
Abstract
Objectives
To assess and contrast the decline of force in long, short, and continuous configurations of elastomeric chains after exposure to different commercially available beverages like tea, cola, orange juice, coffee solution, and artificial saliva.
Materials and Methods
Three hundred pieces of Generation II elastomeric chains (long, short, and continuous) were divided into control and test groups. The control group chains were dipped in artificial saliva, while the test group chains were exposed to tea, cola, orange juice, and coffee solutions twice daily for 30 s over a 28-day period. All the chains were pre-extended to two times their initial length and initially tensioned to 250 g. Force measurements were recorded using a digital dynamometer at the end of 28 days. Data were analyzed using descriptive statistics and parametric tests, including pairwise comparisons.
Results
Continuous chains exhibited the highest mean force values, particularly in orange juice (127.47 ± 1.16), followed by artificial saliva (121.26 ± 1.13) and cola (109.21 ± 1.37). Short chains showed the highest mean in artificial saliva (122.05 ± 1.25), while the lowest was in orange juice (79.99 ± 1.42). Long chains also retained maximum force in artificial saliva (123.57 ± 1.51) and the least in orange juice (75.70 ± 1.98).
Conclusions
Continuous elastomeric chains maintained higher residual forces compared with short and long chains. Clinicians should consider chain configuration and patients’ dietary habits to minimize force decay and optimize treatment efficiency.
Introduction
Orthodontic procedures often rely on elastic ligatures and chains for various clinical objectives, such as correcting midline deviations, addressing malocclusions, closing spaces from extractions, and attaching archwires to brackets. These elastomeric chains are favored for their flexibility, durability, cost-effectiveness, and ease of use, making them vital in orthodontic care. Yet, although they can withstand substantial forces, research shows that their effectiveness diminishes over time due to force degradation. 1
The goal of orthodontic therapy primarily involves applying gentle and sustained forces that move teeth effectively with minimal side effects. Elastomeric chains are commonly used to provide this force, but they often lose their effectiveness after 3-4 weeks, requiring replacement. This force degradation is influenced by both internal factors, such as material composition, and external factors such as their configuration, temperature, pH, and moisture absorption. 2 Elastomeric chains are limited by their inability to maintain the applied force for extended periods, with more than half of the force typically relaxing within the first 24 h. 3
As a result, an initial greater force is applied to compensate for this relaxation. If the force is too weak, tooth movement may be less effective, leading to longer treatment durations. Moreover, with the increasing demand for aesthetic outcomes, minimizing discoloration has become a key concern for both clinicians and patients. 4 Various configurations of elastomeric chains may have different degrees of force degradation after consumption of various commonly available beverages, prompting the need for clinicians to use an elastomeric chain of a more suitable configuration for the patients during treatment. This study aims to explore the impact on degradation of force in three different configurations of elastomeric chains following the consumption of routinely consumed beverages.
Materials and Methods
The study received clearance from the Institutional Ethics Committee, and the certification was obtained.
Calculation of sample size: The number of samples was determined with the help of G*Power 3.1.9.7 software.
The given input parameters: Effect size: 0.25 (medium, according to Cohen) α probability error: 0.05 Power (1-β error probability): 0.95 Number of groups: 3
Output parameters: Critical f: 3.03 Sample size: 252
The least necessary sample size is 252. However, it is planned to include 300 samples in the study.
Materials Used in the Study
A total of 300 pieces of orthodontic elastomeric chain (Ormco Generation II power chain), which are used in this study (continuous, short, and long), are grouped into three sets: Set 1 comprises 100 pieces of continuous elastomeric chains, each containing seven loops. Set 2 included 100 pieces of short elastomeric chains, each consisting of six loops. Set 3 consisted of 100 specimens of the long configuration of elastomeric chains, each with five loops. 5 Clinically, elastomeric chains are primarily used for distalizing canines and closing extraction spaces. They are usually positioned between the hook of the first molar’s buccal tube and the bracket of the canine. Hence, we opted to go with the number of loops of elastomeric chains based on variations among individuals. Most frequently, four- and five-loop configurations are used for the distalization of canine teeth. 6 The current study included five, six, and seven loops, which are taken for long, short, and continuous chains, respectively, to offer meaningful clinical guidance.
