
Abstract
Backgrounds and Objectives
The use of a retainer in the retention phase creates different perceptions amongst patients. However, the evidence regarding it is limited. This research was conducted to analyze the difference in patients’ perception of discomfort and aesthetics between Hawley and vacuum-formed retainers.
Methods
This study included 80 patients (n per group = 40). Patients were invited to participate if they had completed their treatment for 6 months to 5 years and complied with the inclusion criteria. Seven questions were given to the patients using a digital-based questionnaire. Each was asked twice to address both maxillary and mandibular retainers. Responses were measured using the Visual Analogue Scale. Blinding was applied through data analysis.
Results
Statistically significant differences were found in the perception of the aesthetic, shape, and retainer color. Statistically significant differences were not found in the perception of comfort, pain, sharpness, pressure, presence of soft tissue cut, and confidence level with the retainer in place. No harm was observed to any patients during the study.
Conclusions
Vacuum-formed retainers (VFRs) were more acceptable than Hawley retainers (HRs) regarding the retainer’s aesthetic, shape, and color. There were no significant differences between HRs and VFRs regarding patient perception of discomfort and confidence when using the retainer.
Introduction
Orthodontic treatment involves various force systems that provide cellular responses, resulting in tooth movement. This movement causes remodeling of the surrounding tissue to maintain the teeth in their new position. 1
However, maintaining orthodontically treated teeth in their final positions after treatment is one of the most challenging aspects of orthodontic treatment. Relapse can occur when the teeth move back toward their initial malocclusion and can result from gingival, periodontal, occlusal, and growth-related factors, as well as normal age-related changes. 2
The extent of the relapse is hard to predict with significant individual variations.1, 2 Extensive studies on orthodontic treatment outcomes have shown that 40% to 90% of patients have dental irregularities within 10 to 20 years post-treatment. 1 Moreover, other researches have reported a 70% rate of changes occurring 10 years after the completion of the retention phase and increasing to 90% a decade later, especially concerning the alignment of the mandibular anterior teeth.3, 4 Recent study have shown a 67% stability rate 10 years after treatment, except for the mandibular incisors. 5 These findings emphasize the possibility of relapse across various post-treatment phases. Prolonged retention is advocated to reduce the risk of relapse. 2 The changes in long-term stability highlight the importance of a continuous retention phase using a retainer to maintain long-term stability.4, 6 Relapse is a long-term problem that requires continuous monitoring. 7 Retention is the final phase of orthodontic treatment, aimed at maintaining teeth in their new positions post-treatment. 8
There are two types of retainers: fixed and removable retainers. 8 Removable Hawley retainers (HRs) and vacuum-formed retainers (VFRs) are the most widely used types.9, 10 Numerous studies have assessed their performances and have reported either no significant differences or only minor differences in their retentive capabilities.11, 12
A major disadvantage of using removable retainers is the need for patients to comply with their retainer regimen.13, 14 The success of orthodontic treatment, including during the retention phase, heavily relies on patient compliance. 13 Previous studies examining patient satisfaction with orthodontic treatment reported that patients had a universally unfavorable view of retainers.15, 16 Wearing a retainer can lead to difficulties in speaking and eating, increased salivation, embarrassment, and overall inconvenience, even more than fixed appliances and headgear.16–18 A study found that 67% of patients had stopped using their retainer within 2 years post-treatment. 19 Moreover, 72% of patients had either stopped wearing their VFRs or rarely used them after 5 years, with 28% of those who continued using them citing concerns of relapse. 20 Negative impacts on appliance acceptance and patient compliance can be attributed to discomfort from wearing orthodontic appliances. 21 However, only a few studies have described patients’ experiences during the retention phase.14, 22 This is unexpected, given the importance of the retention phase. Many orthodontists frequently recommend long-term retainer use, if not for the remainder of the patients’ lives. 22
Literature reviews have shown that only a limited quantity of studies have objectively compared patients’ perceptions of HRs and VFRs. A previous study that compared the aesthetic perceptions on the use of HRs and VFRs found that most patients favored VFRs over HRs. 23 However, this study did not examine the perceptions of patients who had finished treatment and were actively using a retainer. Another study evaluated the cost-effectiveness and satisfaction levels among patients with HRs and VFRs during the initial six months after debonding. Subjects in this study preferred VFRs, although both types of retainers were associated with discomfort. 24 A different study investigated changes in the oral cavity and compliance levels with HRs and VFRs. The results of this study suggested that patients found VFRs more acceptable due to their aesthetic appeal and provide greater oral comfort. 25 However, both studies offered limited detailed analysis of patients’ perceptions and presented the data as secondary outcomes. Given the importance of understanding patients’ perspectives, conducting comprehensive research to fully comprehend their experiences with retainers is crucial. 7 Study by Saleh et al. (2017) primarily aimed to compare the acceptability of retainers. 14 While there is no consensus on the optimal duration of the orthodontic retention phase with removable retainers, many experts recommend wearing the retainer for at least 1 year after debonding.4, 8 The previous 3 studies have refrained from comparing patients’ perceptions beyond a 6-month interval. A recent study assessed patients’ satisfaction 5 years after debonding and reported that patients were equally satisfied with VFRs and bonded retainers. However, it did not examine the same type of retainers.20
Given the background mentioned above, it is essential to carry out a comprehensive study of patients’ perceptions when using retainers. This study aims to collect data on patients’ perceptions of their retainers and analyze differences in discomfort and aesthetic preferences between two removable retainer groups, HRs and VFRs, within 6 months to 5 years following debonding.
