
Abstract
Introduction
In view of the increased use of computers and mobile technologies in orthodontics, there is a need for evaluating the accuracy of commercially available cephalometric software.
Aim
This study compares the accuracies of computer-assisted tracing, smartphone tracing with the manual method of tracing in the pre-treatment lateral cephalograms of the orthodontic patients.
Materials and Methods
A total of 100 cephalograms, both digital and hard copies, were collected from the records available in the department archives. Hard and soft copies were used for obtaining values of 17 parameters for comparison between different groups. i.e (Manual, NemoCeph®, AutoCeph®, CephNinja®, OneCeph®)
Results
No statistical significance between groups for SNA, SNB, ANB, FMA, SN-GoGn, U1-NA Angular,linear, L1-NB Angular, linear, IMPA and interincisal angle (p=0.798, 0.583, 0.895, 0.059, 0.140, 0.680, 0.161, 0.327, 0.906, 0.940, 0.789). A significant difference was seen for parameters Eff-Mx,Mn lengths and differential, L1-Occlusal plane, WITS, NLA.(p=0.000, 0.004, 0.018, 0.004, 0.025). Suggesting the possibility of use of software for tracing instead of manual method.
Conclusions
All the software (NemoCeph®, AutoCeph®, CephNinja®, OneCeph®)as well as applications performed satisfactorily and these can be used instead of manual tracing.
Introduction
Orthodontic cephalometric evaluation methods have improved since Broadbent standardized the lateral cephalometric radiography technique in 1931. 1 Cephalometric tracing can be performed by both manual and computerized approaches. The manual technique was the only method available for an extended period of time. The main disadvantages of manual tracing are that it is time-consuming and possible for errors to originate in manual measurements performed with a protractor and a ruler.2, 3 The unprecedented evolution of computer technologies has paved way for digital programs in cephalometric tracings. The Dolphin imaging software® (Dolphin Imaging and Management Solutions, Chatsworth, California, USA), introduced in 1994, was the first digital cephalometric innovation employed in the orthodontic field. Since then, many other programs have been developed for digital cephalometric tracing. 2 Today, cell phones have undoubtedly become ubiquitous in daily life. As indicated in the 2014 Millard Brown study, this was conducted in 30 countries worldwide, mobile devices account for 47% of the total daily screen time. Moreover, among these devices, 35% are smartphones, the users of which spend 147 minutes per day interacting over their devices, making smartphones the leading most significant screen medium in the world. 4 Orthodontics has been using computer technologies in diagnosis, treatment planning, and data storage more than any other dental specialization. 2
Cephalometry is an integral component of clinical orthodontics and orthognathic surgery, which aims to evaluate the dentofacial proportions, to clarify the anatomic basis for a malocclusion, and analyze growth and treatment-related changes. 5 Manual cephalometric analyses are being primarily replaced by semiautomatic computer-based software, which enables direct landmark identification on screen-displayed digital images. 6 The recently introduced mobile apps facilitate automatic calculation of cephalometric measurements after landmark identification manually on mobile phones. 7 In view of the increased use of computer-assisted cephalometric programs and mobile technologies in orthodontics, there is a need for evaluating the accuracy of commercially available cephalometric software in order to allow the clinician to select the appropriate software. 8 Digital radiographic systems are becoming more popular, and they have several advantages over traditional cephalograms, including the ability to quickly determine treatment plans, perform measurements, eliminate chemical and associated environmental hazards, store images easily, and facilitate communication between providers. Furthermore, quick superimposition of serial radiographs and cost-effective radiograph duplication are achievable. 9
The present study intends to compare the accuracy of smartphone tracing, computer-assisted tracing with the manual method of tracing in the pre-treatment lateral cephalograms of orthodontic patients. The objectives are: (1) to compare which method of tracing is more accurate or nearer to that of manual tracing and (2) to compare between computer cephalometric software and smartphone tracing apps of different companies.
Materials and Methodology
This study was done at the Department of Orthodontics, Lenora Institute of Dental Sciences, Rajahmundry, Andhra Pradesh.
A total of 100 cephalograms, both digital and hard copies, were collected from the records available in the Department of Orthodontics & Dentofacial Orthopedics as per the inclusion criteria where all the cephalograms used had acceptable magnification (not more than 5–7% of magnification).
