
Abstract
Background
Precision Orthodontics (PO) is a revolutionary concept that incorporates genetics into orthodontic practice. While many medical fields have adopted new genomic technologies, dentistry, particularly orthodontics, has been slower to adapt. PO involves the utilization of customized equipment and precise force delivery, coupled with the integration of genetic and proteomic data, to enhance the individualization of orthodontic therapies. With the emergence of precision medicine in healthcare, understanding the adoption and perception of PO is crucial in shaping the future of orthodontic practice.
Objective
This cross-sectional study aimed to assess the current state of knowledge, awareness, and attitudes toward PO among orthodontists in India.
Methods
A questionnaire-based survey was developed which was distributed online to orthodontists across India. The survey comprised three sections focusing on knowledge, awareness, and attitudes related to PO. The survey received 391 responses, representing 41.2% of the orthodontists surveyed.
Results
While 72.3% of surveyed orthodontists demonstrated awareness of PO, only 32% correctly defined it, revealing a notable knowledge gap. Furthermore, 66% of the respondents admitted a lack of knowledge regarding genomic concepts. Despite these gaps, a remarkably positive attitude was observed among orthodontists, with 98% expressing openness to adopting precision approaches.
Conclusion
This study underscores the need for targeted education in genomics for orthodontists to bridge knowledge gaps. To facilitate the integration of PO into routine practice, specific education and training may be required. The positive attitudes and willingness to embrace PO indicate a promising trajectory for its adoption, potentially enhancing patient care and treatment outcomes.
Introduction
Precision medicine (PM) is an emerging approach for disease treatment and prevention, taking into account individual variability in genes, environment, and lifestyle. 1 This new paradigm in healthcare is a culmination of major technical and conceptual advances in genomics, pharmacogenomics, computational science, and bioinformatics. 2 Clinical decisions, practices, and interventions can now be tailored to the individual patient based on assessment of their risk of a disease or disorder and predicted response to treatment as revealed primarily from variations in their genome. National Institute of Health, USA launched the PM initiative to provide impetus to this new paradigm in healthcare. 3
PM is often used interchangeably with the term “personalized medicine,” which, at its core, implies a strong individual patient-centered approach. 4 “Precision medicine” is now often preferred over personalized medicine” as it addresses not only the unique needs of a single patient but also encompasses a wider goal of integrating genomic data toward a more molecularly based taxonomy of disease and its treatment.3-5
The backbone of PM is the rapidly expanding knowledge of the human genome providing a greater understanding of inherited and acquired diseases and disorders that are caused by subtle variations in the genome. Genetic variations affect not only the risk of and susceptibility to certain diseases and disorders but also could explain the variations in response to specific treatment approaches in individuals and groups. Examples of such conditions include cancers; certain infectious diseases (e.g., hepatitis C); neurological disorders (e.g., Alzheimer’s and Parkinson’s diseases); mental disorders (e.g., schizophrenia and bipolar disorder); and endocrine and metabolic disorders (e.g., diabetes and hypercholesteremia). 6 Although the focus is on genomic variation, precision healthcare includes a variety of “-omics,” for example, epigenomics, transcriptomics, proteomics, metabolomics, lipidomics, ionomics, as well as social determinants of health, and so forth, facilitated by advancing technology, increasingly large-scale databases, and bioinformatics.4, 7-9
Dental diseases usually are rarely associated with differential mortality as a primary outcome. Hence, dentistry has lagged behind medicine in the development and implementation of new genomic approaches, as well as transferring those approaches to clinical practice. Unlike many medical and dental fields, orthodontics has been traditionally data-intensive and technologically advanced, and hence, suitably placed to utilize advances in PM. Orthodontics and dentofacial orthopedics, as a specialty, have undergone an extensive reshaping by their collaboration and integration between different scientific fields and clinical disciplines. Thus, Precision Orthodontics (PO) will include not only customized appliances and force delivery to tissues but also the use of additional genomic and proteomic information for further customization of orthodontic diagnosis and treatments.
