
Abstract
Aim
The main aim of the study was to evaluate tooth position in plaster models of nonorthodontic subjects that have optimal occlusion, using the American Board of Orthodontics (ABO) criteria and comparing it to ABO standards.
Methods
Forty nonorthodontic subjects with optimal occlusion were evaluated for teeth positioning with ABO measurement criteria, using the ABO gauge. These measurements were compared to the ABO standards. On the panoramic radiographs of these subjects, distances between the roots of teeth were measured using the digital ruler in Quick CephR. Lateral cephalograms were scanned and digitized into Quick CephR systems to evaluate the skeletal anteroposterior and vertical relationship. Means and standard deviations were calculated for all the variables and compared to ABO standards. Correlations were obtained between attrition and overjet. Correlations were also studied between anteroposterior skeletal relation, vertical skeletal relation, and teeth positioning. In subjects that had accurate age records, the relationship between age and change in buccolingual inclination was evaluated.
Results
A significant difference in the mean values for inclination of maxillary and mandibular first bicuspids, second bicuspids, first molars, and second molars as compared to the board criteria was observed. Accuracy of panoramic radiograph to measure root proximity, especially in the cuspid region, is questionable. There was a positive correlation between overjet at the cuspid region and attrition. There was a minimal correlation between age and buccolingual inclination of teeth, indicating only a trend for mandibular second bicuspid to upright with age.
Conclusion
The ABO criteria and standards used to evaluate finished orthodontic cases are consistent with naturally occurring optimal dentitions, except for buccolingual inclination of posterior teeth in both maxillary and mandibular arches.
Keywords
Introduction
In 1972, Lawrence F. Andrews ushered in a new age in orthodontics. His bellwether study of 120 casts of nonorthodontic patients with normal occlusion gave rise to what was to become the now celebrated “six keys to normal occlusion.” In the 40 odd years that have passed since, orthodontic graduates from all corners of the world have been using Dr Andrews’ guidelines to establish a benchmark to assess the quality of a finished orthodontic case.
The American Board of Orthodontics (ABO) in 1998 introduced the ABO objective grading system to score dental casts and panoramic radiographs. Eight cardinal criteria were employed in this new grading system. The board then suggested that clinicians use these criteria to evaluate cases on an ongoing basis in their practices.
Although there have been numerous studies involving the ABO gradation system,1–9 there has been no published data on the systematic evaluation of subjects with optimal occlusion termed “Non-Orthodontic Optimal occlusion” by Dr Andrews, utilizing ABO criteria and standards.
Therefore, this study was undertaken to evaluate four objectives. The first main objective was evaluating tooth position in plaster models of nonorthodontic subjects that have optimal occlusion, using ABO criteria, and comparing it to ABO standards. The second was to evaluate if, in these subjects, there is any correlation between tooth position and the skeletal relationship. The third objective was to examine tooth wear and evaluate if there is any correlation between tooth position and tooth wear. The fourth objective was also to evaluate if, in these subjects, the buccolingual inclination of teeth changed with age.
Materials and Methods
This retrospective study was approved by the IRB of Ragas College.
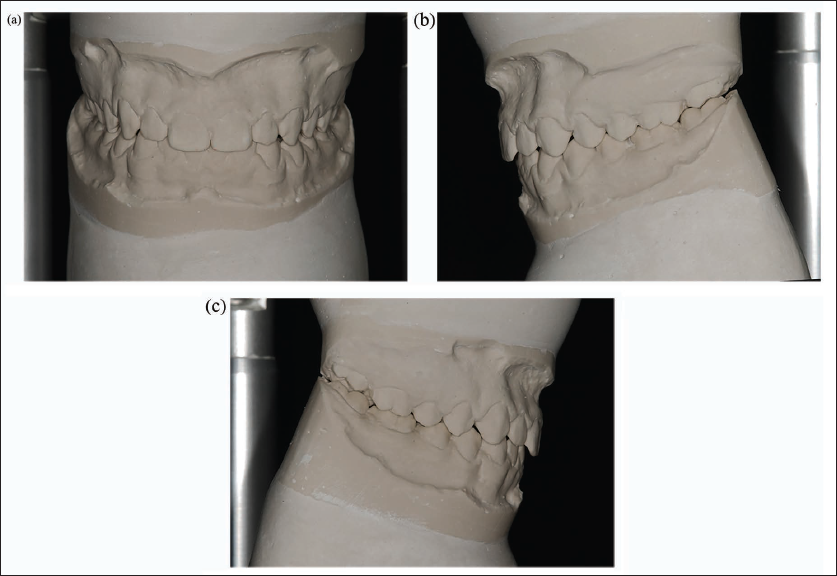
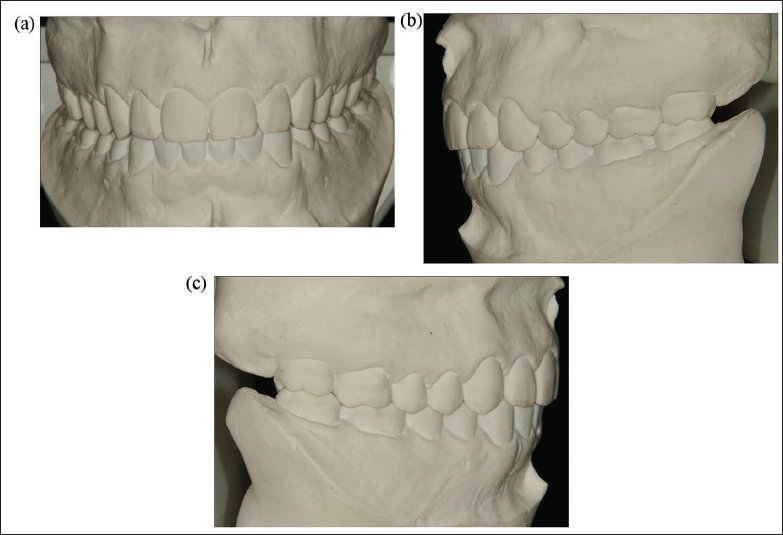
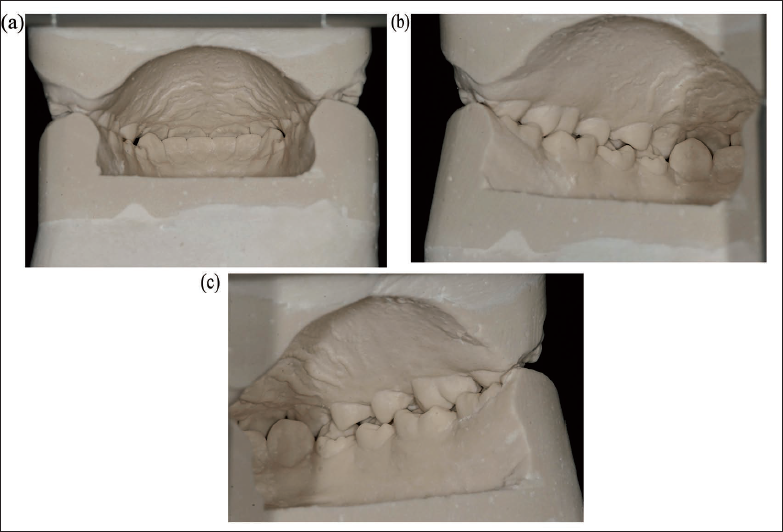
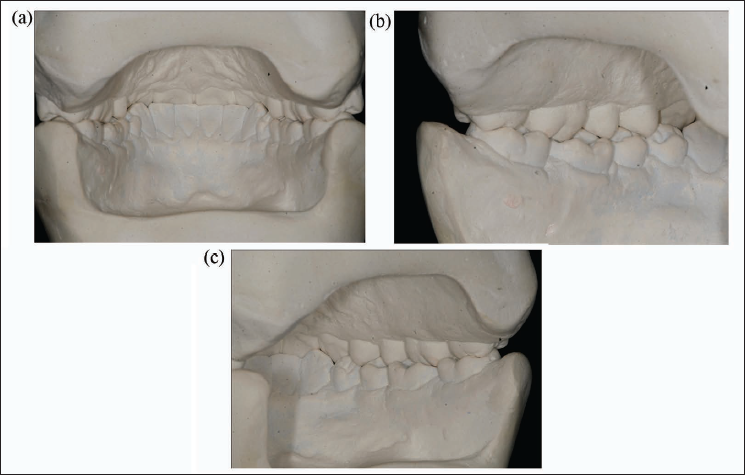
Forty nonorthodontic subjects were selected from the archives at the Dr Lawrence F. Andrews Foundation. To avoid bias, Dr Andrews selected the cases not knowing the scope and objectives of the study. The samples selected had good interdigitation among the cuspids, bicuspids, and molars on the buccal aspect (Figures 1a, b, and c and 2a, b, and c) and good contact of second bicuspids, first and second molars, with the opposing arch on the lingual aspect (Figures 3a, b, and c and 4a, b, and c). The molar relation was Angle’s Class I in all 40 subjects.
