
Abstract
Introduction
The extended duration of traditional orthodontic treatment remains a significant patient concern. This study compared platelet-rich plasma (PRP) and injectable platelet-rich fibrin (i-PRF) for accelerating orthodontic tooth movement (OTM) and assessing associated pain.
Methods
A total of 11 patients were studied using a split-mouth design, with randomized allocation of PRP to one quadrant and i-PRF to the contralateral quadrant. Interventions were administered at 21-day intervals. Canine retraction rates were measured using dental casts, while pain perception was quantified via visual analog scale (VAS) during a 1-week follow-up period.
Results
The i-PRF group demonstrated significantly faster OTM (2.13 ± 0.31 mm/month) compared to PRP (1.61 ± 0.28 mm/month; P = .0002), representing a 32.3% increase in movement rate. Pain levels were low but statistically higher with i-PRF (VAS 2.26 ± 0.98) versus PRP (VAS 1.9 ± 1.0; P = .0001), though both remained within clinically acceptable ranges.
Conclusion
i-PRF is more effective in accelerating OTM than PRP, with only marginally greater transient discomfort. These findings support i-PRF as a clinically viable biological adjunct for reducing orthodontic treatment duration.
Keywords
Introduction
Orthodontic treatment has come a long way, revolutionizing the way we align and correct misaligned teeth. Traditional orthodontics often involves a lengthy treatment duration, which can sometimes discourage patients from pursuing the smile they desire. However, with the advent of accelerated orthodontics, patients now have the opportunity to achieve their dream smile faster than ever before. Clinicians are continuously working to develop various strategies that can improve the rate of orthodontic tooth movement (OTM). 1 Various techniques aim to accelerate OTM, categorized as invasive and noninvasive. Noninvasive methods include biomechanical (e.g., self-ligating brackets), physiological (e.g., electric current simulation, low-dose laser therapy, vibrations, photobiomodulation), and pharmacological approaches (e.g., prostaglandin or relaxin injections). 2 Invasive techniques such as corticision, orthognathic surgery, piezocision, piezopuncture, and micro-osteoperforations are proven to be highly effective in accelerating OTM. However, these surgical methods, while achieving faster results, pose challenges for both patients and orthodontists.
The relationship between platelet concentrates and OTM has drawn some attention lately. Animal studies3, 4 and clinical studies5–13 have evaluated the effects of platelet concentrates on OTM and indicated a positive correlation between local injection of platelet concentrates and acceleration of OTM. These studies conclude that platelet concentrates may accelerate OTM by decreasing alveolar bone density on paradental tissues by transiently enhancing osteoclastic activity. 4
As platelet concentrate research advances, injectable platelet-rich fibrin (i-PRF) emerges as an innovative technique to expedite OTM. This autologous platelet concentrate, rich in healing factors, leukocytes, and growth stimulants, stands out for its anticoagulant-free approach, minimal blood requirement, and cost-effective, time-efficient process. i-PRF, with shorter centrifugation times and reduced RPM requirements, shows promise across various medical and dental fields, including orthodontics, oral and maxillofacial surgery, dermatology, orthopedics, plastic surgery, and ophthalmology. In a cellular study conducted by Wang et al., 14 the impact of i-PRF on osteoblastic activity and bone formation was examined, it was found that i-PRF led to a significant threefold rise in osteoblast migration and proliferation as compared to platelet-rich plasma (PRP) which showed a twofold increase only. Therefore, i-PRF is expected to be more efficient in expediting OTM.
Though there are studies12, 15 examining the use of i-PRF and PRP individually for accelerating OTM, there is currently a lack of scientific literature that presents a direct comparison between the two different platelet concentrates.
To the best of our knowledge, this study is one of the first clinical studies to directly compare two different platelet concentrates on the rate of OTM. The null hypothesis assumes no difference in movement rates between the PRP and i-PRF-treated sites. The study aims to assess the impact of PRP and i-PRF on OTM and evaluate associated pain during the procedure.
