
Abstract
Music performance anxiety (MPA) is considered a social anxiety disorder (SAD). Recent conceptualizations, however, challenge existing MPA definitions, distinguishing MPA from SAD. In this study, we aim to provide a systematic analysis of MPA interdependencies to other anxiety disorders through graphical modeling and cluster analysis. Participants were 82 music students (Mage = 23.5 years, SD = 3.4 years; 69.5% women) with the majority being vocal (30.5%), string (24.4%), or piano (19.5%) students. MPA was measured using the German version of the Kenny Music Performance Anxiety Inventory (K-MPAI). All participants were tested for anxiety-related symptoms using the disorder-specific anxiety measures of the Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5), including agoraphobia (AG), generalized anxiety disorder (GAD), panic disorder (PD), separation anxiety disorder (SEP), specific phobia (SP), SAD, and illness anxiety disorder (ILL). We found no evidence of MPA being primarily connected to SAD, finding GAD acted as a full mediator between MPA and any other anxiety type. Our graphical model remained unchanged considering severe cases of MPA only (K-MPAI ⩾ 105). By means of cluster analysis, we identified two participant sub-groups of differing anxiety profiles. Participants with pathological anxiety consistently showed more severe MPA. Our findings suggest that GAD is the strongest predictor for MPA among all major DSM-5 anxiety types.
Over the last decades, the knowledge of psychopathology, particularly of anxiety disorders, grew substantially. With the publication of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), the traditional categorical approach was extended by a dimensional assessment of psychopathology allowing to assess sub-clinical representations and disorder-specific severity as well as symptom changes over time (Lebeau et al., 2012). Despite its common occurrence, however, performance anxiety in general, and more specifically music performance anxiety (MPA), received less attention in diagnostic classification systems. It still seems to be a rather neglected psychological phenomenon and is rarely discussed in conventional psychological journals or textbooks.
MPA is considered a special form of emotional behavior related to reactions of the nervous system, motor expressive behavior, cognitive appraisal, subjective feelings, and behavioral changes (Kesselring, 2006). It is important to note that MPA is not exclusively a problem of the individual but is partly influenced by a performer’s cultural group (Leech-Wilkinson, 2016; Perdomo-Guevara, 2014). For instance, it has been shown that classical musicians conceptualize performance-related emotions differently from non-classical musicians, that is, reporting a more self-oriented performance view and fewer positive performance experiences compared to non-classical musicians (Perdomo-Guevara, 2014). Unfortunately, epidemiological data of its prevalence are difficult to interpret given the lack of a consistent definition of terms, according to which MPA among musicians ranges from 16.5% to 60% (Fernholz et al., 2019). While a certain degree of arousal is often necessary for an optimal performance, excessive levels of MPA will almost certainly impair performance quality. This relationship is often described as an inverted-U curve, referred to as the Yerkes–Dodson Law. Wilson (2002) refined this relationship by proposing a three-dimensional extension considering grouping major sources of stress into three categories including trait anxiety (a personal characteristic), situational stress (environmental pressures, for example, public performances or auditions), and task mastery (performance of well-rehearsed simple, or under-rehearsed more complex work). The extent to which MPA may be beneficial or debilitating depends on the interplay of these factors. In that way, the nature of MPA differs from most anxiety disorders where the expression of more symptoms often means a more severe expression of the disorder itself. Inconsistent terms have been used to refer to normal or severe levels of performance anxiety; in this article, we refrain from using such terminology. Instead, we refer to normal levels of performance anxiety as MPA and abnormal levels of performance anxiety as “severe” or “debilitating” MPA throughout the article.
Most musicians report MPA directly prior and during a performance; however, some musicians may report anticipation anxiety days, weeks, or even months before a performance (Van Kemenade, Van Son, & Van Heesch, 1995). Depression and anxiety disorders are frequently observed psychiatric co-morbidities when treating severe MPA. Kenny (2011) suggested a tripartite typology of MPA which differentiates between (a) severe MPA as a focal disorder in an otherwise healthy musician, (b) severe MPA as an expression of social anxiety, and (c) severe MPA as a more complex psychopathology in which case, the individual may suffer from an extreme combination of emotional, cognitive, and somatic anxiety as well as serious problems with the sense of self and self-esteem. Particularly, the link between MPA and social anxiety has been widely researched (e.g., Cox & Kenardy, 1993; Dobos, Piko, & Kenny, 2019; Kenny, 2011; Nicholson, Cody, & Beck, 2015). This is underlined by the fact that the DSM-5 now acknowledges evidence of individuals suffering exclusively from performance anxiety as a distinct sub-type of social anxiety disorder (SAD) by introducing a new specifier, performance only which replaces the old generalized specifier.
More recently, however, Kenny (2016) challenged existing definitions of MPA, trying to address inconsistencies with the emerging research and, most importantly, distinguishing MPA from SAD. Although MPA and SAD share common characteristics such as the fear of negative evaluation, both conditions repeatedly showed significant differences (for a discussion, see Kenny, 2008). Previous research by Gorges, Alpers, and Pauli (2007) showed that even though SAD highly correlates with MPA, only the performance anxiety sub-scale, not the fear of social interaction, predicts MPA. In our previous research article about the role of parenting style and adult attachment behavior in MPA, we found a strong relationship between MPA and generalized anxiety disorder (GAD; see Wiedemann, Vogel, Voss, Nusseck, & Hoyer, 2019). Finding that the expression of GAD was such as strong predictor of MPA, we conducted a literature search of MPA and its relation to other anxiety disorders finding that the vast majority of research does not consider GAD as a potential predictor of MPA. The DSM-5 anxiety sub-workgroup, however, suggests that performance anxiety in general should only be considered as an exemplar of SAD if fear of negative evaluation by others is the presenting core issue, whereas the predominance of a fear of failure in a non-social context should always be considered as a manifestation of GAD (Heimberg et al., 2014). Even though classification systems such as the DSM-5 have attracted considerable criticism (for an overview, see Pickersgill, 2013), they are a practical tool for both clinicians and researchers to integrate and guide empirical studies using standardized diagnostic criteria as well as to decide on treatment need and treatment choice (Caspi et al., 2014). Advancing our understanding of how MPA relates to other anxiety disorders may be particularly useful when considering potential treatment choices, for example, cognitive-behavioral therapists may use different tools depending on whether generalized (e.g., exposition) or social (e.g., reality testing) anxieties are more prevalent.