Emergence of PO
Craniofacial growth and form are determined by an interaction between genomic and epigenomic factors. Since the underlying principles of genetics affecting the growth of the craniofacial complex were poorly understood and could not be modulated, therefore, treatment of dentofacial deformities in the early 1980s was directed toward epigenetic factors, including orthodontic treatment itself, to influence the expression of the underlying genome. 10
It was predicted that “within the next several decades, orthodontists will be using molecular kits to diagnose growth-related problems for treatment of specific growth discrepancies.” 10 It was also proposed that “the personalized-genomic medicine approach can be used to determine individual key molecular mediators that could be targeted to modify facial growth and prevent or correct a developing dentofacial deformity.”10, 11
The term “personalized orthodontics” was first used by Hartsfield. 12 According to him, to truly understand how nature (genetic factors) and nurture (environmental factors, including treatment) together affect the treatment of patients, orthodontic researchers need to initiate the use of modern genomic methods, including large genome-wide association (GWA) studies linked with randomized clinical trials (RCTs) with appropriately stratified samples based on genomic profiles. At the beginning of the post-genomic/epigenomic period in orthodontics, a synthesis of the principles of genomics with epigenomics was proposed.6, 10
The beginning of the 21st century witnessed a surge in basic and clinical research into the application of genomic knowledge and PO in the development and growth of the craniofacial complex. 11 Instead of focusing primarily on craniofacial anomalies that are known to have a profound genetic basis, the contemporary focus is on the analysis of gene variants for growth factors and cytokines in an effort to improve the diagnosis and treatment of dental disorders and dentofacial deformities in orthodontic patients such as tooth development, Classes II and III malocclusion, tooth movement and dental crowding.10, 11
For the translation of personalized and precision approaches in the field of orthodontics into daily practice, more research is warranted into the current awareness levels, limitations, possibilities, and challenges posed as well as reforms in healthcare systems and policies in general and in orthodontics particularly. The yields from these efforts will benefit from the emergence of novel technologies like Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR), gene, cell and protein therapies, digital imaging, personalized medicine, and regenerative dental therapies. Therefore, it is critical that orthodontists understand the basics of these novel technologies that are currently used in other medical fields and that they become familiar with the fundamental concepts of providing individualized approaches to assess patients with skeletal deformities and/or malocclusions.
Many studies in the literature discuss the impact of PM in dentistry.13-20 However, few researchers have studied PO. Jheon et al. highlight the emerging field of PO, which utilizes advances in computer technologies and biomedicine to achieve customized treatment approaches and enhance treatment efficiencies. 21 They discuss the current and likely future applications of computer hardware and software, 3D imaging technologies, and 3D printing in orthodontics, particularly in the fabrication of customized appliances such as aligners and retainers. The article also emphasizes the importance of biomedical research in understanding cartilage growth and bone biology, which can potentially be applied to modify mandibular growth and modulate tooth movement in orthodontic treatment. Additionally, the integration of genomic and proteomic information is highlighted as a means to further customize orthodontic diagnosis and treatments.
We did not find any study assessing the knowledge, perception, and attitude of orthodontists toward PO, even though many studies have assessed the attitude and knowledge levels of medical practitioners, medical students, and the general public toward PM. The aim of this study was to assess the knowledge, awareness, and attitude toward PO among orthodontists in India.
Materials and Methods
Study Site and Sample Size Calculation
A cross-sectional study was designed using a questionnaire-based survey to assess the knowledge, attitude, and awareness of PO among orthodontists in India. The study was evaluated by the Institutional Review Board (IRB) with reference no. ACDS/IRB/01/Jan 2022. All orthodontists in India were eligible for inclusion in the study. The sample size required for statistical significance was calculated to be 384, assuming a 95% confidence interval with a 5% margin of error. The population of interest (orthodontists) was taken into account using the Indian Orthodontic Society Directory (2023), and sample size was determined using the following calculation:
where Z = 1.96 for a 95% confidence level, p = 0.5, which maximizes variability and provides the most conservative estimate of the required sample size, and e = 0.05, representing the desired margin of error.