Beverages Used in the Study
Tea solution: Tea solution will be prepared with Red Label Instant Spiced Tea mix (tea premix), which contains sugar, milk solids, maltodextrin, instant tea powder, spice extracts (0.85%), beet juice powder, natural ginger flavor, sweetener (E960), and stabilizers. Concentration of tea solution: 13 g of tea premix in 100 mL of water.
Cola: Aerated water, caramel color (E150d), sugar, phosphoric acid, caffeine, and natural flavor additives.
Orange juice: Commercially available Real Fruit Power active 100% orange juice will be used, which contains orange concentrate 20.40%, orange pulp 0.5%, vitamin C, water, and flavoring substances.
Coffee solution: Coffee solution will be prepared with Atlantis Instacup Coffee Premix, which contains dairy whitener (sugar and milk solids), instant coffee powder 9%, and maltodextrin. Concentration of coffee solution: 14 g of coffee premix in 120 mL of water.
Artificial saliva.
All the sets of orthodontic elastomeric chains are organized into two groups: The control group: Artificial saliva The test group: Tea solution, cola solution, orange juice, and coffee solution, with each solution containing 20 elastomeric chains of long, short, and continuous types.
In Control Group
Artificial saliva includes 20 continuous elastomeric chains, 20 short elastomeric chains, and 20 long elastomeric chains. Thus, 60 elastomeric chains in the control group are included. In the test group, 20 continuous elastomeric chains, 20 short elastomeric chains, and 20 long elastomeric chains are included for per test solution. Thus, the test group includes 60 elastomeric chains for tea solution, 60 elastomeric chains for cola, 60 elastomeric chains for orange juice, and 60 elastomeric chains for coffee solution. A total of 240 elastomeric chains in the test group is included.
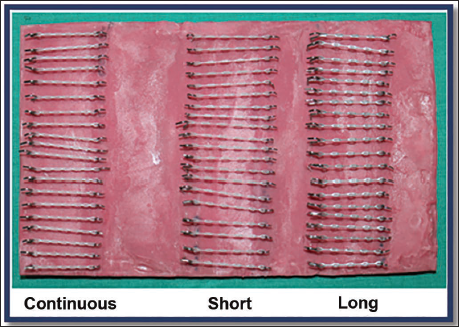
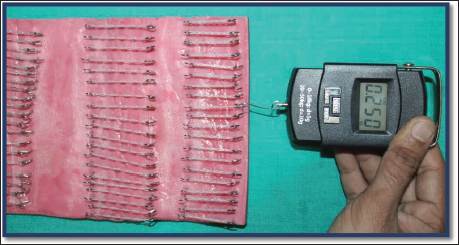
Five sheets of acrylic measuring 25 × 15 × 1 cm are constructed. Each sheet contains 20 vertical columns and 3 horizontal rows consisting of 120 jig pins made of stainless steel (Figure 1). The stainless-steel jig pins of 1.5 cm length (Figure 2) are embedded in the acrylic sheets up to a length of 0.5 mm and are used to keep the orthodontic elastomeric chains at a fixed stretched length. Each set of elastomeric chains is divided into pieces with seven loops from the continuous type, six loops from the short type, and five loops from the long type, and then grouped into five categories. Now the pre-stretching of all the elastomeric chains is done to twice their resting length to minimize the initial loss of force. One end of each elastomeric chain is now engaged with the stainless-steel jig pins and is stretched from the other end up to the force of 250 g, measured with a digital dynamometer, and fixed on the opposite jig pin (Figure 3).
Acrylic Sheet Containing Vertical Columns and Three Horizontal Rows of 120 Jig Pins.
Stainless-steel 20 Jig Pins.
Elastomeric Chain is Stretched up to the Force of 250 g, Measured with Digital Dynamometer.