Study Design and Duration
A prospective, split-mouth randomized clinical study extending for a duration of 15 months. The study duration was from June 2021 to September 2022.
Materials and Methods
The study was approved by the ethical committee of the institute. The Consolidated Standards of Reporting Trials (CONSORT) statement was followed (Figure 1). Patients were enrolled from the OPD of the Department of Orthodontics of the institute for the split-mouth study to compare the effect of PRP and i-PRF on the rate of OTM. Patients who required maxillary first premolar extractions for orthodontic therapy were chosen and randomly allocated to one of the two groups.
Consolidated Standards of Reporting Trials (CONSORT) Flowchart.
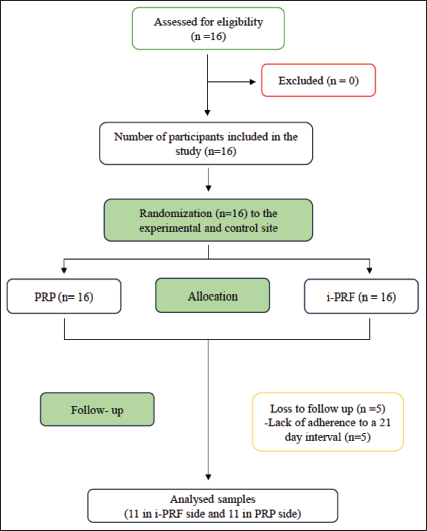
The principal investigator (SR) performed randomization using a web-based randomizer (Stat Trek). Eight unique numbers were generated from 1 to 16, assigning these patients to PRP (right)/i-PRF (left); the remaining eight received the reciprocal allocation. Sequentially numbered opaque envelopes maintained concealment until enrolment by the first investigator (AAM). This 1:1 complete randomization ensured balanced groups and minimized bias. Outcome assessors measuring dental casts were blinded to intervention groups. The inclusion criteria were as follows: (a) patients between 12 and 30 years of age with a comprehensive orthodontic treatment plan involving bilateral symmetric extraction of maxillary first premolars, (b) good general and oral health, (c) complete permanent dentition, (d) full banding/bonding of teeth in both arches. Patients with a history of bleeding disorders and systemic illness, poor periodontal condition, restorations or large carious lesions, abnormalities in teeth size and/or shape, previous history of orthodontic treatment, long-term medication intake such as nonsteroidal anti-inflammatory drugs (NSAIDs), autoimmune diseases, pregnant, and/or lactating women were excluded from the study. No protocol deviations occurred during the trial. Interim analyses and stopping rules were deemed unnecessary.
Sample Size
The sample size of the study was determined using G*Power 3.0 software for a paired t-test. With a target alpha of 0.05, power of 95%, and effect size of 0.55 from a pilot study conducted (mean rate of tooth movement 1.36 ± 0.59 mm vs 1.64 ± 0.32 mm), a minimum total sample size of 22 sites was established, that is, 11 patients. Sixteen patients were enrolled in the study to overcome attrition of samples, if any, during the course of the study. Patients were randomized 1:1 into two groups: PRP (right)/i-PRF (left) and PRP (left)/i-PRF (right).
