
Abstract
Background
Malocclusion, a common dental anomaly, results from complex interactions between genetic, environmental, and nutritional factors. Vitamin D and calcium play key roles in bone metabolism and craniofacial development. However, their influence on malocclusion patterns remains underexplored.
Aim
To investigate the relationship between serum vitamin D and calcium levels and the presence of malocclusion in an orthodontic patient population.
Method
A cross-sectional in vivo study was conducted on 96 patients aged 15-40 years. Clinical evaluation included Angle’s classification, overjet and overbite measurements, and the assessment of crowding. Serum 25-hydroxyvitamin D [25(OH)D] was analyzed via enzyme immunoassay (EIA), and calcium levels were analyzed by ion-selective electrode (ISE) potentiometry. Data were analyzed using one-way analysis of variance (ANOVA) and Tukey’s Honestly Significant Difference (HSD) test.
Result
The majority of participants (77.1%) had suboptimal vitamin D levels; 21.9% were calcium-deficient. Class I malocclusion was most prevalent (60.4%). While trends suggested higher overjet and overbite values in vitamin D-deficient individuals, no statistically significant correlation was found between malocclusion types and serum vitamin D or calcium levels.
Conclusion
Although no significant associations were identified, subtle trends suggest vitamin D and calcium may influence occlusal development. Longitudinal studies are warranted to validate these findings.
Introduction
Malocclusion, defined as a malalignment of teeth or incorrect relation between the dental arches, affects a large proportion of the global population and is considered one of the most prevalent dental issues.1, 2 It can have significant effects on oral health, psychological well-being, and social interactions, particularly among adolescents and young adults.3, 4 The etiology of malocclusion is multifactorial and includes hereditary components, environmental influences, and functional habits such as thumb sucking, mouth breathing, and abnormal swallowing.5-7
Among various environmental factors, nutrition plays an increasingly recognized role in craniofacial development. 8 Of particular interest are calcium and vitamin D, which are integral to bone health and tooth development. Vitamin D facilitates calcium absorption and regulates bone remodeling by influencing osteoblast and osteoclast activity via its receptor, VDR (vitamin D receptor).9, 10 A deficiency in vitamin D has been linked to delayed tooth eruption, enamel hypoplasia, and structural deformities such as mandibular underdevelopment.11-13
Calcium is equally essential in the development of enamel and dentin, and in maintaining the structural integrity of alveolar bone.14, 15 Studies have shown that hypocalcemia may impair odontogenesis, increase caries susceptibility, and interfere with normal occlusal development. 16 While orthodontic research has historically focused on biomechanical factors, emerging evidence supports the role of vitamin D and calcium in influencing tooth movement, bone turnover, and craniofacial growth patterns.17-19
Despite these known functions, the direct correlation between vitamin D/calcium levels and malocclusion type remains insufficiently studied. In South Asian populations, vitamin D deficiency is endemic even in sun-rich regions, with adolescent and young adult groups showing the highest rates of deficiency.20, 21 Furthermore, dietary calcium intake often falls below recommended daily allowances, especially among lower socio-economic groups.22, 23
Therefore, this study aims to explore whether serum levels of vitamin D and calcium are associated with malocclusion patterns in orthodontic patients. Such research could help guide preventive interventions through dietary supplementation and improve treatment planning for patients at risk of altered bone metabolism.
Materials and Methods
The sample size was determined using the formula for proportion estimates based on the following parameters: Z 2 α/2 = 1.96 (for 95% confidence), expected prevalence (p) = 35%, and margin of error (E) = 5%. The minimum sample size was calculated to be 84 participants. To improve statistical power and account for potential data variability, 96 participants were recruited.
A total of 96 subjects aged between 15 and 40 years were enrolled using stratified random sampling to ensure a representative distribution across age and gender. Inclusion criteria were: (a) age ≥15 years, (b) full complement of permanent teeth excluding third molars, (c) no prior orthodontic treatment, (d) absence of systemic or metabolic disorders affecting bone physiology, and (e) no congenital craniofacial anomalies. Exclusion criteria included current chemotherapy, bisphosphonate therapy, gastrointestinal disorders affecting nutrient absorption, pregnancy, and edentulism.
