
Abstract
Background:
The COVID-19 pandemic has caused many changes in the practice of orthodontics, with the main focus being prevention of cross-infection. Clinical audits can help assess the extent to which practices/practitioners adhere to standard cross-infection control protocols, thereby providing scope for improvement resulting in better treatment outcomes.
Objective:
Phase 1—to investigate the type of cross-infection control procedures being followed by orthodontic residents of 5 dental institutes in Hyderabad city and compare them to recommended guidelines. Phase 2—after identification of the shortcomings, analyzing how re-education and revision of guidelines can lead to improvements in cross-infection prevention protocols.
Methodology:
Orthodontic residents of 5 dental institutes were observed with regard to their routine infection control practices, which were compared to a set standard. A second audit cycle was conducted on the same clinicians after a seminar where they were encouraged to work on shortcomings at their workplace. The results from the 2 audit cycles were then compared to assess differences.
Results and Conclusion:
While most clinicians were aware of the recommended cross-infection control guidelines, few steps were neglected while in practice. Comparisons between the 2 audit cycles revealed definite improvements.
Introduction
Infection control practices of an orthodontic office are generally reflective of the standard of health and patient care being provided. In this fast-developing world where information can be obtained with the click of a button, one of the main reasons for patients to seek treatment at a certain place is the belief that standards of cross-infection control are met. This is especially relevant in the current time, when the world is struggling with the rapid spread of the SARS-CoV-2 virus. The highly infectious nature of this virus has caused apprehension in people’s minds with regard to seeking basic health care, or orthodontic treatment, which is primarily esthetically driven and deemed “nonessential” by the general population.
In this scenario, ensuring safe cross-infection free orthodontic care for our patients has become very critical. An effective way to evaluate the standard of services rendered in a clinical setup is to conduct an “audit.” The Oxford Dictionary defines the term “audit” as an official inspection of an organization’s accounts, typically by an independent body.1 When applied to clinical practice, audits can be helpful in quality assessment, quality improvement, and bringing light to lacunae in the health-care service process of a place or practitioner.2 A clinical audit, therefore, can be regarded as a means of comparing the personal activity of a practitioner with expected published standards.3
Clinical audits are said to have originated in 1750 BC when King Hammurabi of Babylon initiated an audit for health workers by instructing them to measure the level of their care against some set standards. Florence Nightingale, during the Crimean war (1853–1855), is also credited to be one of the originators of clinical audits, when she conducted an audit with detailed statistical calculations to help improve sanitary conditions helping to bring down mortality rate from 40% to 2%.4 According to World Health Organization (WHO) statistics, India has witnessed more than 33 million cases of COVID-19 since the breakout of the pandemic, with more than 4 lakh people succumbing to the virus or comorbidities caused due to it. These numbers are bound to increase as the third wave is anticipated. At such a time, auditing our infection control practices can be an eye-opener and a necessary step to ensure the safety of clinicians, staff, and patients.