Methodology
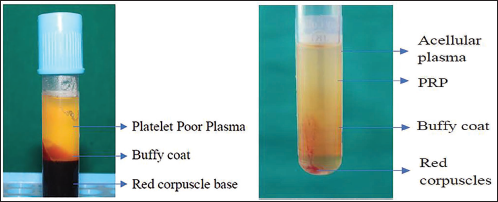
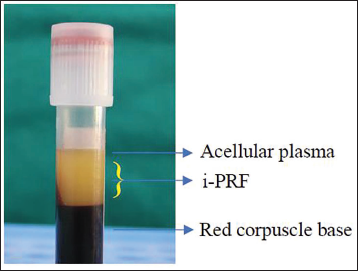
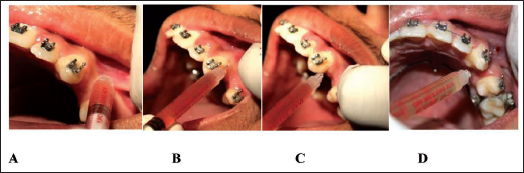
A total of 16 patients who fulfilled the inclusion criteria were selected from the Department of Orthodontics for the study. The procedure was explained to the patients/parents, and informed written consent was obtained in their vernacular language. Preoperative records were taken, and the orthodontic treatment plan was established. After banding and bonding with the MBT prescription with 0.022 slots (Mini Diamond Single Patient Kit, ORMCO, USA), as per the treatment plan, the extraction of both maxillary first premolars was done. Initial alignment and leveling were carried out with NiTi wires. A transpalatal arch, soldered to the first molars, was used for conserving anchorage. After reaching 0.019 × 0.025 SS wire, sliding mechanics was used for the canine retraction using the active tie-back method with 150 g force. A reverse curve of speed was also incorporated into the working wire. An alginate (Tropicalgin, Zhermack, Italy) impression was recorded before the administration of PRP and i-PRF at every visit, and a study cast was made. The distance between the distal wings of the canine bracket and the mesial opening of the buccal tube of the first molar was measured with a digital vernier caliper by the principal investigator (SR) and was considered as T0 (Figure 2). The process was repeated four times with an interval of 21 days, and the data collected were represented as T1, T2, T3, and T4, respectively. The difference between T0 and T4 was the amount of canine retraction in 84 days. The injections were administered by the first investigator (AAM) four times during the study period. Second investigator (AS) repeated the measurements on the cast after 1 week to assess the interclass coefficient and determine the reliability of the measurements. PRP was freshly prepared using a double centrifugation (first: 2,000 RPM/10 min; second: 3,000 RPM/15 min) and i-PRF using the single spin method (700 RPM/3 min, no anticoagulant) as per Miron’s protocol 16 (Figures 3 and 4). The intervention site was anesthetized with 2% lignocaine. Forty units (1 mL) of either PRP or i-PRF were then injected intraligamentally in the middle, distobuccal, and distopalatal/distolingual areas of the distal surface of the canines (8 units each area) together with submucosal injections buccally and palatally/lingually (8 units each area) on the allotted right or left side by using an insulin syringe (Figure 5). The patient was then recalled three more times at an interval of 21 days, and the process was repeated. An alginate impression was recorded, and a study cast was made at each visit.
Measuring the Distance Between the Distal Wing of Canine Bracket to the Mesial Opening of Molar Tube by a Digital Vernier Caliper on Both Right and Left Sides in the Dental Cast.

Parts of Platelet-rich Plasma (PRP)—First Centrifuge, Parts of PRP—Second Centrifuge.
Parts of Injectable Platelet-rich Fibrin (i-PRF).
Injection Sites of Local Anesthesia and Platelet-rich Plasma (PRP) and Injectable Platelet-rich Fibrin (i-PRF) Injections; (A) Submucosal Injection, (B) Intraligamentally to Distobuccal; (C) Intraligamentally to Distal; and (D) Intraligamentally to Distopalatal Surface of Canine.
The pain due to the injection was assessed using a visual analog scale (VAS) (Figure 6) that was completed by the patient starting from day one and repeated every day till the first 7 days of every visit. The patients were instructed not to use any analgesics. A form with seven sets of the VAS was provided to the patient. Patients were reminded telephonically every day at 10 am and were asked to fill out the questionnaire until the 7th day of every visit.
Visual Analog Scale.