Survey Tool and Recruitment of Participants
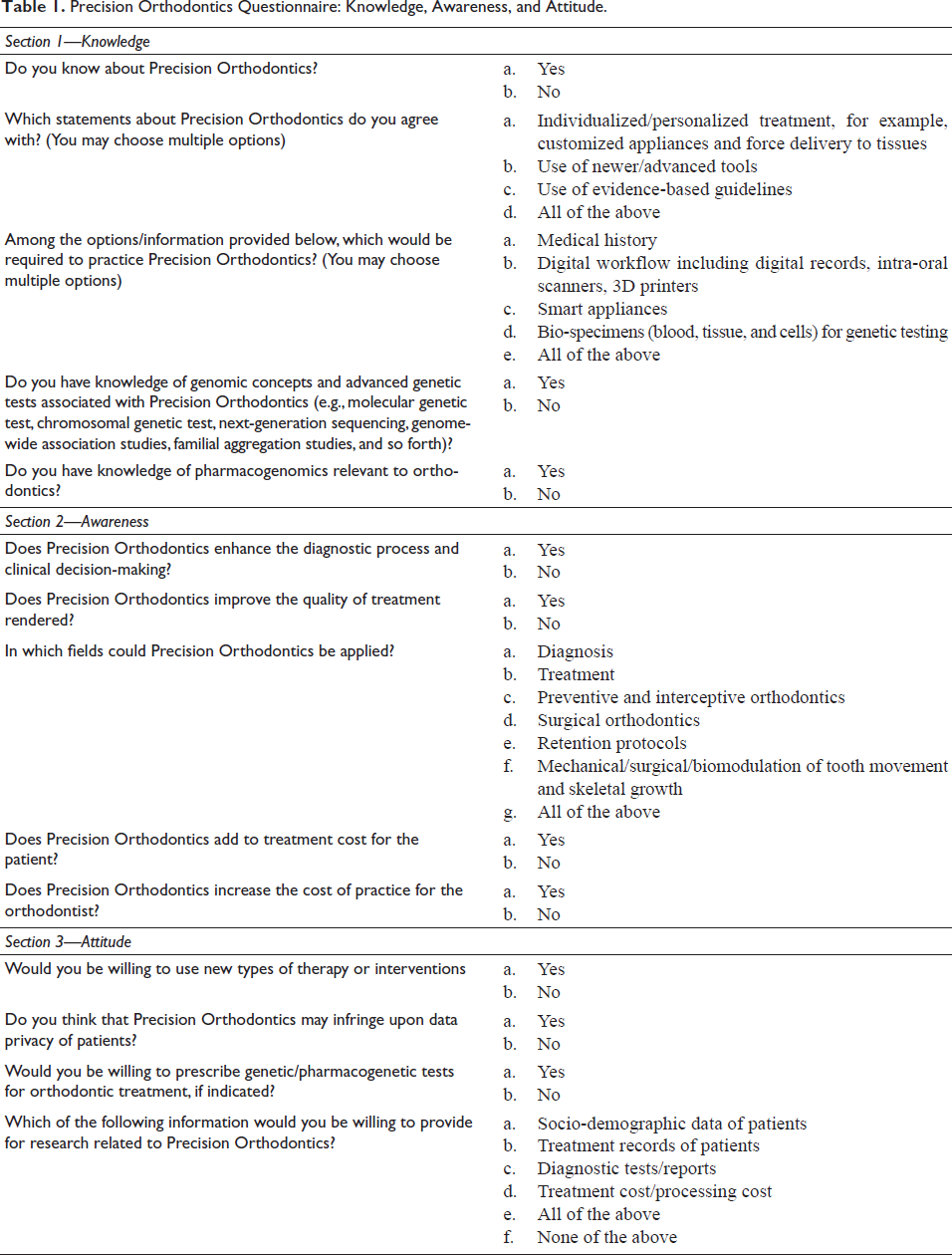
The questionnaire (Table 1) was divided into three sections: section 1 contained five questions to gauge the practitioners’ knowledge of PO; section 2 contained five questions to assess awareness about PO, and four questions in section 3 determined attitude toward the practice of PO, its applications, limitations, and ethical considerations. The questionnaire was reviewed by three senior orthodontists with more than 10 years of clinical and academic experience. Feedback was obtained regarding the relevance, clarity, and completeness of the questions. Prior to its distribution, the survey tool was piloted on 10 orthodontists to assess the validity and time required to understand, interpret, and fill responses to the questions. These individuals were later excluded from the study. Participants were able to answer all questions in the survey tool within a reasonable time and their responses were determined to be suitable for analysis.
