
Abstract
Extractions or grossly damaged teeth without prosthetic rehabilitation can lead to the supraeruption of their opposing teeth in many clinical situations. These, if allowed to persist, may cause occlusal disturbances and complicate the placement of any dental restorations. These clinical situations are frequently managed with a combination of endodontic treatment, surgical intrusion, or even extractions. This article discusses the biomechanics and clinical procedures for intruding the maxillary molars using temporary anchorage devices (TADs). It also details the advantages, disadvantages, and case studies involving the use of two TADs (infrazygomatic miniscrews and palatal miniscrews) to intrude one or two maxillary molars. Following the intrusion of the maxillary molars, restoration can be completed on the mandibular molars using a crown on the implant or an overlay of the lower molar.
Introduction
When mandibular molars are missing or have a broken crown, the maxillary molars can overerupt, which can lead to several clinical problems, such as occlusal interferences, periodontal issues, and mesial inclination of the mandibular second molar. 1 However, the intrusion of an overerupted maxillary molar using traditional orthodontic treatment is a real challenge, and this must be done carefully to ensure that the desired movement is achieved without any significant movement across the rest of the dentition. 2 Some options for replacing the mandibular molars are occlusal reduction of the opposing tooth, aligners, intrusion using appliances or miniscrews, or continuous archwire mechanics. 3 In such cases, orthodontics is mostly an adjunctive option, with the emphasis of the treatment being the correction of the position of the supraerupted teeth. 4 Care must be taken to achieve the desired movement without significant iatrogenic effects across the dentition. 5
Biomechanics of Maxillary Intrusion
When using orthodontic appliances, it is essential to consider biomechanics. The biomechanics approach is crucial for maxillary molar intrusion and must be designed before the treatment. 6 If we intend to intrude only one of the first or second molars, we need to design and apply force through the center of resistance (CR) of that specific molar. If we plan to intrude both the first and second molars simultaneously, the force must be applied through the CR of the group (first and second molars). This is especially important when using temporary anchorage devices (TADs) (Figure 1).
(A) Biomechanics of Single Tooth Intrusion. (B) Biomechanics of Double Teeth Intrusion. (C) Biomechanics of Single Tooth Intrusion using Two Miniscrews and Two Power Chains. (D) Biomechanics of Single Tooth Intrusion using Two Miniscrews and One Power Chain.
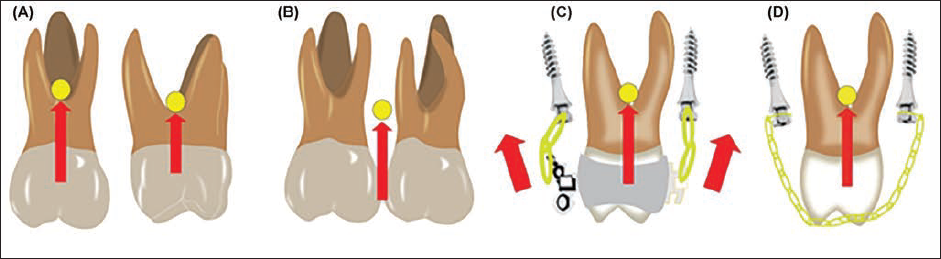
Checking the CR of a single tooth is a relatively simple procedure, as its CR is usually located at the center of the tooth and facilitates intrusion. However, determining the CR for a group of teeth is a more complex matter, as multiple factors influence it. For example, the precise location of the CR cannot be predicted with certainty in the first and second molars. Factors such as root length, root quantity, and bone density all play a role in determining the CR. Ideally, the force applied during treatment should be directed through the CR (as shown in Figure 1A and B) to achieve pure intrusion without causing any side effects. However, in practice, it is necessary to carefully monitor and control the biomechanics of the treatment to ensure optimal results. However, it is difficult to check the CR of the tooth and more difficult for the group of teeth because it is affected by multifactor. Ideally, the CR of one tooth is in the center of the tooth, but it is complicated to predict the CR for a group comprising the first and second molars. It depends on the root length of two teeth, the quantity of the root, and the density of the bone. The force must be through the CR, like in Figure 1, for pure intrusion and no side effects, but in clinical, we must check and control the biomechanics during the treatment. In the clinical, we use two TADs to achieve the force through the CR by using one labial and one lingual miniscrew in the maxillary (Figure 1C). 7 We usually use an infrazygomatic miniscrew for the buccal side and a palatal miniscrew for the lingual side. In addition, we must apply the power chain from both miniscrews, and it should exert pressure through the CR or by using two power chains in buccal and lingual (as shown in Figure 1C). It can be challenging to regulate the force of both sides, but it can prove effective if we want to control the buccal or lingual inclination (Figure 1D).