The lack of a systematic approach of MPA and its anxiety correlates in more broader terms, led to the aims of this study. First, by using an exploratory approach, where we consider all major anxiety disorders currently listed in the DSM-5, we will be able to shed further light onto the anxiety-related characteristics of MPA. This will also provide further evidence toward the debate of whether MPA should be considered in the context of SAD. Second, based on participants’ anxiety profiles, we will be able to establish different anxiety-related clusters. This will provide further insight into different typologies of MPA as introduced by Kenny (2011).
Methods
Participants
Data were obtained from 82 participants aged 18 to 33 years (M = 23.5, SD = 3.4 years; 69.5% women). An a priori power analysis showed a sample size of N = 82 is sufficient to draw statistically legitimate conclusions. Most participants were classical music students studying voice, strings, or piano. Other studied instruments, however, included woodwind, plucked, percussion, or brass as well as conducting. The full study characteristics relating to participants’ musical education can be seen in Table 1. At the time of the study, most participants were either single (n = 59, 72.0%) or married/ living together with their partner (n = 21, 25.6%), and rated their status of general health as excellent (n = 19, 23.2%), very good (n = 39, 47.6%), or good (n = 22, 26.8%). Sixteen subjects (19.5%) indicated regular medication intake such as, for example, hormonal contraception (n = 6), thyroid hormonal (n = 3), anti-allergic (n = 4), or antidepressant medication (n = 2). Twelve participants (14.6%) reported a chronic illness.
Sample characteristics (N = 82).
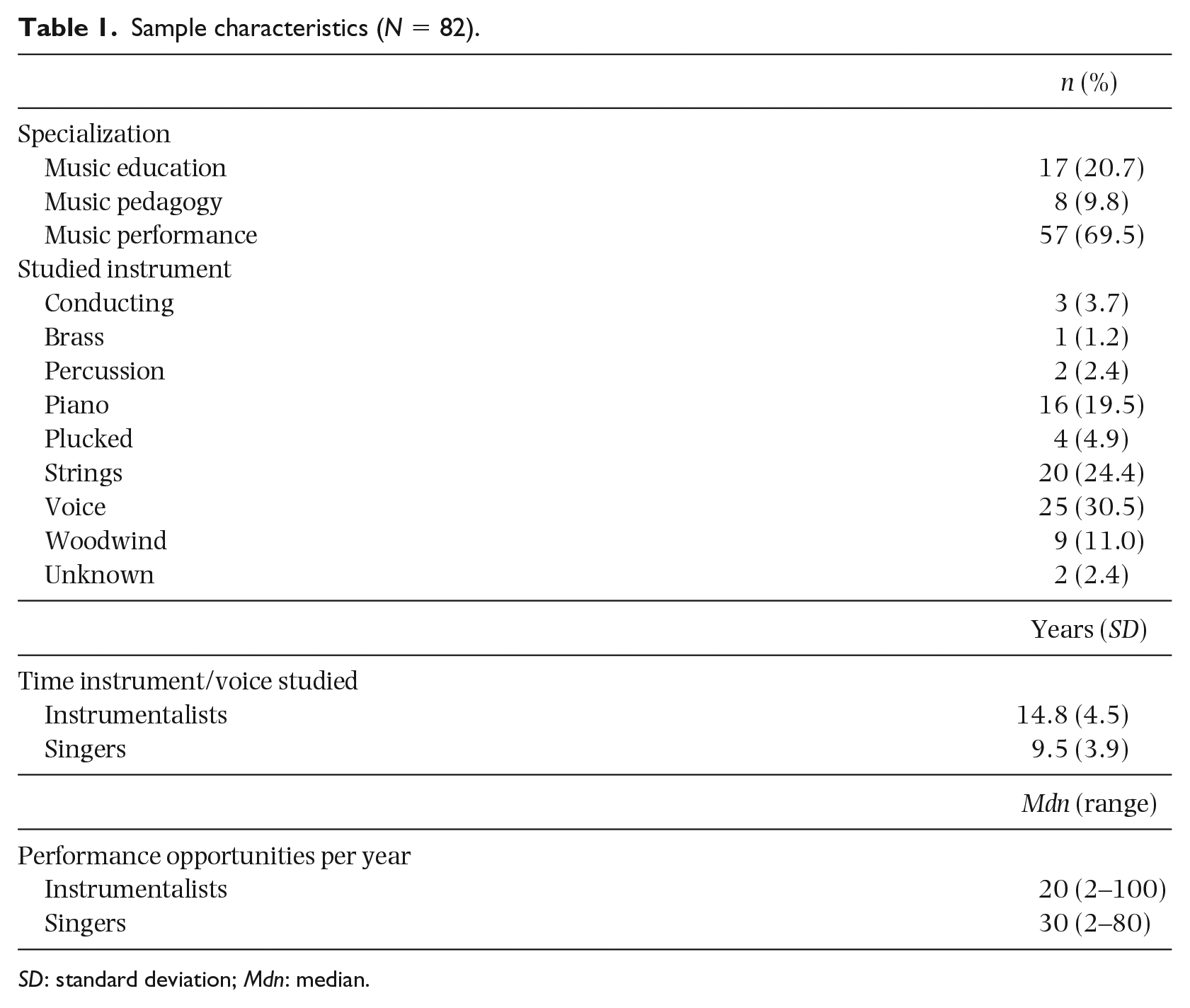
SD: standard deviation; Mdn: median.
