
Abstract
An innovative method to successfully erupt buccally impacted canines in difficult positions, that is, sector III and IV mesial to the root of lateral incisors into occlusion, has been described. 3-dimensional retraction spring is fabricated using 0.017 × 0.025-inch Titanium Molybdenum Alloy(TMA) wire and 45-degree bends are made simultaneously in 2 directions. The first bend is given distally starting from mesial of the first premolar and the second buccally at the same location. This 3-dimensional spring with its unique design provides the required labial and distal force with least chances of root resorption. A representative case is illustrated to demonstrate the clinical use of the same.
Introduction
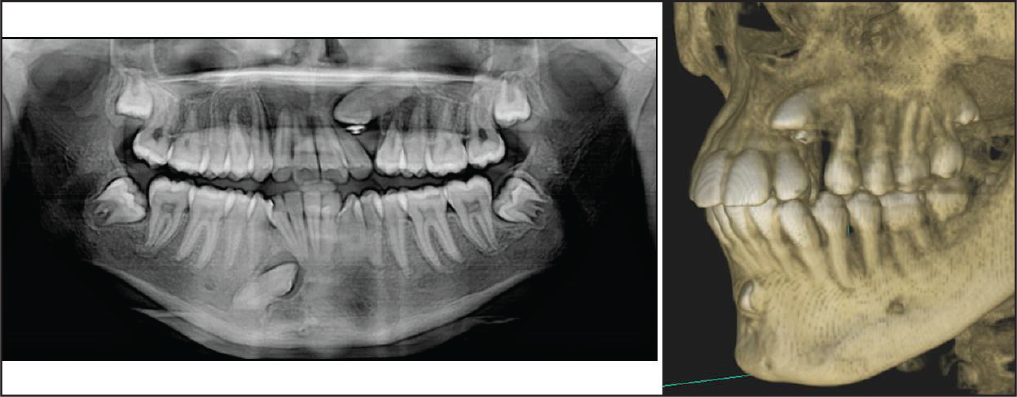
Maxillary canine impactions are a common orthodontic clinical problem, and the position and angulation of the impacted canine determine the method for surgical exposure and mechanics to be used. 1 Buccally impacted canines are often difficult to manage due to the proximity of roots of lateral and central incisors and, thus, the risk of root resorption. There have been earlier attempts to erupt similar impactions using thick labial wires and cantilever springs, but the mechanics were complex.2-4 This article describes an innovative method to successfully erupt buccally impacted canines in difficult positions, that is, sector III and IV, according to Lindauer et al. (Figure 1), 5 mesial to the root of lateral incisors into occlusion. The representative retreatment case depicts the management of buccally placed impacted left maxillary canine in sector III approximating the root of left lateral incisor.
Fabrication
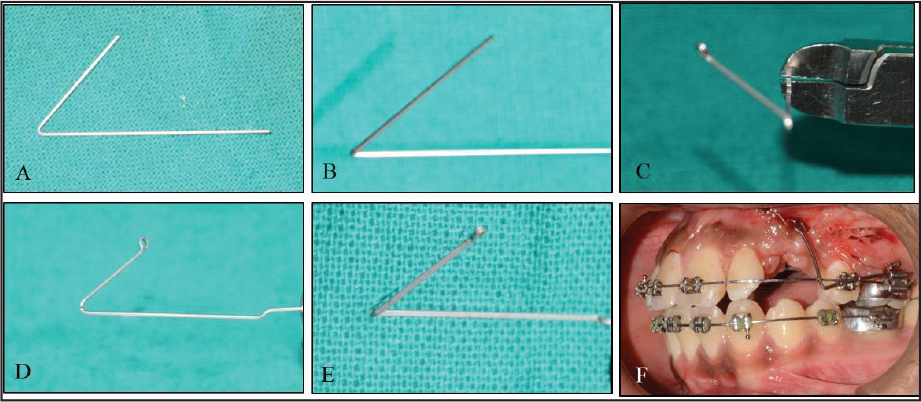
The straight 0.017 × 0.025-inch TMA wire for 0.018-inch slot (0.021 × 0.025-inch TMA wire for 0.022-inch slot) is given 45-degree bends simultaneously in 2 directions. The first bend is given distally starting from mesial of the first premolar (Figure 2A) and the second buccally at the same location (Figure 2B to C).
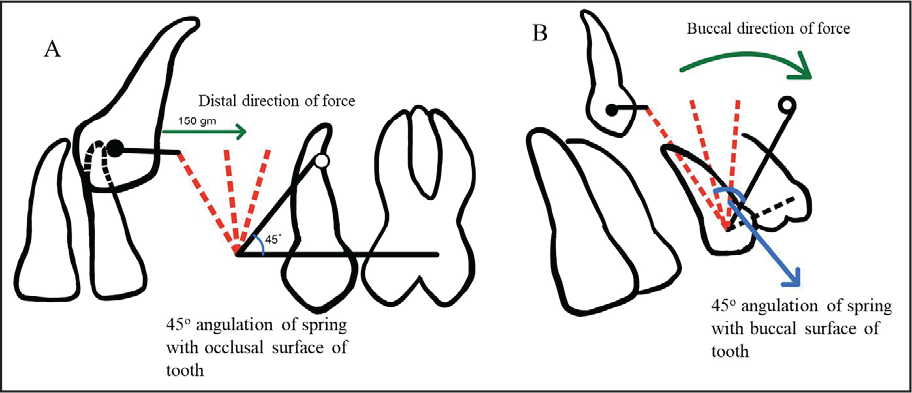
The wire is inserted in the preadjusted edgewise accessory buccal tube to provide necessary torque for the buccal traction force. The height of the spring is kept at 10 to 15 mm to avoid initial occlusal forces, and the activated spring is then ligated to the exposed canine to provide 150 g of resultant force (buccal and distal, simultaneously) (Figure 2D to F). Graphical representation of biomechanics of force system is shown in Figure 3. The buccal force may be adjusted according to the requirement of the case to retract the canine away from the roots of the incisor. Anchorage enhancement of maxillary molars was obtained with Nance palatal button/temporary anchorage devices before placement of spring.
Alignment of the retracted canine into the arch was achieved with piggyback wire and sequential archwires in 11 months (Figure 4A to D).
Source: Unit of Orthodontics and Dentofacial Orthopaedics, OHSC, PGIMER, Chandigarh.
Source: Unit of Orthodontics and Dentofacial Orthopaedics, OHSC, PGIMER, Chandigarh.
Source: Unit of Orthodontics and Dentofacial Orthopaedics, OHSC, PGIMER, Chandigarh.

Source: Unit of Orthodontics and Dentofacial Orthopaedics, OHSC, PGIMER, Chandigarh.
Discussion
This 3-dimensional spring with its unique design provides the required resultant force with a labial and distal component with least chances of root resorption. The higher initial labial force component is necessary to move the impacted tooth away from roots of approximating teeth. The height and distal angulation of the spring may require adjustment for individual case. It may also be required to change the angulation with the progress of treatment as the position of the impacted canine changes. Thus, the spring has to be adjusted or sometimes refabricated a couple of times in more complicated impactions. Moreover, the design is easy to fabricate chairside with no extra laboratory time required.
Conclusion
The presented 3-dimensional retraction spring is very easy to fabricate and is a useful clinical tool for management of buccally impacted teeth. The same spring can be successfully used for eruption of most buccal maxillary canine impactions in sectors III and IV with minimal modifications.
Footnotes
Author Contributions
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.