Orthodontic assessment included Angle’s classification (Class I, II, and III), overjet and overbite measurements, and crowding evaluation using the Hotz Scale. Overjet and overbite were recorded in millimeters, using a standardized orthodontic ruler. Dental crowding was categorized as mild (1–3 mm), moderate (4–6 mm), or severe (>7 mm). Diagnostic radiographs included lateral cephalograms for skeletal relationship assessment and orthopantomograms (OPGs) for identifying developmental or dental anomalies.
Maxillary and mandibular impressions were obtained using irreversible hydrocolloid (alginate), and casts were immediately poured using Type III dental stone (Orthocal). The study models were utilized for detailed occlusal and sagittal relationship analyses.
Fasting venous blood samples (8-10 h fasting) were collected from each participant under aseptic conditions. Serum was separated by centrifugation at 3,000 rpm for 10 min.
Vitamin D estimation: Serum 25-hydroxyvitamin D [25(OH)D] was measured using enzyme immunoassay (EIA). Interpretation followed the Endocrine Society guidelines:
<20 ng/mL—Deficient
20–29 ng/mL—Insufficient
30–50 ng/mL—Sufficient
100 ng/mL—Toxic
Calcium estimation: Ionized calcium was measured using ion-selective electrode (ISE) direct potentiometry. Values were categorized as:
<4.64 mg/dL—Low
4.64–5.28 mg/dL—Normal
5.28 mg/dL—High
All samples were processed at a centralized laboratory under standardized calibration and quality control protocols.
Data were entered in Microsoft Excel and analyzed using Statistical Package for the Social Sciences (SPSS) software (version 25.0; IBM Corp., Armonk, NY). Descriptive statistics summarized demographic, clinical, and biochemical variables. One-way analysis of variance (ANOVA) was used to compare mean vitamin D and calcium levels across malocclusion types. Tukey’s post hoc test was applied where relevant. Pearson’s correlation coefficient was employed to evaluate the relationships between serum vitamin D and calcium levels with overjet and overbite measurements. A P value < .05 was considered statistically significant.
Results
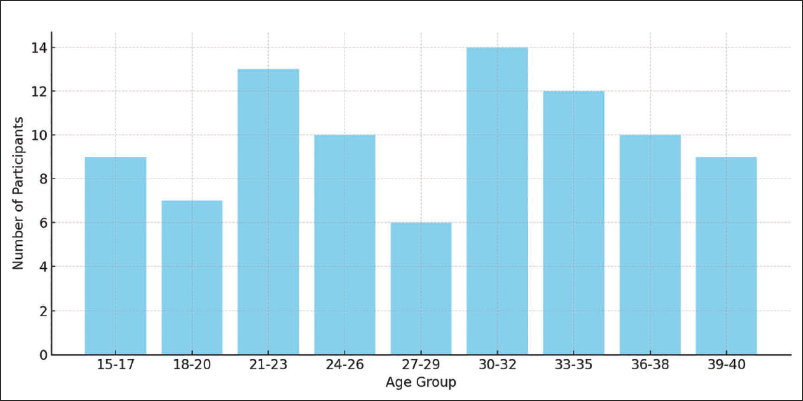
A total of 96 participants aged between 15 and 40 years (mean age = 28.1 ± 7.48 years) were included in this study. The cohort comprised 51 males (53.1%) and 49 females (46.9%). Participants were stratified based on socio-economic status into low (34.4%), middle (43.8%), and high (21.9%) income groups (Figure 1).
Biochemical Analysis
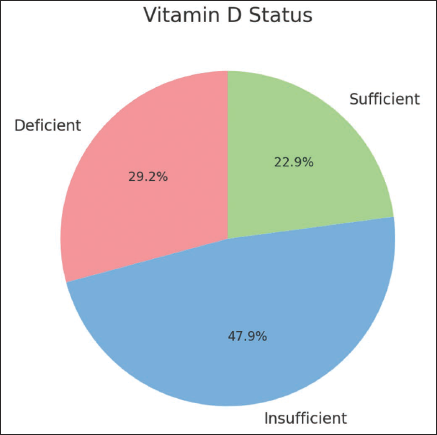
The mean serum 25(OH)D level was 24.75 ± 7.83 ng/mL. According to standard clinical guidelines, serum vitamin D levels of ≥30 ng/mL are considered sufficient, 20–29 ng/mL are considered insufficient, and <20 ng/mL are considered deficient. 24 29.2% of participants were vitamin D deficient (<20 ng/mL), 47.9% had insufficient levels (20–29 ng/mL), and only 22.9% had sufficient levels (30–50 ng/mL) (Figure 2). None of the participants had toxic levels (>100 ng/mL).
