
Abstract
Aim
To evaluate and compare the accuracy of bracket positioning in the incisogingival and mesiodistal aspects with the MBT gauge and new multipurpose bracket positioning tool.
Materials and Methods
Bracket positioning of maxillary anterior teeth (n=30) was assessed on the typhodont model. The UNC-15 (University of North Carolina) probe was modified as an MBP tool. Five different malocclusions: (a) Class II Division 1 (n=6); (b) Class II Division 2 (n=6); (c) Class I with mesially inclined maxillary anterior teeth (n=6); (d) Class I with crowding in maxillary anterior teeth-3 mm (n=6); (e) Class I with different vertical heights of maxillary anterior teeth (n=6). The measurements of the study were divided into three groups; Group A: Central Incisor, Group B: Lateral Incisor, and Group Canine, based on positioning with MBT Gauge and MBP tool. The measurements on each tooth were recorded using vernier calliper, on the basis of which the discrepancy in vertical and axial bracket positioning was assessed.
Results
The comparative evaluation of the MBT gauge and MBP Tool showed statistically insignificant differences between all the groups (p>0.05). The mean standard deviation with the MBT gauge was 0.5-0.7 mm, whereas with the MBP tool was only 0.05- 0.3 mm only; suggesting clinical relevance and acuity during bracket positioning.
Conclusion
The MBP tool is relatively accurate and comparable to the MBT gauge as the horizontal and vertical arm of the MBP tool facilitates proper visualization by coinciding with the long axis of the tooth on the typhodont model leading to augmented precision.
Introduction
Earlier orthodontist had to be good wire bender but modern orthodontist needs to be precise bracket positioner. Any inaccuracy in the bracket positioning at the start of the treatment is carried on till the end of the treatment. Inaccurately placed brackets can cause in-out discrepancies, loss of tip and inability to express the torque completely. The facial axis point (Andrews plane) 1 was chosen to place the brackets because it was easily and consistently located. 2 Ricketts 3 and later Kalange 4 recommended the use of marginal ridges as a guide for the vertical positioning of brackets and bands. In Begg’s technique, the bracket is centered mesiodistally on the labial or buccal surface with the base of the archwire slot 4 mm from the incisal edge of the cusp tip. 5
Ronald Roth developed the second generation of brackets with some modifications in the Andrews’s prescription. Canine and premolar were used as references for bracket height positioning in Roth’s system. According to McLaughlin et al., 6 the accuracy of bracket positioning is a prerequisite so that the built-in features of the bracket system can be expressed wholly and efficiently. They advocated the positioning of brackets at a measured distance from the incisal edge, with different vertical positions recommended for different-sized teeth. MBT gauge was introduced by Richard McLaughlin, John Bennett, and Hugo Trevisi.
Gauges are used for the placement of the brackets at proper height. Appropriate usage of gauge accentuates the precision of the bracket position and affects initial alignment, thus diminishing the need for arch wire bends and bracket repositioning. 7 For accurate bracket positioning in contemporary orthodontics, two types of gauges are used—Star-shaped gauges or Boone’s gauge—developed by Edgar R Boone, an American orthodontist, and straight rod-shaped gauges or Dougherty gauges. These gauges help in vertical alignment (occlusogingival) of the brackets, but horizontal positioning of the brackets cannot be done by them. Ideally, these gauges should be placed perpendicular to the labial or buccal surface of the teeth. Also, varying the angle of placement of these gauges over the tooth can change the height of the bracket, which is usually in the range of 2 mm. As the angle between the gauge and the tooth decreases, it means that the bracket is positioned more gingival. Furthermore, it will result in changes in torque expression and compromise of the Smile arc.
The height bracket positioning gauge (HBPG) and Boone’s gauge have no component to assess the precise placement of brackets along the horizontal plane. For horizontal positioning of the bracket along the long axis of the crown, indirect vision is required via a mirror. Bracket positioning at times is altered during the removal of these instruments from the bracket on the tooth surface.