(a) Photographs Illustrating Frontal View of Sample Nonorthodontic Optimal Subject Age 13 Years. (b) Photographs Illustrating Left Buccal View of Sample Nonorthodontic Optimal Subject Age 13 Years. (c) Photographs Illustrating Right Buccal View of Sample Nonorthodontic Optimal Subject Age 13 Years.
(a) Photographs Illustrating Frontal View of Sample Nonorthodontic Optimal Subject Age 41 Years. (b) Photographs Illustrating Left Buccal View of Sample Nonorthodontic Optimal Subject Age 41 Years. (c) Photographs Illustrating Right Buccal View of Sample Nonorthodontic Optimal Subject Age 41 Years.
(a) Photographs Illustrating Straight Lingual View of Sample Nonorthodontic Optimal Subject Age 13 Years. (b) Photographs Illustrating Left Lingual View of Sample Nonorthodontic Optimal Subject Age 13 Years. (c) Photographs Illustrating Right Lingual View of Sample Nonorthodontic Optimal Subject Age 13 Years.
(a) Photographs Illustrating Straight Lingual View of Sample Nonorthodontic Optimal Subject Age 41 Years. (b) Photographs Illustrating Left Lingual View of Sample Nonorthodontic Optimal Subject Age 41 Years. (c) Photographs Illustrating Right Lingual View of Sample Nonorthodontic Optimal Subject Age 41 Years.
Other criteria Dr Andrews used for selection included minimal tooth irregularity of less than 1 mm, spacing of less than 1 mm, and mild attrition; as evaluated from the dental casts were allowed in the study (Figures 5a and b and 6a and b). Only 17 of the 40 subjects studied had panoramic films. In these subjects, that had panoramic films, overall tooth angulations as assessed from panoramic radiographs appeared to be good (Figure 7a and b). Only 21 of 40 subjects had accurate age records. In these subjects that had accurate age records (ages ranging from 12.2 to 48 years), relationship with age and change in buccolingual inclination was evaluated.
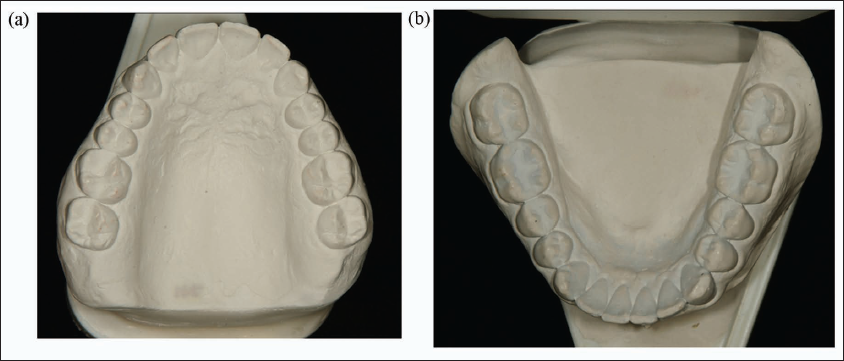
(a) Photographs Illustrating Maxillary Occlusal View of Sample Nonorthodontic Optimal Subject Age 13 Years. (b) Photographs Illustrating Mandibular Occlusal View of Sample Nonorthodontic Optimal Subject Age 13 years.
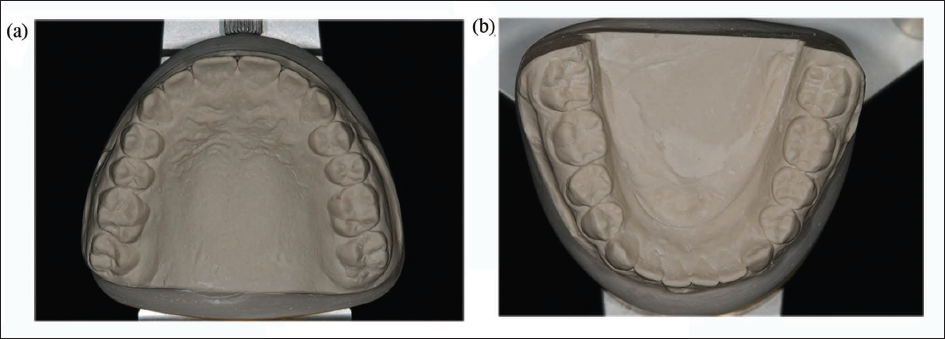
(a) Photographs Illustrating Maxillary Occlusal View of Sample Nonorthodontic Optimal Subject Age 41 Years. (b) Photographs Illustrating Mandibular Occlusal View of Sample Nonorthodontic Optimal Subject Age 41 Years.