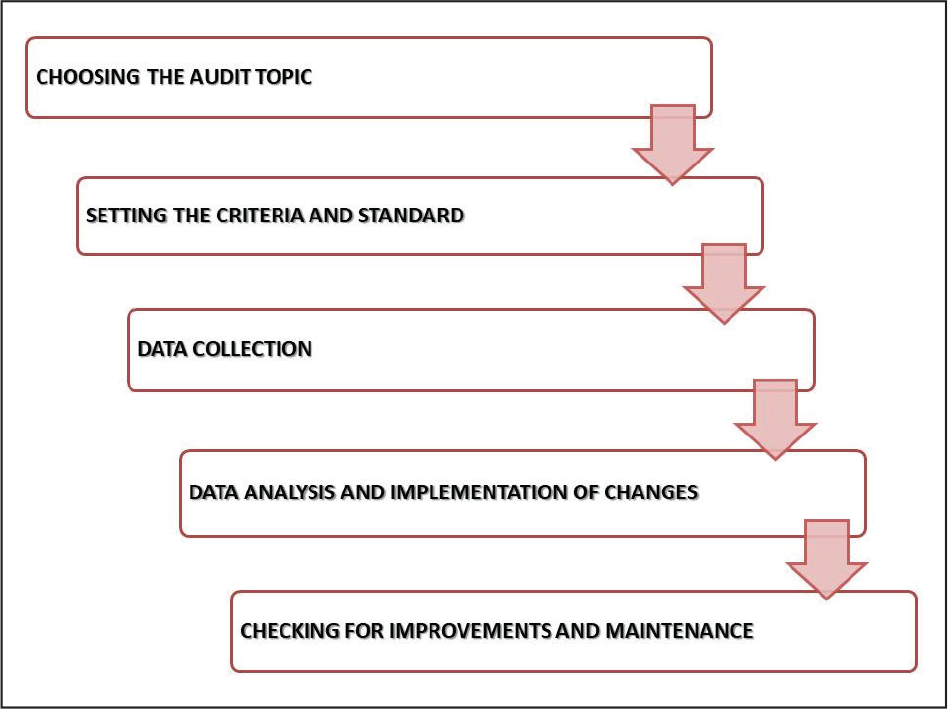
A standards-based clinical audit comprises of a number of steps, starting from selecting an important aspect of clinical practice which requires auditing, setting the standard, auditing practices and accumulating data, comparison of the data against the standard, identification of shortcomings in the practice, implementation of necessary changes, and in some situations, reaudit of said changes after a certain period of time (Figure 1).3 To the best of our knowledge, orthodontics-based clinical audits have not been conducted commonly, especially on a city-wide scale, with postgraduate trainees being the subject of assessment.
Steps in a Clinical Audit.
The aim of this audit was to investigate the type of cross-infection control practices being followed by postgraduate orthodontic residents of multiple dental institutes in a city and compare them with the recommended guidelines. Shortcomings in practice would be identified and the effect of re-education and revision of guidelines leading to improvements in clinical practice would be evaluated.
Methodology
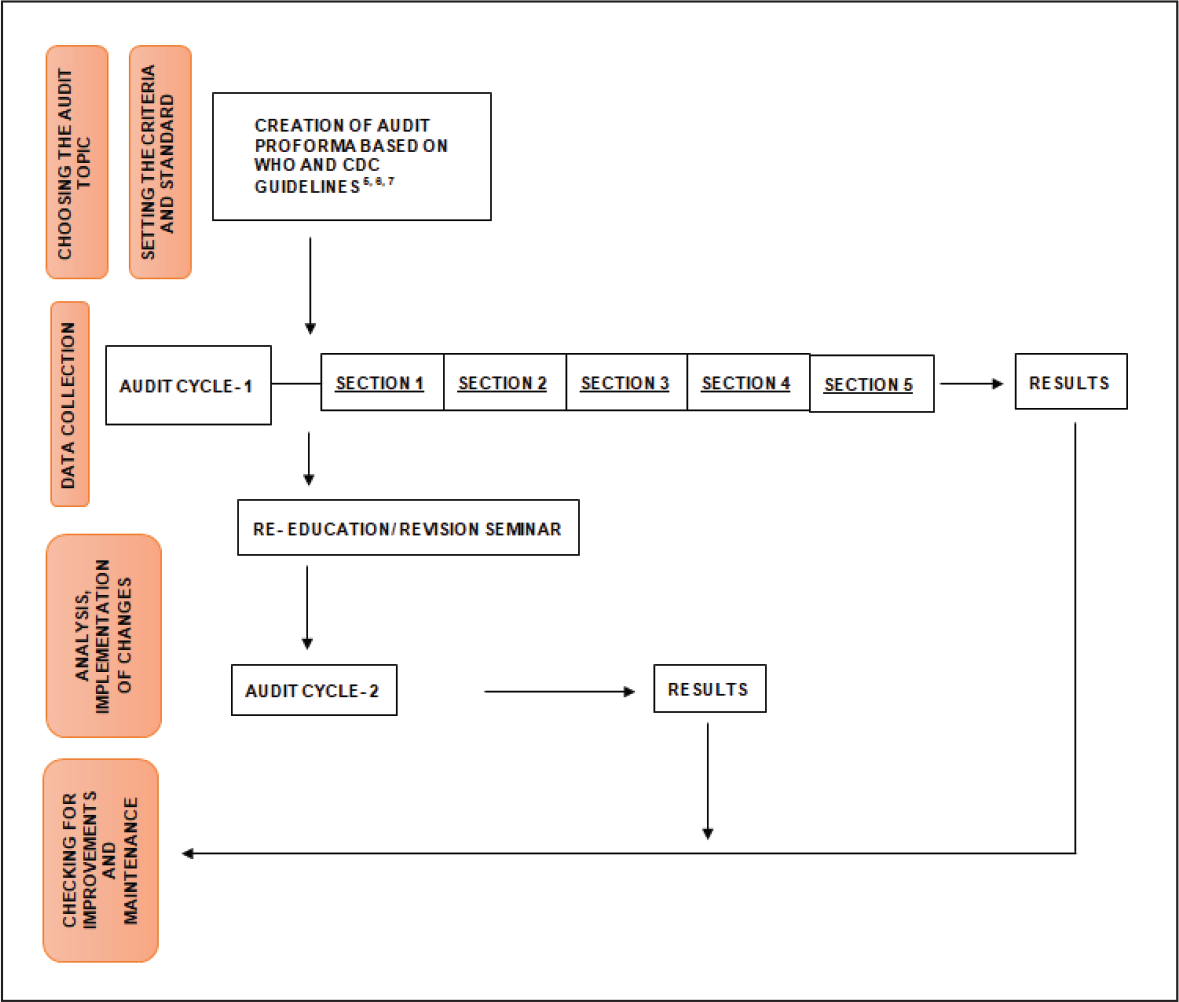
Two authors (AT, JS) designed a pro forma which was based on the latest guidelines for cross-infection control during COVID-19 as given by the WHO,5 Centers for Disease Control and Prevention (CDC),6,7 and those published in high-impact orthodontic journals.8,9 This would be used as the basis for evaluating orthodontic postgraduate residents of 5 dental institutions in Hyderabad, India, that were included in the clinical audit. The pro forma consisted of 5 main sections, namely:
