
Abstract
Objective:
To estimate the maximum voluntary molar biting force (MBF) and incisor biting force (IBF) and their relationship to morphological variables in subjects with different vertical skeletal patterns.
Materials and Methods:
Maximum voluntary MBF, IBF, and morphological variables were recorded in 120 subjects (60 males and 60 females) with skeletal class I pattern in the age range of 14 to 24 years. All subjects were divided into 3 groups: Normodivergent, hypodivergent, and hyperdivergent, according to the maxillomandibular plane angle and Jarabak ratio. Bite force measurements were undertaken using a custom-made portable digital gnathodynamometer on the left and the right sides of the jaw in the molar and incisor regions during maximal clenching. Statistical analysis was performed using independent t-test, chi-square test, and ANOVA test using SPSS version 22.0.0.0 software.
Results:
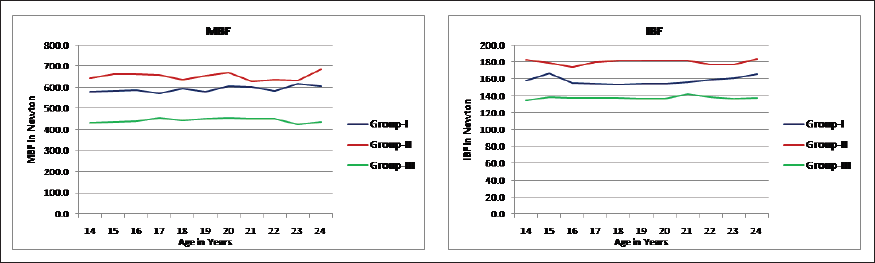
MBF and IBF are influenced by gender with higher values obtained for male subjects in all groups in the following order: hypodivergent > normodivergent > hyperdivergent. No significant changes were seen with morphological variables in different groups.
Conclusion:
Molar and incisor biting forces are highest in hypodivergent subjects and least in hyperdivergent subjects as a reflection of jaw morphology and muscular efficiency. In all groups, males exhibit higher force values than females, underlining a strong gender influence on biting force and facial pattern.
Keywords
Introduction
Biting force estimation is a potent tool for assessing the functional status of the masticatory system. Human bite force has been traditionally recorded in the first molar area1, 2 and a strong correlation between biting forces, strength of jaw elevator muscles, and craniofacial morphology has been demonstrated by numerous authors.3-7 The review of maximum voluntary biting force and its influencing factors has revealed wide-ranging values. These variations can be attributed to individual related factors like craniofacial morphology, physical characteristics (weight, height, and body mass index), 8 condition of the dentition, strength of jaw-closing muscles, and the pain threshold of the subjects 9 and technique-related factors like interocclusal clearance, site of measuring device placement, and head posture during biting force recording. 9 Based on the vertical skeletal pattern, craniofacial morphology can be grouped as hypodivergent, normodivergent, and hyperdivergent. 10 Diagnostic features of a hyperdivergent subject includes increased maxillomandibular plane angle and increased SN–MP angle, 5 whereas hypodivergent subjects present with deep bite and decreased SN–MP angle. 11 Among the 3 groups, normodivergent subjects produce higher molar biting forces than the hyperdivergent subjects (long face and open bite) with the highest values demonstrated by hypodivergent subjects (rectangular craniofacial morphology and skeletal deep bite). 12 Some investigators have established the influence of age and gender on biting force.13, 14 A weak correlation exists between maximum voluntary bite force and physical characteristics. On the other hand, bite force was found to exhibit an age-dependent increase in intensity.15, 16 Higher biting force values in males in comparison to females highlight the underlying gender influence on jaw morphology,12, 15, 17 but these correlations are less apparent in children. 1 The assessment of relationship of biting force with craniofacial morphology is essential to understand the variations in biting force, muscle strength, and masticatory efficiency in different individuals. In the past, orthodontic diagnosis and treatment planning focused solely on the anteroposterior dimension, in accordance with the Angle’s classification of malocclusion. With continued research, the importance of vertical dimension also came into existence, opening investigations into the possibility of association between MBF and IBF and its relationship with morphological parameters in different vertical patterns. Hence, such measurements have potential application as a screening tool for assessing the status of the masticatory apparatus. 18
The aims of the present study were as follows:
to evaluate maximum voluntary biting force in MBF and IBF regions in different skeletal patterns and to evaluate the relationship of maximum voluntary biting force with different morphological variables in different vertical skeletal patterns.