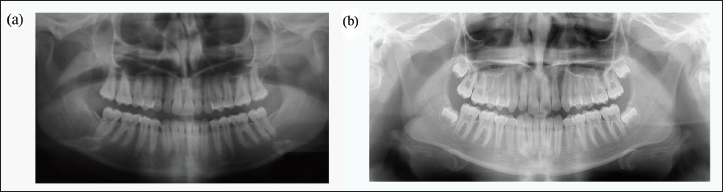
(a) Sample Panoramic Radiograph of Nonorthodontic Optimal Subject 41 Years. (b) Sample Panoramic Radiograph of Nonorthodontic Optimal Subject 12.2 Years.
Measurements
Two separate observers were standardized using the ABO standardization kit for measurements (American Board of Orthodontics Standardization Kit, July 1998). All the measurements were made on the dental casts using the ABO gauge. 10 After standardization, measurements were made by both the observers on 15 cases, and measurements were subjected to Pearson correlation test to determine inter and intraobserver reliability.
Individual tooth angulations were evaluated for 17 of the 40 subjects that had panoramic radiographs. Panoramic radiographs of these subjects were scanned at 144 dpi and measurements were made at the midroot section between teeth utilizing the digital ruler provided in QuickCephR (QuickCephR System, Diego, CA). Measurements were made by two examiners and the measurements were averaged.
From 30 of the 40 subjects that had lateral cephalograms, skeletal relationship in anteroposterior and vertical planes were obtained from measurements made on images scanned at 144 dpi and digitized using the QuickCephR System (QuickCephR System, Diego, CA). Two observers digitized the cephalograms “on the screen” and utilizing the magnification tool, accurate landmark selection was ascertained. Computer generated values of the two observers for horizontal measurements (SNA, SNB, calculated ANB, and distance N-perpendicular–Frankfort to the “A” point) and vertical measurements (FMA, posterior to anterior facial height ratio, and posterior cranial base to ramus height ratio) were then averaged.
The variables evaluated were as follows:
– Marginal ridge discrepancy in both maxillary/mandibular arches. – Tooth inclination of maxillary/mandibular bicuspids and molars. – Lingual contact of maxillary first bicuspid with teeth in the mandibular arch. – Overjet for both anterior and posterior teeth measured as the horizontal distance of the maxillary teeth from the mandibular teeth. – Overbite measured the vertical overlap of the maxillary incisors over the mandibular incisors. – In 17 of the 40 subjects, distance between the roots of all the maxillary and mandibular teeth was measured on the panoramic radiograph utilizing the digital ruler in QuickCephR System (QuickCephR System, Diego, CA). – The presence of attrition and its location as to the anterior/posterior segment were recorded. – In 30 of the 40 subjects that had lateral cephalograms, skeletal anteroposterior relationship (SNA, SNB, ANB, and distance N-perpendicular–Frankfort to the “A” point) was measured from the lateral cephalogram. – Vertical relationship (FMA, posterior to anterior facial height ratio, and posterior cranial base to ramus height ratio) was measured from the lateral cephalogram. – In 22 of 40 subjects that had accurate age records (ages ranging from 12.2 to 48 years), relationship with age and change in buccolingual inclination was evaluated.
Statistics
Inter and intraobserver agreements for model measurements were found to be significant (r = 0.80 and r = 0.88, respectively). No systematic bias was seen between observers.
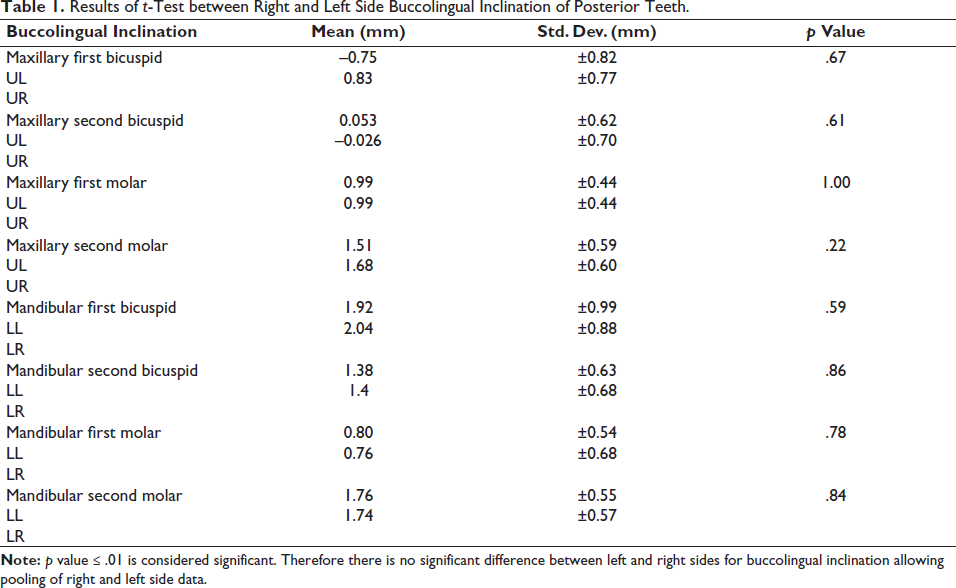
Statistical analysis for all measurements (models, cephalometric, and panoramic radiographic) indicated a normal data distribution. Student t-tests were used to analyze the differences in teeth inclination and angulation between the right and left sides of the maxillary and mandibular arches. No significant differences were present in these two comparisons; therefore, the right and left side measurements were pooled (Table 1).
Results of t-Test between Right and Left Side Buccolingual Inclination of Posterior Teeth.
Correlations between attrition and dental variables, listed above, were assessed using Pearson correlations for numerical measures. Chi-squared test was used for categorical data.
The correlations between buccolingual inclination of teeth in the buccal segment, as measured on models, and anteroposterior/vertical skeletal measurements, as made on cephalograms, were assessed using Pearson correlations and chi-square test. The correlations between buccolingual inclination and age were also assessed using Pearson correlation and chi-square test.
Results
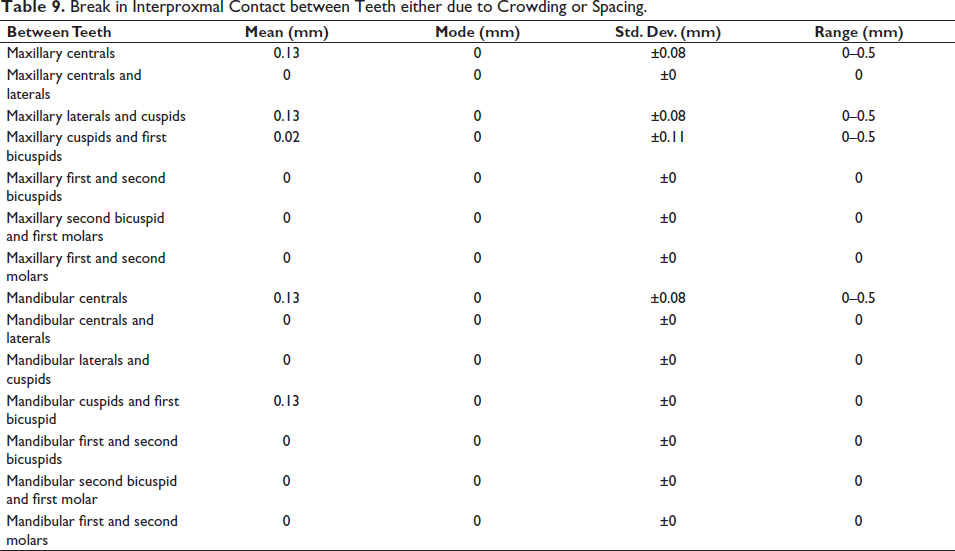
Mean, mode, standard deviation, and range for all variables studied that were compared to ABO standards are presented in Tables 2–10.