Protocol
A specific protocol can be utilized to carry out adjunctive molar intrusion. This involves the placement of two miniscrews, one each on the labial and the palatal sides. For the buccal side, there is the use of an infrazygomatic screw, and for the palatal side, we use an inter-radicular miniscrew. For intrusive purposes, there are three methods for carrying out the desired tooth movement: Using power chains directly across the occlusal surface, which are stabilized using orthodontic composite to minimize any chances of slippage of the chain.
7
Using buttons bonded on the labial and palatal surfaces and placing power chains from the buttons to the miniscrews. A wire segment across the occlusal surfaces of the molars is used to achieve intrusion of the molars together, if there are no alignment problems.
For intrusion of the molars, the force levels range between 100 and 200 g for a single tooth and 200–400 g if we aim to achieve segmental intrusion. 8 The intrusion rate for the molars is approximately 0.5 mm per month, which allows us to calculate the period required for intrusion. 8
Case Series
Case 1
Diagnosis and Etiology
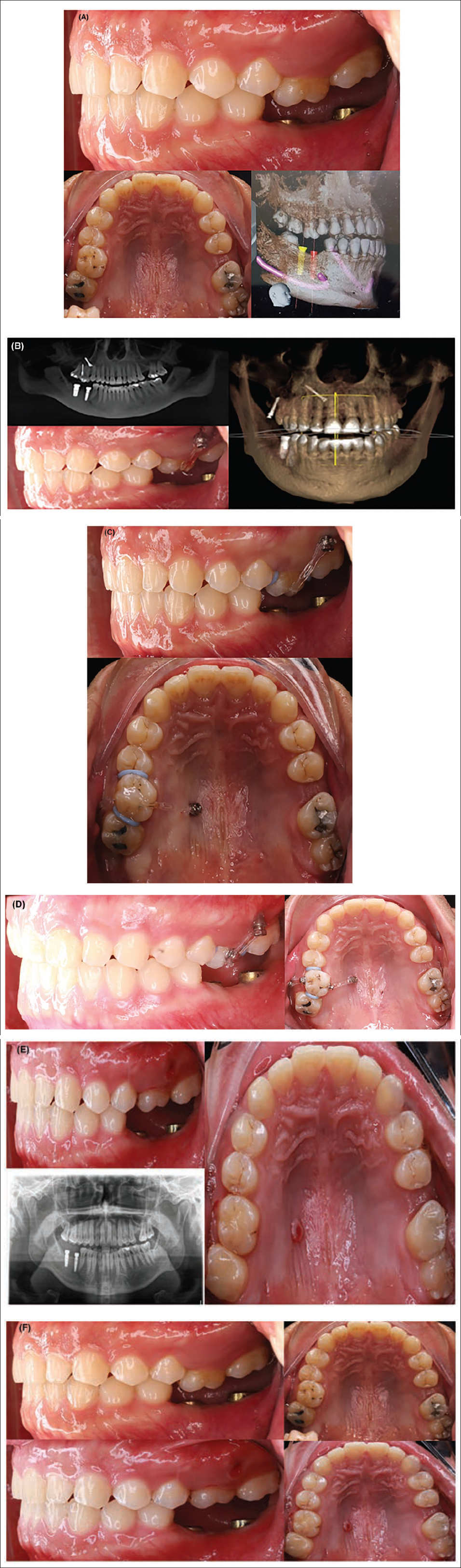
A 26-year-old patient was referred to our dental clinic by another implantologist to have tooth 16 repositioned to its normal position in the upper arch. Upon clinical examination, it was found that tooth 16 was 4 mm higher than its normal position due to missing teeth 46 and 47. Additionally, another clinic installed two implants in the mandibular region. To assess the position of tooth 16 in 3 dimensions, cone beam computed tomography (CBCT) X-rays were taken (as shown in Figure 2A).
