
Abstract
Objective
To evaluate the inclination of incisors after retraction with double wire using double-slot brackets (DSC) versus single wire using single-slot brackets.
Materials and Methods
Twenty-four patients aged 18 ± 5 years with maxillary anterior proclination requiring extraction of upper first premolars were randomly divided into two groups equally. Group I utilized double wires for retraction in DSCs, whereas Group II received a single wire retraction protocol in single-slot brackets. Pre- and post-retraction cone beam computed tomography scans were compared to assess the changes in inclination, vertical position, anchorage loss, and root resorption between the groups. An independent t-test was done for inter-group comparison, and a paired t-test was done to determine significant changes within the groups.
Results
Group I revealed a significant reduction in labiolingual inclination by 5.59° ± 6.56°, whereas Group II showed a reduction by 8.02 ± 6.53. The central incisors in Group I showed a vertical change of −1.13 ± 1.34 mm, whereas in Group II, significant vertical changes were limited to the lateral incisors at −1.79 ± 1.35 mm. Inter-group comparisons revealed no significant differences (P >.05) with respect to torque, anchorage loss, and root resorption.
Conclusion
The changes in the double-slot group post-retraction were comparable to those in the single-slot group, with no significant statistical difference.
Introduction
Precise and controlled space closure during anterior segment retraction is critical and should be achieved within the normal limits without any ramifications. 1 Achieving appropriate torque of the maxillary incisors is essential for establishing an adequate interincisal angle, tooth contact, and facilitating sagittal adjustments to achieve optimal occlusion. 2 While first- and second-order information are relatively easy to express, achieving the desired torque is more complex, with at least 13 influencing factors. 3 The challenge associated with the advent of straight-wire appliances involves the “play” or deviation between the archwire and the bracket slot. 4 This phenomenon arises from the discrepancy between the theoretical concept of a perfectly fitting archwire within the bracket slot and the realities of manufacturing tolerances. 5 Research indicates that archwire beveling at the edges, commonly referred to as the edge bevel radius (EBR), accounts for the majority of this play, up to 63%. 3 It is often overlooked in clinical practice due to its complexity and lack of readily available manufacturer data. While greater beveling may reduce patient discomfort, it simultaneously compromises torque control within the bracket slot. 3
These inherent archwire-bracket discrepancies can inevitably cause torque loss despite adhering to the standard retraction mechanics, prompting methods like increased built-in torque, arch torsion, and torquing auxiliaries.6, 7 To improve torque control, the bimetric system, utilizing dual-slot brackets for a precision fit, was introduced, followed by other bi-dimensional techniques.8–10 However, limitations like compromised control with less rigid wires in a 0.018″ slot, increased play in posterior segments, and unconventional twisting of archwires hindered their widespread adoption. The double-slot bracket (DSC), an innovation introduced in 2018 with two distinct slots in the same bracket, offers versatile treatment options, such as simultaneous use of both slots, selective use of a single slot, or switching between slots during treatment. 11 Despite its potential, research comparing single versus double wire retraction in DSC brackets is scarce. The null hypothesis states that the use of double wires in DSCs does not provide superior torque control, improved incisor inclination, reduced anchorage loss, or decreased root resorption compared to single-wire methods.
Materials and Methods
Study Design and Sample Size Determination
This was a 1:1 allocation ratio, parallel-group, randomized, clinical trial following the Consolidated Standards of Reporting Trials (CONSORT) 2010 Statement reporting guidelines. Before the start of the study, the proposal was approved by the respective ethical committee. The study was also successfully registered and approved by the Clinical Trials Registry of India (CTRI registration number masked).
