
Abstract
Purpose:
Efficacy evaluation of casein phosphopeptide amorphous calcium phosphate complex (CPP-ACP), casein phosphopeptide amorphous calcium fluoride phosphate complex (CPP-ACFP), fluoride mouthrinse, and fluoride containing toothpaste as compared to control group for the remineralization of white spot lesions (WSLs) in orthodontic patients with fixed brackets in an in vivo study.
Methods:
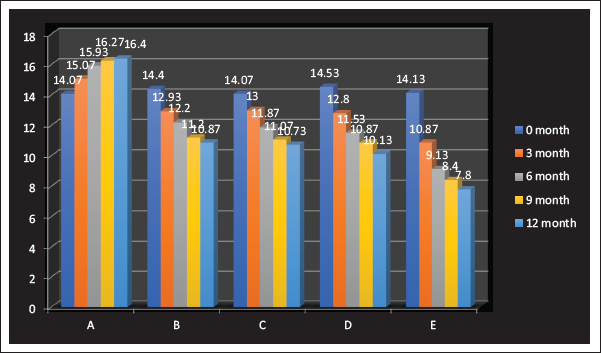
Seventy-five subjects with WSL determined by DIAGNOdent were randomly divided into 5 groups. The WSLs DIAGNOdent values for 0, 3, 6, 9, and 12 months were tabulated and subjected to statistical analysis.
Results:
Among the groups, the remineralizing potential of fluoride mouth rinse, fluoride containing toothpaste, and CPP-ACP were similar; however, CPP-ACFP value was superior in comparison to all other groups.
Conclusion:
The CPP-ACFP technique is highly beneficial for the remineralization of WSL in an orthodontic patient when compared to fluoride mouth rinse, fluoride-containing toothpaste, and CPP-ACP paste.
Keywords
Introduction
Dental caries occurs as a result of destruction of tooth structure by acid produced during the process of fermentation of carbohydrates by acidogenic oral bacteria. There exists a delicate balance between the demineralizing and remineralizing phases at the tooth microenvironment. Prolonged multiple exposures to cariogenic food substrates result in an imbalance in this process leading to formation of an early enamel lesion which may progress into caries or may remain stable and remineralize with time in plaque with a suitable composition. Currently, with the increase in preventive dental care and awareness, the progression of caries is slow in the majority of individuals. This has resulted in an increase in research that focuses on early diagnosis and treatment of caries at the precavitation level.
Prevalence of enamel demineralization adjacent to orthodontic brackets is as high as 50% to 96% in patients.1, 2 Remineralization after fixed appliance removal does not always occur. 3 Incidence of white spot lesions (WSL) is higher in orthodontic patients when compared to those who did not undergo orthodontic treatment even 5 years after treatment. 4 Orthodontic WSL develop and progress more rapidly than conventional smooth surface lesions. 5
There are numerous published studies on the topic of remineralization of WSL, but few studies have focused specifically on the performance of various treatments in the masking of WSLs. The proposed mechanisms of action of fluoride, which remains the mainstay of caries prevention, include inhibition of demineralization, enhancement of remineralization, and inhibition of plaque micro-organisms. Recently, casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) nanocomplexes were developed as an adjunct to fluoride therapy, and for the effective delivery of bioavailable calcium and phosphate to enhance remineralization under normal conditions.
Mouthrinse containing a combination of CPP-ACP and fluoride may deliver higher levels of fluoride to the enamel than a plain fluoride rinse, thus making them more insoluble.6, 7 The increased benefit due to the synergistic effects of CPP-ACP and fluoride has led to the manufacturing of Tooth Mousse Plus® (TMP), that incorporates 900 ppm of fluoride along with the 10% CPP-ACP. While the effects of combining different levels of fluoride with CPP-ACP have been demonstrated in different studies, the effectiveness of this product (10% CPP-ACP + 900 ppm F) was demonstrated in an in vitro study on bovine teeth, 8 when applied as a 30% diluted solution for 10 days. However, till date there is lack of any clinical evidence or research or records in the current literature stating above facts and no study till date has been carried out in Indian population to prove this finding with a significantly large sample size. Thus, the present in vivo study was undertaken to assess the WSL and enamel remineralization in orthodontic patients with fixed brackets using fluoride mouth rinse, fluoride containing toothpaste, CPP-ACP paste, and CPP-ACP paste containing fluoride (CPP-ACFP).
