
Abstract
Occipitalization of atlas is an osseous anomaly of the craniovertebral junction, which occurs at the base of the skull in the region of the foramen magnum. It is the fusion of first cervical vertebra with the occipital bone of the skull. A 16-year-old patient reported with chief complaint of irregularly placed teeth. Routine lateral cephalogram assessment revealed the presence of fusion between first cervical vertebrae (C-1) and base of skull. The radiographic investigation revealed the presence of fusion along with the clinical findings of short neck, short face, cleft palate, missing teeth, and pain during neck extension and flexion. Such cases of craniocervical anomaly can cause orthopedic and neurological problems like abnormal posture of head, restricted neck movements, cervical pain, pain in extremities, wasting of muscles, and convulsions. The comprehensive radiographic assessment of all structures visible in cephalogram of orthodontic patient can help in identification of such anomalies and sensitize the patients about symptomatic or asymptomatic condition.
Keywords
Introduction
Atlanto-occipital assimilation of atlas is an osseous congenital anomaly of the craniovertebral junction which occurs at the base of the skull in the region of the foramen magnum. It occurs as a result of fusion of atlas with the occipital bone due to failure of segmentation and separation of the most caudal occipital sclerotome and the first cervical sclerotome during the first few weeks of fetal life. 1 It is also known as occipito-cervical synostosis, atlanto-occipital fusion, and atlas assimilation. The knowledge of such a fusion is important because skeletal abnormalities at the craniocervical junction may result in orthopedic problems and neurological symptoms. The incidence of atlanto-occipital fusion ranges from 0.14% to 0.75% of the population, with both sexes being equally affected. 2 The fusion can be partial or complete. It was first described by Rokitansky in 1844 in human skulls and radiographically by Schuller in 1911. 1
Occipitalization of atlas can result in narrowing of foramen magnum, which could compress the spinal cord or the brain stem.3, 4
The case presented here is a 16-year-old girl who reported with the chief complaint of irregularly placed teeth. But, on evaluation of lateral cephalogram, she was diagnosed with incidental finding of atlanto-occipital assimilation and basilar invagination. This further led to the investigation of implications associated with these findings, which can have a serious impact on life and well-being.
Clinical Findings
On general examination, patient was short in stature with a height of 155 cm with a short neck. According to medical history, the patient was born with unilateral cleft palate involving the left side and was operated for cleft palate at the age of 17 months. She also gave history of neck pain during extension of neck. Previous dental history revealed that she had undergone an extraction of one lower incisor teeth during childhood.
Extraoral examination revealed that the patient had convex profile and short face with a facial proportion index (FPI) 4 of Short Face Syndrome (Figure 1). On intraoral examination, the repair of cleft palate deformity was well maintained with minimum scar tissue, arch asymmetry with bilateral missing upper lateral incisors, blocked out upper left canine, missing lower right central incisor, and retroclined upper incisors with mild and moderate crowding in lower and upper arch, respectively. There was bilateral transverse discrepancy, Angle’s class II molar relation bilaterally, minimal overjet, and normal overbite (Figure 2).
Extraoral Records of the Patient.

Intraoral Records of the Patient.

Diagnostic Assessment and Therapeutic Intervention
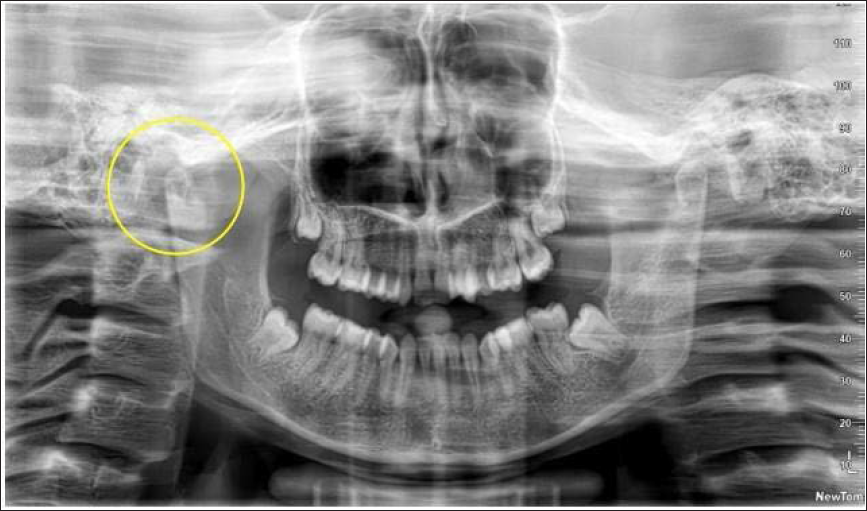
The patient was subjected to radiographic assessment with orthopantomogram (OPG), lateral cephalogram, and PA view of skull. OPG evaluation showed the congenitally missing bilateral upper lateral incisors and third molars in the formative stages (Figure 3). Lateral cephalogram assessment revealed fusion of first cervical vertebra with the occipital bone of skull, basilar invagination, and skeletal Class II malocclusion with significantly reduced gonial angle (Figure 4).