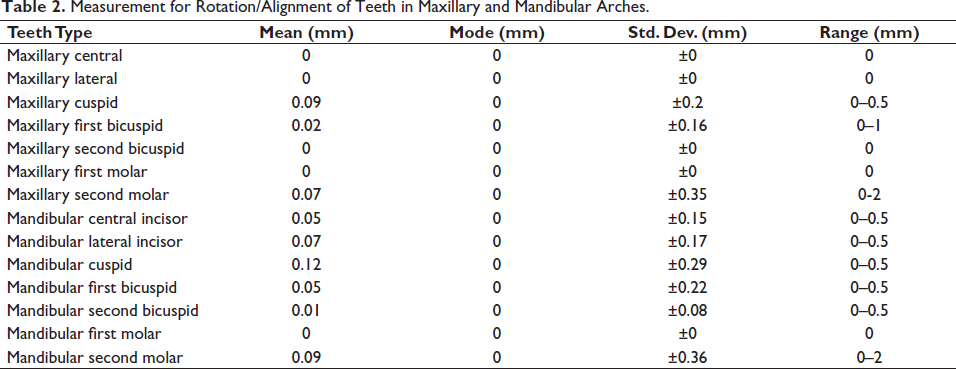
Measurement for Rotation/Alignment of Teeth in Maxillary and Mandibular Arches.
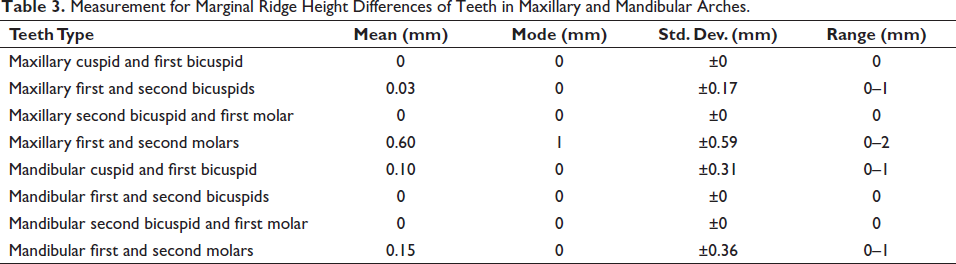
Measurement for Marginal Ridge Height Differences of Teeth in Maxillary and Mandibular Arches.
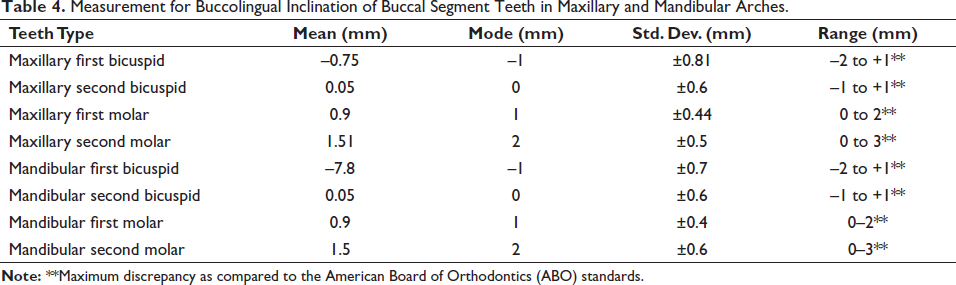
Measurement for Buccolingual Inclination of Buccal Segment Teeth in Maxillary and Mandibular Arches.
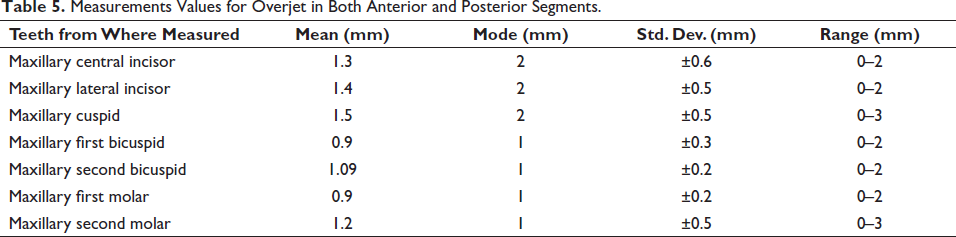
Measurements Values for Overjet in Both Anterior and Posterior Segments.
Measurement for Overbite and Curve of Spee.

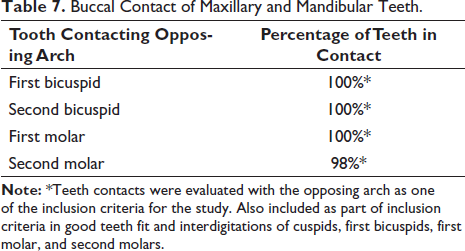
Buccal Contact of Maxillary and Mandibular Teeth.
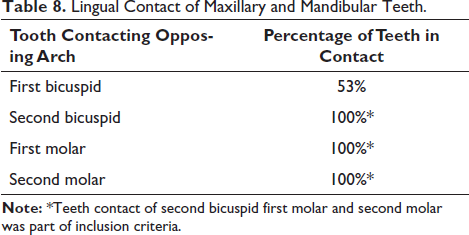
Lingual Contact of Maxillary and Mandibular Teeth.
Break in Interproxmal Contact between Teeth either due to Crowding or Spacing.
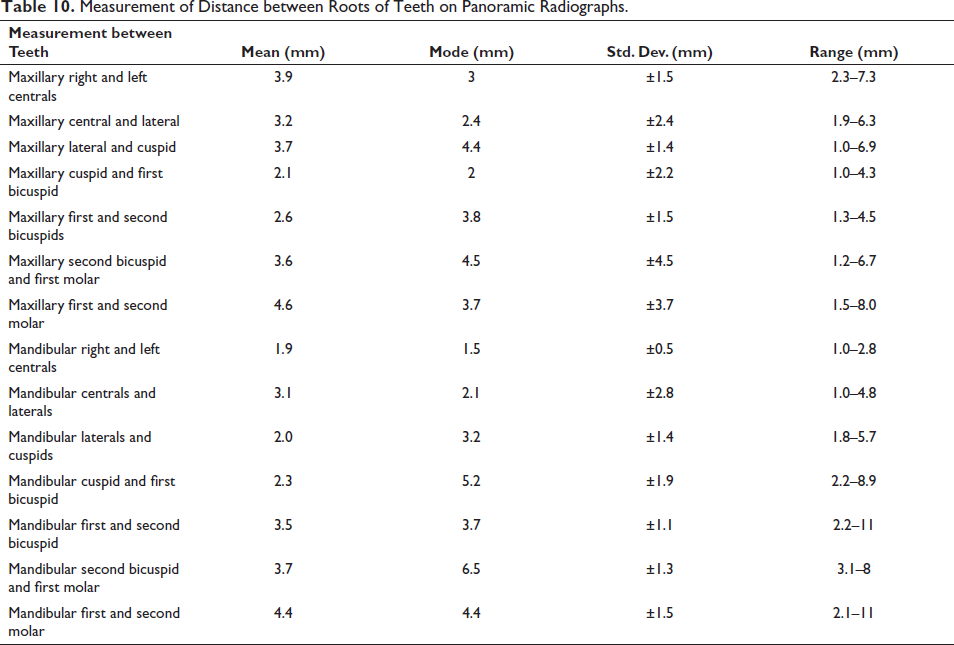
Measurement of Distance between Roots of Teeth on Panoramic Radiographs.