Study design and procedure
A study protocol has been published previously (Wiedemann et al., 2019). Briefly, all data were provided by administering an online survey using LimeSurvey (Version 2.06 + Build 150731). Participants were recruited nationwide via university mailing lists as well as through face-to-face introductions in undergraduate lectures and seminars displaying survey invitations. Participants needed to be enrolled in a music program (Bachelor of Music/Master of Music) as well as showing sufficient language proficiency in German to participate in the study. Study participation was entirely voluntarily and could be withdrawn at any time without consequences. This study obtained ethical approval by the Ethics Committee of the Technical University Dresden (EK 28022012).
Measures
All measurements were self-rating instruments. General information was obtained about age, sex, nationality, marital status, studied instrument/time and specialization, the number of performance opportunities per year, general state of health measured by the general health item of the Short-Form 36 (Ware & Sherbourne, 1992) as well as regular use of medication and chronic diseases. Further assessment methods are outlined below.
Assessing anxiety
All participants were tested for anxiety-related symptoms using the German translation of the disorder-specific anxiety measures (Beesdo-Baum et al., 2012; Lebeau et al., 2012) which are the dimensional anxiety scales of the DSM-5 (American Psychiatric Association, 2013). Included were agoraphobia (AG), GAD, panic disorder (PD), separation anxiety disorder (SEP), specific phobia (SP), SAD as well as illness anxiety disorder (ILL). As obsessive-compulsive disorder is no longer listed under the broad umbrella of anxiety disorders in the DSM-5, it was not included in our study. Each measure included 10 items about thoughts, feelings, and behaviors, often tied to concerns about family, health, finances, school, or work which occurred during the past 7 days. Items were rated on a 5-point Likert scale ranging from never (0) to all of the time (4). A total score was created by summing all 10 item values resulting in a possible score range of 0 to 40 with higher scores indicating greater severity of the dimension. The average total score, calculated by dividing the raw score by the number of items, is thought to provide guidance of the severity indicating none (0), mild (1), moderate (2), severe (3), or extreme (4) manifestation of any anxiety disorder.
Assessing MPA
MPA was assessed using the German version of the Kenny Music Performance Anxiety Inventory (K-MPAI; Kenny, 2009) translated by Spahn, Walther, and Nusseck (2016). The K-MPAI is constructed based upon Barlow’s emotion-based theory of anxiety disorders (Barlow, 2000). It includes 40 questions related to psychological vulnerability (nine items), negative cognitions (six items), proximal somatic anxiety (seven items), parental empathy (three items), memory (two items), pre- and post-performance rumination (two items), generational transmission of anxiety (three items), self/other scrutiny (three items), controllability (two items), opportunity cost (one item), trust (one item), and pervasive anxiety (one item). Participants were asked to rate each item on a 7-point Likert scale ranging from strongly disagree (0) to strongly agree (6) resulting in a possible score range of 0 to 240 with higher scores indicating stronger MPA; scores ⩾105 may indicate severe levels of MPA (see Kenny, 2018).
Data analyses
We performed all statistical analyses in R version 3.3.3 (R Core Team, 2017) using the packages “ggm” for graphical modeling and “stats” for clustering.
Dependence analysis
We first computed the correlation coefficients and partial correlation coefficients between all pairs of variables. The partial correlation coefficient of two variables is the usual correlation coefficient computed from the residuals with respect to the linear regression of both variables on all remaining variables. It provides a measure of conditional (linear) dependence, which, roughly, describes the dependence which is not explained by other variables. Based on the partial correlations, we fitted a Gaussian graphical model. We set near-zero partial correlations (<.18) to zero and fitted a covariance matrix subject to the assumption that the identified near-zero partial correlations are indeed zero. By means of maximum-likelihood theory, we obtained p-values for the goodness of fit. In this case, a large p-value (p > .05) indicated a good fit of the graphical model. Further information on Gaussian graphical models can be found in Supplemental Online Material 1. For further reading on graphical modeling, also see Whittaker (2009).
Cluster analysis
A further aim of our study was to identify potential groups of participants displaying different patterns of anxiety. For that purpose, we performed a cluster analyses based on all major anxiety scales including AG, GAD, PD, SEP, SP, SAD as well as ILL. All variables were standardized beforehand. First, we performed a hierarchical cluster analysis which does not assume a priori knowledge of the number of clusters. We used agglomerative clustering based on Euclidean distances with Ward’s algorithm for the hierarchical clustering (Ward, 1963). In agglomerative clustering, the individuals are successively joined to clusters until in the end one cluster remains. In each step, the two clusters with the smallest inter-cluster distance are joined. The result of the procedure is a dendrogram (as in Figure 3) where the height at which two branches are joined signifies the distance of the clusters. There are a number of agglomerative cluster algorithms which differ in how the cluster distance is defined. For Ward’s algorithm, the cluster distance is, roughly speaking, the increase in the total within-cluster variance after merging. Second, we conducted a partitioning cluster algorithm which assumes a priori knowledge of the number of clusters. For the partitioning algorithm, we used the k-means method with the Hartigan–Wong algorithm (Hartigan & Wong, 1979). In general, this is a two-step approach: The hierarchical clustering aims at finding a suitable number of clusters, the partitioning clustering then finds an optimal separation of the clusters. Cluster analysis is an exploratory tool only, there is no significance (p-value) attached to any of the methods.