A sample size of 20 was decided by the statistical software GPower (version 3.1.9.7). The power of the study was 0.80 with a 5% of Type I error. The sample size was derived by substituting the result from Attia et al. with an effect size of 1.56. 12
Study Settings
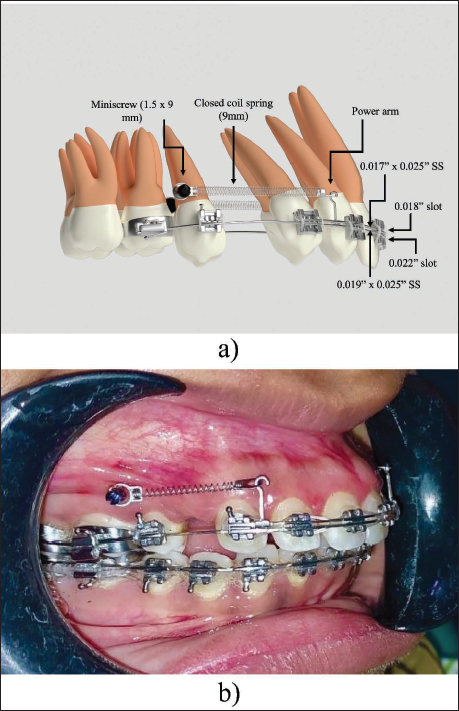
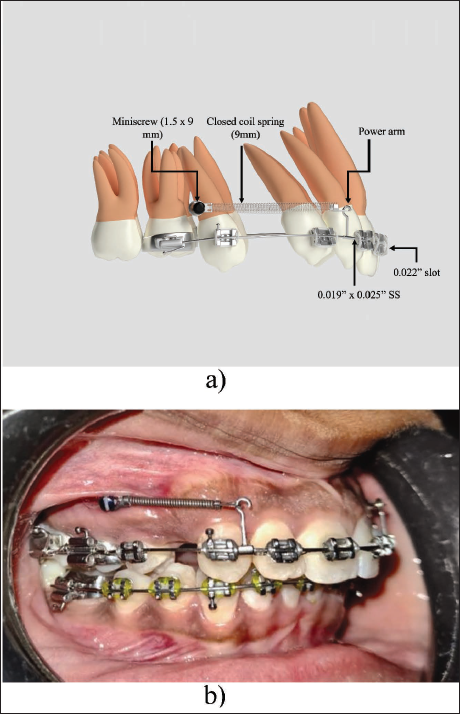
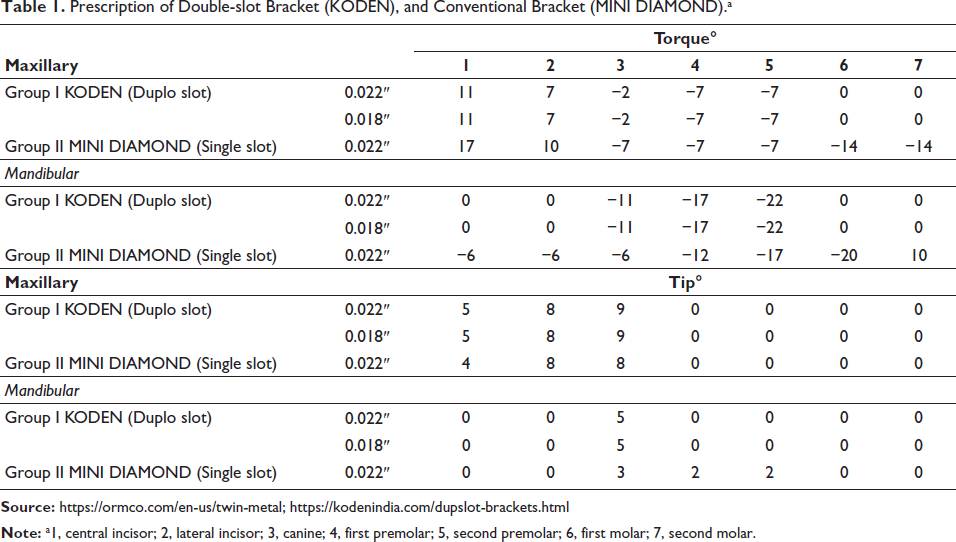
A total of 24 female patients aged 18 ± 5 years, requiring first premolar extractions due to maxillary anterior teeth proclination with minimal crowding (<3 mm using Little’s Irregularity Index), were included in the study. Informed consent was obtained from all subjects and their parents for study participation, as well as for radiation exposure in the form of cone-beam computed tomography (CBCT), performed solely for methodological assessment purposes. Subjects were randomly assigned to Group I and Group II. All participants underwent a comprehensive diagnostic evaluation, including the acquisition of study models, facial photographs, and radiographic records (orthopantomogram and lateral cephalogram). Group I received orthodontic treatment using DSCs with a 0.022″ occlusal slot and a 0.018″ gingival slot (KODEN SORTECH DUPLOSLOT), while Group II received treatment with single-slot 0.022″ × 0.028″ brackets in McLaughlin–Bennett–Trevisi (MBT)-prescribed appliances (MINI DIAMOND ORMCO LTD) (Table 1). Both groups initiated treatment with flexible NiTi wires in conjunction with a transpalatal arch and a lingual arch, progressing to 0.019″ × 0.025″ stainless steel (SS) wires in the 0.022-slot. Leveling and alignment were completed within 5-6 months. At this stage, CBCT scans were acquired to assess the labiolingual inclination of the maxillary incisors, the sagittal position of the maxillary molars, and the initial root length of the upper incisors. Following first premolar extractions, Group I utilized a double wire retraction technique with 0.019″ × 0.025″ SS archwire throughout the entire arch, while the anterior segment contained a 0.017″ × 0.025″ SS wire in a 0.018″ slot (Figure 1). In Group