Precision Orthodontics Questionnaire: Knowledge, Awareness, and Attitude.
Inter- and intra-rater reliability of the questionnaire was evaluated using a subset of 20 participants who completed the survey twice within a 2-week interval. The intra-class correlation coefficient (ICC) for reliability was calculated, yielding an inter-rater reliability of 0.89 and an intra-rater reliability of 0.92, indicating excellent agreement. Based on participant feedback, the survey format was modified (correcting language and grammar mistakes, summarizing and shortening long questions, and omitting some questions because of repetition). Participation was voluntary, and no prior information on the topic was provided to them.
An online survey was conducted from April 2022 to September 2022 using Google Forms. The link was circulated randomly through social media platforms, in groups where orthodontists across India had participated. Hence, the online link was shared via social media platforms to 950 orthodontists for participation. No personal data were collected and the decision to participate in the survey was completely voluntary. Data gathered were tabulated and subjected to statistical analysis.
Statistical Analysis
Data were presented in mean or percentage where appropriate. Descriptive analysis was used to present the results.
Results
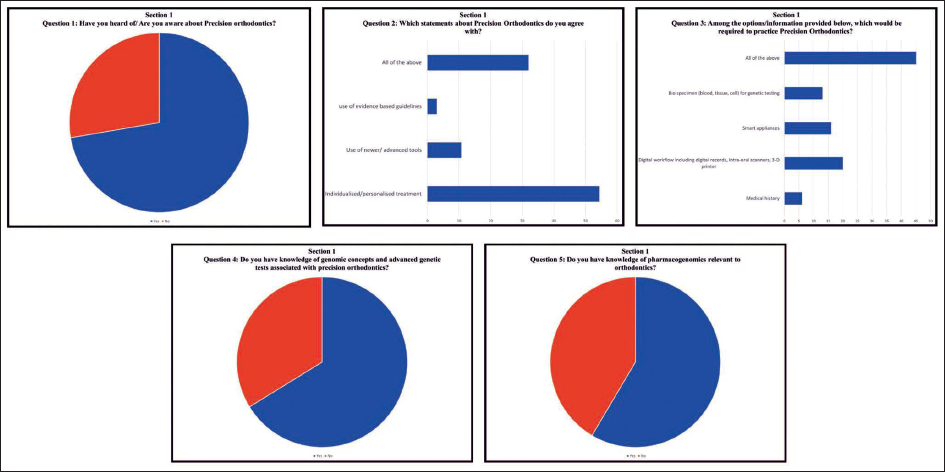
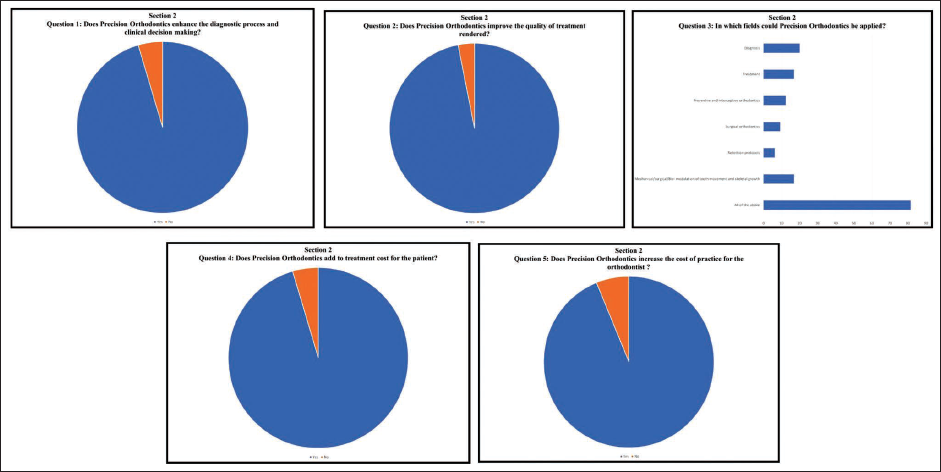
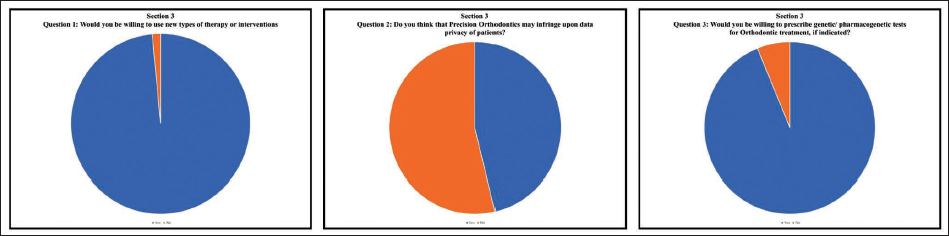
Three hundred and ninety-one orthodontists out of 950 (41.2%) responded to the survey. The results are discussed in three sections as follows: Knowledge of PO (Figure 1): Nearly three-fourths of the surveyed orthodontists (72.3%) answered in the affirmative when asked if they knew about PO. However, when asked for the meaning of the term PO, 54.3% of participants understood it to be limited to individualized or customized orthodontic appliances. 