Materials and Methods
Ethical approval was obtained from institutional ethics Committee. The objectives and methodology were explained to all participants and written consent was obtained.
A total of 400 subjects were screened, and 120 subjects (60 males and 60 females) were included in this study, with a skeletal class I pattern, absence of crossbites, absence of previous extractions, absence of extensive restorations in first molars and central incisors, and no history of previous orthodontic treatment. None of the subjects had craniofacial anomalies and other bony disorders. A total of 120 subjects were divided into 3 equal groups, based on the maxillomandibular plane angle and Jarabak ratio,
2
as presented in the Table 1:
normodivergent that served as the controls (Max/Mand = 27 ± 5 degrees; Jarabak ratio = 59% to 63%); hypodivergent (Max/Mand ≤22 degrees; Jarabak ratio >63%); and hyperdivergent (Max/Mand ≥ 32 degrees; Jarabak ratio <59%).
Total Subjects Were Divided into 3 Groups.
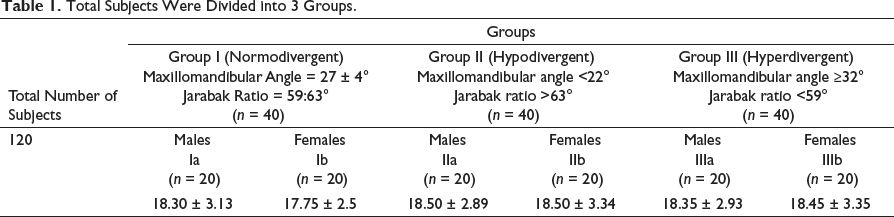
Their ages ranged between 14 years and 24 years, with a mean age of 18.38 ± 2.96 years for males and 18.23 ± 3.1 years for females, respectively. For each subject, maximum voluntary biting force at MBF and IBF) regions were measured, and morphological variables that included age, gender, height in meters, weight in kilograms, and body mass index (BMI: weight/height 2 ) were also recorded.
Maximum Voluntary Biting Force
Before the recording, the subject was seated upright, looking forward and without head support, with the Frankfort plane nearly parallel to the floor. Measurements were undertaken during a single session for each subject according to a standard procedure. 15 Maximum voluntary biting force was measured bilaterally, using gnathodynamometer at the first MBF and central IBF regions. The incisor bite force was recorded with the incisors in the biting off position, whereas the MBF was noted in the habitual closing position. 3 A novel portable digital gnathodynamometer (Loadmaster, Bangalore, India) was used to record biting force that consisted of a digital pressure gauge and a metal biting fork, encased in poly-vinyl material. Biting force was displayed digitally in newtons. The total vertical dimension of the biting fork was within the permissible physiological range of vertical opening for the masticatory muscles. Disposable plastic envelope covering the bite fork was used for each subject, and after each recording, the device was cleaned with cotton moistened with 70% alcohol (Figure 1). All subjects were instructed to bite as hard as possible on the gauge without moving the head. For each subject, bite force was measured 4 times, alternately on the left and right sides, with a 15-s resting time between each bite, and an average of values from both the sides was obtained (Figure 2). All subjects were comfortable during biting on the instrument. Overall, 10% of the subjects were randomly chosen and force measurements were repeated 1 day after initial data recording. The maximum MBF was 80% reliable and 84 % for the IBF. 19 The gnathodynamometer was calibrated after every 30th subject in the laboratory, using the E 3000 Instron universal testing machine, at The Central Institute of Plastic Engineering and Technology, Amausi, Lucknow, UP, India.
Custom-Made Digital Gnathodynamometer.

Method of Recording Right First Molar (MBF) and Right Central Incisor Biting Force (IBF).