(A) Pretreatment Intraoral Pictures and Cone Beam Computed Tomography (CBCT) X-ray (First Case). (B) First Day Treatment (First Case). (C) After 1 Month (First Case). (D) After 2 Months (First Case). (E) The Result with Intraoral Pictures and X-ray after 4 Months (First Case). (F) Pretreatment and Post-treatment Intraoral Pictures (First Case).
Treatment Objectives and Treatment Plan
Intrude 16 to normal position using two TADs (one buccal and one lingual) without side effects and complications.
Treatment Progress
On the first day of treatment, two miniscrews were placed in the buccal and palatal alveolar bone. A power chain was then put through the center of the occlusal surface of tooth 16, which was fixed with composite, and separators were used to create space for intruding tooth 16 (Figure 2B).
After 1 month, the buccal alveolar bone screw failed, so we replaced it with infrazygomatic miniscrews that followed the same biomechanical principles. However, after 2 months, we needed to control the buccolingual dimension, so we bonded two buttons on the buccal and lingual sides. We then used a power chain on both sides, applying greater force on the buccal side. We continued this biomechanical approach for 6 months until the intrusion was complete (Figure 2C–E).
Treatment Result
The result was satisfactory, and the patient returned to the implantologist to complete the crown on the implant. After the intrusion, we used a thermoforming aligner with a 1 mm thickness for the retainer (Figure 2F).
Case 2
Diagnosis and Etiology
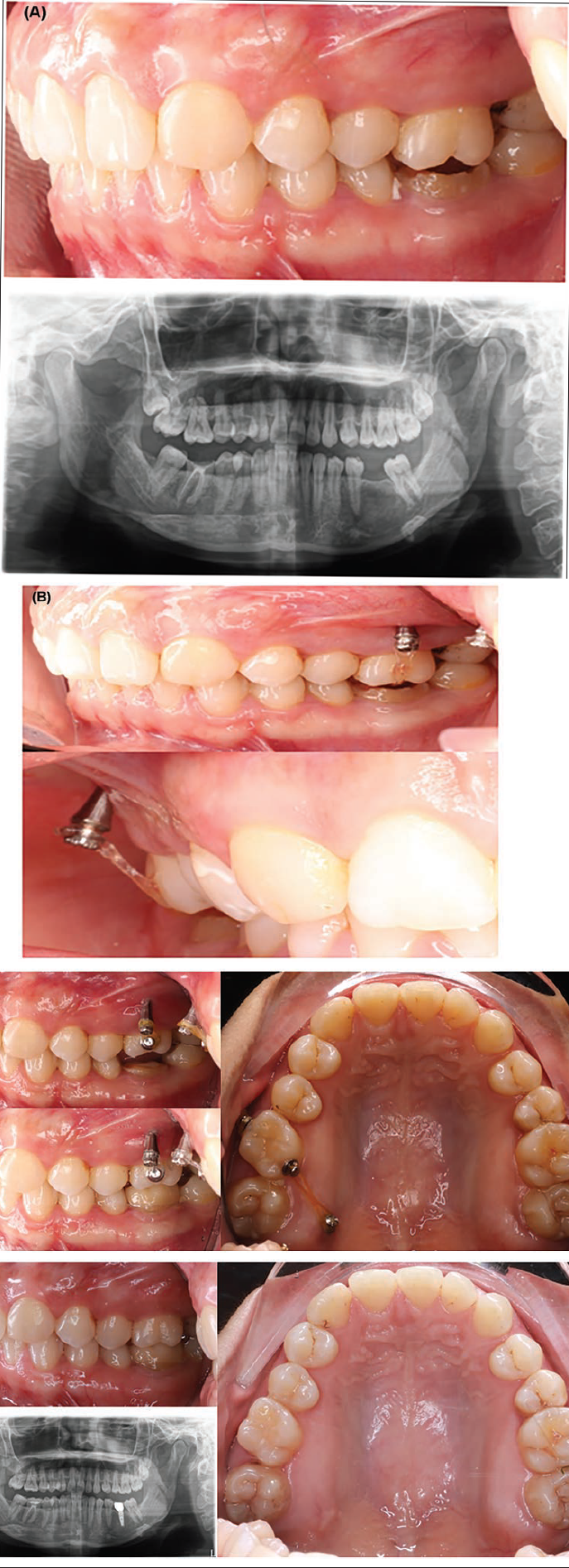
A 28-year-old dental assistant working in our clinic had a chief complaint of a broken crown on tooth 46, an extrusion of 16, and a missing tooth 36. After a clinical examination, it was discovered that tooth 16 was 4 mm higher than its normal position due to a broken tooth 46. A panoramic X-ray was taken to check the extent of the problem (Figure 3A).
(A) Pretreatment Records (Second Case). (B) First Day of Treatment (Second Case). (C) After 4 Months of Treatment (Second Case). (D) The Result after Intrusion, Overlay of 46, and Implant and Crown 36 (Second Case).
