
Abstract
Objective:
To evaluate and compare the effect of high-intensity light-emitting diode (LED) light-curing unit at different curing times on the shear bond strength (SBS), surface enamel loss, and degree of polymerization of a light-cure and dual-cure adhesive system.
Materials and Methods:
One hundred and twenty extracted human premolar teeth were divided into 2 groups— group 1 (light cure) and group 2 (dual cure), depending on the adhesive system used. These groups were further subdivided into 3 subgroups with 20 teeth each, depending on the duration of curing. A high-intensity LED curing unit was used to bond metal brackets onto the teeth. The samples were tested on a universal testing machine to measure the SBS. The samples were then observed under a simple microscope and modified adhesive remnant index scores were assigned. The bracket bases were mapped with energy-dispersive X-ray spectrometry to evaluate the amount of enamel present. Cured adhesive was scraped and was subjected to Fourier-Transform Infrared Spectroscopy to assess the degree of cure (%DC).
Results:
An increase in curing durations increased mean SBS values, %DC, and calcium-phosphorous ratios (Ca:P). Similarly, these parameters were higher for dual-cure subgroups when compared to light-cure subgroups.
Conclusion:
High-intensity LEDs can be used successfully for bonding orthodontic brackets with reduced curing duration. These LEDs help to reduce chairside time and can minimize damage to enamel without compromising bond strength.
Introduction
The concept of direct bonding of orthodontic attachments was introduced by Newman in the year 1965. 1 This technique resulted in enhanced patient comfort, esthetics, better oral hygiene, and reduced clinical chairside time. 2 Light-cured composites have the advantages of increased working time and higher initial bond strength, thereby enabling accurate bracket positioning and immediate placement of archwires. 3 Later, dual-cure composites were developed in an attempt to overcome the problems of limited depth of cure seen in light-cured composites.4, 5
The time needed for photopolymerization of orthodontic brackets has been a major concern in orthodontics. Recent advances in light-curing technology have made it possible to increase light power density and thus reduce the duration of exposure without compromising bonding efficacy. 6 Light-emitting diode (LED) light-curing units have been the choice to cure orthodontic resins due to their brief durations of curing. 7 Research into LED-curing units to achieve desired power output at reduced curing durations resulted in the development of the third-generation LED lights. They had high irradiance levels in the range of 1,000 mW/cm 2 to 3,000 mW/cm 2 and so were used for brief durations of 3 s to 6 s. 8
Bond strength of orthodontic brackets depends on the degree of cure (DC) of an adhesive, which in turn is affected by light intensity, curing time, and the type of adhesive used.9–11 Reynolds 12 suggested that a minimum bond strength of 6 MPa to 8 MPa was needed for most clinical orthodontic applications. Although increased bond strength of an orthodontic adhesive is often desirable, bond strength values greater than 9.7 MPa have shown to cause enamel fractures. 13
However, to date, there are no studies in the literature determining the effect of high-intensity curing light on the shear bond strength (SBS), debonding interface distribution, and DC of dual-cure composite systems. Hence, in an effort to provide some complimentary information on high intensity-curing lights, the aim of this study was to evaluate and compare the effect of high intensity LED light-curing unit at different curing times on the SBS, surface enamel loss, and degree of polymerization of 2 different orthodontic adhesive systems.
Materials and Methods
Sample Distribution.

Bonding Procedure
Stainless steel premolar brackets with double mesh base were bonded onto the teeth using a light-cure adhesive (ENLIGHT; Ormco Corporation) and a dual-cure adhesive (Phase II Dual Cure; Reliance Orthodontics). The adhesives were photopolymerized using an LED light-curing unit (iLED; Guilin Woodpecker) in high-intensity mode for 3, 6, and 9 s depending on the subgroup (Table 1). Following bonding, the teeth were stored in sealed containers for 24 h.
Debonding Procedure
All the samples were loaded into a universal testing machine (Instron Universal Testing Machine; Autograph Model AGS 10 ANG) (Figure 1) with long axis of the specimen kept perpendicular to the direction of applied force. Bond strength was determined in shear mode at a crosshead speed of 0.5 mm/min until the brackets debonded. Maximum force required to debond the bracket was recorded in MPa.
Instron—Universal Testing Machine.

