible emotions, but especially nostalgia.
Musical expectancy: a specific feature of the music violates, delays, or confirms the listener’s expectations about the continuation of the music. The expectations are based on the listener’s previous experience of the same music style. Musical expectancy may induce emotions such as interest, anxiety, surprise, chills, hope and disappointment.
Aesthetic judgment: when certain aspect of the music’s form and content are evaluated by the listener with regard to their value as art. Aesthetic judgment will either result in liking (preference) or dislike.
Style of music
Based on the BRECVEMA framework (Juslin, 2013), the activation of different psychological mechanisms induce different emotional reactions. To make a patient feel more relaxed in the dental chair, certain mechanisms (e.g rhythmic entrainment, visual imagery) are more desirable to occur than others (e.g., brain stem reflexes, musical expectancy). Therefore the choice of music genre could be of importance to decrease AX.
Our descriptive analysis showed that classical and relaxing music were most effective in reducing AX. This is in accordance with the literature. Studies have shown that classical music has larger effects on the reduction of stress than non-classical music such as heavy metal music and hard rock music (Burns et al., 2002; Labbe, Schmidt, Babin, & Pharr, 2007). Other studies have shown that romantic music and stimulating classical music make the participants significantly more relaxed than atonal music (Stratton & Zalanowski, 1984), while no difference is found between the genres pop, classical and jazz music in decreasing the levels of state anxiety and relaxation (Chafin, Roy, Gerin, & Christenfeld, 2004). In terms of levels of arousal, music is also categorized as relaxing and stimulative music. Relaxing music is generally characterized as soft and slow, with less rhythmic activity, while stimulative music has loud volume, fast tempos, and more rhythmic patterns (Iwanaga, Ikeda, & Iwaki, 1996; Pellitteri, 2009). In a study by Jiang, Zhou, Rickson, and Jiang (2013) the effects of stimulative and relaxing music and music preference on stress reduction was evaluated. Significantly lower levels of tension and state-anxiety were found when participants listened to relaxing music compared to stimulative music when the music was non-preferred. No difference was found between stimulative and relaxing music when the music was preferred by the patient. These findings demonstrate that music preference can maximize the anxiolytic effect of musical intervention. Therefore, respecting the patient choice and taste of music appears necessary to obtain the optimal effect of music intervention.
Walczak, Turska-Szybka, Kollar, and Olczak-Kowalczyk (2016) asked patients to select a style of music they are most likely to listen to during dental treatment and to specify if they would choose headphones or not. Women chose classical music (43.33%), pop music (25%) and the sounds of nature (18.33%). Men’s answers were more diverse: classical music (25%), rock music (25%), pop music (20.45%), the newest hits (18.18%), hip hop (15,91%) and soundtracks (15.91%). A comparable number of men (13.64%) and women (11.67%) would prefer silence during the dental appointment. The majority of the respondents, declared they would prefer to listen to music from loudspeakers.
Music preference may also depend on the ethnical or religious background. One study included in this review (Maulina et al., 2017) was conducted among Indonesian Islamic participants. In the classical music group DBP and SBP increased, while in the Islamic music group DBP and SBP decreased. A possible reason could be that most of the participants in the study were more familiar with religious Islamic music.
The dental care professional should also take into account that not every patient experiences listening to music as relaxing. There are also patients that do not like music at all (Mok & Wong, 2003). So if the operators strive for quality patient-centered care then proper communication before the treatment is crucial to obtain the most accurate information regarding the patients music preferences (Jiang et al., 2013; Mok & Wong, 2003).
Pre-operative music
The aim of this study was to determine the effects of music on AX during a dental treatment, but music played pre-operatively also presents beneficial effects on AX, as was investigated by Thoma and colleagues (2015). Ninety-two adult patients waiting for their scheduled dental hygiene treatment were randomly allocated to either listening to music for 10 minutes or waiting in silence. State anxiety levels in the music group decreased significantly as compared to the control group. Mejia-Rubalcava et al. (2015) found that patients who listened to music pre-operatively had significant lower HR, SBP and DBP than the control group. Thus, considering those facts, further research needs to be conducted on the effects of music played both pre-operatively and peri-operatively, as a combination of music played during the treatment and in the waiting room could prove to be a more viable anxiolytic treatment.