Statistical Analysis
The IBM-SPSS Software (version 20.0; IBM, Armonk, NY) was used for statistical analysis. The interobserver reliability was studied by the interclass correlation coefficient (ICC) test. A paired t-test was implemented to assess the differences between the PRP and i-PRF sides. P values ≤.05 were considered statistically significant, accompanied by a 95% confidence interval. No additional subgroup or sensitivity analyses were conducted. All analyses adhered to the prespecified statistical plan and followed a per-protocol approach. Since all endpoints were continuous (OTM distance, VAS scores), binary outcomes were not evaluated.
Results
Patient Flow
The study enrolled 16 patients who met the inclusion criteria. Sixteen patients with 32 sites (both right and left) were randomly allotted to PRP (right)/i-PRF (left) and PRP (left)/i-PRF (right). Five patients dropped out of the study because of the lockdown and the difficulties of returning to the department at 21-day intervals during the COVID pandemic. All other patients were followed until the end of the study period with no loss of follow-up, and the rate of OTM, together with concomitant pain assessments, was studied.
Interclass Correlation
The ICC was higher than 0.99, showing that the interexaminer reliability was high.
Canine Retraction Rate
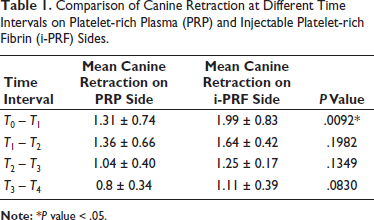
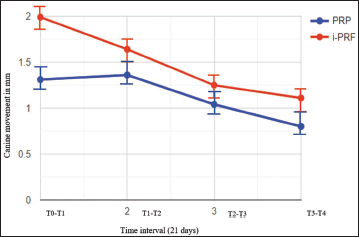
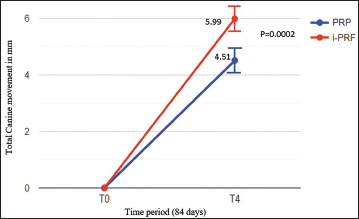
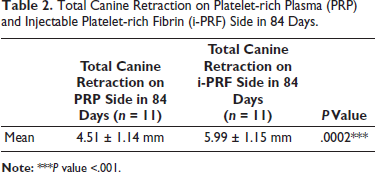
At T0, the mean distance between the distal wing of the canine bracket and mesial opening of the molar tube was 20.63 ± 2.52 mm for the PRP group and 21.48 ± 2.16 mm for the i-PRF group, showing a nonsignificant (P = .408) difference between the preintervention values. Mean maxillary canine retraction at the end of 21 days (T0 – T1) was 1.31 ± 0.74 mm on the PRP side and 1.99 ± 0.83 mm on the i-PRF side. In the second 21-day interval (T1 – T2), the mean canine retraction was 1.36 ± 0.66 mm on the PRP side and 1.64 ± 0.42 mm on the i-PRF side. In the third 21 days interval (T2 – T3), the mean canine retraction was 1.04 ± 0.40 mm on the PRP side and 1.25 ± 0.17 mm on the i-PRF side and in the fourth 21 days interval (T3 – T4), the mean canine retraction was 0.8 ± 0.34 mm on the PRP side and 1.11 ± 0.39 mm on the i-PRF side (Table 1, Figure 7). There was a notable disparity in canine retraction between PRP and i-PRF, with statistically significant findings (P = .0002). On the PRP side, the average retraction in 84 days measured 4.51 ± 1.14 mm, whereas on the i-PRF side, it was 5.99 ± 1.15 mm (Table 2, Figure 8). The rate of canine retraction was 1.61 mm per month for PRP and 2.13 mm per month for i-PRF.
Comparison of Canine Retraction at Different Time Intervals on Platelet-rich Plasma (PRP) and Injectable Platelet-rich Fibrin (i-PRF) Sides.
Mean Canine Retraction at Four-time Intervals on Platelet-rich Plasma (PRP) and Injectable Platelet-rich Fibrin (i-PRF) Side.
Total Canine Retraction of Platelet-rich Plasma (PRP) and Injectable Platelet-rich Fibrin (i-PRF) in 84 Days.