Age Distribution of Participants
Vitamin D Status Among Participants.
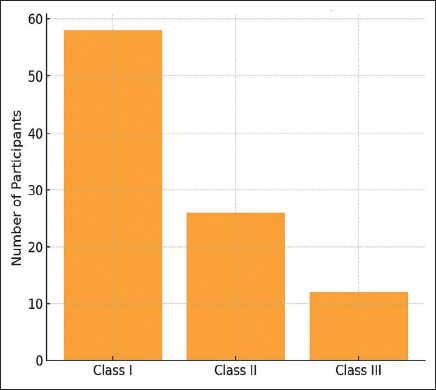
Frequency of Malocclusion Types.
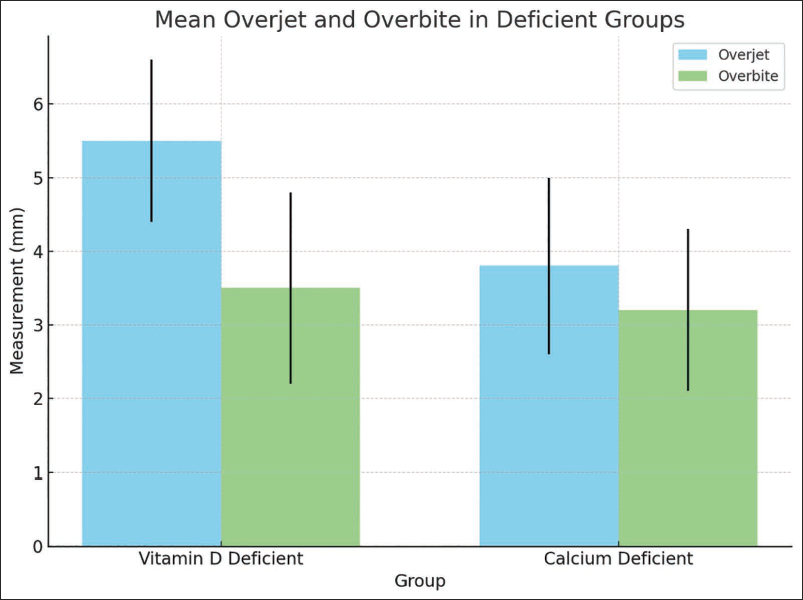
Impact of Deficiencies on Overjet and Overbite.
The mean serum calcium level was 4.87 ± 0.31 mg/dL. Of all participants, 21.9% were classified as calcium deficient (<4.64 mg/dL), 68.8% had normal levels (4.64–5.28 mg/dL), and 9.4% had high levels (>5.28 mg/dL).
Malocclusion Classification
Based on Angle’s classification, Class I malocclusion was the most prevalent, observed in 60.4% of participants (n = 58), followed by Class II in 27.1% (n = 26), and Class III in 12.5% (n = 12) (Figure 3). The mean serum vitamin D levels in Class I, II, and III malocclusion groups were 18.4, 17.9, and 19.1 ng/mL, respectively, with no statistically significant differences observed among the groups (P > .05).
Dental Crowding Assessment
Using the Hotz scale, crowding was classified as mild in 44 participants (45.8%), moderate in 26 (27.1%), and severe in 8 participants (8.3%). No crowding was reported in 18 individuals (18.8%). The presence of dental crowding showed no significant correlation with vitamin D or calcium levels.
Overjet and Overbite Measurements
The mean overjet and overbite were marginally higher in vitamin D-deficient individuals compared to those with sufficient levels. Vitamin D-deficient subjects had a mean overjet of 5.5 ± 1.1 mm and a mean overbite of 2.5 ± 1.3 mm, while calcium-deficient participants had values of 2.8 ± 1.2 and 2.2 ± 1.1 mm, respectively (Figure 4).