II, retraction was progressed conventionally using a single 0.019″ × 0.025″ SS wire in a 0.022″ slot (Figure 2). En-masse retraction was performed in both groups using mini-implants (1.5 × 9 mm) placed between the roots of the maxillary second premolars and first molars. NiTi coil springs (KODEN) 9 mm were installed, extending from crimpable hooks (6-8 mm) to mini-implants for retraction of anterior teeth. A 150-200 g force was applied on each side during retraction. Coil springs were activated at each appointment to maintain consistent retraction forces, and space closure was monitored at an interval of 6-8 weeks. After achieving complete en-masse retraction, a second CBCT scan was acquired to assess labiolingual inclination and vertical changes in the maxillary incisors, anchorage loss in the upper arch, and root resorption in the maxillary incisors. Finishing and detailing were performed, followed by occlusal settling prior to bracket removal.
Prescription of Double-slot Bracket (KODEN), and Conventional Bracket (MINI DIAMOND).a
Randomization, Blinding, and Intra-examiner Reliability
Subjects were assigned to two groups via sequentially numbered, opaque, sealed envelopes (SNOSE). The patients were blinded; however, the study design precluded blinding of the operator. To minimize bias, the data were de-identified and forwarded to an independent, blinded statistician for analysis. The same researcher performed all measurements twice to reduce method error. A 1-month interval preceded a second measurement of the radiographs, with discrepancies beyond 0.5 mm (linear) or 0.58° (angular) led to remeasurement of the affected data.
Radiological Assessment
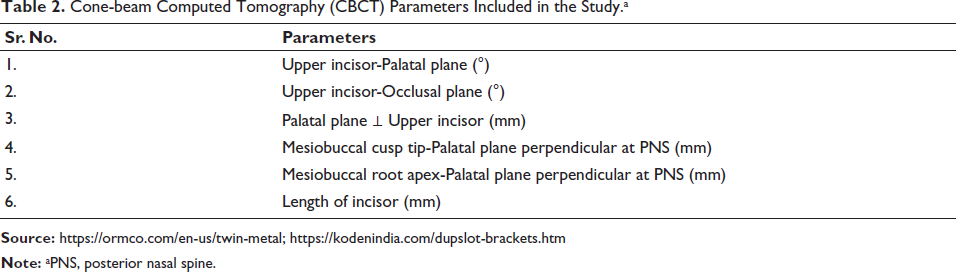
The Digital Imaging and Communications in Medicine (DICOM) images from CBCT scans (5 × 8 cm field of view (FOV)) were analyzed using NewTom Technology (NNT) Viewer version 16.4, with measurements performed as detailed in Table 2. SEDENTEXCT guidelines were adhered to, as the effective radiation dose of 50 µSv remained well below 200 µSv and the FOV was limited to the dentition itself.