Materials and Methods
A prospective study was conducted in the Department of Orthodontics & Dentofacial Orthopaedics, Loni, from January 2016 to October 2017. Ethical approval from relevant committee was obtained.
Materials
One hundred and fifteen patients were screened to participate in the study, Out of these, 21 patients did not meet inclusion criteria. The remaining 19 patients did not give consent for the study. Finally, 75 participants aged 14 to 23 years were selected in this study with the mean age of 17.8, of which 44 were males and 31 were females. All participants were recruited from patients treated with fixed orthodontic appliances in the Department of Orthodontics at Loni. The sample was further divided into 5 groups of 15 subjects each.
Patient Inclusion Criteria
Patients undergoing fixed orthodontic treatment between 14 and 23 years, with good general health, with no proven or suspected milk protein allergy and/or with protein allergy and/or sensitivity, or allergy to benzoate preservatives.
Patients undergoing treatment with fixed appliances for at least 1 year and having at least 1 clinically visible WSL on the facial surface of a maxillary anterior tooth that had not undergone any type of remineralization/demineralization regimen.
Patient Exclusion Criteria
Patients with high DMF index and with severe systemic diseases or syndromes.
Patients living in an area where the water supply was fluoridated.
Patients failing to satisfy the inclusion criteria.
Patient with enamel diseases or demineralization.
Informed written consent for the participation of all eligible participants was obtained.
Methodology
Seventy-five patients were selected based on the inclusion criteria and were randomly assigned to the control and all treatment groups (n = 15 per group). Oral hygiene instructions were given in verbal and written form to the participants and to the responsible adult to facilitate and reinforce compliance. Instructions were also given that other sources of fluoride (environmental, supplements, professional, or other dental products) should be avoided during the study period.
Participants were explicitly instructed not to rinse their mouths after application and not to eat or drink for at least 30 min.
Compliance was checked at each visit to assess the frequency of brushing and application of the study paste in all groups. Furthermore, subjects were asked to bring their study paste to each visit to monitor usage level.
Evaluation of White Spot Lesions
Following recruitment, baseline characteristics were assessed. Teeth were cleaned with a prophylaxis brush without paste. Using a dental light reflector, visual inspection of all tooth surfaces for WSLs was undertaken, initially with wet tooth surfaces and again after 5 s of drying with a gentle air stream. Multiple lesions were recorded per tooth by DIAGNOdent (Figure 8).
Laser fluorescence (LF) examination for each lesion was performed using DIAGNOdent. It operates with a diode laser having a wavelength of 655 nm and 1 mW peak power. Sound enamel does not fluoresce at this wavelength, but caries and bacteria do. Probe A was used on the occlusal surfaces because of its comparatively narrow tip (Figure 7), which allowed superior access into the pits and fissures, over the wider-tipped. Probe B was used on the smooth surfaces. The instrument was calibrated according to manufacturer’s instructions. Under cotton roll isolation and after air drying with an air syringe, the DIAGNOdent probe was placed perpendicular to the test site and rotated along the lesion to scan the area completely (Figure 6). Three measurements were taken and averaged to give the final test value. Measurements were taken at baseline and at 3, 6, 9, and 12 months after starting treatment (Figure 9). All measurements were conducted by a single orthodontist; calibration was done before every measurement. Changes occurring in WSL were observed and recorded properly in each interval of 3, 6, 9, and 12 months after treatment (Figure 10).
Comparasion of Groups at Different Ttime Intervals.
Fluoride Containing Mouthwash.