The orthodontic postgraduate residents were observed independently over a full working day by 2 investigators who were well versed with all guidelines. The standard was set at 100% compliance with published guidelines.4 Practices being followed as per the pro forma would be marked as “yes” by the auditors and those not being followed would be marked as “no.” The findings of the 2 investigators were averaged and any disagreements were resolved by re-examination of the clinicians by a third investigator.
The audit was conducted in 2 cycles, where findings of the first cycle (undertaken during April 2021) were analyzed and shortcomings in the maintenance of cross-infection control protocols by the residents were highlighted. An online seminar for re-education and revision of the guidelines was held immediately after the first audit cycle, where the same clinicians being audited were trained in cross-infection control guidelines as given by the CDC6,7 and considerations for the provision of essential oral health services in the context of COVID-19 published by the WHO.5 Shortcomings found in the first audit cycle were stressed upon during the seminar and clinicians were urged to put the guidelines and considerations into routine practice as soon as possible.
A second audit cycle was undertaken by the same auditors on the same set of orthodontic residents 3 months after the revision seminar. Following an evaluation process similar to the first audit cycle, the findings obtained were statistically evaluated and mean differences in the practices between cycles 1 and 2 were compared to assess differences. A flowchart explaining the steps undertaken in the current clinical audit in accordance with the steps required for a clinical audit has been illustrated in Figure 2.
A Flowchart Explaining the Steps Undertaken in the Current Clinical Audit in Accordance With the Steps in a Clinical Audit.