Cone-beam Computed Tomography (CBCT) Parameters Included in the Study.a
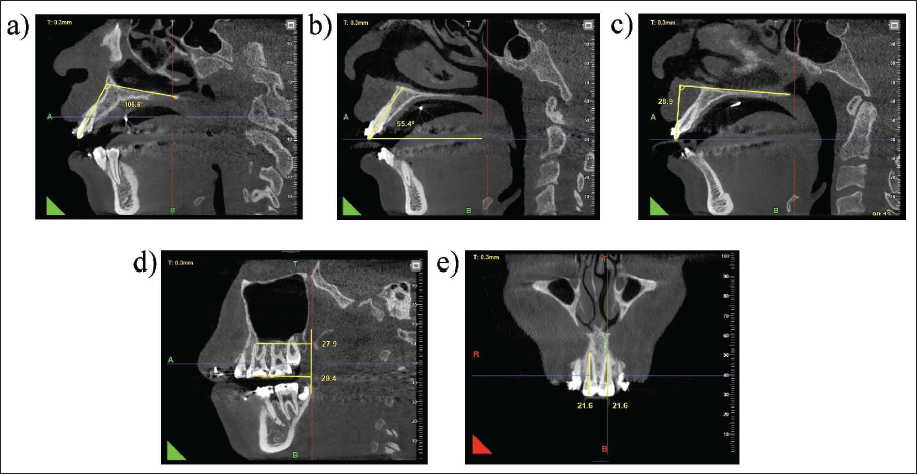
Following head orientation, multiplanar reconstruction was selected. In the axial plane, individual teeth were aligned along their long axis, as verified in the sagittal and coronal planes. Reference planes were noted on the pre-retraction CBCT, which became the reference lines for evaluation of torque, anchorage loss and root resorption in the post-intervention CBCT. In the corrected midsagittal view, the palatal plane extending from anterior nasal spine (ANS) to posterior nasal spine (PNS) and the occlusal plane passing through the premolars and molars were used as reference planes.
Labiolingual inclination was measured primarily as the inner angle between the long axis of the incisors and the palatal plane, viewed from the sagittal aspect, as seen in Figure 3a. A second measurement for torque was recorded as the inner angle between the long axis of each incisor and the occlusal plane (Figure 3b). The difference between pre- and post-retraction values for both these parameters determined the change in labiolingual inclination. The vertical position of maxillary incisors was recorded by measuring the perpendicular distance from the palatal plane to the incisal edge of each incisor (Figure 3c). The change in length determined the corresponding vertical change of each incisor.
Anchorage loss was measured as the linear distance between the mesiobuccal cusp tip and a perpendicular to the palatal plane at point PNS, and the distance between the mesiobuccal root apex and the same plane, as seen in Figure 3d.
In the coronal aspect, tooth length was measured as the linear distance extending from the incisal edge to the root apex of each incisor (Figure 3e). Apical root resorption was quantified as the difference between pre- and post-retraction values.
Statistical Analysis
Statistical analysis of the recorded data was performed using IBM Statistical Package for the Social Sciences (SPSS) version 25. A paired t-test was used for intragroup comparisons of the labiolingual inclinations, vertical changes, anchorage loss, and root resorption between pre- and post-retraction within both groups. An independent t-test was used for comparison between the study groups. Data were described in terms of mean ± standard deviation. The significance level was set at P < .05.
Results
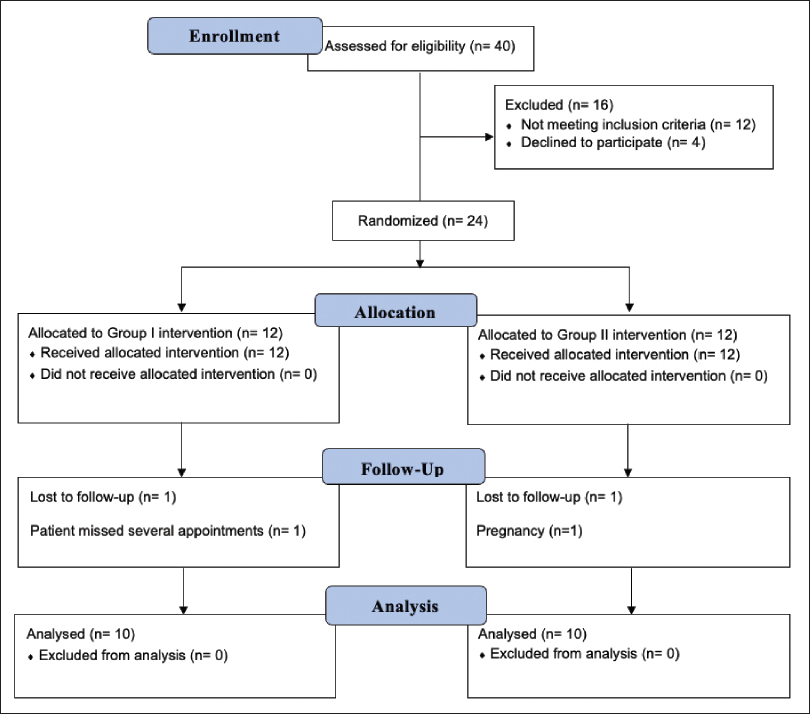
A CONSORT diagram, as shown in Figure 4, illustrates the flow of participants throughout the study, including recruitment, allocation, and any attrition that occurred.