Fluoride Containing Toothpaste.

CPP-ACP Paste.

CPP-ACFP Paste.

DIAGNOdent Pen.
DIAGNOdent Tip.
KaVo DIAGNOdent Kit.

White Spot Lesions During Orthodontic Treatment.

White Spot Lesions After Debonding.

Results
The data was coded and entered into Microsoft Excel spreadsheet. Analysis was done using SPSS version 20 (IBM SPSS Statistics Inc) Windows software program. Descriptive statistics included computation of means and standard deviations. The repeated measures analysis of variance (ANOVA) (for quantitative data within three groups) with post hoc Bonferroni test (to make more intragroups comparison) was used for comparison of all clinical indicators. Level of significance was set at P ≤ .05 (Figure 1).
Discussion
There is a potential of remineralization of enamel lesion demonstrated by spontaneous disappearance of the WSL in young individuals as a result of the remineralizing ability of saliva. 9 Subsequently, many studies were conducted to assess the effect of various preparations of calcium, phosphate, and fluoride on enamel remineralization.
The plaque retentive properties of the fixed appliances predispose the patient to an increased cariogenic risk. 10 Recently, many authors have advocated CPP-ACP and CPP-ACP-F as the preventive agents for WSL occurring during orthodontic treatment.11, 12
Noninvasive analysis methods are required for this to be achieved, and LF technologies such as DIAGNOdent represent a promising method for monitoring the progression of caries lesions.13-18.
Regular topical application of fluoride varnish is currently the gold-standard method for protecting teeth against the development of WSLs and for reversing demineralization. Fluoride varnish has the advantage of being independent of patient compliance and is quick and simple for a dentist to apply. It has been shown to be especially useful in patients undergoing fixed orthodontic treatment. 19
In this 12-month longitudinal study that we performed, evaluation of WSLs with 2 CPP-ACP-based treatments was compared with the gold-standard treatment of professionally administered high-concentration fluoride varnish. We noted that each treatment was to some extent effective, but has also recorded some interesting findings that suggest that each has particular strengths and weaknesses depending on the nature of the lesion.
Many in vitro studies have proved that CPP-ACP has a remarkable ability to remineralize caries. While in 1 study authors have concluded that although CPP-ACP can remineralize surface lesion, it is not effective in remineralizing the early enamel caries at the subsurface level.
The present study allowed quantification of the remineralization potential of 4 agents, and the determined sample size was adequate to show the difference. The age group of the subjects belonged to the high caries attack period and thus added relevance to the outcome measure. 20 Surface lesions were selected for this study, for better identification and reproducibility. 21
The DIAGNOdent system is highly sensitive compared to radiographic methods of occlusal caries detection. The system has a high degree of specificity and sensitivity in detecting carious lesions restricted to enamel and sensitivity in detecting occlusal WSL.13, 16, 22
A recent systematic review has stated that the quantity and quality of clinical trial evidence is insufficient to make conclusions regarding the long-term effectiveness of casein derivatives, specifically CPP-ACP, in preventing caries in vivo and treating dentin hypersensitivity or dry mouth.23, 24 The current evidence on clinical efficacy of remineralizing WSL has been addressed by the following studies.
CPP-ACP, when used alternating with fluoride mouth rinse, was significantly better in promoting regression of WSL after orthodontic treatment when compared to fluoride alone. 13 This supports our study result in which CPP-ACPF (group E) is more effective then CPP-ACP (group D).
The improvement with CPP-ACP was not superior to the “natural” regression following daily use of fluoride toothpaste. 25 This also supports our study in which remineralizing potential of group B (fluoride mouth rinse), group C (fluoride toothpaste), and group D (CPP-ACP) is nearly similar after 12 months of study.
Another study by involving 2,720 subjects with approximal lesions found that proximal caries in subjects chewing CPP-ACP gum had slowed progression and increased regression. 26 A randomized, double-blinded cross-over study showed beyond doubt that the combination of CPP-ACP with fluoride was much superior to all other formulations. 6
The CPP-ACP technique has also been demonstrated to significantly increase the levels of calcium and phosphate ions in supragingival plaque when delivered in a mouthrinse and to promote the remineralization of enamel subsurface lesions in situ. 27 These studies highlight the importance of the CPP in stabilizing the high levels of calcium and phosphate ions but also in delivering the ions to the tooth surface. It has been reported that the CPP-ACP complexes interact with fluoride ions to produce a novel ACFP phase. The CPP-ACFP treatment (group E) appeared to reduce caries lesion severity more rapidly than the CPP-ACP treatment (group D). This increased rate of remineralization could be caused by the presence of unstabilized calcium, phosphate, and fluoride ions in the formulation, because these will readily form fluorapatite in the enamel surface layer. In the absence of CPP, this reaction is undermined by the rapid formation of calcium phosphate phases, 28 but when stabilized by CPP, these ions can diffuse down into the subsurface lesion and form fluorapatite. 6
Furthermore, some experimental studies have determined that CPP-ACFP solutions may have higher remineralization capacity than CPP-ACP at acidity levels below pH 5.5, suggesting that it may continue to function even in highly acidic environments. 29 Our results appear to confirm the superiority of CPP-ACFP to both CPP-ACP and fluoride varnish in the immediate to very short term (3 months) after treatment initiation. Moreover, CPP-ACFP generates a significantly greater decline in caries lesion severity than fluoride varnish after 12 months of use, suggesting that daily use of this product may also provide better protection than the current gold-standard treatment over the medium term.
Fluoride, when added to CPP-ACP, gives a synergistic effect on remineralization of early carious lesion.11, 12 It has been observed in an in vitro study that the remineralization effect of fluoride is confined to superficial enamel layers, leaving the deeper sections in a demineralized state. 30 Hence, it may not be advisable to use fluoride preparations alone for treating WSL. Cochrane et al found that the levels of remineralization produced by the CPP-ACFP and CPP-ACP solutions were similar from pH 7.0 to 6.0.
However, the CPP-ACFP solutions exhibited significantly greater remineralization than the CPP-ACP solutions at pH 5.5, 5.0, and 4.5. The difference in remineralization between CPP-ACP and CPP-ACFP at the lower pH values was attributed to the presence of fluoride31.
In the present research, group B and group C have shown remineralization in 3 months with improved DIAGNOdent scores of 12.93 and 13, respectively. Fluoride is found to be nearly effective as CPP-ACP paste. All fluoride-containing groups showed better or nearly the same performance than CPP-ACP alone.
In agreement with previous studies,15, 32, 33 it is likely that clinically visible changes in the WSLs will only be detectable over study periods longer than 3 months.
Limitation of Study
First, a larger sample size would have allowed a more desired level of precision. Second, patient’s compliance. Third, human error. WSL measurement taken from a DIAGNOdent is variable, even though in the study intra- and interexaminer reliability was found to have no significant difference. The intraclass correlation coefficient for intraexaminer reliability was 0.76. The intraclass correlation coefficient for interexaminer reliability was 0.82. The principal limitation of this method is that an increased reading could also mean disturbed tooth development or mineralization as well as deposits of calculus or organic material,34, 22 and sensitivity in detecting occlusal WSL. 16
Conclusion
The use of toothpastes containing CPP-ACFP such as GC Tooth Mousse™ Plus has been shown to reduce demineralization caused due to orthodontic treatment and promotes remineralization. CPP-ACP pastes in combination with regular fluoride toothpaste should be recommended for patients undergoing orthodontic treatment who are at high risk of demineralization or who have demonstrated early signs of WSL formation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.