Treatment Objectives and Treatment Plan
The treatment objective was to intrude tooth 16 into its normal position using two TADs without any side effects or complications. Additionally, an overlay was planned for tooth 46, and an implant and crown for tooth 36.
Treatment Progress
The treatment progress involved the insertion of two miniscrews into the infrazygomatic crest and the palatal on the first day of treatment. A power chain was then put through the center of the occlusal surface of tooth 16, which was fixed with composite, and separators were used to create space for the intruding tooth.
After 2 months, two buttons were bonded on the lingual and buccal sides, and the exact mechanics continued (Figure 3B and C).
Treatment Results
Finally, after 4 months of treatment, the overlay of tooth 46 and restoration on tooth 36 were done, resulting in good and stable occlusion (Figure 3D).
Case 3
Diagnosis and Etiology
A 50-year-old patient reported to the clinic with the primary concern of having unaesthetic teeth and missing teeth. During a clinical examination, we discovered a problematic crown and bridge in the upper teeth and unaesthetic upper and lower teeth, as well as missing teeth in positions 36, 46, and 47. We took CBCT X-rays to assess the problems and evaluate the quality of the bone in the positions where the teeth were missing.
Treatment Objectives and Treatment Plan
We have created a treatment plan for aesthetic restoration on the upper and lower arch, focusing on teeth 16–25 and 35–45. Before proceeding with the crown and implant combination restoration on 36, 46, and 47, we need to intrude tooth 16. However, we want to minimize the invasiveness of the treatment, so we will avoid performing a root canal on tooth 16 (Figure 4A).
(A) Pretreatment Records (Third Case). (B) After Upper and Lower Aesthetic Restoration and Biomechanics in First Day of 16 Tooth Intrusion (Third Case). (C) After 6 Months of Intrusion. Implant Installation (Third Case). (D) After 1 Year, Result of Intrusion (Third Case). (E) Result of All Treatment (Third Case).