Initially, hard copies of 100 cephalograms were traced manually on tracing sheets by the primary operator. The computer cephalometric software used in this study were AutoCeph® v1.1.3 and NemoCeph® 2016. The digital cephalograms were opened in the respective software, and relevant landmarks were marked (Figure 1A, 1B).
(A–D) The User Interfaces of the Commercially Available Cephalometric Tracing Applications and Software. These photographs are screenshots taken from licensed versions of the softwares and applications by the authors.
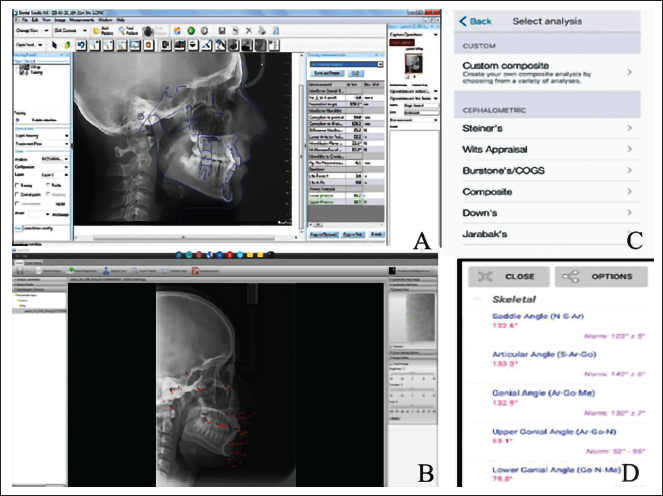
The smartphone apps used in this study were CephNinja® v 4.0 (IOS® platform) and OneCeph® (Android® platform). The digital cephalograms were exported to smartphones and the apps were used to locate the relevant landmarks (Figure 1C, 1D).
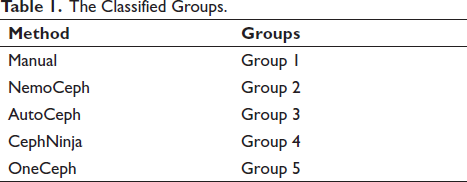
Each cephalogram was traced manually and in all four applications (viz. NemoCeph®, AutoCeph®, CephNinja®, and OneCeph®) by the same investigator (Figure 1A–D). A total of five groups were included in this study (Table 1).
The Classified Groups.
The lateral cephalograms were traced manually using matte lacquered polyester acetate tracing sheets with a sharp 3H pencil under the same illumination and the digital copies of the lateral cephalograms were transferred to the corresponding software/applications, and the relevant landmarks were identified.
In all the applications, the landmarks were identified by the same operator to eliminate inter-examiner bias.
The following parameters were used for comparison between the methods: (1) Angular parameters: (1) SNA, (2) SNB, (3) ANB, (4) FMA, (5) SN-GoGn, (6) U1-NA, (7) L1-NB, (8) L1-OP, (9) IMPA, (10) NLA, and (11) II angle
Linear parameters: (1) Eff-Mx, (2) Eff-Mn length, (3) Mx-Mn differential, (4) Wits AO-BO, (5) U1-NA, and (6) L1-NB
Statistical Analysis
All the statistical analysis were carried out by using IBM SPSS version 23.0 and MS Excel 2016. The descriptive data are presented as mean ± SD and percentages. Frequency distribution charts and tables are used to know the correlation of the means of the values obtained from the parameters in different groups. The p value was set at 95% of confidence interval. Analysis of variance (ANOVA) test was applied for testing the differences among different groups of data for homogeneity and post-hoc Tukey test was used to uncover specific differences between three or more group means when an ANOVA F test is significant.
Results
There was no statistical significance between groups for SNA, SNB, ANB, FMA, SN-GoGn, U1-NA Angular, U1-NA linear, L1-NB Angular, L1-NB linear, IMPA, and interincisal angle (p = .798, .583, .895, .059, .140, .680, .161, .327, .906, .940, .789) (Table 2).
Means and SDs of Cephalometric Measurements Obtained with Manual, NemoCeph, AutoCeph, Ceph Ninja, and OneCeph for all 17 Parameters and Their Corresponding p Values.
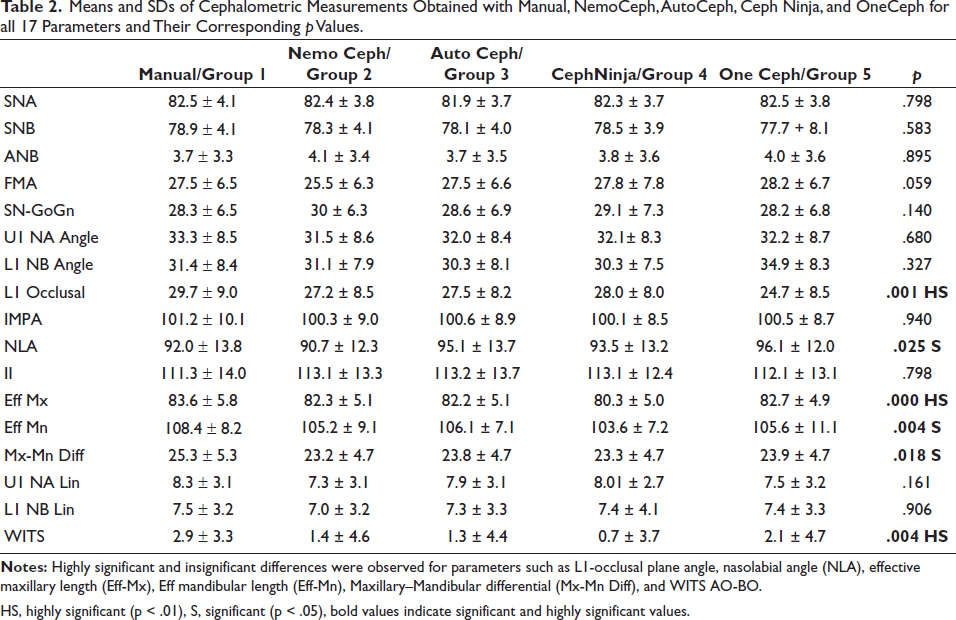
HS, highly significant (p < .01), S, significant (p < .05).
Effective maxillary and effective mandibular lengths showed a highly significant difference (p = .000, .004). and maxillary mandibular differential showed a significant difference between the groups (p = .018) (Table 1).
Table 3 represents the respective post-hoc comparisons between groups for Eff - Mx length and Eff - Mn length.
Post-hoc Table for the Parameters with Significant p Values.
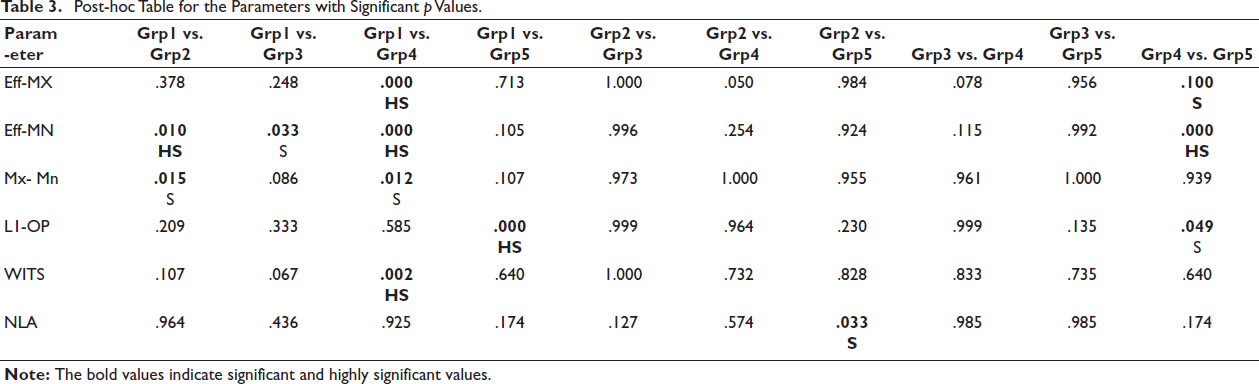
A significant difference in post-hoc comparison was seen in CephNinja group when compared to manual (p = .000) and OneCeph (p = .100) for Eff-Mx length (Table 3).
Post-hoc comparison for Eff-MN length groups showed a difference in NemoCeph, AutoCeph, and CephNinja groups when compared with manual (p = .010, .033, and .000, respectively) and when compared between CephNinja and Oneceph (p = .000) (Table 3).
The differential between MX-MN lengths was found to be significant between manual compared with NemoCeph and CephNinja (p = .015 and .012) (Table 3).
Table 2 represents the L1-Occlusal plane angle parameter showing a highly significant difference (p = .001). In post-hoc test, manual group when compared to OneCeph group showed the statistical difference (p = .000) and with Ceph Ninja with OneCeph (p = .049) (Table 3).
WITS appraisal showed a significant difference in the five groups (p = .004) (Table 2). Manual group when compared with CephNinja group showed a highly significant difference (p = .002) (Table 3).
A significant difference in NLA was seen in all five groups (p = .025) (Table 2), which was the result of a significant difference in the NLA values obtained between NemoCeph and OneCeph groups (p = .033) (Table 3).
Discussion
In view of the increased use of smartphones and computer-assisted cephalometric programs in orthodontics, there is a need for evaluating the accuracy of commercially available cephalometric software in order to allow the clinician to select the appropriate software.8 The present study provides a detailed analytical assessment of the accuracy of cephalometric tracing in the applications used (AutoCEPH® V1.1.3 and NemoCeph® 2016 in computer software and CephNinja® v3.10 on IOS devices, and OneCeph® v9 beta on Android devices).
The use of measurements was preferred to landmark identification because measurements are the end product of the cephalometric process and provide data for treatment planning. According to Santoro et al., 10 any investigation aiming to demonstrate the accuracy of digital cephalometrics should focus on significant factors, such as the use of measurements instead of identification of landmarks. Although earlier studies investigated landmark identification, recent research has focused on cephalometric measurements.
The cephalometric software programs can be either completely automated or semiautomated. 11 This study used semiautomated software. In semiautomatic software, location of landmarks is done manually on the computer screen, and then, the cephalometric analysis is performed by the computer. By using computer programs, the errors which result from drawing and measuring with a ruler and a protractor may be eliminated. 12
The increasing use of digital cephalometry has highlighted the need to evaluate the accuracy of these computerized software programs and compare them with the traditional manual measurement technique. Many studies have examined the performance of commercially available software and mobile apps used for cephalometric analysis. 13 Mobile applications have the potential to advance dentistry. Orthodontic clinicians and patients have employed a variety of smartphone apps relevant to orthodontics.14, 15
Results of the present study for parameters SNA, SNB, ANB, SN-GoGn, U1NA angle, and linear, L1NB angle, and linear and interincisal angle showed statistically no significant differences (p = .798, .583, .895, .140, .680, .161, .327, .906, .798, respectively) in comparison to all the five groups, which is consistent with the results obtained in the studies conducted by Sayar and Kilinc, 16 Mohan et al., 17 and Farooq et al. 18 on Steiner’s analysis (Table 2).
The parameters FMA (p = .059) and IMPA (p = .940) showed no statistically significant difference in the comparison between all five groups. These are consistent with the results obtained by Farooq et al. 18 and Khader et al. 19 (Table 2).
There was a significant difference in the measurement results obtained in our study for six parameters, namely, effective maxillary length (p = .000), effective mandibular length (p = .004), maxillo-mandibular difference (p = .018), Wits appraisal (p = .004), lower incisor occlusal plane (p = .001), and nasolabial angle (p = .025) (Table 2).
As statistically significant difference was found, post-hoc test for intergroup comparison was done for the abovementioned six parameters.
There was a highly significant difference in the effective maxillary length (p = .000) between manual tracing and CephNinja®, and a significant difference was observed (p = .010) between CephNinja® and OneCeph® app (Table 3).
With respect to effective mandibular length, a highly significant difference was found between manual tracing and CephNinja® app (p = .000). A significant difference was found between manual groups compared with AutoCeph® and NemoCeph® groups (p = .010, .033, respectively) (Table 3).
The difference in effective lengths of maxilla and mandible would have affected the Mx-Mn differential, which showed significant difference in manual and AutoCeph® groups and manual and CephNinja® groups (p = .015, .012). This may be due to the difficulty in identification of Condylion (Co) (Table 3).
Sekiguchi and Savara 20 mentioned that Condylion point is not easily located without auxiliary methods, as the point is overlapped by the basilar part of the occipital bone, parts of the middle cranial fossa, and structures around both sides of the glenoid fossa. Ongkosuwito et al. 21 mentioned that because of overlap between the right and left condyles in the lateral cephalogram, Condylion point is difficult to locate precisely.
Similar to our study, significant difference was observed in the effective mandibular length by Prabhakar et al. 22 A significant difference in the mandibular body length was found in the manual and computer tracing groups. This might be because of an error in identification of the corresponding landmark (Gnathion-Gn).
When manual tracing and AutoCeph® groups were compared, most of the parameters (Table 3) showed a positive agreement, which shows that AutoCeph® can be used instead of manual tracing, as it is user-friendly, time saving, and makes work easier, which is similar to the study by Sangroula et al.13
The results of this study when comparing manual method with the NemoCeph® (Table 3) cephalometric tracing showed a similar conclusion as that reported by Francisco et al. 23 The results showed that NemoCeph® may be used with reliability to make cephalometric measurements. There is no significant difference between the manual and Nemoceph® for most of the linear and angular cephalometric parameters. Our findings are consistent with the claims of different authors. Paixao et al. 2 and Chen et al. 3 found no significant differences in any of the measurements acquired with digital cephalometric tracing and manual cephalometric tracing.
When the manual method was compared with the phone applications CephNinja® and Oneceph®, a statistically insignificant difference in some of the parameters was found, which is consistent with a similar study by Livas et al. 5 who claimed that the phone applications CephNinja® and OneCeph® performed satisfactorily. However, they concluded that OneCeph® might be considered a slightly more valid alternative to Viewbox than CephNinja®. These claims by Livas et al. 5 showed similarity with our results (Table 3).
Our study also found a highly significant difference in the measurement of Wits AO-BO (p = .002) when compared between manual method and CephNinja® (Table 3). Similar result for Wits appraisal was found in the study by Farooq et al. 18
Aksakalli et al. 24 conducted a study in which they concluded that CephNinja® application was not reliable for measurement of the Wits appraisal, which is consistent and in agreement with our results.
With regards to lower incisor occlusal plane angle, a highly significant difference was found between manual and OneCeph® groups (p = .000) and a significant difference was found between CephNinja® and OneCeph® groups (p = .049) (Table 3).
It is well known that identifying points on the incisor apexes in both radiographic film and digital images is difficult. Due to the existence of grey shades that combine in that location, digital photographs can be harder. The challenge of locating such sites will be difficult in digital X-ray images, even when software tools such as magnification and filtering are used. 2 On the other hand, Albuquerque-Júnior and Almeida 25 and Chen et al. 26 claimed that computerized technique is reliable, as it exhibits lower error variance than the conventional method.
The difference in lower incisor occlusal plane may be due to the difficulty in locating the associated cephalometric points (apex of lower incisor, occlusal plane) as reported by Livas et al. 5
Baumrind and Frantz 27 and Lim and Foong 28 expressed tracing difficulties of the incisor position and variation in incisor angular measurements between the different tracing methods. But in our study, the interincisal angle (Table 2) showed an insignificant difference in all the groups proving that identification of the incisal apices was not difficult. So, the fault may be a difference in the location of the points for occlusal plane.
The main problem in obtaining the occlusal plane might have been due to difficulty in identification of the MB (Mesio-Buccal) cusp tips in OneCeph® and other applications, and anterior and posterior occlusal points in CephNinja® Prompter. So, these differences might have been the cause of the change in the occlusal plane and statistical difference in results for both the parameters.
All the results of this study are consistent with previous studies which compared manual tracing with computer software and smartphone apps (Tables 2 and 3).
Nowadays, digitizing X-rays is a preferred method to perform cephalometric measurements. As technology evolves, it becomes easier for professionals to adapt to routine tasks of clinical practice.
However, the disadvantages of desktop cephalometric software are that it can only be used on a desktop or a laptop, which might be expensive and requires an internet connection.
Mohan et al. 29 in a cross-sectional study conducted recently in 2021 compared digital cephalometry using OneCeph® application with manual method and the results concluded that the reliability and accuracy of the OneCeph® software application was at par with the manual tracing.
Overall, all the software as well as applications performed satisfactorily. Comparisons with manual tracing and intergroup comparisons were also carried out in this study. The satisfactory results suggest the potential use of easy-to-reach digital technology to make cephalometrics more readily accessible.
Conclusion
AutoCeph®, NemoCeph®, CephNinja®, and OneCeph® can be used as a reliable application and the overall performance was consistent with previous studies. Overall, all the software as well as applications performed satisfactorily.
The satisfactory results suggest the potential use of easy-to-reach digital technology to make cephalometrics more accessible.
In comparison with the manual tracing method of measurement, results showed that AutoCeph® and NemoCeph® software were equally efficient followed by OneCeph® and CephNinja®.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was granted by the Institutional Ethical Clearance Committee, Lenora Institute of Dental Sciences.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.