Results
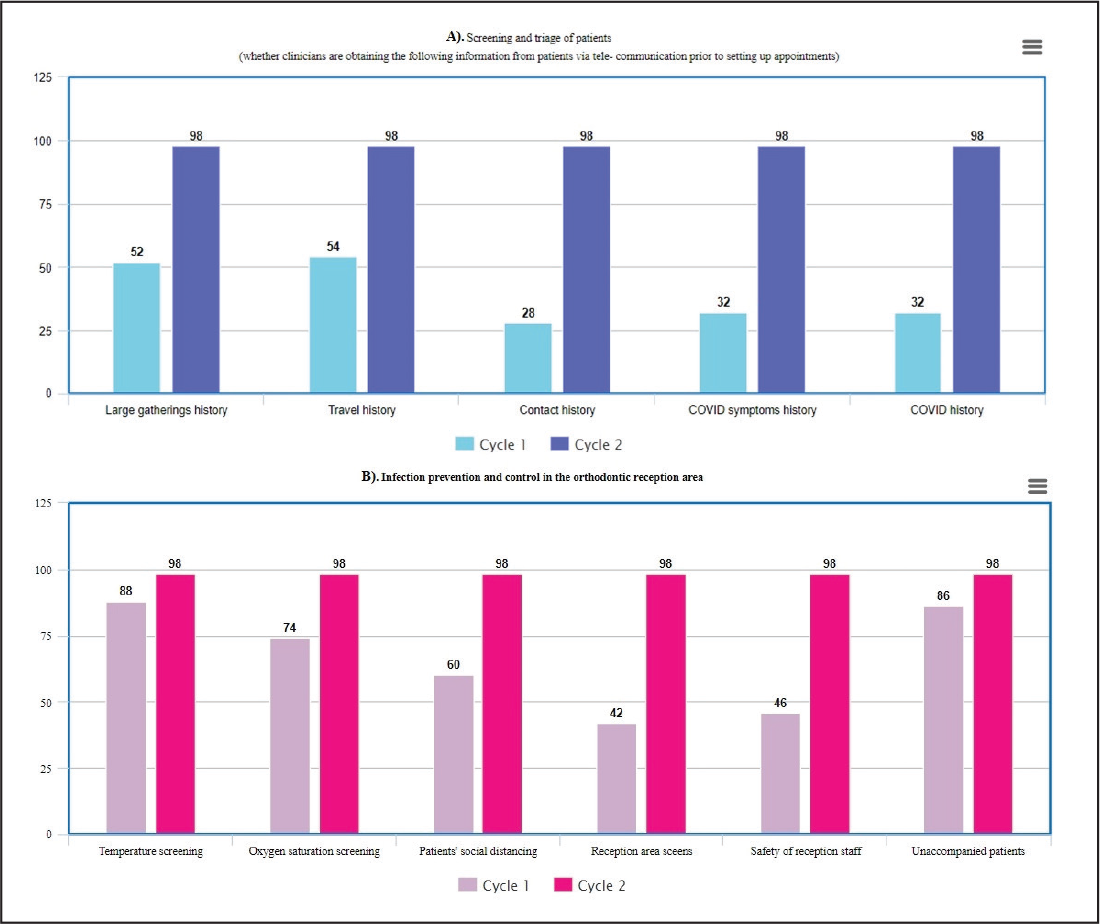
Summary of Results. (A) Section 1: Screening and Triage of Patients; (B) Section 2: Infection Prevention and Control in the Orthodontic Reception Area.
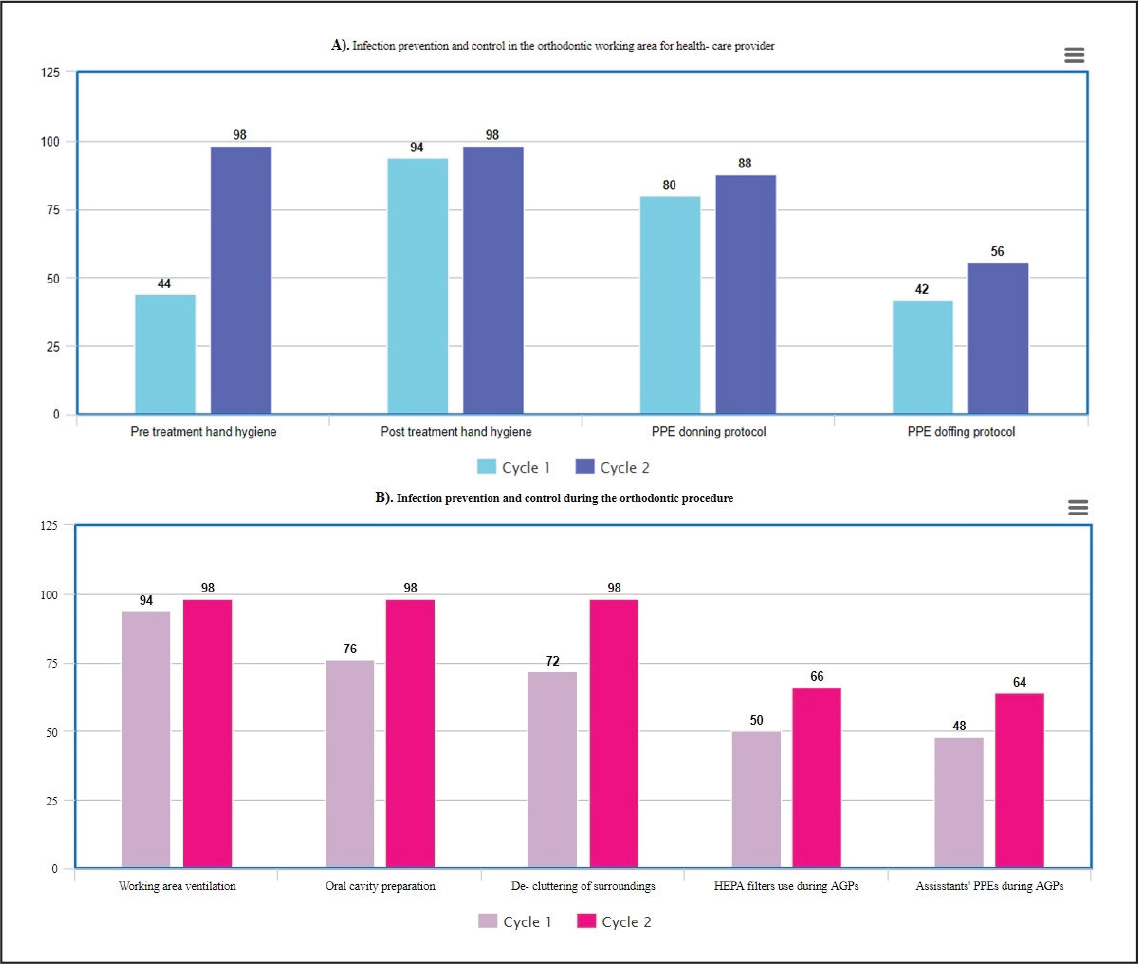
Summary of Results. (A) Section 3: Infection Prevention and Control in the Orthodontic Working Area for Health-Care Provider; (B) Section 4: Infection Prevention and Control During the Orthodontic Procedure.