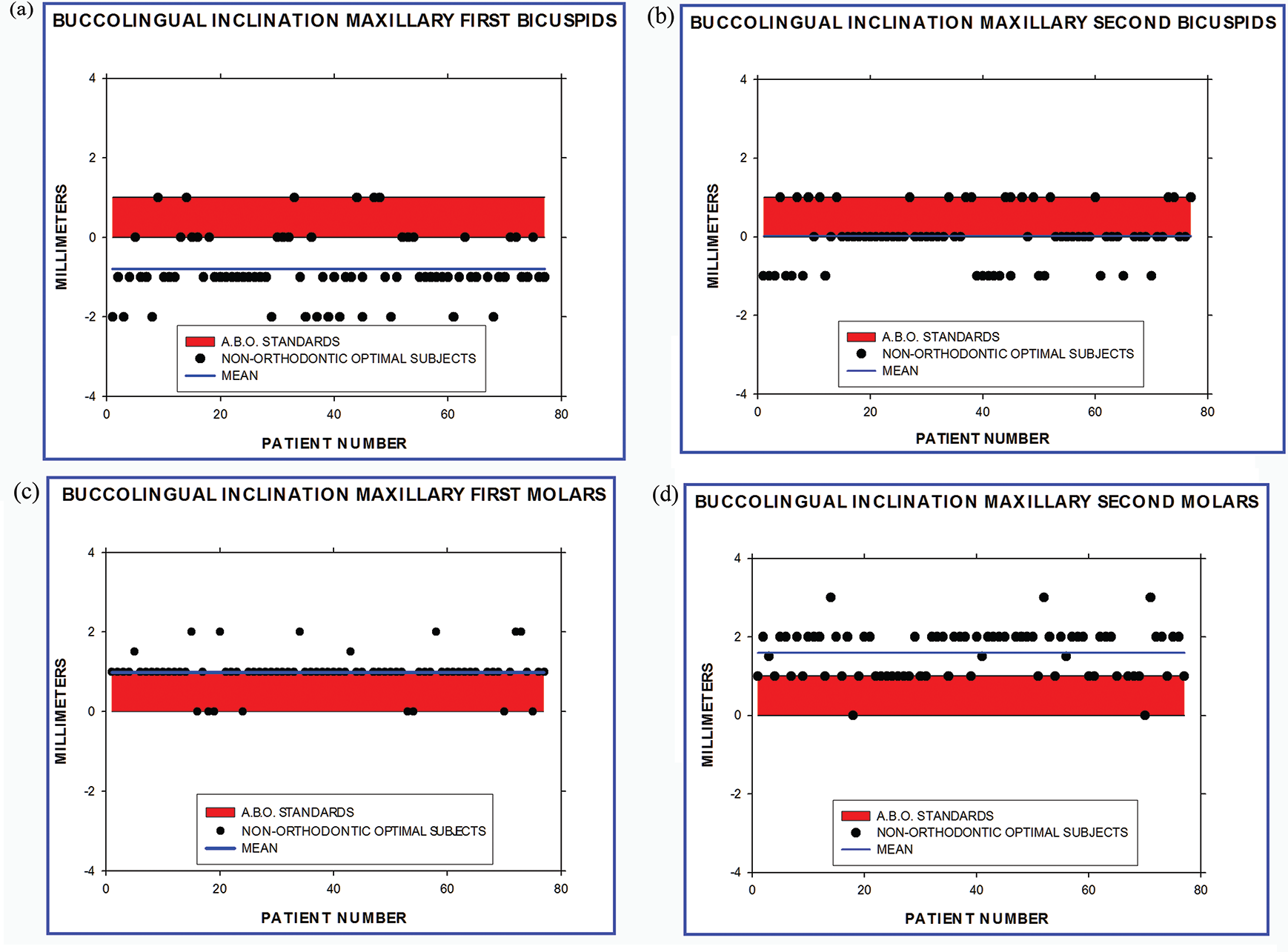
In the maxillary arch, the mean observed data on the buccolingual inclination of the maxillary first bicuspids, second bicuspids, first molars, and second molars as illustrated in Table 4 are consistently different from the prescribed ABO standards (Figure 8a, b, c, and d). Mean value for buccolingual inclination for maxillary first bicuspid was –0.75 ± 0.81 mm, mode was –1 mm, and the values ranged from –2 to +1 mm. Suggested ABO values for maxillary first bicuspid ranged from 0 to 1 mm. The mean value for maxillary second bicuspid was 0.05 ± 0.6 mm, mode was 0 mm, and the values ranged from –1 to +1 mm. Suggested ABO values of maxillary second bicuspid ranged from 0 to 1 mm. Mean value for maxillary first molar was 0.9 ± 0.44 mm, mode was 1 mm, and the values ranged from 0 to 2 mm. Suggested ABO values for maxillary first molar ranged from 0 to 1 mm. Mean value for maxillary second molar was 1.5 ± 0.5 mm, mode was 2 mm, and the values ranged from 0 to 3 mm. Suggested ABO values for maxillary second molar ranged from 0 to 1mm.
