
Abstract
Huntington’s disease is a progressive neurodegenerative disease characterized by motor, cognitive, and psychiatric symptoms. Dystonia of muscles is a characteristic feature of this condition. A case of Huntington’s disease, with orofacial dystonia, leading to severe uncontrolled biting of the lips, was referred by the Department of Neurology. Deep traumatic ulcerations were found in both upper and lower lips. A simple Essix retainer was fabricated and inserted, which acted as a barrier for the teeth from injuring the lips. The ulcers showed complete resolution in 3 to 4 weeks. The vacuum-formed retainers resulted in a good fit and resisted removal by the uncontrolled contortions of the orofacial muscles. The Essix retainer can be effectively used in improving the quality of life of patients, with Huntington’s disease, having such dystonia-related injuries to lips.
Introduction
Huntington’s disease is an inherited neurodegenerative disease primarily characterized by progressive motor, cognitive, and psychiatric symptoms. 1 The condition is extremely debilitating, eventually leading to death. No treatment modality is available to slow the disease progression. The current treatment of Huntington’s disease aims at managing symptoms and improving the quality of life, involving pharmacological and non-pharmacological measures. 2
Oral health aspects of Huntington’s disease have been sparsely enquired and written about in the literature. A literature search on the topics “Huntington’s disease AND Oral health,” “Huntington’s disease AND Dental,” and “Huntington’s disease AND Teeth” yielded only 13 results.3-15 These elucidate protocols on dental health care in patients with Huntington’s disease,4,5,7,10,11,15 implant-supported prosthetic management in elderly patients with Huntington’s disease,8, 12 dental pulp stem cell description in a primate, 13 and a case of endodontic management in a patient with Huntington’s disease. 9
This is a report on a case of Huntington’s disease with severe self-inflicted lip injuries caused by uncontrolled biting due to orofacial dystonia.
Case Report
A 29-year-old male patient with Huntington’s disease was referred from the Department of Neurology, Rajiv Gandhi Government General Hospital, Chennai, India. The referral was pertaining to the uncontrolled tongue and lip biting due to dystonia of the facial and masticatory musculature (Figure 1a and b).
(a) and (b) Uncontrolled Lip Biting. (c) Upper Lip Ulceration. (d) Lower Lip Ulceratiobn.

He presented with an altered gait with chorea. Seated in the dental chair, he showed dystonic neck movements and contortion of facial musculature. His mandibular movements were random, continuous, and uncontrolled, bringing the upper and lower lips between the teeth. He presented with lip ulcerations of varying dimensions and depth (Figure 1c and d).
The primary aim of this management was to prevent the ulcerations by forming a barrier between the teeth and lips. A conventional intraoral appliance was ruled out due to the dystonia of the musculature. Instead, a vacuum-formed thermoplastic Essix retainer was used as the barrier (Figure 2). This appliance, routinely used as a retainer after orthodontic treatment, snaps over the teeth, and is unaffected by movements of the tongue and jaws. Three to four weeks post insertion, the ulcers had resolved completely, while dystonia still remained (Figure 3a and b).
Fabricated Essix Retainer.

Healed Ulcers Post 3-4 Weeks of Wearing Essix Retainer.

Discussion
Huntington’s disease, originally named Huntington’s chorea, was first described by the American physician George Huntington in 1872. After the recognition that chorea is not the only manifestation, it is now termed Huntington’s disease. This rare neurodegenerative disease has a prevalence of 7 to 10 cases per 100,000 population in the Western hemisphere.16, 17 The prevalence is 1/10 of this in Asia. Prevalence and severity of pathology is more in women as compared to men. 18 Though the mean onset of symptoms is 40 years, early onset or juvenile Huntington’s disease sets in before 20 years of age and older-onset Huntington’s disease has onset as late as 70 years. 1
Huntington’s disease is a single-gene disease caused by autosomal-dominant inheritance of an expanded cytosine-adenine-guanine (CAG) trinucleotide repeat in the Huntington (HTT) gene on chromosome 4. HTT codes for protein “Huntington” which is essential for normal neuronal development. A normal Huntington gene has 36 repeats or less of the CAG nucleotide. It is abnormal if the repeats are more than 36. CAG repeats of 40 or more result in Huntington’s disease. 19
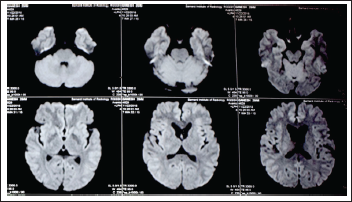
The referred patient was diagnosed at 29 years of age. Apart from the genetic feature of 45 repeats, he manifested neuroacanthocytosis and caudate atrophy 20 (Figure 4). There was no family history. Instability of intermediate alleles has been shown as a cause for sporadic Huntington’s disease in someone without a family history. 21
MRI Showing Caudate Atrophy.
Initially treated for psychiatric manifestations, he developed chorea and progressive dystonia. Dystonia of the orofacial musculature led to frequent injuries to the lips. The patient was responding to drugs initially but later became unresponsive, leading to alarming degrees of self-mutilation. A barrier in the form of an appliance, which, in this case, has to be uninfluenced by the dystonic musculature was planned and designed. The Essix retainer is an ideal barrier, owing primarily to its tight fit and being least influenced by the dislodging forces of dystonic orofacial musculature.
Conclusion
Lip and mucosal injury due to uncontrolled biting, owing to dystonia of the orofacial musculature, is a new clinical presentation in patients with Huntington’s disease. Contemporary treatment philosophy in the care of patients with Huntington’s disease is focused on managing the symptoms and improving the quality of life of the patient. This report is highlighted for its contribution in recommending effective management and prevention of self-inflicted lip injuries using an Essix retainer, which is a commonly used orthodontic appliance, requiring very less patient cooperation and chair time. As the retention of the appliance is completely independent of uncontrolled movement of the orofacial musculature, it can be an effective part of non-pharmacological repertoire available in the management of Huntington’s disease.
Footnotes
Statement of Informed Consent
Written informed consent was obtained from the subject for the use of photographs for publication.
Declaration of Conflicting Interests
Funding
The author received no financial support for the research, authorship, and/or publication of this article.