OPG Showing Altered Morphology of Right-side Condyle.
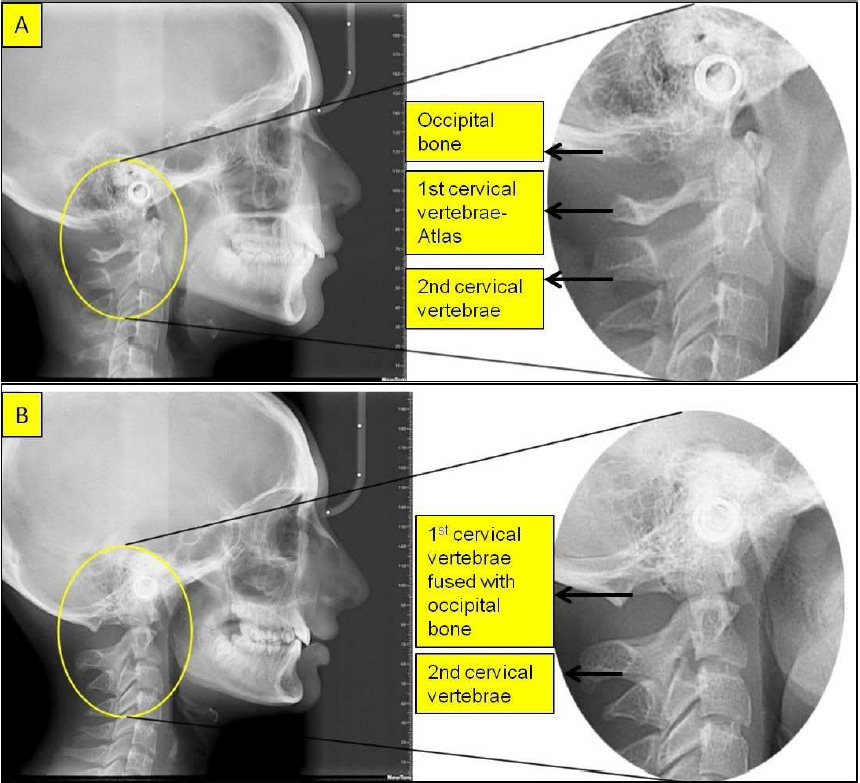
Normal Cervical Spine and Occipital Bone Anatomy (A) and Atlanto-occipital Assimilation (B).
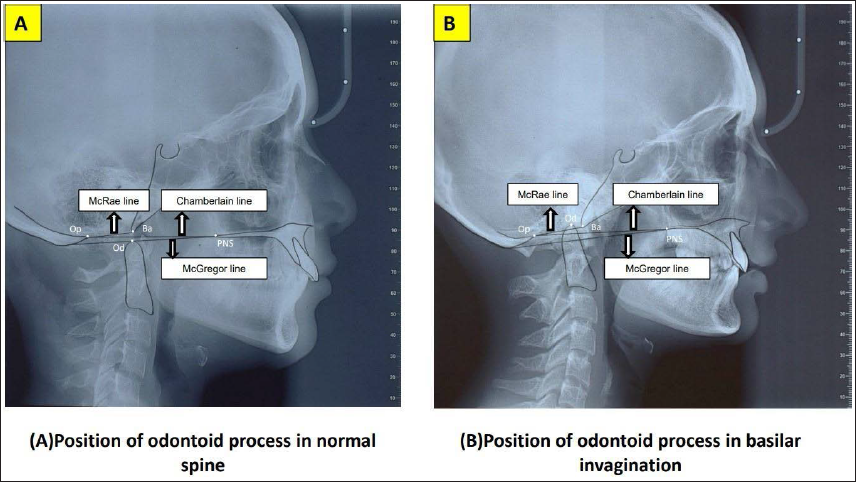
Radiographic Landmarks and Reference Lines Used for Evaluating Basilar Invagination and their Relation of Odontoid Process.