10.7% of respondents believed it to refer to newer advances in tools/technology, and 3% chose the practice of orthodontics based on evidence-based guidelines. Only 32% of participants correctly identified the definition/meaning of PO. On the question of diagnostic aids required for practicing PO, 45% agreed to the diverse gamut of investigations that may be performed. In contrast, 29% of the participants responded by selecting only bio-specimens or smart appliances. 66% of participants acknowledged their lack of knowledge of genomic concepts and advanced genetic tests associated with PO (e.g., molecular genetic test, chromosomal genetic test, next-generation sequencing, genome-wide association studies, familial aggregation studies, and so forth) even as 58.5% responded as having knowledge of pharmacogenomics relevant to orthodontics (local delivery of proteins/drugs). 2. Awareness of PO (Figure 2): 95.4% and 96.9% of participants, respectively, believe that PO enhanced the diagnostic process and clinical decision-making and improved the quality of treatment rendered. 81.5% of respondents believe that PO encompassed all sub-fields of orthodontics, such as diagnosis, prevention, interception, treatment, retention, as well as mechanical/surgical/biomodulation of tooth movement and skeletal growth. Nearly all orthodontists agreed that PO may add to treatment costs for the patient (95.4%) as well as increase the cost of practice for the orthodontist (93.1%). 3. Attitude toward PO (Figure 3): An astounding 98% of orthodontists exhibited a positive attitude toward PO and were willing to use newer types of therapy or interventions (e.g., customized/smart appliance, pharmacogenetic modulation of tooth movement) and were also willing to prescribe genetic/pharmacogenetic tests for orthodontic treatment, if indicated (93.8%). Majority of them (53.8%) did not believe that the use of PO would infringe upon the data privacy of patients. 47.7% of orthodontists were willing to share all the practice-related data, while 15.4% were unwilling to provide any practice-related data for research related to PO.
Responses of Section 1 of the Questionnaire—Knowledge of Precision Orthodontics.
Responses of Section 2 of the Questionnaire—Awareness of Precision Orthodontics.