Materials and Methods
Trial Design and Ethics
This research, a descriptive-analytic study with a cross-sectional design, evaluates the patients’ perception when using removable HRs and VFRs. Perceptions were assessed using a digital-based questionnaire. The Dental Research Ethics Commission (KEPKG) from the Faculty of Dentistry, University of Indonesia and UI Dental Hospital approved the study protocol (no. 68/Ethical Approval/FKGUI/IX/2022 and 035/UN2.F2.RSKGM/PPM.00/202).
Participants, Eligibility Criteria, and Settings
The research was conducted at the Department of Orthodontics, Faculty of Dentistry, University of Indonesia (FKG UI) in Jakarta, Indonesia, from September to November 2022. The study included all individuals who had completed their treatment at the Orthodontic Clinic, University of Indonesia Dental Hospital (UI Dental Hospital) in Jakarta, Indonesia.
Patients willing to participate and complied with the inclusion criteria were invited to participate in the study. The criteria were as follows: male and female aged 19 to 44 years who were previously treated orthodontically with fixed appliances at the UI Dental Hospital on both arches, with a minimum high school educational background, had finished their treatment for 6 months to 5 years, was given the same removable retainer that was either Hawley or VFRs on both arches, and was willing to fill out an online questionnaire. Patients were excluded for the following reasons: they did not fulfill the inclusion criteria and were unwilling to participate in the study.
Sample Size Calculation
The study used a convenience sampling method with simple randomization drawn from the population. A sample size calculation was carried out to assess perceptions regarding the use of retainers. A sample size calculation was based on an alpha significance level of 0.05 (5%) and a beta of 20% to achieve 80% statistical power (1-β) of the test to detect a minimum difference of 1 degree of perceived discomfort and aesthetic, with a standard deviation of 0.78 based on previous research. 14 The calculated sample size indicated the need for 37 individuals. Forty patients were enrolled per group to increase the power and account for a potential dropout, resulting in 80 subjects. No differentiation was made regarding gender.
Interventions
A digital-based closed questionnaire was used in the study during the data collection phase to assess the patient’s perception regarding the use of HRs and VFRs. Written informed consent was obtained at the beginning of the questionnaire. The questionnaire contained self-report questions used in previous studies.14, 22, 24 Additional modified questions were included in this study. The questions covered perceived discomfort and aesthetic experiences while using the retainers. The questionnaire consisted of 7 questions, each posed twice to address both maxillary and mandibular retainers, thus totaling 14 questions.
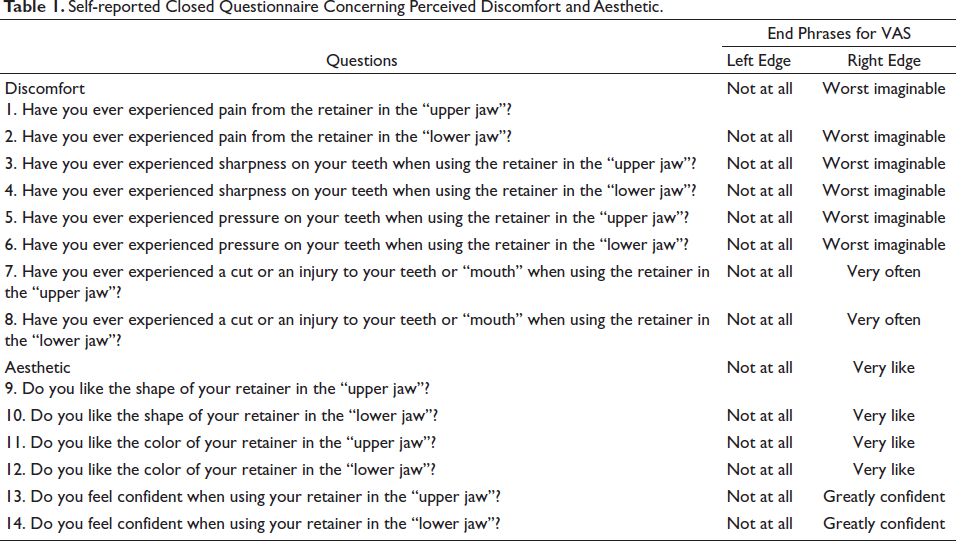
A 100-mm Visual Analogue Scale (VAS) was given at the end of each question. Respondents gave their responses by sliding the analog scale of the VAS line. The left edge of the VAS line represented an extremely negative response, while the right edge indicated an exceedingly positive one, aligning with the nature of the questions asked. The score range spanned from “0” (least favorable) and the highest score was “100” (most favorable). The participants were given written information on how to respond at the beginning of each question. The completion of the questionnaire required approximately 5 to 10 minutes per participant. The questionnaire used in this study is presented in Table 1.
Self-reported Closed Questionnaire Concerning Perceived Discomfort and Aesthetic.
Outcomes
The study assessed patients’ perceptions of discomfort and retainer aesthetics during the retention phase. Perceptions were evaluated using a 14-question questionnaire related to perceived discomfort and aesthetics. Responses were made using a 100-mm VAS. Answers were measured by digitally measuring the distance between the analog slide and the left edge of the scale in millimeters.
Before data collection, a trial was conducted to determine the questionnaire’s validity and reliability and estimate the time required to complete the questionnaire. This trial involved different sample groups, with a minimum of 10% of the planned assessment sample.
Blinding
Blinding was performed through data analysis by assigning an internal ID number for each participant. The principal examiner was unaware of the participant’s age, sex, and the specific group to which the patient belonged.
Statistical Analysis
The validity of the questionnaires was assessed using the Pearson Product Moment by comparing r tables and r counts, while the reliability was tested using a test-retest approach by calculating the inter-correlation coefficient (ICC) and Cronbach’s Alpha.
Shapiro-Wilk normality tests were conducted (n < 50) to evaluate data distribution. The differences between patients’ perceptions were analyzed. The collected data displayed a nonnormal distribution; nonparametric analyses were conducted using median (Mdn) and interquartile range (IQR). The Mann–Whitney test was used to compare questionnaire responses between the different groups. Descriptive statistics were also performed and group comparisons were made to ascertain if there were any significant statistical differences in perceptions between the two types of appliances.
The IBM Statistical Package for the Social Sciences (SPSS) version 25.0 software (SPSS Inc.) was used to perform all statistical analyses. At p < .05, the results were considered to be statistically significant.
Results
Participants Recruitment and Flow
Patient recruitment began from September 2022 to November 2022. Among the 167 patients (HRs = 55; VFRs = 112) who fulfilled the inclusion criteria and were initially informed about the study, 63 were excluded as they chose not to participate, resulting in 104 (HRs = 49; VFRs = 55) who agreed to take part. During the intervention period, 24 participants (HRs = 9; VFRs = 15) did not fully complete the questionnaires.
Participants’ Characteristics
Eighty participants were included in the study (n per group = 40). The HRs group had a mean age of 25.8 years, while the VRFs group had a mean age of 28 years. The demographic characteristics of the patients in each group are detailed in Table 2.
Study Sample Characteristics Based on Age and Gender.

Questionnaire’s Validity and Reliability Tests
The validity of the questionnaire was determined using Pearson Product Moment. The calculated r-count exceeded the r-table value (the r-table: 0.31). To assess the questionnaire’s reliability, a test-retest was conducted to assess the questionnaire’s reliability by collecting data from patients on 2 different occasions, with a 2-h gap between each data collection. The test-retest reliability analysis showed a high intraclass correlation value (high ICC) of 0.974 (confidence interval: 95% of 0.913-0.992), indicating strong reliability. These results affirm the validity and reliability of the questionnaire.
Perception Results for HRs and VFRs
When comparing the perception results between the HRs and VFRs groups, it was observed that the HRs group reported higher levels of comfort, pain, and pressure on both arches, along with the presence of mandibular soft tissue cuts while wearing the retainer, compared to the VFRs group. Conversely, the VFRs group reported higher levels of perception regarding sharpness and pressure with both retainers in place compared to the HRs group. However, no statistically significant differences were found between the two groups regarding perceived comfort across all aspects (p ≥ .05), as shown in Table 3.
Median Values (Mdn), Interquartile Ranges (IQR), and Minimum and Maximum Values Concerning Perceived Discomfort When Using Retainer.

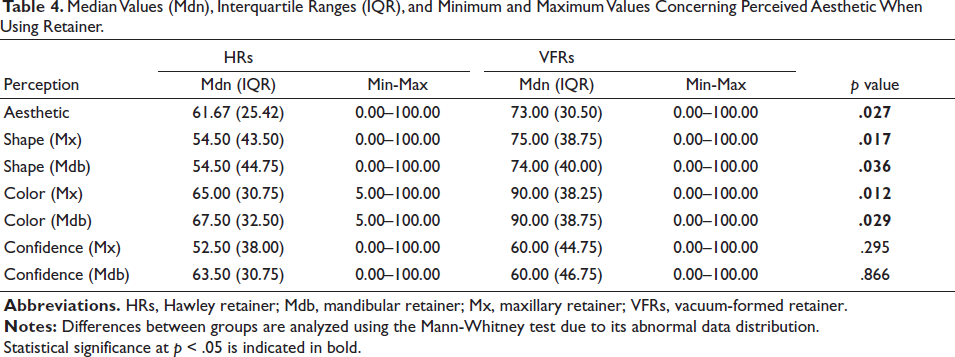
All participants, regardless of the group, preferred the aesthetic, shape, and color of the VFRs. Additionally, it was reported that the participants had higher confidence levels when using maxillary VFRs. In the HRs groups, higher values were observed only regarding confidence when using mandibular retainers. Statistically significant differences between groups were found in the perception of both maxillary and mandibular retainers’ aesthetic, shape, and color (p < .05). No statistically significant differences were found regarding the perception of confidence while wearing the retainers (p ≥ .05), as detailed in Table 4.
Median Values (Mdn), Interquartile Ranges (IQR), and Minimum and Maximum Values Concerning Perceived Aesthetic When Using Retainer.
Harms
No harm or undesirable effects was reported by the patients throughout the study.
Discussion
Main Findings in the Context of the Existing Researches
This descriptive-analytic study aimed to analyze the perceptions of patients who had finished their orthodontic treatment with fixed appliances for 6 months to 5 years, comparing their experiences when using removable HRs and VFRs. The importance of using qualitative methods to study patients’ perceptions has grown recently. Consequently, methods like focus groups, in-depth interviews, and questionnaires have been increasingly employed for research and audits to assess patient satisfaction. 26 Before the research, the questionnaire’s validity and reliability were evaluated, confirming its validity and reliability.
There was no significant difference (p ≥ .05) in this study in terms of patients’ comfort when using HRs and VFRs (Table 2). This finding aligns with a previous study that reported similar levels of discomfort among post-orthodontic patients, irrespective of the type of retainer used. 24 However, another study reported that patients felt more comfortable using the VFRs. 14 Discrepancies in results between these two studies could be attributed to differences in research methodologies and the interpretation of perception derived from the questions posed. This study evaluated the perception of comfort by considering average values of other related perceptions like pain, sharpness, pressure, and soft tissue cuts. Discomfort during orthodontic treatment can be perceived as a sensation of pressure, tension, pain, or a combination thereof. 27 Furthermore, previous studies treated the perception of comfort as a single question on the questionnaire, potentially leading to varied interpretations of comfort for each patient. 14 Pain is a highly subjective experience. 28 The perception of pain covers various multidimensional aspects, and its intensity and discomfort can be expressed in different ways. 29
Earlier studies evaluated patients’ perceptions only up to 6 months after debonding. In contrast, this study extended the post-treatment time interval from 6 months to 5 years. This longer timeframe allows patients more time to adapt to their retainers, potentially minimizing initial discomfort. However, this aspect remains significant, considering that 17.14% to 28% of patients choose their retainer based on perceived comfort. Comfort plays a pivotal role in improving patient adherence.30, 31 A significant correlation between patients’ comfort level and adherence to their retainer regimen was identified. 32
Patients who use HRs reported higher pain levels in both arches while wearing their retainers, although these differences did not attain statistical significance (p ≥ .05). Patients also experienced an increased level of pressure when using their mandibular HRs. These could potentially be attributed to the acrylic structure of HRs, which extends to cover the palatal and lingual areas up to the oral mucosa’s soft tissue, in combination with the metal wire components such as clasps and labial bows, creating a potentially more pressurized sensation for patients.
A previous study highlighted a notable increase in mandibular soft tissue cuts among patients using HRs. 14 Conversely, participants in the VFRs group reported greater senses of sharpness in both arches and increased occurrence of cuts on the maxillary soft tissue. These results may be attributed to the shape of the retainer. Moreover, the plastic edges of VFRs may not have a uniformly smooth texture, thus leading to friction-induced irritation in the oral cavity.
Patients’ aesthetic perceptions on the use of HRs and VFRs differed significantly (p < .05) (Table 3). This study concluded that VFRs were perceived as more aesthetically pleasing than HRs. Patients also preferred the shape and color of VFRs to HRs and the differences were statistically significant. These findings are consistent with previous studies, which similarly reported that patients favored the aesthetic appeal of VFRs while expressing disapproval for the labial bow wire present in HRs.14, 24, 25
The study found that patients reported higher confidence levels when using VFRs, particularly in the maxilla, compared to HRs. Although this difference did not attain statistical significance (p ≥ .05), it corresponds with prior research, indicating that the transparent visibility of VFRs increases patient confidence compared to HRs. Furthermore, HRs could potentially result in more significant embarrassment for patients. 24 Orthodontic appliances that are almost invisible have been associated with increased attractiveness. The degree of invisibility appears to correspond with the extent of social and aesthetic acceptability. 33
Limitations
In this study, the growing popularity of VFRs posed a challenge in recruiting participants who met the specific inclusion and exclusion criteria for the HRs group. Additionally, the study was conducted entirely online. Communication within the online space proved insufficient in conveying the significance of the study, resulting in a notable discrepancy between the number of respondents who completed the questionnaire and those who were initially contacted. Technical factors, such as internet signal strength, also emerged as a weakness of online questionnaire-based research.
The VAS method was used in this study to assess patients’ perceptions regarding the use of a retainer. The VAS method has frequently been employed to evaluate perceptions of pain, discomfort, and aesthetics in orthodontic treatment and various retainer studies.14, 22, 24, 27 However, the outcomes obtained using this method often show a broad range of values. The use of VAS presents challenges in maintaining uniformity of judgment across respondents at every point along the scale. Moreover, it is difficult to ensure consistent judgment levels among different respondents.34, 35 Abnormal data distribution can influence the wide range of results obtained.
Generalizability
The findings of this study were constrained by factors including the choice of questionnaires, retainer types and designs, and wear regimen. The study’s participants represented an expected range of patients seen at an orthodontic clinic. However, it is important to acknowledge that the study did not involve patients treated with removable appliances, highlighting a limitation in generalizing the results to all individuals undergoing orthodontic treatment.
Implication for Clinical Practice
Previous studies have indicated minimal differences in retentive abilities between HRs and VFRs.11, 12 Therefore, when selecting the appropriate retainer type for the retention phase, it remains essential to comprehensively evaluate patients’ final clinical conditions compared to their initial diagnosis. However, the results of this study underline the divergence in perspectives among post-orthodontic patients regarding the use of removable retainers; it is important to incorporate patient preferences into the decision-making process. Each patient should be individually assessed, considering various factors influencing their adherence to retainer usage. Successful compliance depends on a solid patient-orthodontist relationship, sufficient support, continuous patient education about the retainer regimen, and motivation and encouragement from the patient’s social environment. Furthermore, patients should be well-informed about the potential experiences they might encounter during retainer use over time. Noncompliance with the prescribed regimen may lead to discomfort, pain, and even relapse.
Future Research
Another article (Part II) will evaluate patients’ perceptions of acceptability and satisfaction using the same methodology and originating from the same patient cohort.
Conclusion
VFRs’ aesthetics, shape, and color were perceived as more favorable than HRs. No significant differences were found between the 2 types of retainers concerning patients’ perception of comfort, pain, sharpness, pressure, confidence, and soft tissue cuts while wearing the retainer.
Authors’ Contributions
AAL was involved in the design of the project and predetermined the expected outcomes, dealt with all the administrative procedure of the research and technical details of the project execution (sampling, questionnaire making, scheduling of data taking, and data input), drafting the manuscript, analysis, and interpretation of the data; BMS was involved in the design and conception of the project as well as overseeing the entire project, revising the manuscript critically for important intellectual content and gave the final approval of the version to be published; FJ was involved in providing editorial guidance and revising the manuscript critically for important intellectual content; All authors read and approved the final manuscript.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was given by Dental Research Ethics Commission (KEPKG) from Faculty of Dentistry, University of Indonesia and UI Dental Hospital (no. 68/Ethical Approval/FKGUI/IX/2022 and 035/UN2.F2.RSKGM/PPM.00/202).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
All participants have consented to the submission of the article to the journal.