Treatment Progress
In the first stage, we perform cosmetic restoration on both the upper and lower jaw. In the second stage, once the restoration is complete, we plan to intrude tooth 16 using two miniscrews. During the intrusion process, we will also install three implants in positions 36, 46, and 47. We will follow the biomechanics of molar intrusion for this case, but we may need to adjust the force application point, as the position of the buccal miniscrews was not ideal. To do so, we will use a 0.019 × 0.025 stainless steel wire through the hole of the buccal miniscrew. In the third and final stage, after 1 year of intrusion, we will place the crown on tooth 16 and the three implants (Figure 4B–D).
Treatment Results
All objectives were achieved with minimally invasive treatment, resulting in aesthetic and functional occlusion for the patient (Figure 4E).
Case 4
Diagnosis and Etiology
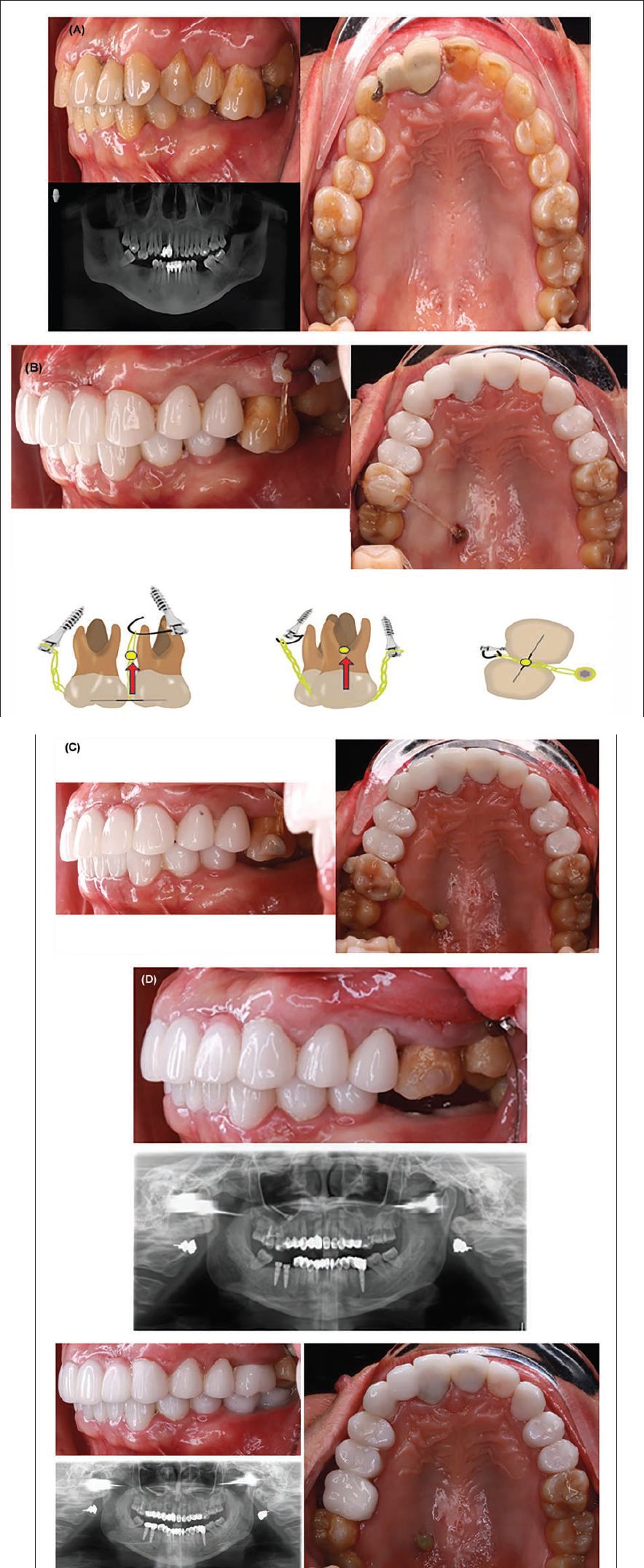
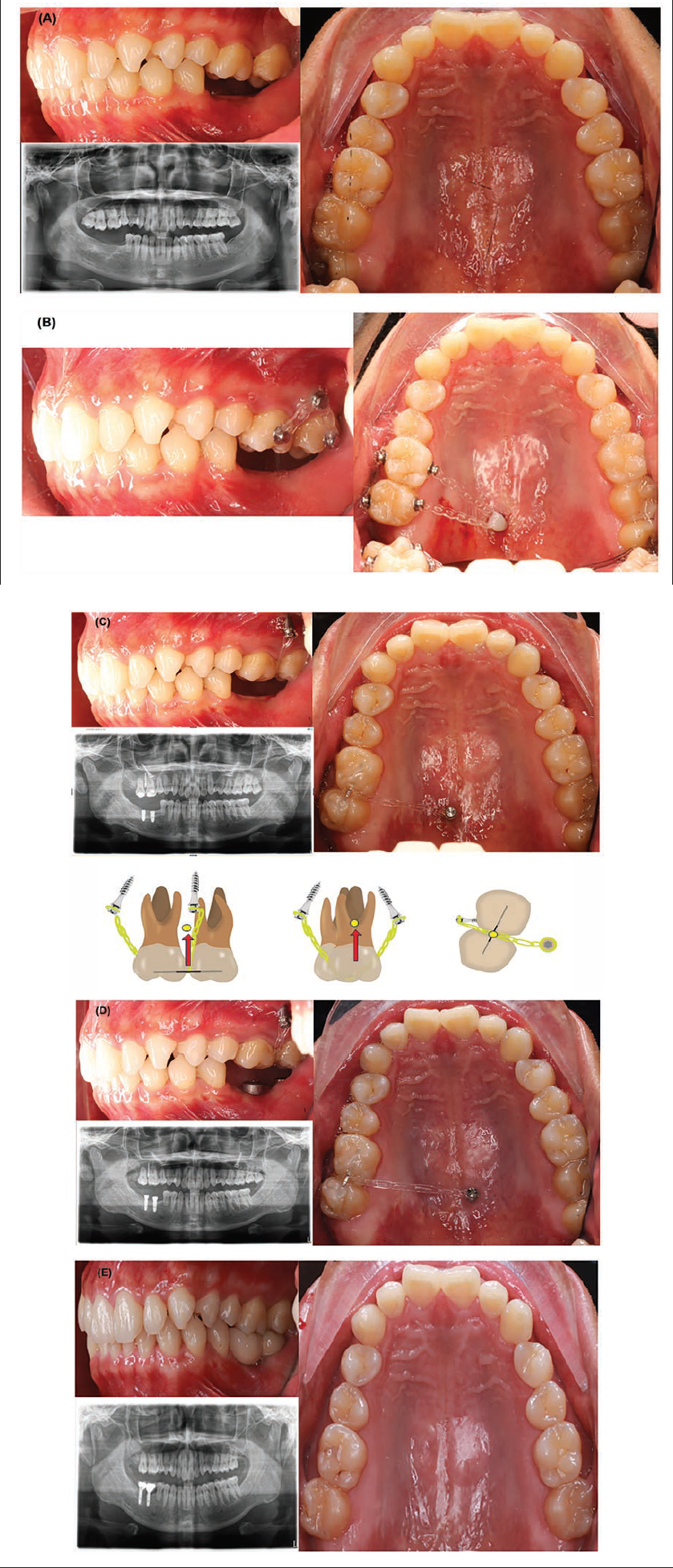
A 30-year-old patient was referred to our dental hospital by another implantologist to have teeth 16 and 17 repositioned to their normal position in the upper arch. Upon clinical examination, it was found that teeth 16 and 17 were 4 mm higher than their normal position due to missing teeth 46 and 47. Additionally, another clinic installed two implants in the mandibular region. Panoramic X-ray was taken to check the position of 16 and 17 (Figure 5A).