For allocation to the groups, standardized lateral head cephalograms with teeth in centric occlusion for each participant were taken, using a Carestream cephalostat (CS 9000, Carestream Dental), at 64-kV, 16-mA, and 0.64-s exposure. The cephalograms were traced manually by 2 different authors, and 16 hard tissue cephalometric points were registered.
Morphological Variables (Weight, Height, and Body Mass Index)
Body weight was recorded in kilograms with personal scales to the precision of 0.1 kg, and body height was measured with the subjects in an erect position without shoes, using a height meter with a precision of 0.1 cm. The BMI of each subject was calculated. All the measurements were conducted by 1 examiner. 2
Statistical Methods
All statistical analyses were performed, using SPSS 16.0 windows software. Comparisons between groups were assessed by using independent t-test. All the categorical data were compared by using chi-square test. Parametric data were compared using chi-square test. Intergroup comparison was performed using the ANOVA test. A P-value of <.05 was considered significant.
Results
Maximum Voluntary Bite Force
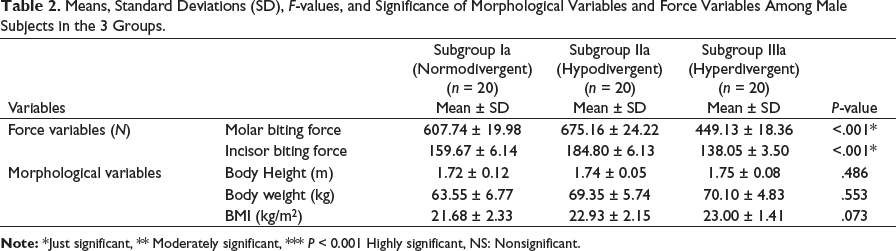
Means, Standard Deviations (SD), F-values, and Significance of Morphological Variables and Force Variables Among Male Subjects in the 3 Groups.
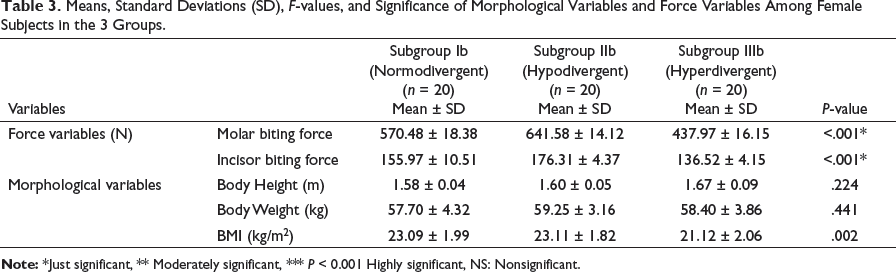
Means, Standard Deviations (SD), F-values, and Significance of Morphological Variables and Force Variables Among Female Subjects in the 3 Groups.
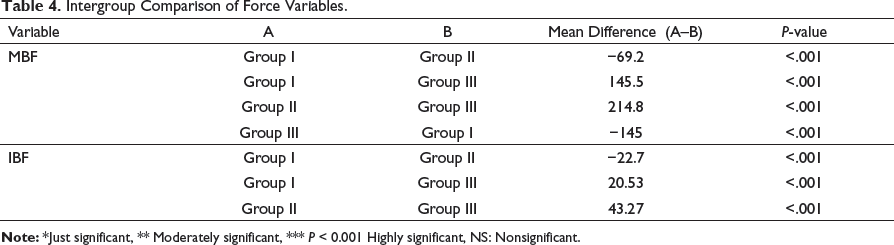
Intergroup Comparison of Force Variables.
Morphological Variables
The mean weight, height, and BMI for subjects in each group are presented in Table 2.
The mean weight of the subjects was 60.63 ± 6.34, 64.30 ± 6.86, and 64.25 ± 7.33 kg in group I, group II, and group III, respectively. The mean height ranged around 1.65 ± 0.11, 1.67 ± 0.09, and 1.71 ± 0.09 in the normodivergent, hypodivergent, and hyperdivergent groups, respectively, and the mean of BMI ranged around 22.38 ± 2.26, 23.02 ± 1.96, and 22.06 ± 1.99 in the normodivergent, hypodivergent, and hyperdivergent groups, respectively.