Responses of Section 3 of the Questionnaire—Attitude Toward Precision Orthodontics.
Discussion
The practice of medicine is undergoing a rapid transformation, becoming increasingly technology-driven and technology-enabled. Genomics and PM are at the forefront of these changes, requiring future doctors to be proficient in using these newer tools as part of their everyday clinical work. Personalized orthodontics combines genomics, bioinformatics, and digital technology and aims to tailor orthodontic treatment to individual patients based on their genomic evidence and clinical data. This approach seeks to anticipate the susceptibility to malocclusions in patients and execute treatment plans with precision. The primary goal is to reduce diagnostic errors, enhance treatment outcomes, and minimize unnecessary side effects.
Given the reliance of orthodontic specialties on appliances and forces for tooth movement and craniofacial orthopedics, precision approaches are expected to significantly transform this field by synthesizing genomic and clinical data. The results of this cross-sectional survey shed light on the knowledge, awareness, and attitude of orthodontists in India toward PO to bridge the gap between research in this field and its practical implementation. The discussion section is divided into three parts to analyze these findings in detail.
Knowledge of PO
The survey revealed a notable gap in the understanding of what PO entails among the surveyed orthodontists. While a substantial proportion (72.3%) indicated that they were aware of the term “Precision Orthodontics,” the understanding of its precise meaning was limited. Only 32 participants correctly identified the definition of PO, with many respondents mistaking it for customized orthodontic appliances, advances in tools/technology, or evidence-based orthodontic practice. The diverse opinions on diagnostic aids for practicing PO, ranging from a broad acceptance of various investigations to the preference for bio-specimens or smart appliances by some, underscore the varied levels of familiarity and engagement within the orthodontic community regarding PO.
The findings are similar to a study by Addis et al. wherein about half of the respondents stated that they were not sufficiently informed about PM even though most respondents agreed with the basic principles and definitions of PM. 22 Similarly, Bipin et al. conducted a descriptive cross-sectional survey on PM among dental students using a self-administered questionnaire. Even though 61% of the dental students surveyed were aware of PM, they were not well aware of the role of PM in the medical field. 20 In an online survey of rheumatologists and fellows to assess the expectations and educational needs for PM in Canada, Ruel-Gagne found that, while physicians recognize the potential benefits of PM tests, they feel their training is insufficient to incorporate them into clinical practice. 23
Further, in this study, a significant number of orthodontists (66%) admitted to lacking knowledge of genomic concepts and advanced genetic tests relevant to PO. This knowledge gap in genomic concepts, such as molecular genetic tests and next-generation sequencing, suggests the need for additional education and training in these emerging areas within orthodontics. A similar lack of knowledge of pharmacogenomics in PM can be seen across literature. Kamp et al. explored practicing clinicians’ perceptions of PM-based cardiovascular disease risk stratification in South Africa’s public health setting. 24 Fewer than 25% of respondents used clinical genetic testing, and only 14% had formal genetics training. Bunjo et al. also reported that a majority of medical students expressed discomfort with knowledge regarding PM concepts, such as basic genomic testing concepts and terminology, pharmacogenomics, and “Big data collection tools.” 25
Tsuji et al. conducted a nationwide survey of Japanese pharmacists regarding the application of pharmacogenomic testing in PM. Majority of respondents recognized the potential role of germline pharmacogenomic testing in determining individual drug responses, but only 26% of pharmacists, were involved in pharmacogenomic testing and only 12.4% of pharmacists had received specific pharmacogenomic-related education. 26
These consistent findings across disciplines highlight that the barriers to implementing precision approaches are not unique to orthodontics and call for a systemic strategy to improve genomic literacy. The knowledge gaps identified in this study highlight the need for tailored educational initiatives to prepare orthodontists for the future demands of PO, paralleling efforts in other healthcare domains.
Awareness of PO
The survey results indicated a high level of awareness about the potential benefits of PO among participating orthodontists. The overwhelming majority believed that PO enhanced the diagnostic process (95.4%) and clinical decision-making (96.9%). Additionally, most respondents perceived PO as having a positive impact on the quality of orthodontic treatment (96.9%).