Assessment of Adhesive Remnant Index
The debonded specimens were examined at 10× magnification under a simple microscope and were assigned a modified adhesive remnant index (ARI) value.
14
The index uses 6 scores:
Score 0: No adhesive present on the bracket base. Score 1: Less than 25% of adhesive left covering the bracket base. Score 2: A total of 25% to 50% of adhesive left covering the bracket base. Score 3: A total of 50% to 75% of adhesive left covering the bracket base. Score 4: A total of 75% to 100% of adhesive left covering the bracket base. Score 5: A total of 100% of adhesive left covering the bracket base.
Energy Dispersive X-ray Spectrometry
The bracket bases were mapped with energy-dispersive X-ray spectrometry (EDX/EDS Oxford Instruments INCA x-act) (Figure 2) to evaluate the amount of enamel present and the distributive percentages were recorded.
Energy Dispersive X-Ray Spectrometer.

Fourier Transform Infrared Spectroscopy
Cured adhesive bonded on to the etched enamel surface was scraped with a BP blade after debonding from the base of the brackets and from the debonded teeth surfaces. Scrapings were collected and subjected to Fourier Transform Infrared Spectroscopy (FTIR) (Thermo Nicolet Nexus 670 FTIR) (Figure 3) to assess the DC.
Fourier Transform Infrared Spectrometer.

Statistical Analysis
The data was subjected to statistical analysis and tabulated. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS version 22.0). Descriptive tests were performed for scale data, two-way ANOVA, and Tukey multiple post-hoc for intergroup comparison. The dependent variables in the two-way ANOVA were the SBS, mean calcium-phosphorous ratios (Ca:P), DC, and surface enamel loss, whereas the independent variables were the type of curing light used, adhesive system used, and duration of curing. The normality of the data was assessed using Shapiro-Wilk test.
Results
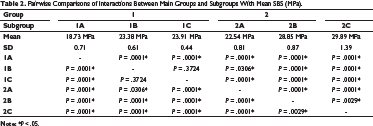
Shear Bond Strength
Pairwise Comparisons of Interactions Between Main Groups and Subgroups With Mean SBS (MPa).
Adhesive Remnant Index
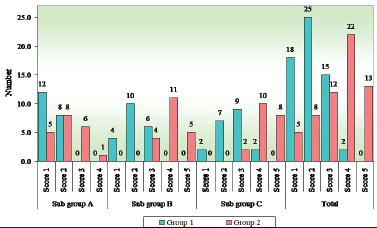
Figure 4 represents the modified ARI scores of groups 1 and 2. The mean ARI scores were higher for group 2 (dual cure) for a given duration of cure. Subgroups 1C and 2C (9 s) showed higher ARI scores (4 and 5) compared to other subgroups.
Modified ARI Scores for Groups 1 and 2.
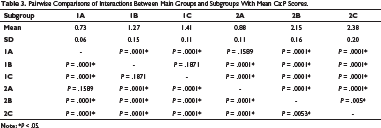
Elemental Composition
Pairwise Comparisons of Interactions Between Main Groups and Subgroups With Mean Ca:P Scores.
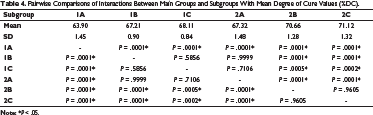
Degree of Cure
Pairwise Comparisons of Interactions Between Main Groups and Subgroups With Mean Degree of Cure Values (%DC).
Discussion
Advances in orthodontic materials, especially mechanotherapy and biomechanics research, have had an impact on orthodontic practice. The search for efficient materials and convenient techniques to improve the quality of treatment and to reduce the treatment time has made significant progress. 15
Two important features of orthodontic bonding materials, SBS and degree of conversion, were tested in this study. Light output intensity, adhesive composition, and exposure time are the main factors that affect the SBS and degree of polymerization.4, 16–18 The manufacturers claim that the new high-intensity LED light-curing units combine all the advantages of their predecessors, maximizing bond strength and degree of polymerization with a considerable reduction in exposure time. 8
Üşümez et al 19 suggested that an irradiance of at least 400 mW/cm 2 for 60 s is required for curing a 1-mm composite sample. Mavropoulos et al 20 reported that an exposure time of less than 4 s, irrespective of the power density, could not guarantee sufficient bond strength. However, Staudt et al 21 suggested curing durations of 3 s and 6 s for orthodontic bonding while using a high-power light source and Amato et al 22 suggested that the curing time can be reduced to 6 s by using 760 mW of power to achieve a satisfactory DC. The LED curing unit used in this study had a light intensity of over 2,000 mW/cm 2 which was measured using a radiometer provided by the manufacturer (Figure 5). Since the intensity of the curing unit exceeded the minimum intensity suggested, curing durations of 3 s, 6 s, and 9 s were evaluated.
Radiometer.