Pain Assessment
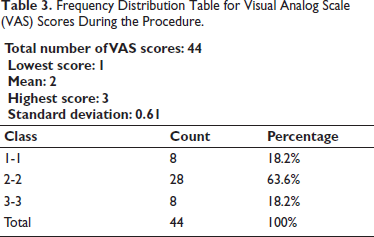
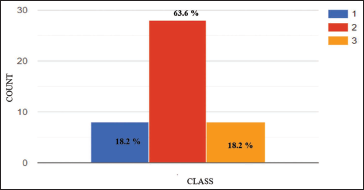
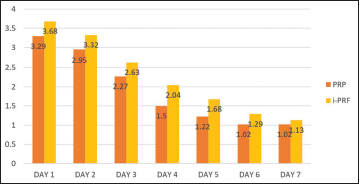
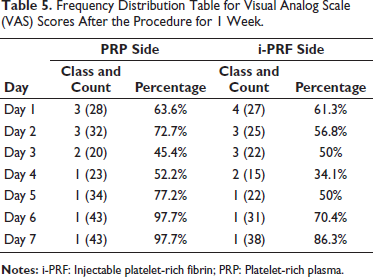
Pain during the procedure at every visit was assessed using the VAS on both sides. A VAS score of 2 was observed in 63.6% of patients, and 18.2% of patients had VAS scores of 1 and 3 each. The mean VAS score during the procedure was 2 ± 0.61; thus, 63.6% of the patients reported having mild pain during the procedure (Table 3, Figure 9). An increase in pain scores was reported on both sides during the study. The i-PRF side showed a greater increase in the pain score than the PRP side. A mean VAS score of 2.26 ± 0.98 was observed on the i-PRF side. The PRP side exhibited a mean VAS score of 1.9 ± 1.0 throughout the 1-week follow-up, which was statistically significant (P = .0001) (Table 4, Figure 10). About 52.2% of patients reported pain to be at baseline by the 4th day on the PRP side, and 50% of patients reported pain to be at baseline by the 5th day on the i-PRF side. By the end of the 7th day, 86.3% of patients reported no pain on both sides (Table 5).
Total Canine Retraction on Platelet-rich Plasma (PRP) and Injectable Platelet-rich Fibrin (i-PRF) Side in 84 Days.
Frequency Distribution Table for Visual Analog Scale (VAS) Scores During the Procedure.
Histogram Showing Frequency Distribution for Visual Analog Scale (VAS) Scores During the Procedures.
Average Pain After the Procedure for 1 Week.
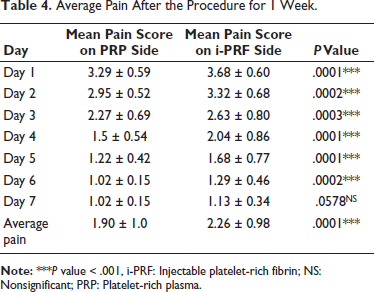
Average Pain After the Procedure for 1 Week.
Frequency Distribution Table for Visual Analog Scale (VAS) Scores After the Procedure for 1 Week.
Discussion
The need of the hour is to accelerate OTM and decrease the overall treatment time. Many methods have been used to accelerate OTM, varying from noninvasive to invasive. PRP and i-PRF have garnered attention due to their user-friendly nature and relatively noninvasive application. Several studies3–13 have provided evidence supporting a positive relationship between the local injection of platelet concentrations and the acceleration of OTM. With the availability of various platelet concentrates, it remains challenging to determine which type is most effective in promoting OTM. Existing studies have predominantly focused on a single type of platelet concentrate, comparing it against a placebo or control group. Our study is the first to directly compare the effectiveness of PRP and i-PRF in this context, addressing the gap in current research.