Inclination
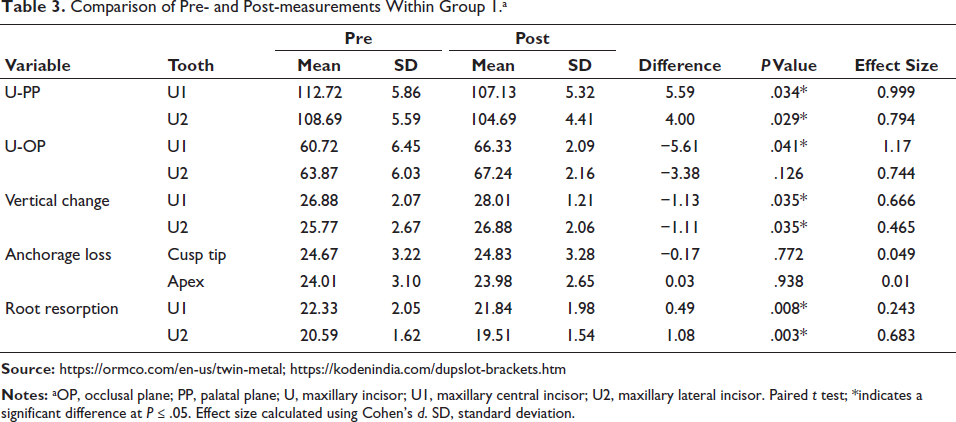
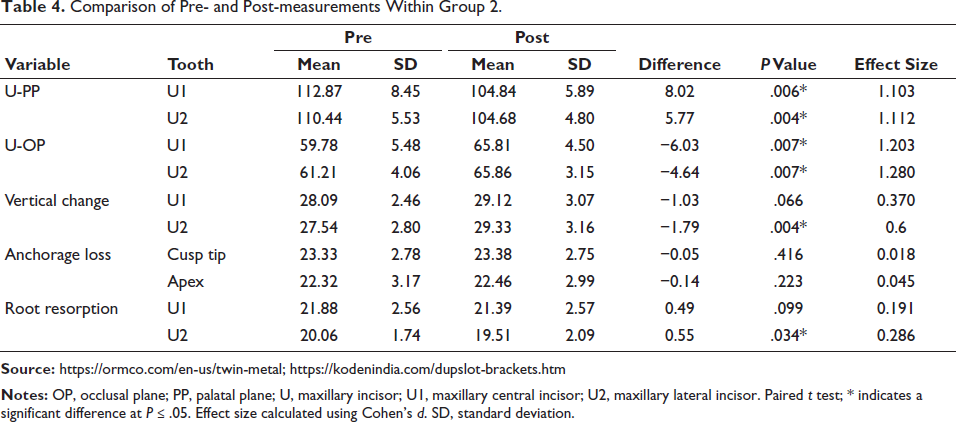
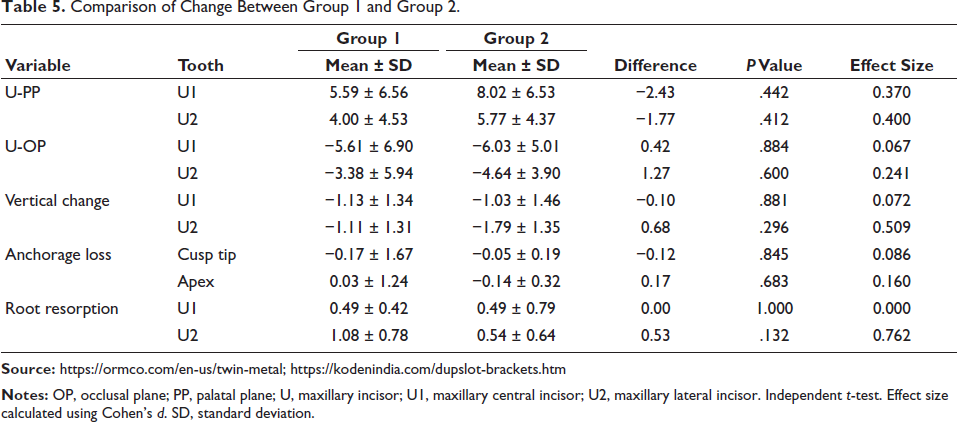
Both groups revealed a statistically significant decrease in the labiolingual inclination of the maxillary central and lateral incisors following retraction. In Group 1, a significant reduction of 5.59° ± 6.56° was observed in U1-PP (P = .034) and 4.00° ± 4.53° in U2-PP (P = .029), while U1-OP significantly increased (P = .041) (Table 3). In Group 2, both U1-PP (8.02° ± 6.53°) and U1-OP angles showed significant changes, as did U2-PP and U2-OP angles (Table 4). Inter-group comparisons showed variations in magnitude, with Group 1 exhibiting smaller alterations than Group 2. However, these differences were not statistically significant (Table 5).
Significant vertical changes occurred in Group 1 for both central and lateral incisors (Table 3). In Group 2, only lateral incisor extrusion was significant (Table 4). Inter-group comparison did not reveal any statistically significant differences. The mean change in vertical position for the maxillary central incisors was −1.13 ± 1.34 mm in Group 1 and −1.03 ± 1.46 mm in Group 2. Correspondingly, the mean change in vertical position for the lateral incisors was −1.11 ± 1.31 mm in Group 1 and −1.79 ± 1.35 mm in Group 2 (Table 5).
Comparison of Pre- and Post-measurements Within Group 1.a
Comparison of Pre- and Post-measurements Within Group 2.
Comparison of Change Between Group 1 and Group 2.
Anchorage Loss
Anchorage loss at the maxillary first molar (cusp tip and root apex) was not significant within or between groups. Mean cusp tip changes were −0.17 ± 1.67 mm (Group 1) and −0.05 ± 0.19 mm (Group 2). Mean root apex changes were 0.03 ± 1.24 mm (Group 1) and −0.14 ± 0.32 mm (Group 2) (Tables 3–5).
Root Resorption