Though there are various modifications of gauges that exist, there is no single bracket gauge that can be used universally for all teeth to orient brackets in both the vertical and axial planes simultaneously.
The purpose of this study was to evaluate and compare the accuracy of bracket positioning in the vertical and horizontal aspect with MBT gauge and modified UNC-15 probe-multipurpose bracket positioning tool (MBP tool) in different malocclusions on typhodont model.
Materials and Methods
MBP Tool Fabrication
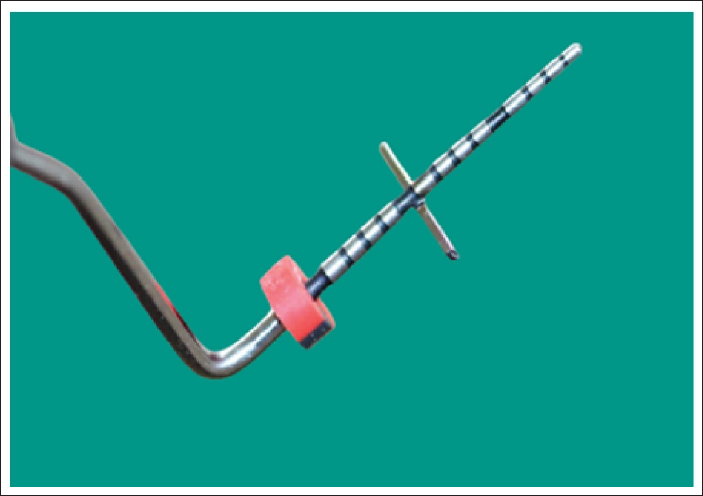
MBP tool 8 was fabricated by modifying UNC-15 probe. The UNC-15 probe is a 15-mm-long periodontal probe with millimeter markings. Zero mm is taken as the marking farthest away from the tip of the working end. In this study, to correlate with the long axis of the tooth, the UNC-15 probe was modified by welding 0.017 × 0.025″ stainless steel wire of approximately 6 mm in length at the 6-mm mark in a horizontal fashion. Furthermore, a vertical arm was welded on the same side as the measuring side to minimize errors in both vertical and horizontal bracket placements. With this adaptation, the probe can now effectively position brackets in the vertical plane while simultaneously orienting them in the axial plane (Figure 1).
Multipurpose Bracket Positioning Tool.
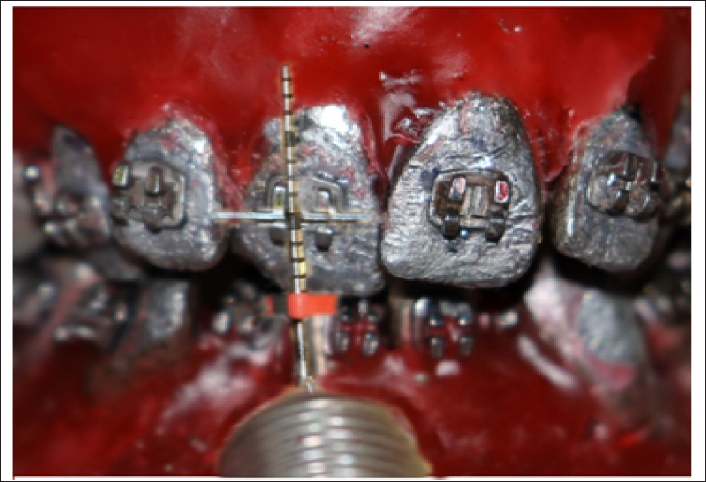
Five different malocclusions were simulated on the typhodont model to determine the accuracy of the MBT gauge and MBP tool. Maxillary anterior teeth were selected for the study (Figures 1 and 2) as indirect vision is required for horizontal positioning of the brackets and chances of errors are higher, whereas in mandibular teeth, positioning along the long axis of the teeth can be done under direct vision.