The split-mouth design used in this investigation helped to account for intrasubject differences. The injections were performed by the first investigator (AAM) into the dentoalveolar ligament of the canines which were helpful by inducing a coagulation cascade and producing thrombin to create a thrombus layer rich with platelets in contact with the alveolar bone and thus facilitating a continuous release of growth factors that begins to leach into the alveolar bone.9, 10 It was also injected submucosally as per the standard protocol for the use of PRP in orthodontics. 2
Previous studies3, 9, 17 have reported that the rate of tooth movement decreased gradually after 21 days of injection. El Timamy et al. 9 have suggested multiple injections to maintain a steady rate of accelerated tooth movement in the long term. The application of multiple injections was considered in this study, and the injections were repeated 4 times at a 21-day interval, and the total duration of the study was calculated to be 84 days.
In the present study, PRP and i-PRF injection accelerated the canine retraction rate during the first month of intervention, and this was perhaps because of the increased release of growth factor that heightened bone regeneration. El-Timamy et al.’s study 9 revealed that canine retraction was faster on the PRP intervention side than on the control side during the first 2 months. However, the movement had slowed down during the third month, which was attributed to the use of calcium chloride as an anticoagulant, which might have affected the results negatively. Our study is in concurrence with Erdur’s 12 and Karakasli’s studies, 13 which showed an acceleration of tooth movement when treatment was combined with i-PRF injections. Our study results are also in agreement with Nemtoi et al.’s 18 and Tehranchi et al.’s 19 studies, which proposed that PRF clots accelerate OTM.
However, our results were not consistent with Pacheco et al., 20 who concluded that the canine distalization rate was faster on the control side than the PRF side. Our study showed a higher increase in the rate of canine retraction in the first month, whereas Zeitounlouian et al.’s 21 observed an accelerated canine retraction in the i-PRF side during the second month. These variations could be related to the differences in injection protocols and may be attributed to the different intervention procedures they adopted in dosage, delivery methods (plug, membrane, or injection), concentrate presentation (PRP, PRF, or L-PRF), and duration of the observation periods.
Effect of PRP on OTM
In our study, we observed a mean maxillary canine retraction at T1 to be 1.31 ± 0.74 mm on the PRP side. At T2, the mean canine retraction was 1.36 ± 0.66 mm. A further increase in the mean canine retraction was seen at this time point. By T3, the mean canine retraction was 1.04 ± 0.40 mm, and at T4, the mean canine retraction was 0.8 ± 0.34 mm. The rate of canine retraction from T0 to T4 was 1.61 mm/month for the PRP side.
Similarly, in the study by Angel et al., 11 the OTM after PRP injection was 2.06 ± 0.36 mm in the first month and 1.12 ± 0.32 mm in the second month. Joy et al. 22 also found that the OTM rate in the PRP group was 1.24 times faster than that of the control group. Interestingly, El-Timamy et al. 9 showed that the rate of canine retraction was faster in the first 2 months (1.55 ± 0.63 mm and 1.33 ± 0.87 mm) but slower in the 3rd month (0.59 ± 0.96 mm). The method of canine retraction used was NiTi closed coil spring with temporary anchorage devices (TADs) as anchorage in these studies.
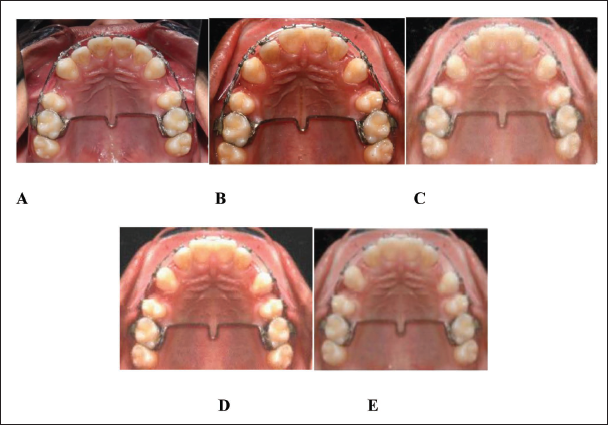
Angel et al. 11 demonstrated a greater increase in OTM; however, their study was limited to a period of 2 months. In contrast, El-Timamy et al. 9 observed a faster rate of canine retraction during the first 2 months but a slower rate in the third month. To achieve an accelerated canine retraction, we employed multiple injections, which resulted in a significant enhancement. It is noteworthy that the previous studies utilized a single-time injection and employed a coil spring with TADs for continuous tooth movement. In our study, we employed the active tie-back method, which is commonly practiced in clinical settings. Figure 11 illustrates the treatment progress of a representative case.