Root resorption was assessed by measuring the change in length of the central and lateral incisors between pre-retraction and post-retraction time points. Significant root resorption was observed in Group 1 for central (0.49 ± 0.42 mm) and lateral (1.08 ± 0.78 mm) incisors. Group 2 had significant resorption in lateral incisors only (0.54 ± 0.64 mm). Inter-group resorption changes were not significant for either incisor type (Tables 3–5).
Discussion
Increased facial convexity and lip incompetence are frequently associated with anterior teeth proclination, necessitating the extraction of the first premolars. 13 In such cases, meticulous torque control becomes paramount not only for achieving functional and stable occlusion but also for optimizing aesthetic outcomes. 14 Torque loss may be associated with bite deepening, increased gingival display, limiting the full range of retraction, and prominent roots. 15 The prescribed torque within a bracket is not fully expressed due to inherent mechanical constraints. These include a restricted area of torque application, dependent on the twist effect of a relatively small wire compared to the tooth’s volume, and clearance between the wire and bracket interface, influenced by manufacturing tolerances and wire edge radiusing.3, 16 A standard 0.022″ slot bracket used with a 0.019″ × 0.025″ SS wire for retraction exhibits a 9.6° play. In contrast, a 0.017″ × 0.025″ wire in a smaller 0.018″ slot shows significantly less play of 4.1°. 15 Consequently, supplementary mechanisms are often required to minimize this loss during retraction. Given the recognized limitations of traditional pre-adjusted edgewise bracket systems, bimetric and bidimensional techniques were designed. Building upon these advancements, the DSC system emerged as a versatile solution, addressing multiple clinical challenges.8–11 This study aimed to elucidate the potential advantages of double wire in enhancing torque control during anterior retraction.
The sequelae of anterior torque loss were assessed by two parameters, consisting of labiolingual inclination changes and vertical position changes pre- and post-retraction. 17 Notably, statistically significant changes in labiolingual inclination were observed within both groups (5.61° for U1-OP in Group I and 6.03° in Group II), confirming the occurrence of torque loss despite utilizing a double wire in Group I. This aligns with previous studies employing similar retraction mechanics with reported torque loss of 9°-13°. This suggests that even with robust biomechanics, clinical realities can challenge ideal torque maintenance.1, 12, 18, 19 However, the limited existing literature comparing single versus double wire retraction techniques presents a gap in understanding clinical efficacy. Extrusion of incisors is an inherent effect associated with torque loss. It can cause an unesthetic increase in the display of anterior teeth, deepen the bite, and compromise stability. The present study recorded extrusions of 1.13 mm in Group I and 1.03 mm in Group II, values that are consistent with the reported literature range of 1.53-2.15 mm. 20 While a typhodont study suggested the superiority of double wire retraction in maintaining torque control and limiting incisor extrusion in lingual orthodontics, our clinical findings, utilizing vestibular mechanics, revealed no statistically significant differences between single and double wire retraction groups. 17
To ensure uniform retraction mechanics, closed coil springs with temporary anchorage devices (TADs) were installed as an anchorage device. 21 To accurately quantify anchorage loss in the upper first molars, CBCT parameters measured displacement from two distinct points: the cusp tip and the root apex. 22 Notably, our findings indicated no statistically significant anchorage loss in either group. Group I presented with changes of −0.17 (cusp tip) and 0.03 mm (root apex), and Group II with −0.19 (cusp tip) and −0.32 mm (root apex). Similarly, intergroup comparisons showed no significant differences, with changes of −0.12 (cusp tip) and 0.17 mm (root apex). While the existing body of literature on double slot mechanics remains limited, our findings are consistent with previous studies utilizing single-slot brackets, with a similar report on minimal anchorage loss of 1.92 mm for the cusp tip and 0.64 mm for the root apex during retraction.12, 23
To accurately assess orthodontically induced root resorption (OIRR), we measured total tooth length (incisal edge to apex) to avoid cementoenamel junction (CEJ) delineation errors caused by CBCT artifacts and labial–palatal differences.24, 25 Our study revealed a statistically insignificant difference in the extent of incisor root resorption between the single and double wire retraction groups. However, intragroup analysis demonstrated significant root resorption post-retraction, with lateral incisors exhibiting a greater degree of resorption of 1.08 and 0.55 mm in Group I and Group II, respectively, as compared to central incisors with 0.49 mm in both groups. This observation aligns with established literature, which consistently identifies the maxillary lateral incisor as being particularly susceptible to root resorption during orthodontic treatment. 17 Our results corroborate prior research showing that OIRR is common after orthodontic treatment, especially with en-masse maxillary incisor retraction.24, 26
Despite the lower torque prescription of DSCs, Group I shows comparable outcomes to Group II. This finding may be attributable to the reduced play in the gingival slot. However, the small sample size restricts definitive conclusions on single versus double wire retraction efficacy in different bracket systems. Future studies could explore integrating advanced bracket designs and prescriptions with better torque control with a higher sample size to enhance treatment outcomes and minimize undesirable side effects.
Conclusion
En-masse retraction of maxillary incisors leads to changes in labiolingual inclination, vertical position, and root resorption, despite using standard retraction protocols.
Both Group 1 (double slot) and Group 2 (single slot) patients exhibited significant torque loss post retraction. However, comparative analysis amongst the two groups revealed no statistically significant differences.
Similarly, incisor extrusion was observed as a concomitant effect of torque loss in both groups. No significant changes were observed between the double wire and single wire retraction groups.
Statistically significant root resorption was evident within both groups, with lateral incisors demonstrating a greater degree of resorption compared to central incisors. Findings were insignificant amongst the two groups.
Footnotes
Authors Contribution
Sharvari Mairal: Methodology, formal analysis, writing—original draft.
Vipul Kumar Sharma: Conceptualization, writing—review and editing.
T.P. Chaturvedi: Supervision, writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
Prior to the commencement of this study, ethical approval was duly obtained from the Institutional Ethics Committee (Dean/2023/EC/6687), and informed consent was secured from all participating subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.