Statistical Analysis
ANOVA was employed to evaluate differences in vitamin D and calcium levels across the three malocclusion groups. For vitamin D, the F value was 0.585 (P = .559), and for calcium, the F value was 0.141 (P = .868), indicating no statistically significant differences. Tukey’s Honestly Significant Difference (HSD) test also confirmed the absence of significant intergroup differences.
Pearson correlation analysis revealed no significant correlation between vitamin D levels and malocclusion type (r = −0.12, P = .22), or calcium levels and malocclusion type (r = 0.06, P = .52). However, a weak positive correlation was observed between vitamin D levels and both overjet (r = 0.10, P = .24) and overbite (r = 0.18, P = .08), indicating a trend toward increased values in vitamin D-deficient individuals.
These findings suggest that although vitamin D and calcium deficiencies are prevalent, they may not be directly associated with the type of malocclusion. However, their subtle effects on occlusal parameters such as overjet and overbite could be of clinical interest.
Discussion
This cross-sectional study evaluated the association between serum vitamin D and calcium levels with the type of malocclusion among 96 orthodontic patients aged 15 to 40 years. Despite finding no statistically significant association between these nutrient levels and Angle’s classification of malocclusion, the data reveal concerning trends in the prevalence of vitamin D and calcium deficiencies. These deficiencies were present in 77.1% and 21.9% of participants, respectively.
Vitamin D is essential for calcium absorption and bone mineralization, and it plays a crucial role in osteoblastic differentiation and osteoclastic regulation via the RANK/RANKL pathway.9, 24 It also influences craniofacial development, especially mandibular growth and alveolar bone stability.10, 25 Several studies have suggested that VDR polymorphisms are associated with skeletal discrepancies, including mandibular retrognathism and maxillary hypoplasia.6, 26
Although the current study did not show a direct relationship between malocclusion types and biochemical deficiencies, this may be due to the cross-sectional design and the age group studied. Most craniofacial growth occurs during childhood and adolescence, and deficiencies occurring in the early developmental stages might have a more significant impact than deficiencies observed in adults.27-29 It is plausible that the long-term effects of early-life vitamin D and calcium deficiencies were not detectable at the time of the examination. Our findings align with Alqahtani et al., 11 who reported no significant correlation between vitamin D levels and malocclusion in their patient cohort. In contrast, Küchler et al. 6 observed associations between VDR gene variants and craniofacial patterns, suggesting a gene-nutrient interaction rather than a direct cause–effect relationship. Additionally, animal models have demonstrated that VDR knockout leads to mandibular micrognathia and delayed tooth eruption, further supporting the biological plausibility of our hypothesis. 5
The observed higher overjet and overbite measurements in vitamin D-deficient individuals, although not statistically significant, align with studies highlighting the effect of vitamin D on bone density and remodeling dynamics.19, 24 Vitamin D is also known to modulate the pace of orthodontic tooth movement and to influence periodontal ligament function.30, 31 Calcium, similarly, is essential for tooth mineralization and alveolar bone integrity; its deficiency can exacerbate periodontal disease, potentially influencing tooth positioning.16, 32
Several limitations must be acknowledged. The sample size, though adequate for preliminary analysis, may have limited power to detect subtle differences. The cross-sectional design precludes causal inference, and serum measurements reflect short-term status rather than cumulative nutritional history. Future longitudinal studies incorporating genetic screening and dietary assessments would provide more robust evidence.
Despite these limitations, our study highlights the importance of addressing nutritional deficiencies in orthodontic populations. Early detection and correction of vitamin D and calcium deficiencies could have implications not only for systemic health but also for improving craniofacial development outcomes and orthodontic treatment responses.
Conclusion
Although no significant association was found between vitamin D or calcium levels and malocclusion types, there was an increase in overjet and overbite in cases of vitamin and calcium deficiency. A widespread deficiencies and subtle clinical trends highlight the need for further research. Nutritional assessments may support preventive orthodontic strategies and enhance treatment planning in deficient populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Institutional Ethical Committee (Ref: IEC/P-259/2023), and informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.