Bracket Positioning by MBP Tool.
As this study was conducted on the typhodont model, no patient consent or ethical approval was required. Five types of malocclusions were as follows:
Angle’s Class II division 1 Angle’s Class II division 2 Angle’s Class I mesially inclined maxillary anterior teeth Angle’s Class I crowding in maxillary anterior teeth: 3 mm Angle’s Class I with different vertical heights of maxillary anterior teeth
This was an in vitro split-mouth study to eliminate any discrepancies in bonding due to malocclusion. MBT gauge and the MBP tool were used to bond 15 teeth on a typhodont model, respectively.
The crown height of the typhodont teeth was measured using a millimeter scale and the height of bracket placement was determined according to the tables provided by McLaughlin and Bennett. The 0.022 × 0.028 MBT (American Orthodontics, Mini Master Series) brackets were used, from the right central incisor to the canine, were positioned at the specified height using the MBT gauge (Figure 2), while brackets from the left central incisor to the canine were positioned by the MBP tool (Figure 3). They were bonded by Enlight light-cured composite resin (Ormco) and cured with an LED curing light for 5 s.
Bracket Positioning by MBT Gauge.

An insize digital point Vernier caliper (Figure 4) was used (accuracy rate: 0.01 mm) for recording the measurements. The recorded four (Figures 5 and 6) measurements were:
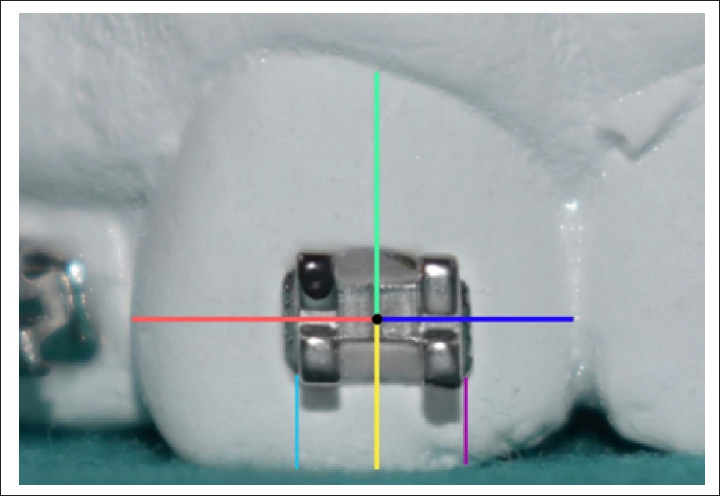
Mesial surface measurement: From the center of the vertical scribe line to its adjacent mesial interproximal surface. Distal surface measurement: From the center of the vertical scribe line to its adjacent distal interproximal surface. Incisal surface measurement: From the center of the vertical scribe line to the center on the incisal edge or cusp tip. Gingival measurement: From the center of the vertical scribe line to the gingival zenith.
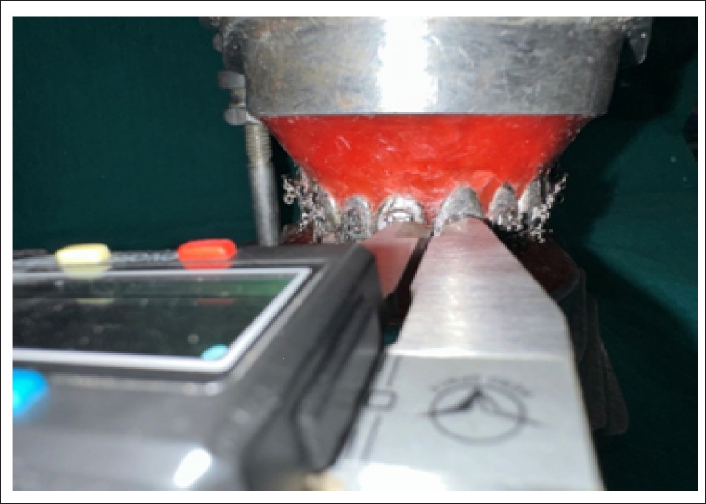
Insize Pont Vernier Caliper—0.01 mm Accuracy.