Results
The average score of the K-MPAI was 99.6 (SD = 40.6, range: 0–240). Even though the mean K-MPAI score did not differ from Spahn et al. (2016), it was significantly higher than mean scores reported by Kenny, Driscoll, and Ackermann (2012); n = 373, M = 83.7, SD = 40.7; two-tailed independent t-test: t(453) = 3.2, p < .05, d = 0.39. Severe levels of MPA (K-MPAI ⩾ 105) were reported in 36 participants. The severity measures for anxiety disorders of the DSM-5 showed that the majority of participants displayed no or only mild symptoms of a clinically relevant condition. A full descriptive analysis of all anxiety measures can be found in Supplemental Online Material 2.
Dependence analysis
The pairwise correlation analysis of anxiety variables, including MPA, showed all measures were positively, and mostly strongly, correlated (see Figure 1, left). The partial correlation results shed further light on the multivariate dependence structure of all variables where many partial correlations were close to zero, and only a few significant (see Figure 1, right). Results of Pearson’s and partial correlation analyses in a tabular format can be found in Supplemental Online Material 3.
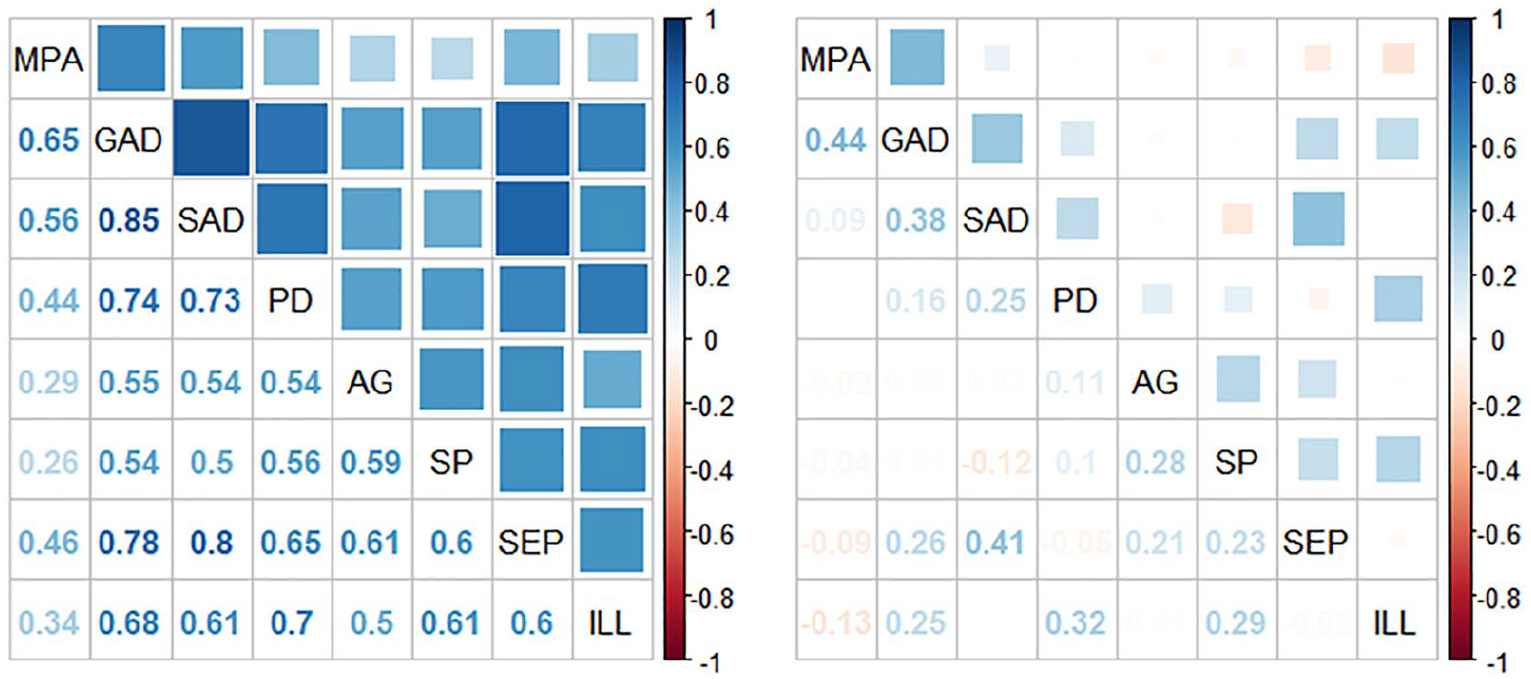
Correlation Matrices Showing Pearson’s Correlation Coefficients (Left) and Partial Correlation Coefficients (Right) of MPA and Other Anxiety Measures in 82 Music Students; correlation coefficients and p-values can be found in Supplemental Online Materials 3.
Based on the partial correlations, we fitted a Gaussian graphical model with p = .51, that means, a test for all partial correlations corresponding to absent edges being simultaneously zero returned a p-value of .51, hence, demonstrated no evidence against the model (see Figure 2; for more information on Gaussian graphical models, see Supplemental Online Material 1). Any absent edge between two nodes signifies a zero partial correlation, and thus conditional independence, of the corresponding two variables conditional on all remaining variables. GAD displayed most connections to other anxiety variables. MPA, however, was conditionally independent given GAD of all remaining anxiety variables which means the association between MPA and any remaining anxieties, including SAD, was fully mediated by GAD. Furthermore, our model also provided a good fit (p = .58) when considering severe cases of MPA only (n = 36 for K-MPAI ⩾ 105). Please note that the K-MPAI also includes items not directly related to performance, for instance, three items related to generational transmission of anxiety. We previously used a sub-scale of performance-related items only (K-MPAI-24, see Wiedemann et al., 2019) which we also employed in the current analysis to assess whether our graphical model remained the same. As the key message did not change, GAD was the strongest predictor for MPA among all major DSM-5 anxiety types, we refrain from reporting this analysis here.
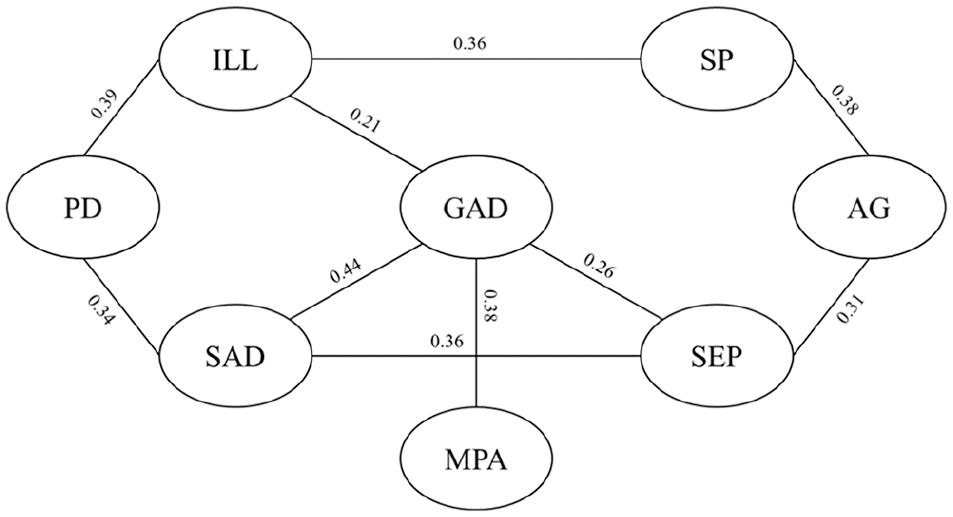
Fitted Gaussian Graphical Model (p = .51) for Anxiety Measures Including Music Performance Anxiety (MPA; Measured by the Kenny Music Performance Anxiety Inventory), Agoraphobia (AG), Generalized Anxiety Disorder (GAD), Panic Disorder (PD), Separation Anxiety Disorder (SEP), Specific Phobia (SP), Social Anxiety Disorder (SAD), and Illness Anxiety Disorder (ILL). The numbers along the edges indicate partial correlations fitted under the graphical model which means they differ slightly from the empirical partial correlation given in Table 3 in the Online Supplemental Material 3.
Cluster analysis
The results of the hierarchical cluster analysis, the dendrogram, can be seen in Figure 3 (with all 82 individuals listed on the x-axis). The performed cluster analysis was based on all seven DSM-5 anxiety measures, that is, excluding MPA. All individuals were successively merged together to one large cluster. The distances in the horizontal direction represent distances between two clusters that were merged. That means, large distances indicate rather well separated clusters. We found two clusters emerging, one consisting of 74 individuals (Cluster 1) and one of 8 individuals (Cluster 2).
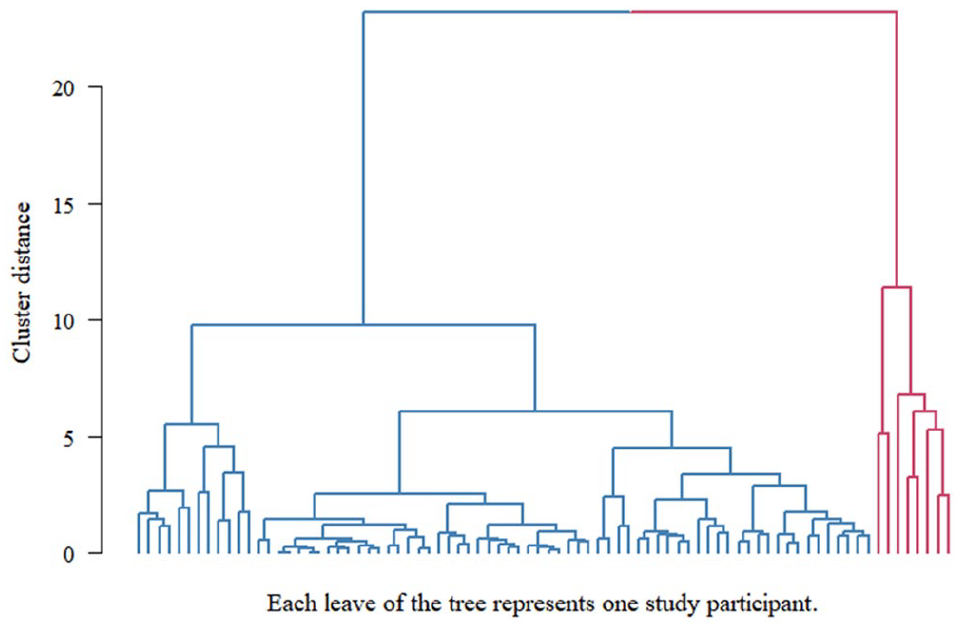
Dendrogram based on Participants’ Anxiety Profile which Included Agoraphobia, Generalized Anxiety Disorder, Panic Disorder, Separation Anxiety Disorder, Specific Phobia, Social Anxiety Disorder, and Illness Anxiety Disorder (Cluster 1 = Blue, Cluster 2 = Red).