Now all five acrylic sheets (one sheet of the control group and four sheets of the test solutions) are individually immersed in 37°C artificial saliva to mimic oral conditions and placed in an incubator to maintain a consistent room temperature. The elastomeric chains of the test groups are then submerged in their respective test solutions: tea solution, cola solution, orange juice, and coffee solution for 30 s twice daily throughout the 28-day testing period. 30 s exposure of the test group with the test solution is measured with a digital clock. After immersion in the test solutions, the elastomeric chains are individually dipped for 10 s into distilled water to mimic the mouth rinses from the oral cavity. The test group is then kept back in 37°C artificial saliva and again housed in an incubator. The measurement of remaining force values was taken after 28 days using a digital dynamometer.
The data that were collected were input in Microsoft Excel 2016 and analyzed with IBM Statistical Package for the Social Sciences (SPSS) Statistics for Windows, version 25 (IBM Corp., Armonk, NY, USA), for descriptive statistics. Descriptive statistics, like standard deviation and mean values, were computed to analyze the force reduction of orthodontic elastomeric chains upon submersion in various kinds of test solutions at different time intervals. A normality test was conducted to assess if the force decay data followed a normal distribution. The Shapiro–Wilk test was used because it is appropriate for small- to medium-sample sizes. The Shapiro–Wilk test results revealed P > .05, indicating that the data were normally distributed; therefore, parametric tests were used for analysis.
Results
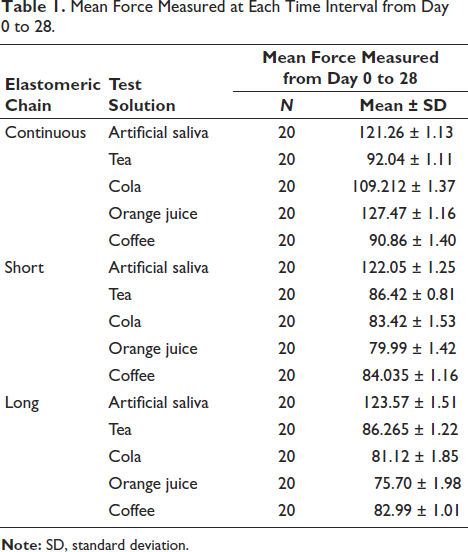
The data were analyzed using both descriptive and inferential statistical methods. Descriptive statistics, including the mean and standard deviation, were calculated for each group of elastomeric chains (continuous, short, and long) as shown in Table 1 across the various test solutions to summarize central tendencies and variability in force values.
Mean Force Measured at Each Time Interval from Day 0 to 28.
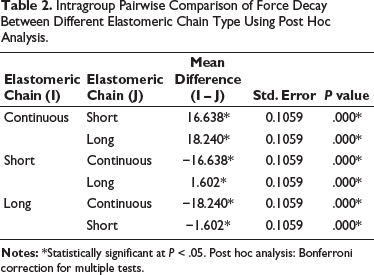
To determine statistically significant differences among the three types of elastomeric chains, a series of pairwise comparisons was conducted, given in Table 2. Independent sample t-tests were applied to compare the average force values between each pair of chain types (continuous vs. short, continuous vs. long, and short vs. long). A statistical significance threshold of P < .05 was applied across all comparisons to assess the statistical relevance of the observed differences. Each experimental group comprised 100 specimens to ensure adequate statistical power. All analyses were performed using standard statistical software.
Intragroup Pairwise Comparison of Force Decay Between Different Elastomeric Chain Type Using Post Hoc Analysis.
Descriptive analysis revealed that for the continuous chains, the highest mean value was observed in orange juice (127.47 ± 1.16), followed by artificial saliva (121.26 ± 1.13) and cola (109.21 ± 1.37). Lower mean values were recorded in tea (92.04 ± 1.11) and coffee (90.86 ± 1.40). In the short-chain group, the highest mean value was also noted in artificial saliva (122.05 ± 1.25), with lower values in tea (86.42 ± 0.81), coffee (84.04 ± 1.16), cola (83.42 ± 1.53), and orange juice (79.99 ± 1.42). For the long chains, artificial saliva again yielded the highest mean value (123.57 ± 1.51), followed by tea (86.27 ± 1.22), coffee (82.99 ± 1.01), cola (81.12 ± 1.85), and orange juice (75.70 ± 1.98). Overall, across all chain types, artificial saliva consistently maintained the highest mean values, suggesting minimal degradation of elastomeric force in this medium. In contrast, exposure to orange juice and coffee resulted in lower mean values, particularly in the short- and long-chain groups.
Pairwise Comparisons
In pairwise comparison of mean differences among the three types of elastomeric chains, continuous chains demonstrated significantly higher mean values compared with short chains (mean difference, 16.638; P < .05) and long chains (mean difference, 18.240; P < .05). Furthermore, short chains exhibited slightly higher mean values than long chains (mean difference, 1.602; P < .05), and this difference was also statistically significant. These results indicate significant differences among all three types of elastomeric chains, with continuous chains maintaining the highest force values, followed by short chains and then long chains. The mean force measured differences between continuous and short, continuous and long, as well as short and long, were found to be statistically significant (P < .05). The continuous chains maintained superior force values across all test solutions, with relatively better performance in artificial saliva and citrus-based liquids. Short chains showed moderate force retention, while long chains exhibited the most pronounced degradation, particularly in acidic and pigmented beverages.
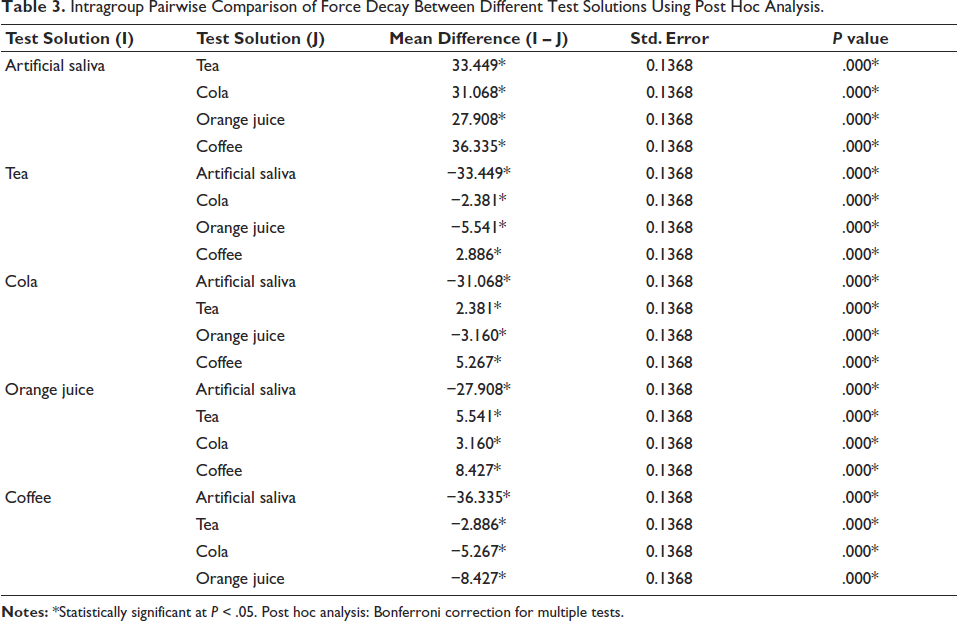
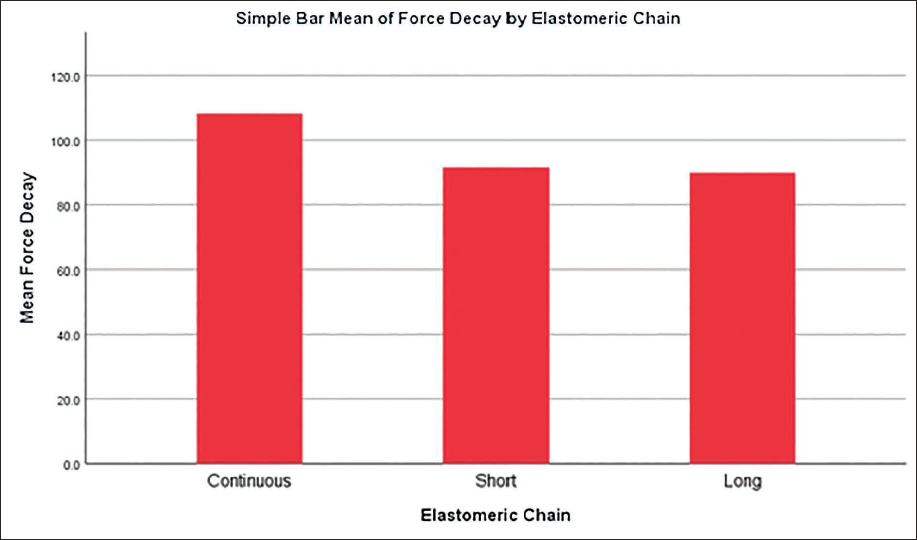
Intragroup pairwise comparison of force reduction between different test solutions and artificial saliva was conducted using post hoc analysis, given in Table 3, which revealed that the mean difference in force decay was statistically significant between all pairs of test solutions (P < .05). These results indicate that each solution had an impact on the force decay rate, emphasizing the varying effects of different beverages on the elastomeric chains. Among the tested solutions, artificial saliva consistently showed the least force decay, serving as a control. Conversely, coffee showed the highest mean force decay, with a mean difference of 36.335 g when compared to artificial saliva. The following patterns were noted: (a) tea, cola, orange juice, and coffee each caused significantly greater force degradation compared to artificial saliva. (b) When compared amongst each other, coffee caused significantly more force decay than tea (mean difference: 2.886 g), cola (5.267 g), and orange juice (8.427 g). (c) Similarly, tea caused more force degradation than cola and orange juice, but less than coffee. (d) Cola demonstrated greater force decay than orange juice. A simple bar graph of mean force decay in different groups of orthodontic elastomeric chains is shown in Figure 4.
Intragroup Pairwise Comparison of Force Decay Between Different Test Solutions Using Post Hoc Analysis.
A Simple Bar Graph of Mean Decay of Force in Different Groups of Orthodontic Elastomeric Chain.
These findings indicate that all tested beverages influenced the decay of force in elastomeric chains differently, with acidic and caffeinated solutions such as coffee and tea showing a more detrimental effect.
Discussion
Orthodontic treatment aims to accomplish efficient tooth movement with minimal side effects, and this is often achieved through the application of light, continuous forces. Various methods are available for generating these forces to close orthodontic spaces, each with its own advantages and limitations. Elastomeric chains are a widely used method due to their ease of application, affordability, and ensuring comfort for patients as well as clinicians. However, one of the significant challenges of using elastomeric chains is force decay, which occurs over time. This degradation can affect the efficiency and effectiveness of orthodontic treatment.
Mirhashemi et al. 7 studied the force degradation in elastomeric chains from three manufacturers (American Orthodontics, Gestenco Applied Composite (GAC), and Ortho-Technology) immersed in distilled water. They found that within the initial 24 h, 50%-70% of the applied initial force was lost, with most of the decay in force generated during the first hour. By the end of 2 weeks, only a small percentage of the original force was preserved. This degradation is affected by several factors, including the chain’s design, manufacturing process, environmental factors, and temperature.
Additional studies have highlighted various elements that influence the decay of force in elastomeric chains. For example, Ferriter et al. 8 explored how the pH of the mouth affects the rate at which orthodontic elastics lose their strength. They found that elastics degrade faster in a more basic (alkaline) environment, making such conditions particularly challenging for maintaining the strength of polyurethane elastics. Jeffries and von Fraunhofer 9 also studied the effects of alkaline glutaraldehyde solutions on elastomeric chains, finding that exposure weakened the chains, making them stretch more to apply a consistent force. Additionally, both artificial saliva and fluoride treatments were found to further weaken the elastics, making them less effective in generating the required forces.