Diagrammatic Representation of Measurements in Mesial, Distal, Occlusal, and Gingival Direction.
Measurement by Vernier Caliper on Typhodont.
Result
Statistical Analysis
IBM SPSS Statistics version 23 (Statistical Package for the Social Sciences) was used for the statistical analysis. A descriptive and independent t test was done to examine whether there was a difference in bracket positioning between the MBP tool and MBT gauge, and p ≤ .05 was considered significant.
Sample size determination was not done as it is a prototype study and clinical evaluation of the MBP tool is yet to be carried out.
Measurement of Vertical Error in Bracket Positioning
Tables 1 to 3 show the vertical error distributions of bracket positioning for each tooth by two gauges separately. The mean difference between the MBT gauge and MBP tool in the central incisor on the gingival side was 0.27 mm and on the occlusal side was 0.34 mm, in the lateral incisor on the gingival and occlusal side was 0.43 mm and 0.52 mm, respectively, demonstrating more error of placement along the occlusal direction.
Comparison of MBT Gauge and MBP Tool in Central Incisor.

Comparison of MBT Gauge and MBP Tool in Lateral Incisor.

Comparison of MBT Gauge and MBP Tool in Canine.

Whereas in canine, on the gingival side, it was 0.09 mm, and on the occlusal side it was 0.06 mm. The overall result is statistically insignificant (p > .05), but this is clinically significant, as this error can lead to1st and 3rd order errors and affecting further outcome.
Measurement of Horizontal Error in Bracket Positioning
Tables 1 to 3 also show the horizontal error distributions of bracket positioning for each tooth by two gauges separately. The mean difference between the MBT gauge and MBP tool in the central incisor mesial and distal side was 0.03 mm, in the lateral incisor on the mesial and distal side was 0.11 mm and 0.12 mm, respectively.
Whereas in canine, the mean difference on the mesial and distal sides was 0.24 mm, suggesting more placement error horizontally due to its eminence.
The result is statistically insignificant (p > .05) but clinically significant as even a slight variation leads to in-out discrepancies.
The mean standard deviation with MBT gauge was 0.5 to 0.7 mm, whereas with MBP tool was 0.05 to 0.3 mm only suggesting clinical relevance and acuity during bracket positioning.
Discussion
In the original edgewise appliance, bracket placement was typically done using gauges and standard millimeter measurements from the incisal edge of each tooth, regardless of tooth size. This approach often resulted in larger incisors having brackets placed more incisally, leading to variations in torque and in-out effects produced by the brackets. McLaughlin et al. proposed that the bracket wings must be parallel to the long axis of the tooth and the most difficult aspect is obtaining the axial accuracy, so it is essential to visualize the long vertical axis of the clinical crown of each tooth. Numerous instruments have been introduced to make bracket positioning more convenient, but very few offer the simplest method for the same.9, 10
Apart from the HBPG and Boone gauge, other gauges have been introduced by Droschl, Samuels, and Geron.11–13
The bracket positioning gauge by Droschl 11 is a modification of the Boone gauge in which the sharp metal pens for marking the enamel are replaced by pencil leads set at 3.5, 4.0, 5.0, and 7.5 mm from the instrument base. Russell H A Samuels 13 designed The TN3 TM bracket positioning instrument specifically for positioning orthodontic brackets and cleaning up the excess composite. It is a simple double-ended hand-held instrument with a bracket positioning blade at one end and a composite cleaning at the other end. With the Height Gauge Tweezer introduced by Geron, 12 bracket height is measured from the bracket slot to the incisal edge at two points simultaneously, thus eliminating angulation errors. The tweezer holds the bracket by its slot with two cylindrical extensions engaged from the mesial and distal, eliminating in-out errors. When the bracket is pressed against the tooth, it adapts to the contour of the labial surface, eliminating torque errors and squeezing out excess adhesive.