When performing k-means for k = 2, we obtained almost the same two clusters as suggested by the dendrogram. The clusters obtained by k-means had the same sizes (n = 74 and n = 8) with the cluster membership of two individuals being swapped. Two rather different methods, Ward’s agglomerative clustering and k-means, returning very similar results is an indicator that a good discrimination between healthy and pathological anxiety profiles (excluding MPA) among our participants is possible. Moreover, performing cluster analyses based on all anxiety variables, including MPA, also returned similar results. For instance, performing k-means on all eight variables (including MPA) yielded a Cluster 2 with nine individuals, which was exactly the union of both second Clusters found by the two different methods on the seven variables (excluding MPA). In the pairwise scatterplots in Figure 4, the results of k-means on the seven variables is shown: Cluster 1 is blue, Cluster 2 red.
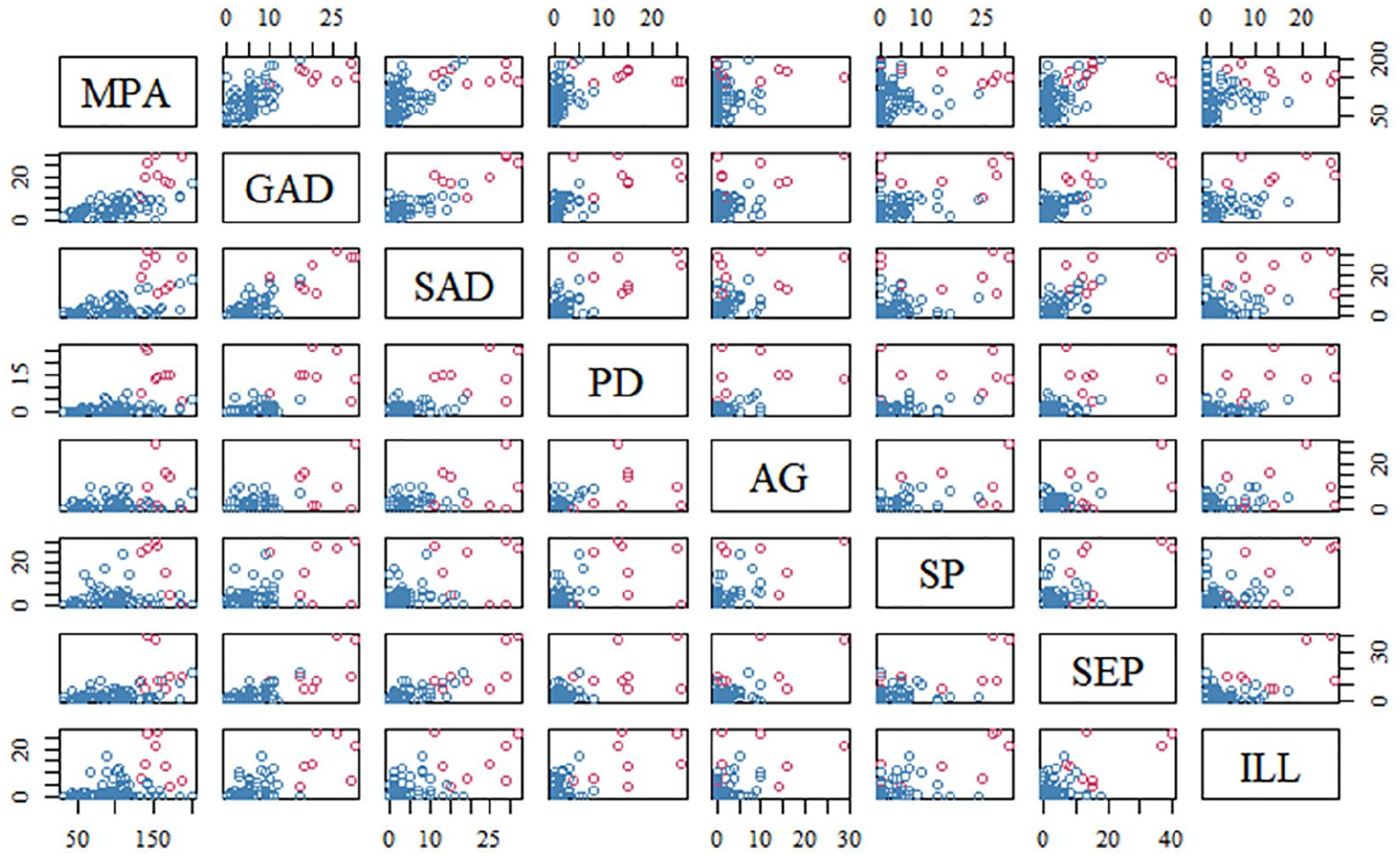
Distribution Characteristics of MPA and Other Anxiety Measures in 82 Music Students with Cluster Analyses Showing Two Groups (Cluster 1 = Blue, Cluster 2 = Red).
Individuals of Cluster 2 showed elevated anxiety levels in nearly all measures. For example, nearly all individuals (7 of 8) from Cluster 2 displayed clinically relevant GAD which means the manifestation of GAD exceeded a mild symptomatology (see Figure 5). These individuals consistently showed high levels of MPA (K-MPAI ⩾ 105). In contrast, individuals of Cluster 1 displayed no pathological anxiety symptoms across all DSM-5 anxiety measures; their MPA, however, included lower and higher levels. Applying the previously performed dependency analysis to Cluster 1 only, we also found no evidence of MPA being partially correlated, given GAD, to any other variable, including SAD (see Supplemental Online Material 4). The size of Cluster 2 was too small to draw any statistically valid conclusions.
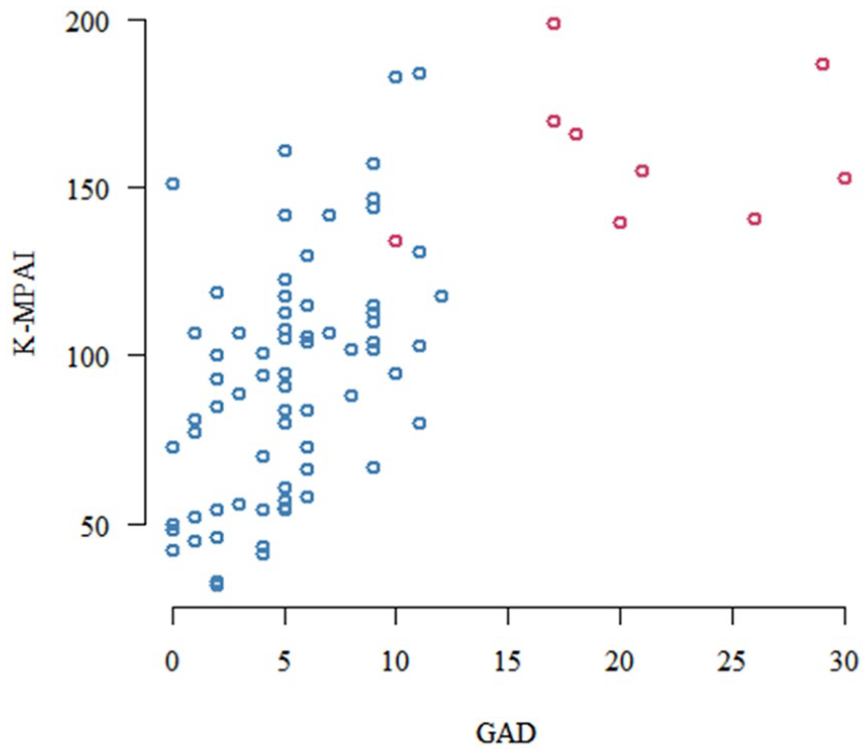
Self-Reported Music Performance Anxiety (MPA), Measured by the Kenny Music Performance Anxiety Inventory (K-MPAI), in Relation to Generalized Anxiety Symptoms/Disorder, Measured by the Generalized Anxiety Disorder (GAD; 0 = none, 10 = mild, 20 = moderate, 30 = severe, 40 = extreme) in 82 Music Students; Pearson’s r = .65, p < .001, with Cluster Analyses Showing Two Groups (Cluster 1 = Blue, Cluster 2 = Red).
Discussion
Summary of results
Our aim was to visualize the complex interplay of dependencies between MPA and major anxiety disorders, including SAD. We wanted to identify most important anxiety variables in relation to MPA through graphical modeling, and analyze anxiety profiles by means of cluster analysis. Accordingly, our main results can be summarized as follows:
We found no evidence that MPA is primarily connected to SAD.
GAD acted as a full mediator between MPA and SAD as well as between MPA and any other anxiety type.
The above-mentioned findings were valid regardless of the attention being restricted to severe MPA (K-MPAI ⩾ 105).
Based on all DSM-5 anxiety measures, we identified a sub-group of participants displaying a healthy anxiety profile and a sub-group of participants displaying a pathological anxiety profile, meaning that those individuals displayed clinically relevant levels in several of the DSM-5 dimensional anxiety scales.
(a) Individuals with a pathological anxiety profile consistently showed clinically relevant levels of MPA.
(b) Individuals with a healthy anxiety profile showed both lower and higher levels of MPA.
What can the graphical model tell us?
Our graphical model in Figure 2 shows that GAD is connected to the majority of anxiety variables considered in the model including MPA, SEP, SAD, and ILL. Hence, it can be regarded the most representative of the set of variables. The foremost advantage of graphical models, however, lies in the information we can deduct from any two nodes that are not connected by an edge. For example, MPA is, given GAD, conditionally independent of all other six anxiety disorders. This means that the association between MPA and any of the remaining six anxieties, including SAD, is fully mediated by GAD. In terms of information, GAD is fully sufficient for predicting MPA. Additional knowledge of SAD provides no further information. However, the converse is not true: The connection between MPA and GAD is not mediated by SAD since no edge can be found in between MPA and SAD in the graph.
One could argue that attention should be restricted to severe MPA levels (K-MPAI ⩾ 105) since lower levels of the K-MPAI may indicate an optimal arousal in performance situations. However, the above-mentioned findings were valid regardless of the attention being restricted to severe levels of MPA (K-MPAI ⩾ 105). This means that our findings support the idea of MPA being distinguished from SAD as suggested by Kenny (2016). In fact, our graphical model does not support the current DSM-5 guidelines in which an individual who suffers exclusively from performance anxiety would receive a diagnosis of SAD. The introduction of the new specifier performance only evoked more debate within the working group than any other proposed changes to SAD. Going into more detail, it becomes clear that the DSM-5 anxiety sub-workgroup also suggested that performance anxiety in general should only be considered as an exemplar of SAD if fear of negative evaluation by others is the presenting core issues, whereas the predominance of a fear of failure in a non-social context should always be considered as a manifestation of GAD (Heimberg et al., 2014). To which extend this is actually taken on by clinicians remains unknown. To conclude, our model suggests that GAD is the strongest predictor for MPA among all major DSM-5 anxiety types. MPA may therefore be considered as a manifestation of GAD rather than SAD.
MPA as a focal disorder or part of a more complex psychopathology?
Kenny (2011) previously suggested a tripartite typology of MPA differentiating between (a) severe MPA as a focal disorder in an otherwise healthy musician, (b) severe MPA as an expression of SAD, and (c) severe MPA as a more complex psychopathology. One approach toward a refined analysis is to identify sub-groups in respect to the overall anxiety profile based on the seven DSM-5 anxiety measures. Following this, we examined the potential differences in MPA. By means of the cluster analyses, we identified two groups: Individuals in Cluster 1 (n = 74) scored low on all seven anxiety measures whereas individuals in Cluster 2 (n = 8) displayed varied and complex pathological anxiety patterns. Considering individuals of Cluster 1 only, we still found no evidence for MPA being partially correlated, given GAD, to any other variable, including SAD. The size of Cluster 2, however, was too small to draw any statistically valid conclusions. Nevertheless, we observed a noticeably different distribution of MPA in both clusters. Individuals in Cluster 2 all exhibited high levels of MPA whereas individuals in Cluster 1 covered the whole range of the K-MPAI scale, including lower and higher levels of MPA. Even though individuals of Cluster 2 all displayed severe MPA, it becomes clear that most participants of our sample showed an isolated type of severe MPA (n = 26). Our data support the idea of differentiating between different MPA types, potentially including MPA as a focal disorder in an otherwise healthy musician, and MPA as a more complex psychopathology. To assess whether individuals with complex pathological anxiety profiles differ in expression of MPA and their relation to SAD remains a question for further research.
Limitations, clinical relevance, and further research
Using the German version of the K-MPAI, we found that the average score of the K-MPAI was higher than mean scores reported in English cohorts (e.g., see Kenny et al., 2012). This has also been the case in other German cohorts (e.g., see Spahn et al., 2016). As the cut-off for severe levels of MPA is based on the English version of the inventory, it is possible that more participants are classified with severe levels of MPA than this is actually the case. It is important that further research addresses these issues and validates a German cut-off for severe MPA. Furthermore, the size of individuals displaying a more complex psychopathological anxiety profile (Cluster 2) reflects a further shortcoming of our research. This group of individuals, however, is of particular interest as our graphical model may not fit for those individuals. Based on Kenny’s (2011) proposed tripartite typology of MPA, the role of SAD may as well be different in those individuals. The majority of participants in Cluster 2 displayed clinically relevant symptoms which would meet DSM-5 criteria for a diagnosis of SAD. Recruiting more participants with a more complex psychopathological anxiety profile is important to fully understand different typologies of MPA which may influence the conceptualization of treatment approaches. However, leaving the question of representativeness aside, the majority of our study sample with elevated MPA (K-MPAI ⩾ 105) did not show clinically relevant levels of other anxiety disorders. The question arises whether it is necessary to differentiate between three types of MPA, that is, differentiating between MPA as a focal disorder and MPA as part of a more complex psychopathological profile may in fact be sufficient.
Finally, we previously discussed potentially confounding factors of our study regarding sample recruitment (Wiedemann et al., 2019). Through our recruitment method of choice (online link distribution), we cannot rule out any participation bias. Individuals who are generally more aware of issues surrounding MPA, or individuals who suffer from debilitating MPA themselves, may have been more likely to take part in our study. We previously highlighted, however, that the sample shows similar distributions to other cohorts in a range of measures, for example, adult attachment behavior.
Conclusion
The aim of our study was to visualize the generally complex interplay of dependencies between MPA and major anxiety disorders including among others SAD. We found no evidence of MPA being primarily connected to SAD. Instead, GAD acted as full mediator between MPA and SAD as well as between MPA and any other anxiety type. These findings were valid regardless of the attention being restricted to severe levels of MPA. This means that our findings support the idea of MPA being distinguished from SAD as suggested by Kenny’s (2016) revised definition of MPA. Based on all seven DSM-5 anxiety measures, we identified a sub-group of participants displaying a healthy anxiety profile and a sub-group of participants displaying a pathological anxiety profile. We observed a noticeably different distribution of MPA in both groups: Whereas individuals with a healthy anxiety profile showed both lower and higher levels of MPA, individuals with a more complex pathological anxiety profile consistently showed severe levels of MPA. The question whether individuals with complex pathological anxiety profiles differ in expression of MPA and their relation to SAD remains for further research. Investigating individuals with a more complex psychopathological anxiety profile is important to fully understand different typologies of MPA which may lead to more efficient treatment approaches. However, despite some individuals displaying severe levels of MPA, the majority of participants displayed overall moderate levels of performance anxiety suggesting a healthy experience of nervousness on stage.
Supplemental Material
sj-pdf-1-pom-10.1177_0305735620988600 – Supplemental material for How does music performance anxiety relate to other anxiety disorders?
Supplemental material, sj-pdf-1-pom-10.1177_0305735620988600 for How does music performance anxiety relate to other anxiety disorders? by Anna Wiedemann, Daniel Vogel, Catharina Voss and Jana Hoyer in Psychology of Music
Footnotes
Acknowledgements
The authors would like to thank all students and administrative staff of participating music universities. The authors would also like to express their appreciation to Professor Katja Beesdo-Baum and Dr Manfred Nusseck for general support, to Birgit Maicher for programming the basic version of the questionnaires and to Professor Hans-Christian Jabusch for helping to recruit participants as well as for discussions at later stages of the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.