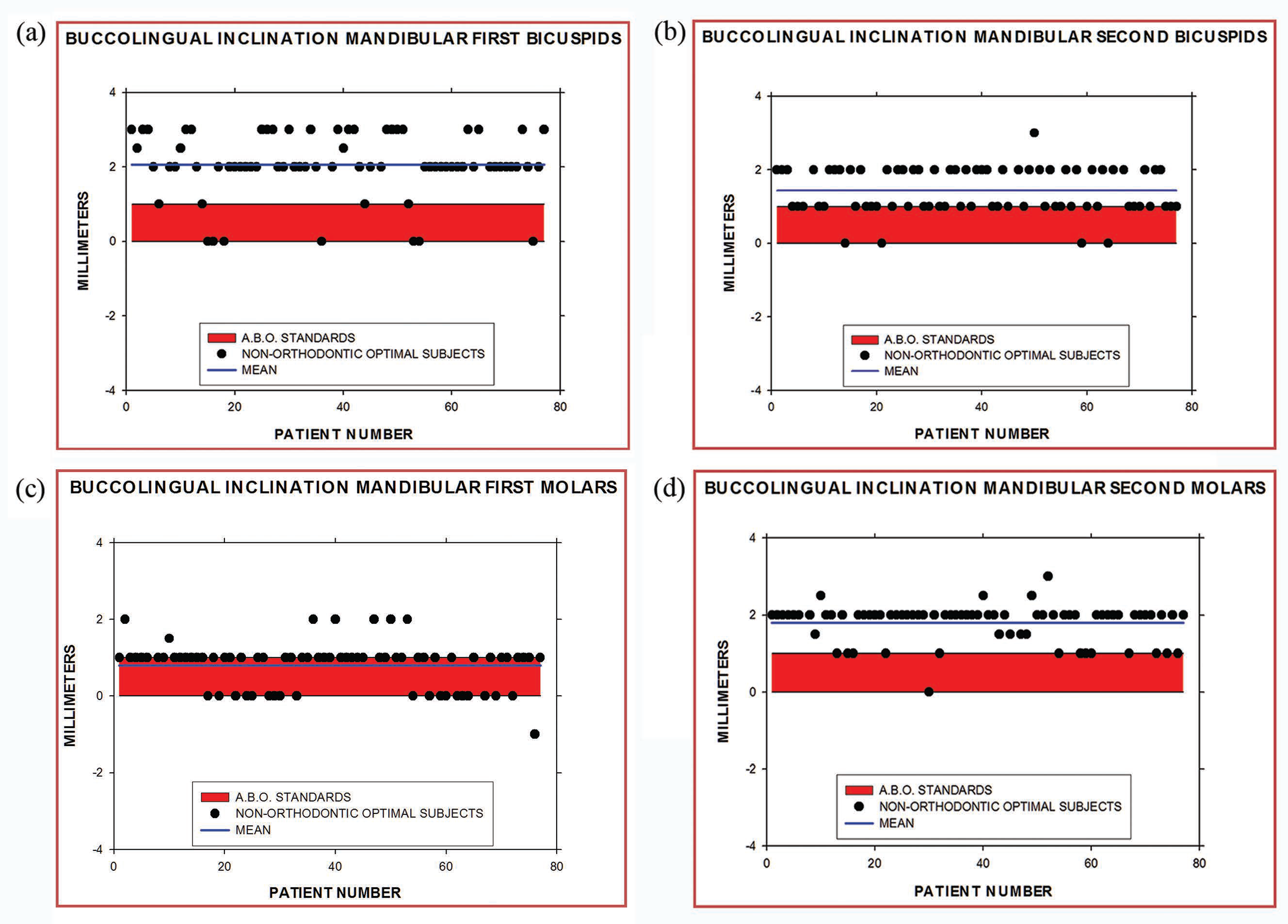
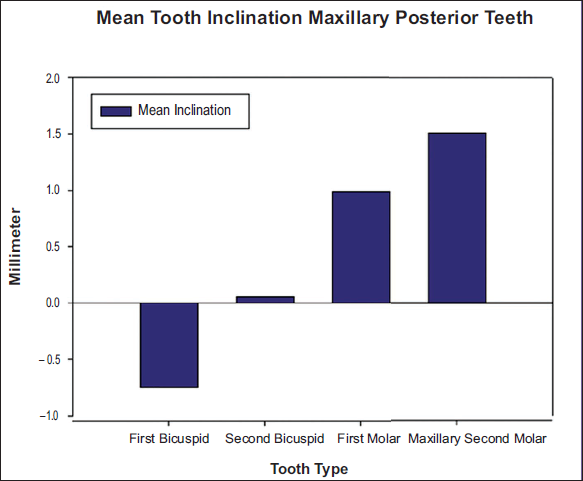
In the mandibular arch, the mean observed data on the buccolingual inclination of the mandibular first bicuspids, second bicuspids, first molars, and second molars illustrated in Table 3 are consistently different from the prescribed ABO standards (Figure 9a, b, c, and d). Mean value for mandibular first bicuspid was –0.78 ± 0.7 mm, mode was –1 mm, and values ranged from –2 to +1 mm. Suggested ABO measurements for mandibular first bicuspid ranged from 0 to 1 mm (ABO does recommend not measuring this tooth if the lingual cusps are rudimentary). Mean measurement for mandibular second bicuspid was 0.05 ± 0.6 mm, mode was 0 mm, and values ranged from –1 to +1 mm. Mean measurement for mandibular first molar was 0.9 ± 0.4 mm, mode was 1 mm, and values ranged from 0 to 2 mm. Suggested ABO measurement for mandibular first molar ranged from 0 to 1 mm. Mean value for mandibular second molar was 1.5 ± 0.6 mm, mode was 2 mm, and values ranged from 0 to 3 mm. Suggested ABO measurements for mandibular second molar ranged from 0 to 1 mm. Therefore, measured values from the nonorthodontic optimum subjects indicate a consistent difference between the measurements from the suggested ABO grading standards. The mean tooth inclination for both maxillary and mandibular posterior teeth showed an increase in value from first molar to second molar (Figures 10 and 11).
Only 53% of the cases evaluated showed contact of the lingual cusp of the maxillary first bicuspid with the opposing arch.
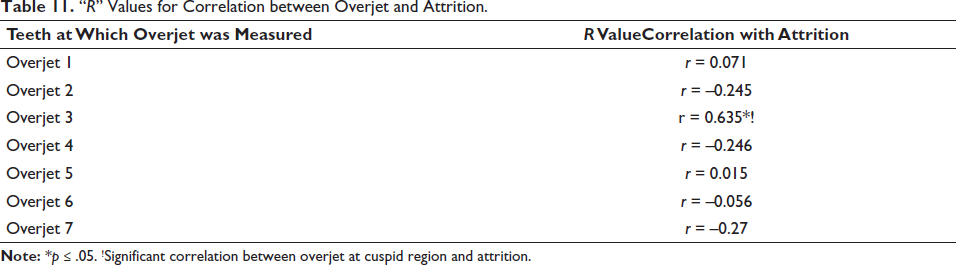
Of the subjects evaluated, 70% had no attrition and 30% of the cases had mild attrition. There was no definitive pattern of attrition noted. In cases that had attrition, a borderline correlation was noted between buccal overjet at the cuspid region and attrition (r = 0.63) (Table 11). There was no correlation between marginal ridge heights, buccolingual inclination of posterior teeth, and attrition of teeth noted. There was also no correlation noted between Curve of Spee and attrition, nor was there any correlation noted between overbite and attrition.
“R” Values for Correlation between Overjet and Attrition.