Treatment Progress of a Representative Case (A) At T0, (B) At T1 (21 Days), (C) At T2 (42 Days), (D) At T3 (63 Days), and (E) AtT4 (84 Days). Right Side Shows Platelet-rich Fibrin (PRP) and Left Side Shows Injectable Platelet-rich Fibrin (i-PRF).
Effect of i-PRF on OTM
The rate of canine retraction from T0 to T4 showed a higher mean retraction rate of 2.13 mm/month for the i-PRF side. In our study, we observed a mean maxillary canine retraction at T1 to be 1.99 ± 0.83 mm on the i-PRF side. At T2, the mean canine retraction was 1.64 ± 0.42 mm. By T3, the mean canine retraction was 1.25 ± 0.17 mm, and at T4, the mean canine retraction was 1.11 ± 0.39 mm. Similar to the PRP side, the mean canine retraction rates showed a decreasing pattern on the i-PRF side.
In 2020, Karakasali and Erdur 13 assessed the efficiency of i-PRF injection in the retraction rate of the maxillary incisor and concluded that the OTM was significantly greater in the i-PRF group, exhibiting notable differences compared to the control group across all time intervals. In another clinical research by Zeitounlouian et al., 21 the maxillary canine retraction was evaluated following i-PRF therapy, and they reported a significantly greater canine retraction on the i-PRF side compared with the control side in the second month. Recently, Erdur et al. 12 found a significantly increased rate of tooth movement for i-PRF, verified by the stimulation in the inflammatory cytokine levels. Another study by Karci and Baka 10 compared piezocision with i-PRF injection in tooth movement during canine distalization and concluded that although both applications facilitate tooth movement, there is no distinction in terms of the amount, speed, duration of tooth movement, or periodontal parameters.
Comparison of i-PRF and PRP
In our study, we observed the mean maxillary canine retraction over four-time intervals. At the end of the initial 21-day period (T0 – T1), the mean retraction on the PRP side was 1.31 ± 0.74 mm, while on the i-PRF side, it was 1.99 ± 0.83 mm (representing a 45.8% increase compared to the PRP side). In the second 21-day interval (T1 – T2), the mean retraction was 1.36 ± 0.66 mm on the PRP side and 1.64 ± 0.42 mm on the i-PRF side (a 20.5% increase compared to the PRP side). Similarly, during the third 21-day period (T2 – T3), the mean retraction was 1.04 ± 0.40 mm on the PRP side and 1.25 ± 0.17 mm on the i-PRF side (a 20.2% increase compared to the PRP side). Lastly, in the fourth 21-day interval (T3 – T4), the mean retraction was 0.8 ± 0.34 mm on the PRP side and 1.11 ± 0.39 mm on the i-PRF side (a 38.7% increase compared to the PRP side) (Table 1, Figure 6). Overall, over the course of 84 days, the mean canine retraction achieved with PRP was 4.51 ± 1.14 mm, while with i-PRF it was 5.99 ± 1.15 mm (representing a 32.8% increase compared to the PRP side) (Table 2, Figure 7).
The rate of canine retraction from T0 to T4 showed a statistically significant difference between the PRP and i-PRF (P = .0002) sides, with a mean retraction rate of 1.61 mm/month for the PRP side and 2.13 mm/month for the i-PRF side. It is worth noting that the average rate of OTM using conventional methods is estimated to range from 0.8 to 1.2 mm per month.