Orthodontists in this study recognized the broad scope of PO, with 81.5% acknowledging its potential in all sub-fields of orthodontics, including diagnosis, prevention, interception, treatment, retention, as well as mechanical, surgical, and biomodulation of tooth movement and skeletal growth. However, there was a consensus that PO might lead to increased treatment costs for both patients (95.4%) and orthodontists (93.1%). However, physicians and the general public surveyed by Kichko et al. did not share the same concerns over the cost of PM. The costs for PM were expected to be covered by health insurance and governmental funds. 27 In contrast, lack of insurance coverage for pharmacogenetic testing was identified as a major barrier to its clinical implementation by 81% of pharmacists surveyed by Tsuji. 26
Attitude Toward PO
The most striking finding of this survey was the overwhelmingly positive attitude of orthodontists toward PO. An impressive 98% of participants exhibited a positive attitude and expressed their willingness to adopt new types of therapy or interventions associated with PO, such as customized/smart appliances and pharmacogenetic modulation of tooth movement. These results are comparable to those of Kamp et al., where 84% of clinicians perceived PM approaches positively despite limited knowledge and resources. 24 A majority of physicians (93.8%) were also open to prescribing genetic and pharmacogenetic tests when indicated, demonstrating a commitment to tailoring treatment to individual patient needs. These results are consistent with Cho et al., who reported that health professionals in Korea showed positive attitudes toward PM, with about 95-96% of respondents agreeing that it would be effective in treatment and precise diagnosis. 28 In a study by Bunjo et al., almost three-quarters of students indicated that they would be willing to adopt PM even if senior physicians around them were not doing so. 25 Similarly, in Kamp et al.’s study, approximately two-thirds of clinicians positively identified themselves as the primary players in traditional patient-facing activities related to PM-based cardiovascular disease risk stratification, such as referring patients for testing, sharing results, and using results to guide prevention and treatment approaches. 24 The results of this study are also consistent with those of Erdmann et al. who reported that many patients and professionals have a positive attitude toward PM, expecting high benefits from it. 29
Data privacy concerns were voiced by some of the orthodontists in this study, with 46.2% believing that using PO might infringe upon patient data privacy. In contrast, Kichko et al. surveyed physicians on awareness, acceptance, use, and opinions on PM aspects in Pennsylvania (US) and Bavaria (Germany). Both states expressed strong concerns about genetic privacy protection and did not support a unified genetic database. 27
A larger portion of orthodontists responding in this study (47.7%) expressed a willingness to share practice-related data for research related to PO, while 15.4% were reluctant to provide such information. In comparison, Cho et al. reported that 69.9% of health professionals in their study were willing to participate as study subjects in PM research. 28
While the positive attitudes toward PO are encouraging, barriers to its adoption remain. A quantitative survey was conducted by Schroll et al. across five stakeholders, including medical oncologists, surgeons, lab directors, payers, and patients, to understand the perceived barriers to PM utilization in the United States. The survey revealed that stakeholders find PM testing challenging primarily due to a lack of education and awareness among healthcare professionals, payers, and patients. However, stakeholders expressed optimism that the barriers to PM adoption will decrease in the future with better alignment on the challenges to PM, education, awareness of reimbursement, and patient support. 30
Other reported risks and challenges to adopting precision approaches in medicine and dentistry include lack of evidence for the accuracy of tests and efficacy of treatments, limited patient knowledge affecting informed consent, potential unavailability of access to PM for underprivileged individuals and ethnic minorities, high cost, limited access to genetics services, misuse of data by insurance companies and employers, racial stigmatization due to genetic information, unwanted communication of incidental findings, changes in doctor–patient relationship, and pressure on patients to optimize their health.24, 28, 29 These concerns emphasize the need for robust ethical frameworks, equitable access to precision care, and enhanced efforts to educate both healthcare professionals and the public about PO and PM.