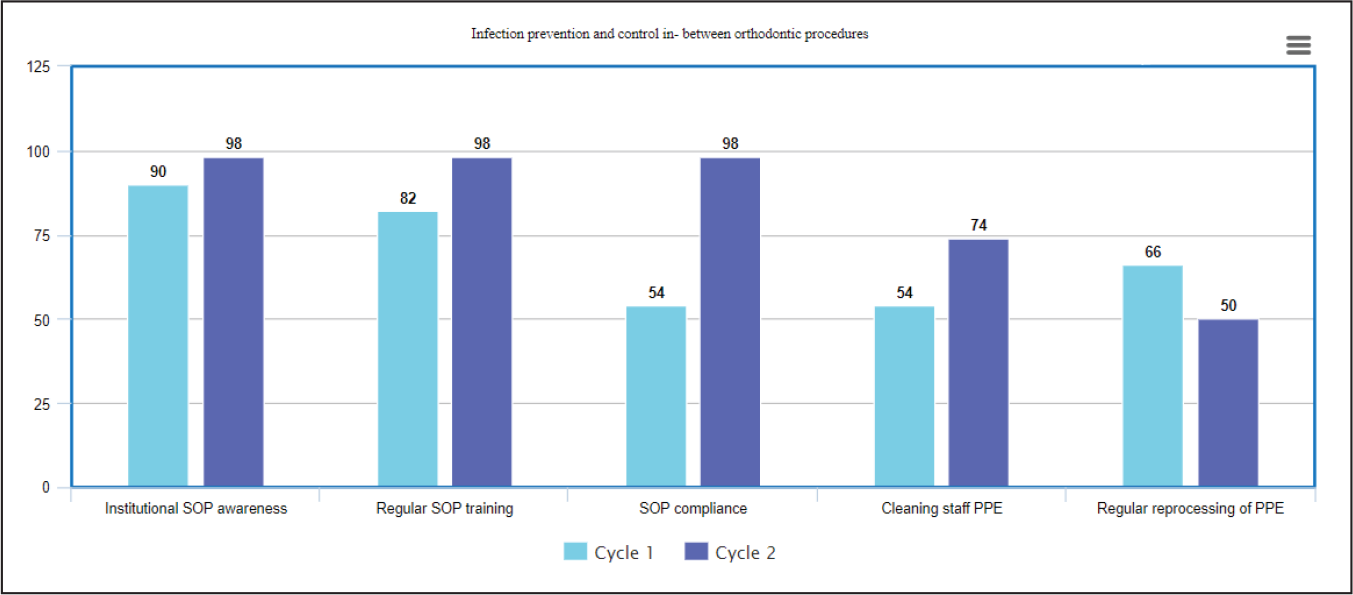
Summary of Results. Section 5: Infection Prevention and Control In-Between Orthodontic Procedures.
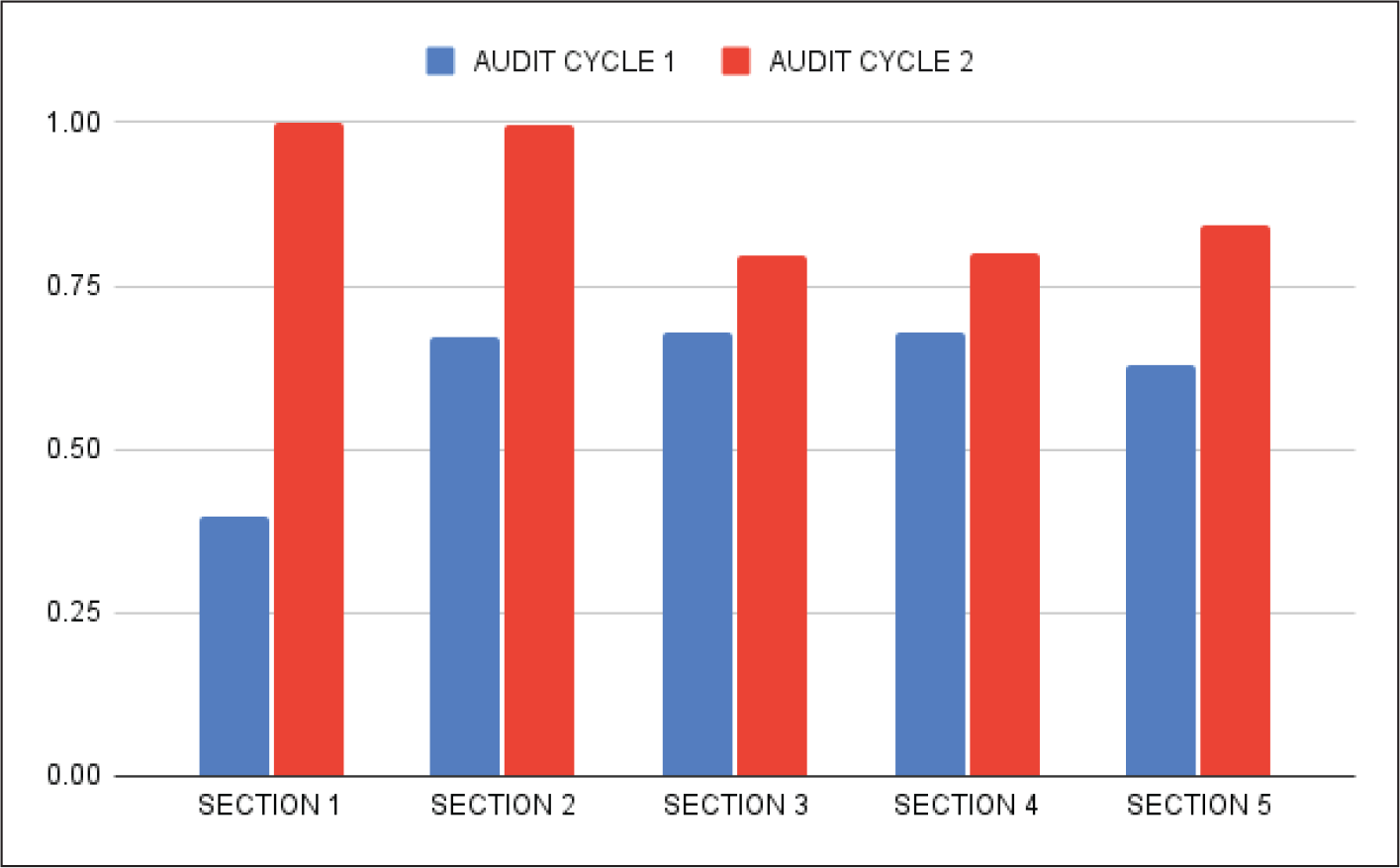
Upon reauditing the same set of residents after a re-education seminar, there was a significant improvement in results, as depicted in Figure 6 where the mean scores from each of the 5 sections of both audit cycles have been summarized.
Summary of Overall Results.
Discussion
Clinical audits are different from conventional research in medicine which allows one to explore different approaches or techniques for treating a particular condition. In contrast, audits help to assess whether the prevailing techniques are up to standards. Another advantage of clinical audits is that they help determine which iatrogenic factors (examples: resources used, type of training, case selection, etc) may be causing a difference in treatment outcomes despite following similar steps for all cases treated in a particular practice or by a group of clinicians.11 Finally, clinical audits provide scope for improvement as they highlight deficiencies in practice. Audits can be conducted multiple times over many years; however, the indicator of a positively growing practice is improvement in patient care every time an audit cycle is complete.12
An audit of clinical audits performed in orthodontics reported that there was improvement in the audit quality and information being published yearly.13 A setback found was that most were single-cycle audits which failed to re-audit and assess the evolution of standards following implementation of change. With this in mind, we conducted this city-wide audit of cross-infection control standards of orthodontic postgraduate residents in 2 cycles, 3 months apart.
Screening and triage of orthodontic patients is expected to be done prior to setting appointments either telephonically or via electronic mail, according to the WHO interim guidance published in May 2020.5 Results of the first audit cycle show that this section of the cross-infection control strategy seemed to be neglected by most residents examined. Amongst the parameters, it was observed that patient’s social gathering and travel history was assessed more frequently than history of their personal symptoms or contact with COVID-19 patients. Lack of habit or relaxation in implementation of anti-COVID-19 protocols after more than a year into the pandemic could be reasons for this. Since screening of patients via telecommunication is a relatively new concept, which has been typically stressed upon during the COVID-19 pandemic, conscious effort and strict protocol will be needed in order to adhere to these new norms. Ghai,14 in his review, concluded that “tele-triage” was an important component of teledentistry, especially during the pandemic, and must be incorporated into routine practice. An Indian government advisory in May 2020 published guidelines for dental professionals during the COVID-19 pandemic and stated that procedures should be undertaken only after teleconsultation, teletriage, and via prefixed appointments.15
Similar to telecommunication, equipping an orthodontic practice for operation during a pandemic also implies special considerations for the reception/waiting area. While a basic screening of patients and attendants for their oxygen saturation levels and temperature was a common practice, our audit revealed that practices like ensuring the safety of the reception staff by equipping them with proper masks and face shields and creating a barrier between the reception staff and patients with the help of glass/plastic screens were not routinely followed. While a majority of residents made sure that patients attended their orthodontic appointments alone unless in absolute need for assistance, it was observed that the number of appointments being scheduled for a day were not in compliance with the WHO interim guidelines which quote that “the patients in the waiting room should be able to maintain physical distancing of at least 1 meter.”5 Screening and infection prevention practices in reception areas improved drastically during cycle 2 of our audit, which shows that regular training/revision of protocols could help in avoiding unnecessary viral transmission.