(A) Pretreatment Records (Fourth Case). (B) Biomechanics of First Day of Treatment (Fourth Case). (C) Second Suitable Biomechanics (Fourth Case). (D) Result of Intrusion Treatment after 8 Months (Fourth Case). (E) Result with Crowns on 46 and 47 (Fourth Case).
Treatment Objectives and Treatment Plan
Intrude 16 and 17 to the normal position using two TADs (one buccal and one lingual) without side effects and complications and extract 18.
Treatment Progress
On the first day of treatment, 18 was extracted, and two miniscrews (infrazygomatic and palatal) were installed. Additionally, four buttons were bonded on the buccal and lingual surfaces. After 1 month, it was observed that the biomechanics were not optimal, so suitable changes were made. A 0.019 × 0.025 stainless steel wire segment was bonded on the occlusal surfaces of tooth numbers 16 and 17, and a power chain was used through the center of the wire, which bonded the two teeth together. Due to the sinus, it was necessary to intrude the two teeth through the sinus, which means the treatment may take longer than expected. During the treatment, the buccal and palatal miniscrews failed and had to be reinstalled into the infrazygomatic miniscrew and another palatal position (Figure 5B–D).
Treatment Results
After 8 months of treatment, the intrusion phase was completed, and the patient returned to the implantologist to have the crowns made for teeth 46 and 47. A retention device was used on the upper teeth with a 1 mm thermoforming aligner (Figure 5E).
Discussion
Severely overerupted molars or entire posterior segments can be difficult for dentists. In such cases, a combination of treatments from a prosthodontist, an implantologist, and an orthodontist may be necessary. Different clinical approaches can be taken, which include the correction of the overerupted teeth, surgical disimpaction, or extractions. Orthodontically planned intrusion of the overerupted teeth or segments can provide a more conservative option to manage such problems. However, fixed orthodontic treatment is not always feasible due to the intense anchorage demands in the vertical dimension, which can lead to the undesirable extrusion of the anchor teeth.
The biomechanics approach is a valuable method for molar intrusion treatment but requires a customized design for each case. Predicting the CR accurately is impossible, so regular clinical checkups are necessary. Additionally, we cannot control certain factors in a clinical setting, such as miniscrew failure or poor positioning due to bone quality or anatomy. Therefore, it is essential to be flexible and use auxiliary methods to achieve the desired biomechanics design. Biomechanics approach is beneficial for molar intrusion treatment, but we must design individually for each case. However, we cannot precisely predict the CR, so checking in clinic every month is always necessary. Besides, in the clinical approach, we cannot control something like the failure of miniscrews; the position is not good because of bone quality and anatomy, so we must be flexible with some auxiliary to achieve our biomechanics design. Using TADs such as miniscrews or miniplates offers a more predictable solution with minimal side effects. This technique brings about intrusion in a specific area, which is particularly beneficial as many adult patients are unwilling to undergo fixed orthodontic treatment. Single overerupted teeth have been successfully treated with the help of miniscrews used alone or in combination with fixed appliances. In some instances, corticotomy might enhance the intrusive action of the appliance.
In the current orthodontic scenario, many options and techniques are available to carry out precise tooth movements.9–11 We can use these methods to carry out comprehensive orthodontic therapy and provide the patient with adjunctive treatment when required. Based on the results from these cases, we observed that it is possible to intrude the molars through the sinus with minimal root resorption 12 or achieve more than 4 mm molar intrusion. However, this process requires time and light force suggestions.13, 14 In some cases, multidisciplinary treatment combining orthodontics, implant, and prosthodontics is necessary to achieve stable results in dentistry. 15
Conclusion
Based on the findings of this case series, it is evident that maxillary molar intrusion can be achieved using TADs and power chains. However, the mechanics and treatment plan should be designed based on the individual case. Orthodontists must carefully plan and place the miniscrews, followed by delivering the right amount and direction of forces to achieve the desired level of intrusion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the patient to use their clinical and radiographic records for academic and research purposes.