Ideally, the bond strength needs to be optimum rather than too high or too low. A study conducted by Reynolds 12 suggested that a minimum bond strength of 6 MPa to 8 MPa was required for orthodontic bonding. Excessive bond strength increases the risk of enamel damage during debonding and lesser bond strength results in frequent bond failures during the course of treatment. 4 Previous studies have reported an increase in the SBS and DC for dual-cure adhesives in comparison to light-cure adhesives when cured with a conventional LED light-curing units.4, 20 Results of the present study revealed a significant increase in SBS when the duration of cure was increased from 3 s to 6 s in both the groups. When the curing durations were further increased to 9 s, there was a statistically significant increase only in the dual-cure group. The findings in the light-cure group were similar to the findings of Swanson et al 17 and Palomares et al. 18 For a given duration of cure, SBS values of dual-cure subgroups were significantly higher than the light-cure subgroups. The results of Verma et al 4 concur with this finding.
The %DC for a resin is defined as the extent to which carbon double bonds (C=C) of the monomer are converted into carbon single bonds (C–C), to form polymers during the polymerization reaction.23, 24 The FTIR spectroscopy technique employed in this study to investigate the degree of conversion is an essential surface analytical method. The increase in the bond strength values obtained in the current study may be explained by the recorded FTIR spectroscopy values. There was a significant increase in the %DC upon increasing the curing duration from 3 s to 6 s in both the groups. There was no significant difference in the values of the light-cure subgroups when the curing duration was increased from 6 s to 9 s, which was similar to the changes in the SBS values. These findings were similar to those of Niepraschk et al. 25 In the dual-cure group, similar to the findings of SBS comparison, there was a significant increase in the %DC when the curing time was increased from 6 s to 9 s. In the present study, for the same curing time, the dual-cure subgroups had a significantly greater %DC than the light cure. These findings are in accordance to the findings of Eliades et al. 23
The main components of hydroxyapatite are Ca and P; hence, these elements were mainly monitored in the present study. The amount of calcium on the bracket base which is indicative of damage to enamel can be quantified in terms of percentage using EDX. The results of this study revealed that with an increase in the curing duration, there was an increase in the Ca:P ratio suggesting enamel loss during debonding. In both the groups, the 3-s subgroups showed significantly lower Ca:P ratios when compared to the 6 s and 9 s subgroups. When the SBS values were compared to the Ca:P ratios, a positive correlation was found suggesting that greater enamel damage occurs with increase in bond strength.
Adhesion has two aspects—one to the tooth surface and the other to the bracket base. Therefore, evaluation of the ARI scores provides information on the site of bond failure as either at the bracket-adhesive resin interface or at enamel-adhesive resin interface. The results of the light-cure subgroups and 3 s dual-cure subgroup were in accordance with the results of previous studies, which reported that majority of the bond failures occurred at the tooth-adhesive interface suggesting a stronger bond between the adhesive and bracket.4, 26–31 However, the results of 6 s and 9 s dual-cure subgroups varied from those of previous studies.4, 26–31 A total of 80% to 90% of brackets in the 6 s and 9 s dual-cure subgroups had modified ARI scores of 4 and 5, suggesting a stronger bond between the tooth and adhesive. This variability could be due to the use of a high-intensity curing light for polymerization.
In this study, a positive correlation was found between all the four parameters—SBS, DC, Ca:P, and ARI scores. Even though dual-cure subgroups at 6 s (2B) and 9 s (2C) and light-cure subgroup at 9 s (1C) exhibited greater bond strength and DC, they also had greater amount of enamel loss. Light-cure adhesive at 3 s (1A) showed least enamel loss, but the bond strength achieved was less when compared to other combinations. Thus, based on the findings of this study, use of a light-cure adhesive or a dual-cure adhesive with a high-intensity curing durations of 6 s (1B) and 3 s (2A) respectively can be recommended to prevent significant amount of enamel loss without compromising bond strength. High-intensity curing lights with reduced curing durations provide an additional advantage of minimizing the chairside treatment time.
Conclusions
Increase in curing time of a high intensity LED light-curing unit increased the SBS, DC, and surface enamel loss.
Dual-cure adhesives produced better SBS and greater DC but had increased susceptibility to enamel fractures when compared to the conventional light-cure adhesives under similar conditions.
Light-cure adhesive cured at 6 s and dual-cure adhesive cured at 3 s using a high-intensity LED light-curing unit could be recommended for bonding brackets to reduce chairside treatment time and potential damage to the enamel surface without compromising bond strength.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.