Discussion
A definite relationship between voluntary biting force in MBF and IBF regions and different skeletal patterns has been well established. But only few studies have investigated the interdependency of voluntary biting force at molar and incisor regions with morphological variables in different vertical skeletal patterns. So, the purpose of this study was to measure voluntary biting force at MBF and IBF regions and its relationship with morphological variables in different vertical skeletal patterns. For this study, we used a custom-made portable digital gnathodynamometer with a biting element.2, 19 This device has several advantages as it is easy to use, does not need any special mounting, has a durable metal fork, does not interfere with the tongue, and can be easily disinfected by changing the disposable plastic coverings that would be safe and comfortable for the patient. However, it has a metal fork that can still be considered hard to bite, and subjects can avoid producing maximum biting performance due to concern regarding dental fracture or pain. In this study, average MBF and IBF was higher than that measured by Ferrario et al 20 and Bakke et al 21 On the other hand, it was lower than that reported by Braun et al, 13 Okiyama, 22 and Kovero et al 23 When considering the male subjects, in hypodivergent group, mean MBF and IBF were found to be higher as compared to the hyperdivergent group, while the normodivergent group had an intermediate MBF and IBF values (Table 2). A similar trend was also obtained in the MBF of female subjects as well, that is, highest in hypodivergent group and least in hyperdivergent group with an intermediate value in the normodivergent group (Table 3). These force values are greater than those obtained by Proffit et al 10 who concluded that MBF and IBF are higher in normal faces as compared with long-face subjects. Ingervall and Helkimo, 4 Proffit et al, 10 Hagberg, 24 and Kiliaridis et al 25 commented that strong muscles produce more uniform facial morphology, while weaker muscles produce more diverse facial morphology. Biting force is considered to be an efficient indicator of the jaw’s lever system formed by associated facial and masticatory muscles. The adductor muscles of the jaws demonstrate a greater mechanical efficiency, in subjects with “short face–square jaw morphology,” rationalized by the vertical ramal anatomy and relatively acute gonial angle. 26 In contrast, increasing gonial angle reduces the mechanical advantage of the masticatory muscles, resulting in an acute-angled force direction to the occlusal plane. 27 This explains why hyperdivergent individuals tend to have poorer mechanical advantage, particularly of the masseter muscle, suggesting that they should have a lower maximum bite force. 28 These findings have been proven by electromyographic (EMG) studies on masticatory muscles, especially the temporalis and masseter muscles.24, 29 However, experimental studies suggest that mechanical advantage makes only a small contribution to maximum bite force as compared to other factors.26, 27 Maximum MBF and IBF are gender influenced with higher values in male subjects in all 3 groups. This is in agreement with the results obtained by Bakke et al 15 and Dean et al. 27 The fact that gender differences were evident at 15 years of age was in concordance with the report of Shiau and Wang 8 who found that bite force in males become significantly stronger than females after 13 years of age. We did not find a definite correlation between maximum biting force and age mainly due to the sample consisting of 14- to 24-year-old subjects. In this study, we did not find any conclusive evidence that biting force is influenced by physical characteristics such as height, weight, and BMI in agreement to the findings of Linderholm and Wennstrom 30 and Castelo. 31 This may be due to the inherent differences between children and adults. Additionally, lack of relationship with body weight and BMI could be the effect of physical training of certain muscle groups in adults due to a habit, sport, or work. 32 Reaffirmation of efficacy and efficiency of this humble and cost-effective novel device in comparison to highly sensitive sensor-based systems may be possible with a clinical trial on a larger and more diverse sample. 33
Conclusion
MBF and IBF are highest in hypodivergent subjects and least in hyperdivergent subjects as a reflection of jaw morphology and muscular efficiency.
In all groups, males exhibit higher force values than females, underlining a strong gender influence on biting force and facial pattern.
Morphological variables had no contribution in prediction of biting force in different vertical skeletal patterns.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.