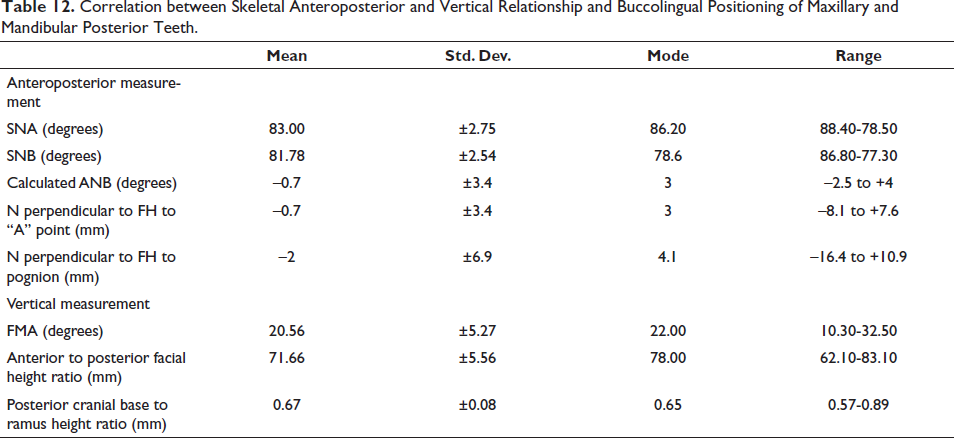
Measurements values for skeletal anteroposterior and vertical measurements are detailed in Table 12. There was no correlation between cephalometric, anteroposterior, and vertical skeletal measurements, with inclination of maxillary and mandibular posterior teeth.
Correlation between Skeletal Anteroposterior and Vertical Relationship and Buccolingual Positioning of Maxillary and Mandibular Posterior Teeth.
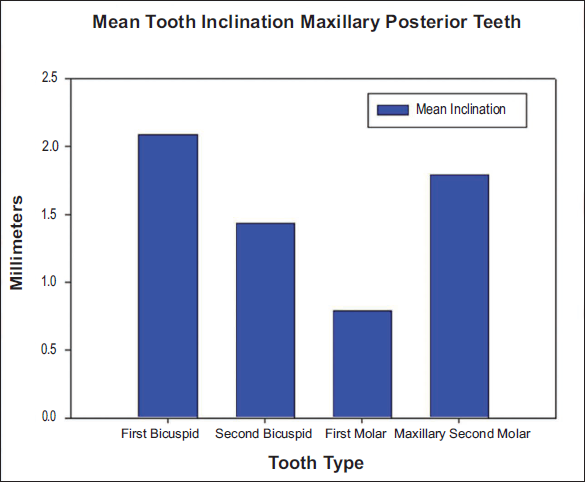
Although visual appraisal of root angulations can be assessed using panoramic radiographs, variance in linear measurement between roots of maxillary cuspid and first bicuspid was too great to be used as a grading criterion. The mean value was 2.1 ± 2.2 mm, mode was 2 mm, and the values ranged from 1 to 4.3 mm (Table 9). ABO suggests the root not be closer than 1 mm and should not contact. Panoramic radiographs of the subjects studied showed proper root separation in the maxillary anterior segment and the mandibular arch. Whereas, in the maxillary posterior segment, the roots although parallel, did not show adequate space between them (Figure 7a and b).
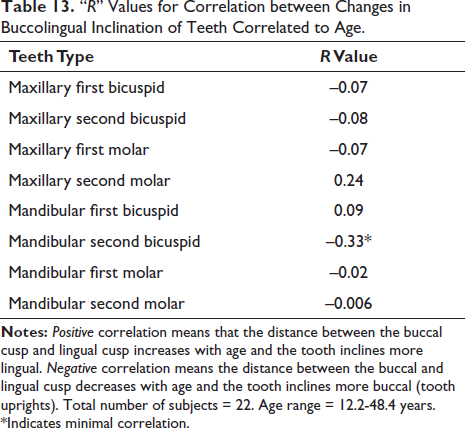
There was only a minimal correlation (r = 0.33) for mandibular second bicuspid’s buccolingual inclination to change with age. Mandibular second bicuspid showed a trend to upright buccolingually with age (Table 13).
“R” Values for Correlation between Changes in Buccolingual Inclination of Teeth Correlated to Age.
Discussion
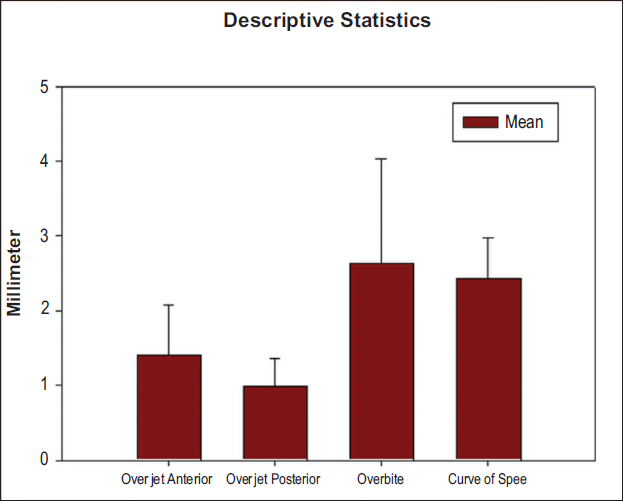
The ABO grading system was formulated more than two decades ago to evaluate the quality of orthodontically finished cases. This study confirms that most of the criteria employed in the objective grading system are consistent with those seen in untreated, naturally occurring optimal dentitions (Figure 12). It definitively validates the use of the ABO grading system both by the clinician and the examiners. All parameters, except the inclination of the teeth in the buccal segments of both arches, were found to be concordant.