Moreover, most gauges are designed to be used in a specific manner for different areas of the mouth. Failure to position the gauge correctly can lead to incorrect positioning of brackets. Interestingly, even when using the same bracket gauge, holding it differently can cause the bracket to shift either incisally or gingivally, further contributing to bracket placement inaccuracies. This highlights the need for a more versatile and standardized bracket positioning tool that can consistently and accurately place brackets in the anterior and posterior regions of the mouth. 8
A new MBP tool was used in this study to minimize the errors caused by the misplacement of other gauges.
The calibrations on the UNC-15 probe made bracket placement accurate and easy. 8 The time required in bracket placement was shorter with the MBP tool. Unlike the MBT gauge, no additional armamentarium was required. A single instrument could be used universally for all teeth for vertical and axial adjustments. Additionally, the instrument could be sterilized by autoclaving. The development of parallax error is reduced with the MBP tool since it offers a more objective way of usage. The visualization errors caused during the positioning of the gauges are minimized as the MBP tool has both vertical and horizontal components.
The result is clinically significant as even a small amount of discrepancy can lead to 1st, 2nd, and 3rd order errors resulting in unnecessary extrusion, intrusion, in-out discrepancies, and inefficient expression of the torque. The result shows that the greatest discrepancy in bracket positioning using the MBT gauge occurs in canines in the occlusal direction because of the eminence. Conversely, when using the MBP tool, the most significant error is observed in the occlusal direction of the lateral incisor. The accuracy of both gauges is comparable in the mesial and distal directions. The mean standard deviation with the MBT gauge was 0.5 to 0.7 mm, whereas with the MBP tool was 0.05 to 0.3 mm, suggesting more inaccuracy while placing the bracket with the MBT gauge compared to the MBP tool.
This study showed a correlation with the research conducted by Fowler et al.14, which aimed to assess the accuracy of bracket placement. They reported that the vertical and mesiodistal errors were ±0.32 mm and ±0.20 mm, respectively. However, they observed the minimal error mesiodistally. Aguirre et al. 15 conducted a study to compare bracket positioning accuracy. They found that measurement error in angulation is more than in vertical and mesiodistal positions. Balut et al. 16 reported average vertical errors of 0.34 mm in placing preadjusted brackets.
Studies by Lahcen Ousehal and Laila Lazrak and his associate 17 and Amir Mohammadi and Seyed Moslemzadeh 18 have assessed the bracket positioning accuracy with the help of photographs, but measurements obtained by Vernier caliper have been proven to be more accurate.
To conclude, the MBP tool can be used for hassle-free bracket positioning.
A further prospective study involving a large sample size with patients having different malocclusion would be beneficial to validate the MBP tool clinically.
Conclusion
The advantages of the MBP tool are:
The horizontal and vertical arms of the MBP tool make it easier to use, as it coincides with the long axis of the tooth. Thus, it is relatively accurate to the MBT gauge. Bracket positioning requires less time, minimizing parallax error and allowing clinicians to streamline their inventory by using a single tool.
Authors’ Contributions
ASR: Manuscript writing, statistical analysis, and data analysis; BJ: Conceptualizing idea and manuscript writing; AS: Review for the manuscript; KT: Review for the manuscript; AP: Proof reading.
Copyright Statement
The undersigned author(s) transfers all copyright ownership of the manuscript (A New Versatile Tool for Accurate Bracket Positioning—An In Vitro Study) to the Journal of Indian Orthodontic Society in the event the work is published. The undersigned author warrants the article is original, does not infringe upon any copyright or other proprietary right of any third party, is not under consideration by another journal, has not been published previously, and includes any product that may derive from reviewed and approved the final version of the manuscript. I sign for and accept responsibility for releasing this material.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable.