
Abstract
Ingestion of a foreign object forms a potential complication, be it any branch of dentistry. The present article describes an incident of accidental foreign body ingestion by an orthodontic patient while trying to consume a firm Indian delicacy leading to fracture, and eventual swallowing of a Transpalatal arch. The case was immediately referred to Department of Gastroenterology, wherein the major part of fractured arch was retrieved endoscopically from stomach while the minor part’s trajectory was followed on subsequent radiographs until it was eliminated. This report concludes in the management and further discussion of possible clinical complications, causes, and practices for prevention.
Introduction
The oral cavity in the human body acts as a common entry point to the airway as well as the digestive system. The potential of aspiration or ingestion of a foreign body (FB) is a ubiquitous health hazard in day-to-day activities. In the field of dentistry, it is all the more, where the oral cavity is primary area of therapeutic care delivery. The emanation of such occurrences could vary from simple pass out of the FB via stools to potential life-threatening situations like airway compromise or perforation of the gastrointestinal tract. Orthodontic components, being no different from a FB, could be accidentally ingested either intraoperatively during placement or postoperatively due to fracture or dislodgement. An important factor impacting the prognosis post swallowing of FB is the presence of sharp edges or pointed tips, which have the highest risk of complications up to 35%. 1
Case Report
Diagnostic Summary
A 19-year-old male patient who was undergoing fixed orthodontic mechanotherapy reported to the department with a chief complaint of sudden disappearance of a wire segment placed across the palate while he was having food. He allegedly complained that the wire segment got mixed with the food bolus and got accidentally swallowed. Initially, he had discomfort in throat while at rest and swallowing which eventually subsided within 20 min spontaneously. On initial evaluation of the patient 30 min post accidental swallowing, it was found that the Tanspalatal arch (TPA) which was inserted into the welded lingual sheath bilaterally on first permanent molars (toward correction of torque by incorporating third order bends) was missing (Figure 1).
Missing TPA.

To confirm the status of the broken wire segment, PA view of chest and abdominal radiographs was recorded (Figure 2), which revealed two wire segments in stomach confirming the diagnosis of accidentally ingested metallic foreign body.
PA Abdomen Showing Location of TPA.

Plan of Action
The case was immediately discussed with Department of Gastroenterology for removal of the foreign body as early as possible due to the presence of sharp ends in the broken wire segments which could have resulted in the traumatic mucosal ulceration or perforations while moving inside the GI tract along with bowel movements. Hence the gastroenterologist planned for immediate removal of the broken segment by upper GI endoscopy guided retrieval.
Intervention
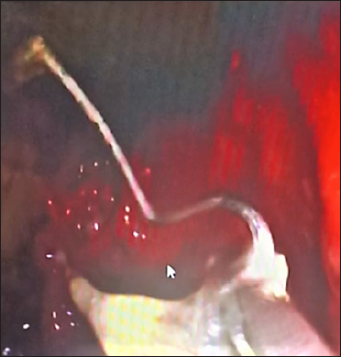
The balance remnant food was flushed out initially through gastric lavage using nasogastric tube. Endoscopically the major fragment of wire was located (Figure 3) followed by securing and retrieval was performed (Figures 4 and 5). The smaller fragment, by the virtue of its small size and difficult traceability was opted to be reviewed for passage and final elimination from alimentary canal through defecation (Figure 6). The patient was further followed up till the passage of wire into the sigmoid colon (Figure 7) and eventually out of the body as confirmed by the follow-up radiograph after 4 days (Figure 8).
Identification of Major Segment via Endoscopy.

Endoscopic Retrieval.
Retrieved Segment.

Minor Segment Located in Transverse Colon.

Minor Segment Located in Sigmoid Colon.

Elimination Minor Segment Elimination.

Discussion
Predilection of foreign objects entering in the oral cavity getting ingested is more (85.19%) as compared to the chances of getting aspirated (14.81%). 2 According to Ono et al., 3 dental foreign bodies accounted for 3.6%–27.7% of all foreign bodies ingested or aspirated, with ingestion being more prevalent than aspiration. Orthodontic appliances among the other dental appliances and materials, are the second most common dental foreign body to be ingested. 4
Though 80%–90% of ingested foreign bodies pass uneventfully. Various complications such as obstruction, aspiration, bleeding, perforation, fistulation, sepsis, and death may occur in balance number of cases. Ingested sharp pointed objects have the highest prevalence of perforation and those within the esophagus, stomach, or duodenum should be removed endoscopically on an emergency basis. 5
According to Eisen et al., 5 patients suspected of swallowing sharp-pointed objects must be evaluated to define the location of the object. Endoscopy of the upper and lower digestive tract is the gold standard for diagnostic and therapeutic purposes for foreign bodies that have entered the gastrointestinal tract, with a failure rate of less than 5% of cases. 6 The European Society for Gastrointestinal Endoscopy recommends immediate (<2 h, maximum 6 h after ingestion) therapeutic endoscopy for foreign bodies causing complete obstruction, sharp objects, and batteries or magnets. Urgent endoscopy (<24 h) should also be performed for other esophageal foreign bodies without complete obstruction. 7
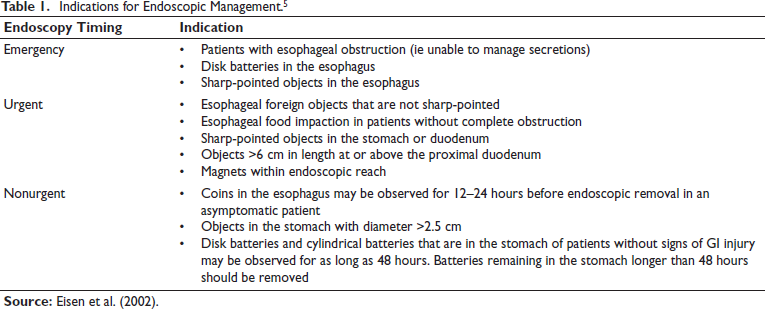
Although endoscopy should still be considered even in the cases of negative radiographic reports, considering radiolucent nature of certain objects, but in the present case the presence of FB was confirmed during initial evaluation of the radiograph only. Prompt endoscopic intervention is the gold standard for all complicated or high-risk situations, with particular relevance to sharp and pointed foreign bodies, such as dentures with protruding hooks, shaving blades, and open safety pins, which increase the danger of perforation. 8 Sharp-bodies getting lodged in the esophagus are considered as a medical emergency, which should be removed via direct laryngoscopy. A rigid or flexible endoscopic retrieval should be performed for objects lodged below the cricopharyngeus. Even though majority of sharp-pointed objects in the stomach pass out from GI tract without any risk of a complications, but an object that has passed into the stomach or proximal duodenum should be retrieved endoscopically if it can be accomplished safely. Also, foreign bodies crossing the digestive tract can cause obstruction or perforation, in addition, sharp objects at any point of impaction may cause perforation before extraction. 8 In case of inability to remove endoscopically, the foreign body may be followed with serial daily radiographs to document their passage, as was done in the present case for the smaller fragment of wire and surgical intervention is to be considered for bodies that fail to progress for three consecutive days. The indications for endoscopic management need to be done in the cases of FB ingestion as are given by Eisen et al. (Table 1).
Indications for Endoscopic Management. 5
In the present case, the sharpness of the ingested body was a high-risk factor which could have resulted in aforementioned complications including rare ones like esophageal hematoma and perforation, esophageal stricture, and sacral osteomyelitis. 9 The patient neither presented any history nor symptom contraindicating the endoscopic intervention. Hence the decision of urgent removal was taken up by the gastroenterologist for the removal of FB.
The specialty of orthodontics is prone to such incidents considering the complex appliances being placed in the oral cavity. Multiple sites of joints and ligations are always prone to breakage due to operator related lacunae in fabrication and/or insertion, or patient noncompliance. Prevention toward such an undesired incident intraoperatively includes preference for a brazed TPA wherever feasible. As in this case, where TPA with a lingual sheath was indicated, careful ligation should be done ensuring a secure fit, avoiding excessive tight ligation which could cause the breakage of ligature wire itself in course of mastication. A loose ligation should also be avoided which can cause the slippage of TPA. Also, patient education toward the inserted appliance, instruction toward strict following of dietary and masticatory restrictions and prompt review shall aid in timely identification as well as intervention toward prevention of situations which could potentially lead to emergencies.
Conclusion
The case report presents successful endoscopic retrieval of a major segment of an accidentally ingested broken TPA. The case was further followed-up towards natural egestion of the minor segment of TPA which could not be retrieved endoscopically through the gastrointestinal tract. The prompt intervention was justified considering the sharp end of the major segment which could have led to serious complications.
Footnotes
Declaration of Conflicting Interests
The authors, whose names are listed above, certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.
Acknowledgment
The authors would like to thank Department of Gastroenterology, Command Hospital, Pune.