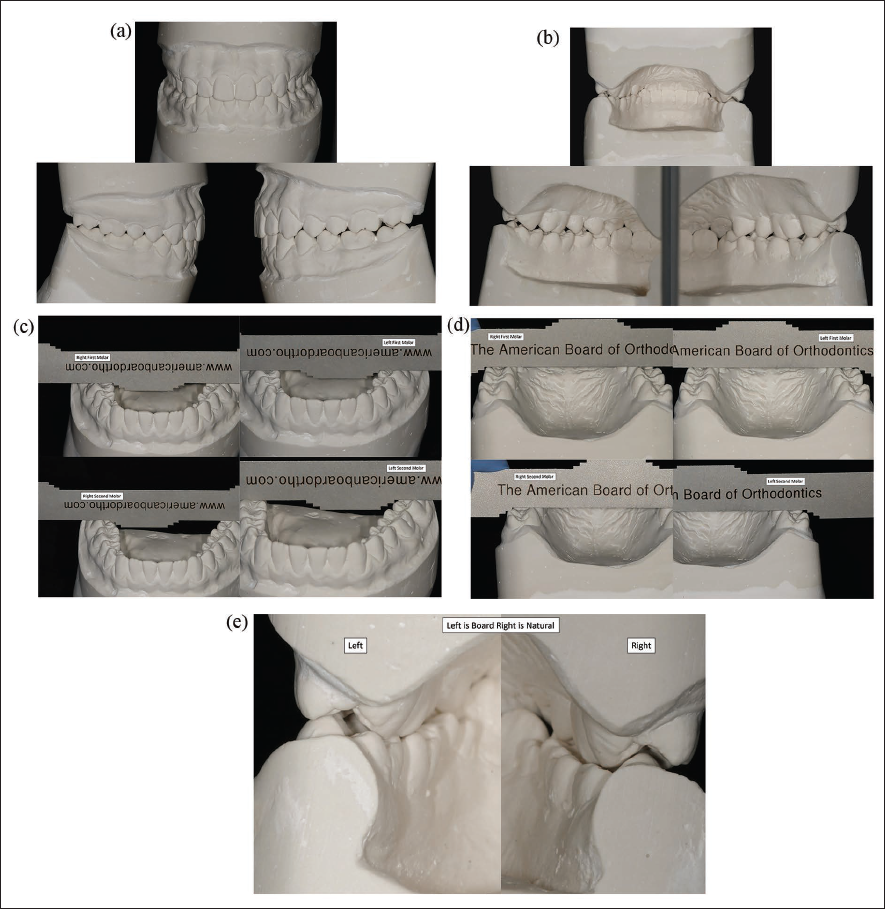
The inclination of first and second bicuspids and first and second molars, seen in the present data, is consistent with the Curve of Monsoon and Curve of Wilson, presented in the literature, which are deemed necessary for resistance to loading and masticatory function. This inclination is needed to resist the forces from the inward pull of the internal pterygoid muscle. This lingual inclination also provides occlusal resistance and axial loading during masticatory function.11–13 The current ABO grading standards for inclination between 0 and 1 mm for all posterior teeth is not consistent with the findings of this study. Following the ABO criteria10, 14 would cause unnecessary buccolingual uprighting of teeth in the buccal segments of both arches. Especially when the second molars are uprighted, it will compromise the cusp to fossa fit between the upper and lower arches (Figure 13a, b, c, d, and e).15–17
Graph Illustrating the Descriptive Statistics of Other Statistically Significant Variables in the Study. “X” Axis Indicates Different Significant Variables. “Y” Axis Indicates Mean and Standard Deviations (in Millimeters).
(a) Buccal View of Finished Case, Left Side Finished to Board Standards and Right Side Finished to Norms Established in the Study. (b) Lingual View of Finished Case, Left Side Finished to Board Standards, Right Side Finished to the Norms Established in the Study. (c) Frontal Occlusal View of Mandibular Arch of Finished Case, Showing Measurements Made with the American Board of Orthodontics (ABO) Ruler, for Lower Right, and Lower Left, First and Second Molars. Left Side Indicating Board Standards and Right Indicating Standards Established in This Study. (d) Posterior Occlusal View of Maxillary Arch Model of Finished Case, Showing Measurements Made with ABO Ruler, for Lower Right, and Lower Left, First and Second Molars. Left Side Indicating Board Standards, and Right Indicating Standards Established in This Study. (e) Distal View of Models of a Finished Case. The Left Side Illustrates Teeth Finished to Board Standards, Showing Lack of Cusp to Fossa Interdigitation. The Right Side Finished to Norms Established in This Study, Illustrating Good Cusp to Fossa Position.
There is a marginal correlation between attrition and increased overjet at the cuspid region (r = 0.63). This finding is of clinical importance as it suggests that increased overjet eliminates the protective nature of the cuspid on the posterior teeth, during the early stages of lateral movement, rendering the posterior teeth more susceptible to attrition, due to an inherent lack of cuspid guidance.
No correlation was found between anteroposterior/vertical measurements done on the cephalogram, when related to the inclination of posterior teeth, in either the maxillary or the mandibular arches. Current literature states that the maxillary posterior teeth in subjects with vertical growth patterns have a statistically significant greater buccal inclination as compared with those with horizontal growth patterns. 18 The results obtained in this study do not support this belief.
The current study also does not validate the findings of Vergalo et al., 19 who indicated that the teeth in the buccal segment upright with age. There was only a trend (r = 0.33) seen in mandibular second bicuspid to upright buccolingually with age, in subjects ranging from 12.2 to 48 years of age.
It was also noted that only 53% of the cases evaluated had the lingual cusp of the maxillary first bicuspids in occlusal contact, with the teeth in the opposing arch. This finding validates the modification of the ABO standard criterion.
Panoramic radiography is recommended by the ABO to assess root inclination and parallelism to evaluate the quality of orthodontic finishing. 14 It is imperative to note that, as reported in contemporary literature, 20 when the buccolingual angulation of a tooth changes, the largest angular differences between adjacent teeth were found in the canine–premolar area. In the present study, variance in the measurement of the linear distance between the maxillary cuspid and first bicuspid was too great to be used as a grading criterion. This variability could be due to the radiographic technique and inconsistency in radiographic equipment. In this vein, it would be worthwhile to note that cone beam computed tomography (CBCT) technology allows clinicians to obtain 3D images of the craniofacial complex with similar absorbed doses as compared with dental radiographs. 21 It provides a powerful and more reliable tool for the visualization of root angulation and should be approached by clinicians as a viable routine diagnostic tool.
One of the foreseeable limitations of the current study is that all the samples were taken from a single source. The second factor is, does this difference in occlusal factors between this studied group and ABO criteria make any difference in long-term stability and longevity of dentition. To ascertain this, further long-term effects of this difference need to be evaluated by conducting longitudinal studies, and long-term follow-up of patients treated to the criteria of both groups.
Conclusion
It can be concluded from this study that the ABO criteria and standards used to evaluate finished orthodontic cases are consistent with naturally occurring optimal dentitions with the exception of buccolingual inclination.
Tooth inclination is progressive from first bicuspid to second molar in both the maxillary arch and mandibular arches.
Inclination of first molars in both the maxillary and mandibular arches is less than the inclination of the second molars.
Maximum difference was found between ABO standards and inclination of the teeth in buccal segments of both maxillary and mandibular arches.
Only 53% of the cases evaluated had contact of the lingual cusp of the maxillary bicuspid with the opposing arch. This supports the new modification of the ABO standard criterion.
Caution should be used when evaluating cuspid root angulation with panoramic radiographs.
Overjet, when excessive in cuspid region, could possibly lead to attrition.
There was no correlation between anteroposterior and vertical skeletal relationship and tooth positioning.
There was a minimal correlation in changes in buccolingual inclination of mandibular second bicuspid with age. Mandibular second bicuspid showed a trend to upright buccolingually with age.
Footnotes
Acknowledgments
Dr Lawrence F. Andrews, Lawrence Andrews Foundation, San Diego, CA, United States for allowing us to use their records. Mrs Deepa Rajan, Ragas College, Chennai, India for statistical help. Dr Richard Kaczynski, PhD, Yale University, CT, United States for statistical help. Miss Janice Lipshy, Roseville, MI, United States for typing and preparing the manuscript. Dr Deepak Chudasama, BDS, MS, Dallas, TX, United States and Dr Robert Bruce MacIntosh, Northville, MI, United States for reviewing the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This retrospective study was approved by the IRB of Ragas College.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.