The current study examined the decay of force in three varieties of elastomeric chains—long, short, and continuous, when exposed to artificial saliva and four beverages: tea, cola, orange juice, and coffee. Using 300 Ormco Generation II Power Chains, each chain type was divided into control and test groups. As Kim et al. 10 suggested, the pre-stretching of elastomeric chains to double their original length to prevent initial force decay, the chains in the current study were pre-stretched and fixed at an initial force of 250 g. The chains were exposed to test solutions twice a day for 30 s over 28 days, then rinsed and returned to artificial saliva. After 28 days, the long chains showed the highest force decay, while the continuous chains showed the least.
These findings are consistent with Blagec et al., 4 who concluded that short elastomeric chains maintained higher forces than medium-length chains, suggesting that the force decay was more pronounced in medium chains than in short chains.
Similar studies, such as that by Nachan et al., 11 which assessed the impact of beverages like tea, cola, and mouthwash on orthodontic elastomeric chain degradation, found that tea caused the greatest degradation, particularly for the Ormco Power Chain. However, this study had several limitations, including the lack of pre-stretching of the elastomeric chains, which would have contributed to greater initial force decay. In contrast, this study adhered to best practices by pre-stretching the elastomeric chains, ensuring that the initial force decay was minimized. Additionally, while Nachan et al. concluded their study after 21 days, this study prolonged the evaluation period to 28 days, making the findings more clinically relevant since orthodontists typically replace elastomeric chains every 28 days.
Sam et al. 5 studied how chlorhexidine mouth rinse affects the force decay of closed, short, and long elastomeric chains. They found that chlorhexidine does not speed up force decay, so it likely does not affect the clinical effectiveness of the chains. The main difference between their study and the current study is the experimental setup. Sam et al. tested only one solution, chlorhexidine, while the current study tested four different beverages: tea, cola, orange juice, and coffee.
In conclusion, the study highlights that commercially consumed beverages, particularly coffee and cola, significantly affect the force decay of various configurations of orthodontic elastomeric chains, particularly on long chains, while the continuous chain had the least impact on force decay. These findings suggest that orthodontic patients may need to limit the use of long chains in patients for desired results.
Conclusion
Continuous elastomeric chains exhibited the least force decay, followed by short chains, with long chains demonstrating the greatest force degradation after 28 days of exposure. Exposure to commercially available beverages, particularly orange juice and coffee, accelerated the force decay in all varieties of elastomeric chains compared with artificial saliva. Continuous chains maintained superior force levels across all test conditions and are thus recommended for clinical situations requiring more sustained force over time. Long elastomeric chains showed the highest susceptibility to force degradation and may be less effective when sustained orthodontic forces are critical. Clinicians should consider both the configuration of elastomeric chains and the potential impact of dietary habits when planning orthodontic treatments to optimize tooth movement and minimize treatment duration.
Footnotes
Acknowledgments
The authors want to gratefully acknowledge the Department of Orthodontics, Modern Dental College and Research Centre, Indore, for providing the infrastructure and resources essential for the successful execution of this study. Special thanks are extended to Dr. Amit Bhardwaj, Dean, Professor, and Head, Department of Orthodontics, for his invaluable guidance and unwavering support throughout the research process. The authors also express sincere gratitude to Dr. Poonam Singh, Associate Professor, Department of Orthodontics, for her continuous encouragement, constructive feedback, and mentorship. The authors would like to thank their fellow postgraduate colleagues for their help with specimen preparation and data collection. Finally, the authors acknowledge all individuals who contributed, directly or indirectly, to the completion of this research.
Authors’ Contribution
Rohan Kumawat: Data curation, investigation, methodology; Poonam Singh: Project administration, supervision; Amit Bhardwaj: Project administration, supervision, validation; Jeenal Gupta: Writing – review and editing; Kratika Mishra: Writing – original draft; Ankit Verma: Formal analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was approved by the Institutional Ethics Committee (approval no. MDC/IECI14/2023) on 22/09/2023, and certification was obtained. No human participants, patient data, or clinical interventions were involved in this study. Hence, informed patient consent was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.