Our study observed a decline in the rate of acceleration in both the PRP and i-PRF intervention groups. This decrease in acceleration rate can be attributed to the degradation of platelet-rich concentrates and the decrease in exogenous growth factors and cytokines over time. This, in turn, may lead to a reduction in autogenous growth factors and cytokines, which could decrease OTM through a negative feedback mechanism. This observation provides a potential explanation for the decreasing pattern of the rate of acceleration observed in our study.
The results of our study were consistent with the results of Gupta et al., 8 Angel et al., 11 Li et al., 23 El-Timamy et al., 9 Güleç et al., 17 Rashid et al., 3 Liou, 2 Erdur et al., 12 and Karakasli and Erdur’s 13 studies, which found that treatment combined with PRP or i-PRF accelerated OTM. Our results showed a faster rate of canine retraction on the i-PRF side (2.13 times) than on the PRP side (1.61 times).
Pain Assessment
About 63.6% of the patients reported having mild pain during the procedure. An increase in pain scores was reported on both sides during the study. The i-PRF side showed a greater increase than the PRP side, with a mean VAS score of 2.26 ± 0.98. The PRP side had a mean VAS score of 1.9 ± 1.0 throughout the 1-week follow-up. This difference was statistically significant (P = .0001).
However, there was no pain by the 4th day on the PRP side in 52.2% of patients, and on the i-PRF side, the pain subsided to baseline levels by the 5th day in 50% of patients. By the end of the 7th day, 86.3% of patients reported no pain on both sides.
The increased pain score in i-PRF might be due to the increased rate of tooth movement or increased concentration of growth factors and bone remodeling at the injection site. But the actual effect and mechanism of pain can only be elucidated by further well-designed studies. No adverse events or treatment-related harms were reported for either PRP or i-PRF interventions during the study period.
While this study demonstrated the superior efficacy of i-PRF in accelerating OTM, certain limitations must be acknowledged. Methodologically, we did not evaluate whether tooth movement occurred through bodily movement or tipping, nor potential gender-based variations in bone response. Moreover, a single-centered design and specific age range (12–30 years) may limit generalizability, despite rigorous standardization. Additionally, in order to holistically evaluate whether this technique reduces the total treatment time, the study should be conducted up to the completion of the treatment.
These limitations are balanced by the study’s strengths: a robust split-mouth design, blinded outcome assessment, and complete datasets without protocol deviations. Future research should (a) employ more extensive studies that encompass the entire duration of orthodontic treatment with CBCT to quantify bone density changes and root movement patterns, (b) investigate en masse retraction protocols, (c) determine optimal injection intervals, (d) examine pain mechanisms associated with various platelet-rich injection protocols, and (e) conduct multi-center trials with oversampling to mitigate attrition. Such studies would validate these findings across broader populations and treatment durations.
Conclusions
The null hypothesis was rejected, and based on the research findings, it can be concluded that:
Both i-PRF and PRP were found to increase the rate of OTM. i-PRF is more effective in accelerating OTM than PRP. Pain during and after the procedure is minimal with both interventions. i-PRF can be used in routine orthodontic practice for increasing the rate of OTM.
Footnotes
Acknowledgments
The authors sincerely thank Dr. Amit Kumar, Dr. Vishal Sharma, Dr. Dhanasekaran, and Dr. Debarun for their valuable contributions, insights, and support during this study.
Author Contributions
AAM and SR have made substantial contributions to the conception and design of the work; AAM, SR, and AS have made contributions to the acquisition, analysis, and interpretation of data; AAM and SR have drafted the work and substantively revised it.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance (SBBDC/2020/152118-A dated 22.12.2020) was obtained from the ethical committee of Shree Bankey Bihari Dental College and Research Centre, Ghaziabad, Uttar Pradesh, India.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed Consent
Informed consent was obtained from the patients and parents.