Future Recommendations
Future studies should focus on understanding the genetic basis of orthodontic conditions and treatment outcomes through etiological factors and response to treatment factors.4, 12, 14 Clinicians will need to develop an “individualized diagnostic eye” considering individual patient variables and their biological and psycho-social backgrounds in order to develop a better understanding of patient characteristics, potentially including genome analysis. 31 Genetic knowledge can enhance the differential diagnosis and lead to novel therapeutic modalities for malocclusion in orthodontics. 32 It acknowledges the long-standing recognition of the significance of genetics in malocclusion, which has been a topic of debate and controversy for centuries. 32
Collaborative efforts and a consortium approach are needed for future genetic studies, as well as the establishment of standards and improvement of technologies in orthodontics. The growing knowledge about bone biology can lead to more effective treatment approaches.33, 34 Increased awareness of current and emerging technologies can improve personalized and precision approaches in orthodontics. National legislation and guidelines are necessary to address the risks and ensure justice in access to PM. 29 Improvements in patient education, data security, communication guidelines, and cost-effectiveness should also be considered. Innovative approaches to orthodontic curriculum are needed to prepare future orthodontists for precision-based orthodontic treatment. Interprofessional education and collaborative care should be facilitated through the development of new competencies. 16
Strengths of this Study
The study focuses on PO, an important emerging field due to advances in genomics and personalized medicine. The study has a substantial sample size of 391 respondents (41.2%), representing Indian orthodontists from different regions of India, providing diverse perspectives on PO. The study objectively assesses knowledge, awareness, and attitudes toward PO offering a comprehensive understanding with quantitative data that allows for identification of trends and relationships. The results provide valuable insights about PO in India, highlighting the need for education and training in genomics and PM among orthodontists in India. The study serves as a baseline for future research on knowledge, awareness, and attitudes in PO.
Limitations of the Study
There are many limitations of this study. Online surveys are inherently limited by potential sample bias and restricted reach, as participation depends on accessibility and willingness. Additionally, the response rate of 41.2% raises concerns about nonresponse bias, where the views of nonrespondents may differ from respondents, potentially influencing the representativeness of the findings. Self-reported data may be influenced by social desirability bias and memory inaccuracies, affecting the accuracy of the information provided. This survey did not explore the reasons behind the responses, limiting the insights gained on knowledge, awareness, and attitudes toward PO. The results of this study may not be applicable to orthodontists in other regions with different healthcare systems and access to information. The wording of the survey questions could have influenced participant responses, impacting the validity of the findings. A cross-sectional design captures data at a single point in time, limiting insights into changes in knowledge, awareness, and attitudes over time. The study did not consider social and cultural factors that may influence the attitudes of orthodontists in India toward PO. The overwhelmingly positive attitudes reported by participants may be influenced by desirability bias, potentially overestimating support for precision approaches.
Conclusion
In summary, this study revealed that while a significant number of orthodontists in India are aware of the concept of PO, there is room for improvement in their understanding of its specific components, particularly in the domain of genomics and advanced genetic testing. Nevertheless, the overwhelmingly positive attitude toward and willingness to adopt PO suggests a promising future for the integration of precision approaches in orthodontic practice, with the potential to enhance patient care and outcomes.
Further education and training initiatives can help bridge the knowledge gaps and ensure that orthodontists are well-prepared to embrace the opportunities presented by PO.
Footnotes
Acknowledgment
Not applicable.
Author’s Contributions
Gyanda Mishra: Conceptualization, data curation, and writing—original draft manuscript. Shubhnita Verma: Methodology and data curation. Pradeep Raj G: Investigation, visualization, writing—review and editing, and supervision. Jangam Sowmya: Data collection and data verification. Prasad Chitra: Supervision, final editing, and revision. The final manuscript has been seen and approved by all the authors, and they have taken due care to ensure the integrity of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was evaluated by the Institutional Review Board (IRB) with reference no. ACDS/IRB/01/Jan 2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.