Personal protection during clinical procedures is one of the most essential aspects for cross-infection control. According to the CDC guidelines, all patients are to be treated as suspected cases of COVID-19 unless discovered otherwise via appropriate testing.5 While most clinicians were well versed with steps in basic hand hygiene and wearing of PPE (donning) correctly, many were not aware that hand hygiene before putting on gloves or step-wise removal of PPE (doffing) was also part of guidelines laid down by the CDC and National Center for Disease Control, Ministry of Health and Family Welfare (MoHFW).10,16 Since PPE components retain viral and other pathogens on their surface, irresponsible removal and disposal of these can increase spread of the disease. Other guidelines such as changes ensuring proper ventilation around the working area,17 decluttering of surroundings, and preparation of the patient prior to starting treatment by mouth rinsing with an antiseptic mouthwash or 0.2% povidone iodine5 were followed to a good extent.
The current clinical audit found that only 48% of dental assistants used PPE in clinical procedures and 50% of operators used HEPA filters during AGPs. Lack of inventory or awareness could be some reasons for this. Re-education and reinforcement of these practices after the first audit cycle caused a semipositive change, with an increase in the use of PPE by assistants by 64% and the use of HEPA filters during AGPs by 66%.
The WHO recommends every institution to have an SOP for cleaning, disinfection, and waste management which is to be carried out after each patient discharge, along with regular training of the dental staff including cleaning staff and assistants in this SOP.5 While awareness about institutional SOPs was high and routine training of staff was followed, proper compliance with SOPs was neglected in most instances. One of the reasons for this could be the increased number of orthodontic appointments being setup after a long period of treatment deferment during the COVID-19 lockdown, leading to less time for disinfection activities. Other reasons such as lack of inventory and dearth of staff members are also probable. It was noted that training of staff in disinfection activities specific to orthodontic instruments was lacking, so this point was reinforced during the revision seminar held by the authors, in compliance with orthodontic guidelines summarized by Turkistani.9 Predictably, these practices improved after cycle 2 of the audit.
Guidelines on rational use of PPE by MoHFW18 state that sanitary staff is at a moderate risk of infection and the appropriate PPE for them is the use of N-95 masks and hand gloves. Use of appropriate PPE by the sanitary staff was another uncommon practice in 46% of cases audited. Despite this, instances of regular reprocessing of PPE kits were observed (66%). Guidelines state that PPE must be reprocessed only when there is shortage; however, given the expected state of funds and inventory in the departments audited and the unpredictable nature of the pandemic situation, strict adherence to this guideline maybe far-fetched. A systematic review by Hegde19 concluded that more research was required to assimilate solid evidence on the types, modifications, and appropriate method of donning and doffing of PPE for dental health-care workers. Cycle 2 in the audit showed an increase in use of appropriate PPE by sanitary staff as well as reduced instances of PPE reprocessing, which can be considered as a step in the right direction in terms of cross-infection prevention.
Conclusion
In the COVID-19 era, seeking routine orthodontic treatment could be considered a luxury rather than a regular medical service. Cross-infection due to lack of appropriate guideline adherence can cause serious harm to orthodontic dental staff as well as patients and their families, so it is important that clinicians ensure their safety by following basic protocols. We therefore conclude that while most practitioners have basic awareness about infection prevention practices, they are not fully compliant in following them either because of lack of equipment, time, or increased patient flow. Re-education/revision seminars and workshops conducted at regular intervals of time can ensure improvement in the said practices.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.