Effect of music on dental staff
This systematic review shows that music played during dental treatment may help patients to feel more relaxed in the dental chair. At the same time, when the music is played via loudspeakers, it may have an influence on the performance of the operator and communication in the dental team. This has been investigated in the environment of an hospital operating room. Literature shows that music can increase the speed and accuracy of task performance of the surgeon (Lies & Zhang, 2015; Moris & Linos, 2013). However, music played in the operating theater can also interfere with team communication (Moris & Linos, 2013; Weldon, Korkiakangas, Bezemer, & Kneebone, 2015)
Limitations
Six of the included studies performed assessments before, during and after dental treatment (Di Nasso et al., 2016; Gulnahar & Kupeli, 2020; Kim et al., 2011; Kupeli & Gulnahar, 2020; Lai et al., 2008; Santana et al., 2017) while the others gathered data pre- and post-operatively. To be consistent for this review only the data obtained pre- and post-operatively were extracted and used for the meta-analysis. This may be seen as a limitation because parameters may decrease by themselves when the dental treatment has come to an end, once the patient “survived” the trigger which caused anxiety. For the future measuring these parameters during the dental treatment would improve our understanding of the direct effect of an relaxing intervention on AX.
A limitation of two included studies is that headphones with noise cancelation mode were used in the control group (Aravena et al., 2020; Packyanathan et al., 2019). Noise cancelation takes away the sound of the dental drill and may therefore reduce the triggers causing anxiety. However, one congress abstract that was not included in this systematic review (Hernandez et al., 2013) showed that the effect of noise cancelation on reduction of dental anxiety, if present at all, is probably minimal. In their study patients were divided in three groups: musical intervention, protective earphones and control group. The musical intervention group showed significant lower AX, SBP, DBP, and cardiac frequency than the other two groups.
Clinical relevance
During dental treatment listening to music may help patients to relax. Adolescent and adult patients could be offered music as an alternative and/or additional anxiolytic treatment. Classical music, relaxing music or music preferred by the patient can be played via loudspeakers or by using headphones.
Conclusion
There is a moderate certainty that playing background music during dental treatment can provide a small reduction in dental anxiety among adolescent and adult patients. With very low to moderate certainty, no effect on physiologic parameters can be expected.
Supplemental Material
sj-pdf-1-pom-10.1177_0305735621998439 – Supplemental material for The effect of playing background music during dental treatment on dental anxiety and physiological parameters: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-pom-10.1177_0305735621998439 for The effect of playing background music during dental treatment on dental anxiety and physiological parameters: A systematic review and meta-analysis by Fawn Nitanee van der Weijden, Ahsan Mehran Hussain, Leo Tang and Dagmar Else Slot in Psychology of Music
Footnotes
Acknowledgements
The authors are grateful to the following authors for their response, time and effort to search for additional data: Dr. Toshiro Kibe (Yamashita et al.), Dr. Pedro Aravena Torres, Dr. Gordana Apostolova, Dr. Luca di Nasso, and Dr. Tantry Maulina.
Author contributions
All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy. F.N.W.: contributed to conception, design, search and selection, analysis and interpretation, and critically revised the manuscript. A.M.H. and L.T.: contributed to design, search and selection, analysis and interpretation, and drafted the manuscript. D.E.S.: contributed design, search and selection, analysis and interpretation, and critically revised the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was in part prepared as obligation of A.M.H. & L.T. to fulfill the requirements of the ACTA bachelor program Dentistry. All authors declare that they have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work for this paper is only funded by a regular academic appointment of F.N.W. & D.E.S. at the Academic Center for Dentistry Amsterdam (ACTA).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.