Based on the history, clinical and radiographic examination, she was diagnosed as a case of operated cleft palate left side with atlanto-occipital assimilation, basilar invagination, skeletal Class II malocclusion, congenitally missing maxillary lateral incisors, bilateral transverse discrepancy, and moderate crowding maxillary and mild crowding mandibular arch. The orthodontic therapeutic interventions were mainly aimed at the correction of malocclusion, which was due to the cleft defect of palate. The orthodontic intervention was planned with fixed mechanotherapy using preadjusted edgewise appliance. The patient was informed about the possible risks associated with this such as a wide range of neurological signs and symptoms varying from transitory headache to a full-blown neurological syndrome. This can lead to numbness and pain in the upper extremities as a prominent complaint; weakness and ataxia of the lower extremities and occipital headache may be present. 2 The patient was advised and sent for necessary orthopedic and neurological opinion. The neurologist on evaluation reiterated the above complications and advised to restrict or avoid sudden neck movements. The neurological symptoms had not yet set-in except neck pain on extension; she was advised against any intervention at present and lifestyle changes were emphasized.
Discussion
Occipitalization of atlas is a congenital anomaly, but symptoms do not develop until the second decade of life. However, the correlation of familial history or birth history is not reported till date. The incidence of occipital assimilation ranges from 0.14% to 0.75% of the population affecting both genders equally. 1 The patient discussed in this case report also reported pain in the neck on extension indicating the neurological association of the anomaly. This may be attributed to the gradual increase in the laxity of the transverse ligament by the repeated flexion and extension of neck leading to compression of the spinal cord. Compression of structures like vertebral artery and first cervical nerve may reduce the blood flow to the brain resulting in neurological symptoms and abnormal posture of the head. 5 Also, the patient discussed here presented with oro-facial defects like cleft palate and missing bilateral upper lateral incisors. de Rezende Barbosa et al. 6 evaluated the occurrence of cranio-vertebral anomalies in cleft patients and found atlanto-occipital assimilation in 1.32% of study sample indicating the association with cleft defects.
Hensinger 7 reported that the onset of clinical symptoms can be sudden, which could be due to minor trauma. One such case presented with findings like cervical pain and convulsions as reported by Kussmaul and Tenner. 8 However, our case did not report any episodes of convulsion. Vakili et al. 9 reported a case of fusion with sudden death. McRae and Barnon 10 mentioned that patients with occipitalization of the atlas may have features like low hairline, torticollis, restricted neck movements, or abnormal short neck. In our case, the patient displayed short neck and restricted neck movements. The compression of the first cervical nerve affects the suboccipital muscles, which are known as postural muscles resulting in abnormal posture of head and an unsteady gait. 11 The headaches associated with this condition are characterized as dull and aching, and are located over the posterior two-thirds of the skull. The headaches may be precipitated by coughing or by neck movements. In our case, there were no episodes of headache reported till date, but it can be possible future implication. 12 Also, jerky neck movements if carried out in such cases may precipitate such episodes. Neurologic findings associated with occipitalization of the atlas also include tinnitus, visual disturbances, auditory disturbances, and lower cranial nerve palsies leading to dysphagia, dysarthria, and nystagmus. 13 Basilar invagination was also one of the finding in this patient along with occipital assimilation. Basilar invagination is evaluated on the lateral cephalogram using reference lines connecting basion (Ba) to opisthion (Op) (Mc Rae’s line), posterior nasal spine (PNS) to opisthion (Chamberlain’s line), and PNS to basio-occiput (Mc Gregor’s line) and their relationship with odontoid (Od) process of atlas. In this patient, the tip of odontoid process was above the McRae line by 2 mm (normal 5 mm below this line), above the McGregor line by 7 mm (normal till 4.5 mm above this line), and above the Chamberlain line by 4 mm (normal till 3 mm above this line) indicating basilar invagination (Figure 5). Basilar invagination puts pressure on the brainstem producing symptoms like headache or pain in the back of the head, dizziness, confusion, difficulty swallowing, numbness in hands or feet, and weakness.
Orthodontic Implications
It is important for an orthodontist to have basic knowledge of cervical spine anomalies and their associated signs and symptoms so that any such incidental anomaly can be detected and patient educated about the consequences.14, 15 Diagnosing such incidental findings, educating patient about their possible implications, and directing them to seek medical advice can prove to be more beneficial for the patient’s wellbeing than dental/orthodontic treatment and establish high credibility of an orthodontist as a doctor. It does not have any direct implication on orthodontic tooth movement, but the orthodontist must ensure that during any kind of treatment neck extensions and forward-backward bending of neck should be avoided and patient must be advised for gentle movements to prevent precipitation of any adverse effect.
Conclusion
The basic knowledge of normal cervical spine and its anomalies is must for an orthodontist since it is an important feature in lateral cephalogram, the most common investigative tool used in orthodontic diagnosis. The knowledge of atlanto-occipital assimilation and its clinical significance can help in sensitizing the patient about potential existing/future neurological implications to seek medical advice and intervention. Since the symptoms of occipital assimilation start in the second decade of life and most malocclusions are treated in the same decade, the routine lateral cephalogram can prove to be a significant diagnostic aid in the diagnosis of occipital assimilation of atlas.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained.